
Abstract
Mental health issues impair decision-making capacity, more so in elderly people. Impaired decision-making capacity can make person unfit to enter into various civil deeds and agreements. Such civil deeds can include guardianship, property transaction, holding a bank account, having voting rights, making a will, donating an organ, etc. This article focuses on importance of mental health in entering into above-mentioned civil agreements, how to do assessments to determine if one is fit to enter into civil agreements, and what are the legal ways in which a person can avail help to execute his/her civil rights even when affected by mental health issues.
The world has witnessed a demographic transition towards the elderly because of increasing life expectancy and reduced fertility rates. Globally there were 727 million persons aged 65 years or above in 2020, 1 which makes 9.3% of the total population, and this group is expected to increase to 16% by 2050. 1 Increased longevity has led to an increase in the prevalence of mental health disorders in the elderly.2,3 Mental health issues compromise an individual’s functioning in several ways, including their decision-making capacity, albeit often temporarily. These conditions pose unique needs in the elderly such as assistance in making decisions and additional support systems such as guardians. However, it is imperative that while additional support is facilitated, fundamental rights such as the right to autonomy and dignity of the elderly are not violated, and there are various legislatures passed to ensure the same.
Civil responsibility (CR) refers to the responsibilities of the individual while he/she executes any civil deed or agreement. Various physical, psychosocial, medical, environmental, and mental health issues are prevalent in the geriatric population, hindering their ability to execute civil deeds or contracts. This hindrance might also attract civil litigation if it is not legally appropriate. The State has a duty of care for the elderly and will have to provide remedies for such civil litigation in which the elderly get entrapped. This article discusses various civil litigation situations that might arise, such as capacity assessments, including testamentary capacity, voting, driving, organ donation, banking, and the role of psychiatrists and provisions in the legislature to address these issues.
Decision-Making Capacity in Civil Issues
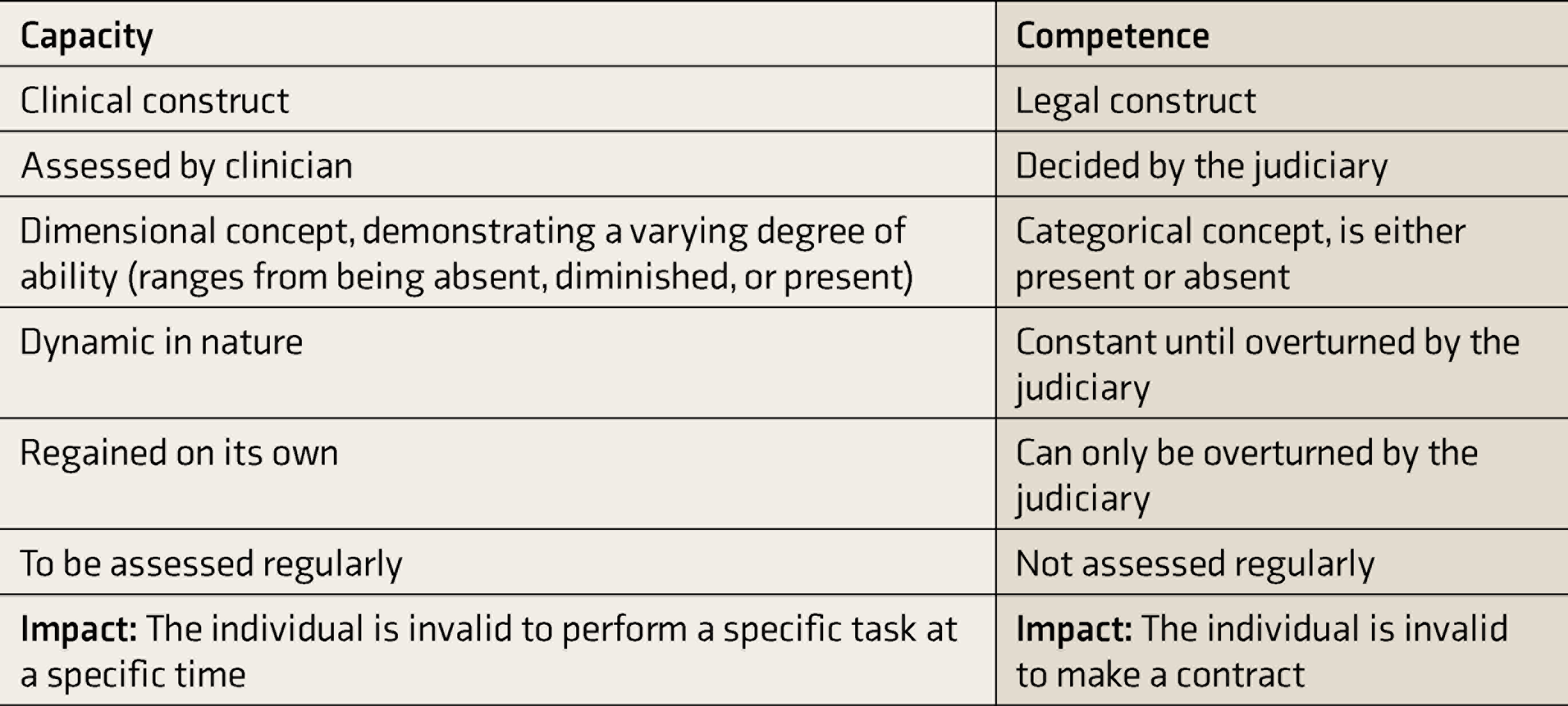
Capacity is a clinical construct, which is task-specific and dynamic. It refers to an individual’s ability to make and communicate decisions in an autonomous manner. A clinician generally assesses capacity. Capacity should be differentiated from competence. 4 A summary of differences between capacity and competence is provided in Table 1.
