
Abstract
Amputation is the surgical removal of all or part of a body part. It demands an adjustment in almost every sphere of a person’s life in addition to physical disability. An amputee faces problems in almost every psychosocial sphere.1, 2 Along with physical pain in the stump, patients may experience phantom sensations.3–5 Patients may also grieve, feel depressed, and anxious3, 6, 4, 7 or have posttraumatic stress disorder symptoms.8, 9 They may be apprehensive about their future plans and inconclusive regarding life challenges. Grief is one of the most common reactions to amputation,10, 1, 7 but often gets neglected in intensive surgical units. 1 Many times, grief reactions are not resolved, turning into complicated grief or prolonged grief, leading to conditions like depression, anxiety, or even suicide. This article is about an attempt to help a patient initiate the grieving process for healthy outcomes.
Case History
Mr. G is 30 years of age, Muslim by religion, from lower-middle socioeconomic status, educated till seventh grade, married, and the father of a three-year-old boy. He is a carpenter by profession and is living with his parents. He is the sole earning member of his family and is occasionally supported by his father. He was known to consume cannabis (one cigarette) and diazepam 2 mg (two to three tabs) on weekends for the last one year. He would also consume hard beer once a month except in the month of Ramadan (fasting). His family knew about his occasional substance abuse, which often resulted in frequent fights and altercations with his wife. He would work on and off only and that also created financial concerns. This was the second topic of frequent altercations with his father as he was not settling for a proper job. One evening, he had an altercation with his father regarding his job, following which he left his home, smoked weed, and consumed alcohol with his friends. In this intoxicated state, he walked on the railway track where he met with an accident. He was admitted through the emergency department of Jai Prakash Narayan Apex Trauma Center, All India Institute of Medical Sciences (AIIMS), New Delhi and underwent left below-knee amputation for mangled extremity.
The clinical psychologist met him in the surgical ward on the second day of his admission, after the surgery, when his vital parameters had settled. The clinical psychologist introduced himself, and after brief interviewing, the patient was found to be depressed, grieving over his lost limb, and had death wishes. He was apprehensive about revealing to the family that drug abuse was the cause of the accident. His family believed that he had tried to commit suicide. This made him terribly guilty, and he was crying throughout the session. A few utterances were found important by the end of the first session: “I don’t remember how this happened, my wife is going to leave me, please don’t tell my wife about amputation, my family will not support me, what will I do for a living, why this happened to me, I should have stayed back home, I shouldn’t have consumed alcohol.”
Consultation with a psychiatrist was done, and the impression formed was of adjustment disorder (grief reaction) as per International Classification of Diseases ten criteria, and he was put on tab clonazepam 0.5 mg sos.
Bedside Grief Counseling
Grief reaction after an amputation is a common reaction that makes a person go through all the stages of the grieving process as devised by Kubler Ross. The prime concern of a psychologist is to help a grieving person go through the stages of grief as smoothly as possible. The index patient was given five bedside grief counseling sessions before his discharge, and the sessions were continued in the amputation clinic every week till 18 weeks of amputation. With respect to the model given by Kubler Ross, 11 the patient seemed to be swinging between denial and anger, and the thoughts of guilt and self-blame were not letting him move forward with the grieving process. There is no doubt that time heals grief, but if the process gets stuck, it can lead to complicated grief, depression, and at times suicide. 12
Grief counseling is based on certain principles like helping the persons to accept the loss, helping them identify and experience their emotions and identify issues like guilt, anger, and sadness and try to deal with it, helping to live life with the loss, helping to find the meaning in the loss, and providing time for healthy grieving. 13 The above goals are achieved by different techniques like cognitive restructuring, imagery, use of metaphors, etc. While dealing with sensitive issues such as grief, basic principles, and techniques of counseling become very handy. Accepting the patient as he/she is with all the positives and negatives without any judgment (unconditional positive regard; he was not judged for his substance behavior), in fact his behavior was medicalized, and he was told that it is a disorder and anyone would have exhibited somewhat similar behavior in the intoxication phase. Expressing empathy by reflecting and validating the emotions the patient is sharing and providing a safe platform to vent out helps initiate a healthy grieving process. 1 Empathy was expressed to him by reflecting and validating his account and emotions. Statements like “I understand how you must be feeling right now,” “It must be hard for you,” etc. were used.
The index patient was not able to initiate healthy grieving as he was engulfed by immense guilt and self-blame. Above all, this was leading to disenfranchised grief14, 15 (grief reaction that is either not validated by or acceptable to a particular society, e.g., death of a pet or death of lover of a person who is married to someone else). In this case, the patient was not able to reveal to the family members that his substance abuse was responsible for the incident.
A brief session on psychoeducating the patient’s family members was done. They were sensitized regarding the emotional state of the patient. The need for essential emotional support from the family was made evident. After the end of every session, the patient was given three to five min of deep breathing exercise. The patient was also psychoeducated regarding amputation, why it was done, and the prosthesis that can make him functional again.
