
Abstract

Dear Sir,
The Mental Health Care Act, 2017 1 is amongst the most progressive legislations espousing a rights-based approach to mental health care. 2 The vehicles of MHCA include the Mental Health Review Board (MHRB), State Mental Health Authority (SMHA), and Central Mental Health Authority (CMHA).
The SMHA functions at the state level, and MHRB has been conceptualized to function at the district level, and the latter’s jurisdiction may be extended to a few districts. 3 The CMHA has been formed vide notification No. V. 15011/09/2017-PH-I and is tasked with registering all the mental health establishments (MHEs) under the central government. 3 Implementation of the MHCA 2017, notifications of rules thereupon, and formation of MHRB were recently discussed in the Rajya Sabha. 4
Current Status of SHMA and MHRB in the South Indian Territory
We examined the notifications of MHCA rules and the formation of SMHA and MHRB across the Indian Psychiatric Society South Zone territories. 5 A rapid review of pertinent central and state government notifications and gazettes was undertaken from websites up to October 30, 2021, to get information on the formation of MHRB and SMHA.
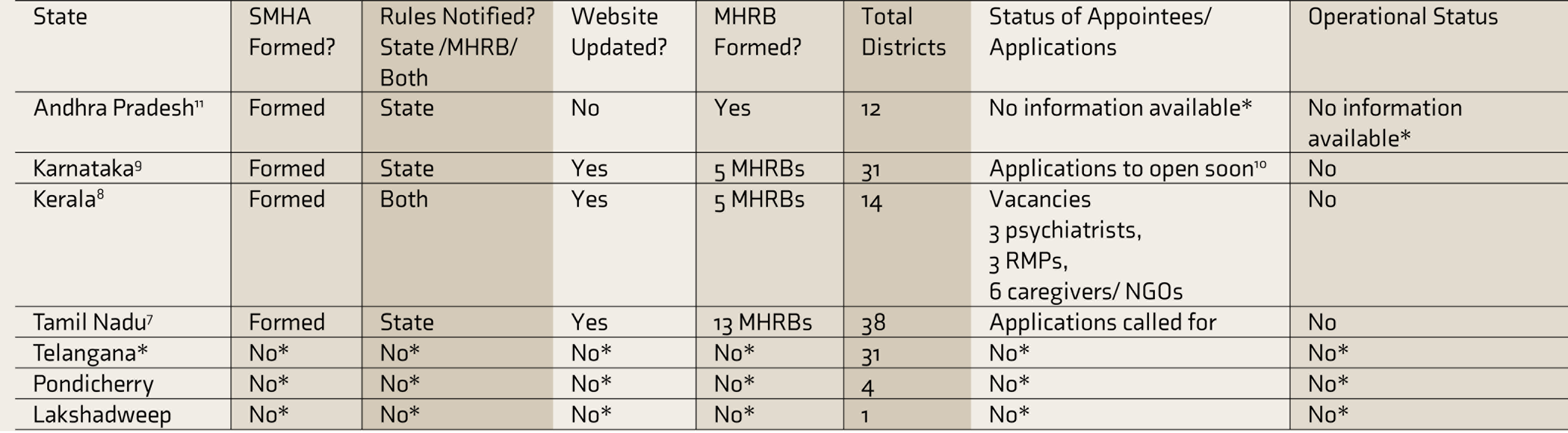
The implementation of the MHCA 2017 across these states is at different stages (Table 1). Three of the five states had websites and MHRBs, while four had notified rules regarding SMHA. None of the union territories have websites or MHRBs. Of the states that had proceeded with the formation of MHRBs, three had received applications and made appointments. Anecdotally, judicial interventions have helped to hasten this process in Kerala. The Kerala Legal Services Authority intervened in the Kerala High Court, requesting hastening the implementation of the MHCA. 6
Implementation Status of the MHCA 2017 Across South India
The Way Forward
Nearing five years post-enactment and over three years since coming into effect, it is high time to examine the extent of implementation of provisions of the MHCA. The COVID-19 pandemic has disrupted and slowed the implementation of various policies and programs. However, on a positive note, mental health has now gained much more traction than ever before. State authority for mental health services under the MHA 1987 persists in some states, while no MHRBs under the MHCA 2017 have been formed. Mental Health Practitioners (MHPs) face challenging clinical situations when their practice intersects with the law. It is the best opportunity for MHPs to review the current legalities and nuances to initiate relevant advocacy efforts.
MHRB is a quasi-judicial body with sweeping powers regarding the treatment of persons with mental illness as well as the functioning of the MHEs. We noted that MHRB formation and MHCA implementation have been tardy at best. It is in the interest of psychiatrists to advocate for MHRB formation as well as participate in its functioning. Psychiatrists must advocate appropriate and quality mental health care through their role in this vehicle of the MHCA. A large professional body like the Indian Psychiatric Society would do best also to safeguard the interests of those psychiatrists who engage with these boards. Some issues that need immediate advocacy are attractive remuneration packages to make such involvement meaningful and worthwhile, given that any psychiatrist would have to extricate themselves from their practice to attend to these added responsibilities. Tamil Nadu has modeled this in specifying remunerations for each MHRB position, with the judge receiving ₹1,00,000 and the psychiatrist receiving ₹50,000. 7 There is a need to have guidelines for professional conduct and review to assuage apprehensions of MHPs because there is only 17% representation for MHPs (of the six members constituting the MHRB, only one is MHP). 7 It would be beneficial if psychiatrists, especially those in private practice, proactively take up positions of the MHRB’s general medical practitioners.
The South Indian states have not stipulated experience thresholds for the positions in MHRB.7–10 However, the qualification and experience of the MHPs in the MHRB should be such that they should be in a position to review the functioning of MHPs and MHEs, have required experience, and be of good standing.
Financial limitations may be an important barrier to overcome in implementing MHCA. There is a need to find innovative and cost-effective means for effective implementation. The appointment of part-time psychiatrists from district hospitals and medical colleges with allowances could be piloted in a few districts and later be implemented at a national level. It is also important to allow for online functioning of the board, considering both the prevailing pandemic and saving costs.
Psychiatrists and their professional bodies would also do well to promote the involvement of their patients and carers by apprising them of such opportunities. Current and prior mental health-care service users who have benefited from mental health care are best positioned to discharge MHRB roles as patient and carer representatives.
It would be prudent to develop incentivized certificate courses toward informing how best the MHRB could function to safeguard user and provider interests. Similar short-term courses on how general practitioners could do capacity assessments and support patients would ensure that motivated practitioners are sufficiently equipped. Over time, these training programs could be incorporated into the emergency room and psychiatric training for medical interns. Professional bodies could also collaborate with advocacy groups and social activists to speed up the implementation. The initial few years of any such endeavor are often riddled with frustrations and misadventures, especially because this involves multiple stakeholders.
It would be ideal if MHRB positions were contractual and full-term so that initial roadmaps and protocols could be ironed out, especially regarding compliance for MHEs, documentations, appeal processes, registration and inspection efforts, and the development of best conduct guidelines. We recommend that the functions of the MHRB listed in the MHCA be codified as terms of reference. Such terms of reference would provide a clear construct within which the MHRB could function—this would help clarify when the MHRB could take Suo moto (on its own) cognizance.
Footnotes
Declaration of Conflicting Interests
The authors have no potential conflicts of interest to declare with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.