The therapist tried to change his cognitions so that he may stop self-blaming and having guilt (cognitive restructuring).
Pt: You don’t know what I did to my life; I abused drugs and consumed alcohol, and because of all that, I lost my limb.
Therapist: Yes, psychoactive substances often impair the judgment and consciousness of the person, and such accidents happen.
Pt: Drugs took everything from me; I can’t even tell my parents what actually happened that night.
Therapist: Yes, that is right, I can understand what you must be going through
(Conversation translated from Hindi)
The use of metaphors was included in the session to make him accept the loss and try to move on with it. “A Journey” metaphor was used, telling the patient that everyone’s life is like a journey and there are ups and downs, sometimes bumpy roads, rough or smooth ones. It keeps on changing as we move forward. Life has the same pattern; there are tough times and happy moments: both keep on coming and going; we all just cover our journey. Further, the imagery was used to help him feel being able to walk again with the help of a prosthesis. He was given reassurance that he would get functional and live a good life. 1
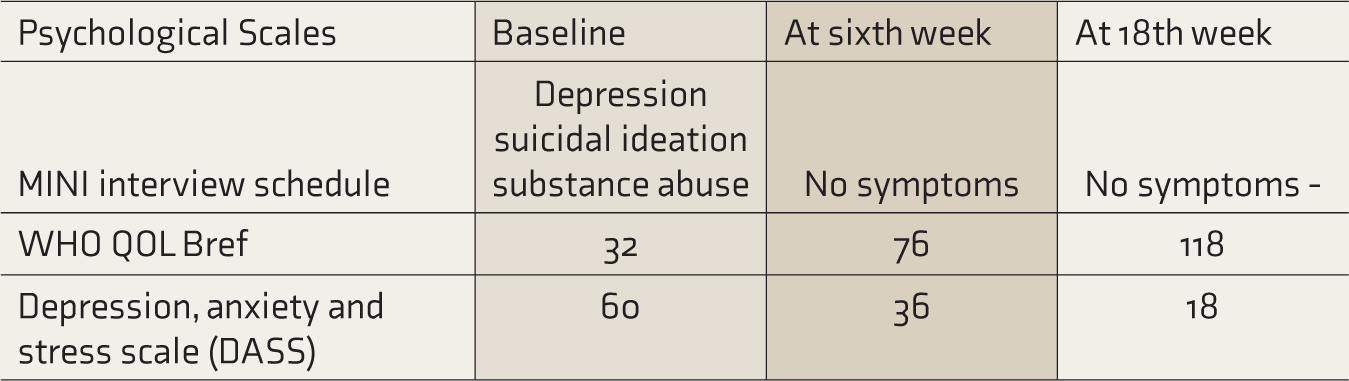
Table 1 depicts scores on psychological scales applied at various time points.
Scores on Rating Scales
Discussion
Amputation leaves the patient in a very stressful condition. 16 Researchers report that loss of a limb is comparable to the loss of relationship with loved ones 17 or even their death.18, 19 The necessary grieving process becomes a way that helps the patients readjust in their lives. Patients go through stages of grief, as described in one of the popular models proposed by Kubler Ross. 11 Grief is something everyone has to go through at some point in time. To resolve grief, there is no need for any psychotherapy or counseling. 20 But one needs help if the grieving process gets halted, delayed, or complicated because of different reasons. Many patients have stressful lives before amputation, which leaves no favorable space for them to express grief. The same was the issue with our case; he could not share with his parents that he was intoxicated while the accident happened. This led to self-blame and guilt. Bedside sessions allowed him to express his emotional state in a safe environment. The patient had chances of getting into disenfranchised grief as the reason for the accident would not have been acceptable to the parents. The therapist provided a safe place for the patient to vent out his emotions so that related issues could be tackled in counseling. The companioning model of bereavement by Dr Alan D. Wolfelt 21 says that we should help people integrate life’s losses by being present to them and observing them – companioning. John Welshons, 22 in “Awakening from Grief,” says, “So there is no way to apply systems, rules or emotional road maps. Our job is to be a presence rather than a savior. A companion rather than a leader. A friend, rather than a teacher.”
Finally, the bedside grief sessions ensure a normal grieving process and a quick check for suicidal ideations, if any, that need to be taken care of in the sessions. When our patient was given the hope of resuming his functioning after using the prosthesis, his affect changed, and it felt like a ray of hope helped him heal quickly. Even if there is the possibility of delivering only a few bedside sessions, they should be included in the protocol of inclusive treatment of physical trauma survivors.
Bedside sessions are not done in settings similar to conditions available in conventional psychotherapy or counseling sessions. So, whole grief therapy may not be possible at the bedside but can be resumed in follow-up sessions.
Conclusion
The benefits of delivering bedside grief sessions were clearly evident in the index patient. Delivery of bedside grief sessions in a surgical ward soon after a surgical procedure would help patients to initiate the grieving process in a healthy way.
Footnotes
Declaration of Conflicting Interests
The authors have no potential conflicts of interest to declare with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Necessary consent was received from the patient for publication.