Difference Between Capacity and Competence
Principles of Assessment
Grisso and Appelbaum in 1998 provided the “four abilities” model in assessing capacity. 5 These include the ability to understand the information, weigh the pros and cons of this decision, appreciate the consequences of the decision, and communicate the decision at hand. Capacity assessment is a right-based approach providing autonomy and dignity to an individual, which marks a shift from paternalistic handling of issues in hand. 6 In practice, the assessment of capacity is ethically, legally, and clinically complex. Lack of capacity is a clinical judgment, and assessment tools merely guide in building the clinical judgment. There are various assessment tools available for specific mental health conditions and the task at hand.4,7,8
Need for Assessment
Capacity assessment might be warranted if there is a suspicion of incapacity in the geriatric population. However, an adult is assumed to have capacity unless proven otherwise. Ability to make treatment-related decisions, ability to enter any contract (example: property, marriage, etc.), making a Will, consenting to sexual activity, power of attorney (PoA) decisions, etc., are some of the situations where capacity assessment might be required. The burden of proof of proving incapacity lies on those who seek the individual’s lack of capacity. 9 Capacity assessment is always done for a specific task, and a specific lack of capacity cannot be generalized to other tasks. For instance, an individual may not have the capacity to make treatment-related decisions but might retain the capacity to consent to sexual activity.
Measures to Reduce the Risk of Abuse if Capacity Is Lost
There are various measures one can take to reduce the risk of abuse if one were to lose capacity. Some of these are:
PoA: It is a legal instrument whereby one person gives another person the authority to act on their behalf as his legal representative and make binding legal and financial decisions on his or her behalf. The basic principles for the PoA are provided in the Indian Contract Act, 1872. There are two types of PoA, namely general and special (limited). Special PoA gets terminated as and when the limited task assigned has been accomplished. In India, in regions where the Registration Act, 1908, is enforced, the PoA should be authenticated by a sub-registrar, and in other areas, attestation should be done by a notary. Advance Directive (AD): As per the Mental Health Care Act (MHCA), 2017, AD is a document written by the individual about how he wishes to be treated and how he wishes not to be treated if he/she loses the capacity to make treatment decisions. While PoA is a document for legal and financial binding decisions, AD under MHCA, 2017, is for admission and treatment of mental illnesses. AD must be signed in the presence of two witnesses, countersigned by the nominated representative, and after that should be registered with the Mental Health Review Board as per the MHCA, 2017. Limited guardianship: It is under section 14 of the Rights of Person with Disability Act, 2016.
Guardianship
A guardian can offer various supports for a person with incapacity. It includes managing assets, bank accounts, treatment procedures, consent for research, residential care, and maintenance due to his/her physical or mental health issues. The ratification United Nations Convention on Rights of Persons with Disability (UNCRPD) in 2007 had a large bearing on the spirit of guardianship in India. The Acts that came before the ratification of UNCRPD, like the National Trust Act (NTA) and the Person with Disability Act, 1995, had approached the concept of guardianship as a substituted decision-making reflecting paternalistic attitude. However, post ratification of UNCRPD, guardianship is viewed as supported decision-making, thereby upholding individual autonomy as evident in the Rights of Persons with Disability Act, 2016 (RPWDA).
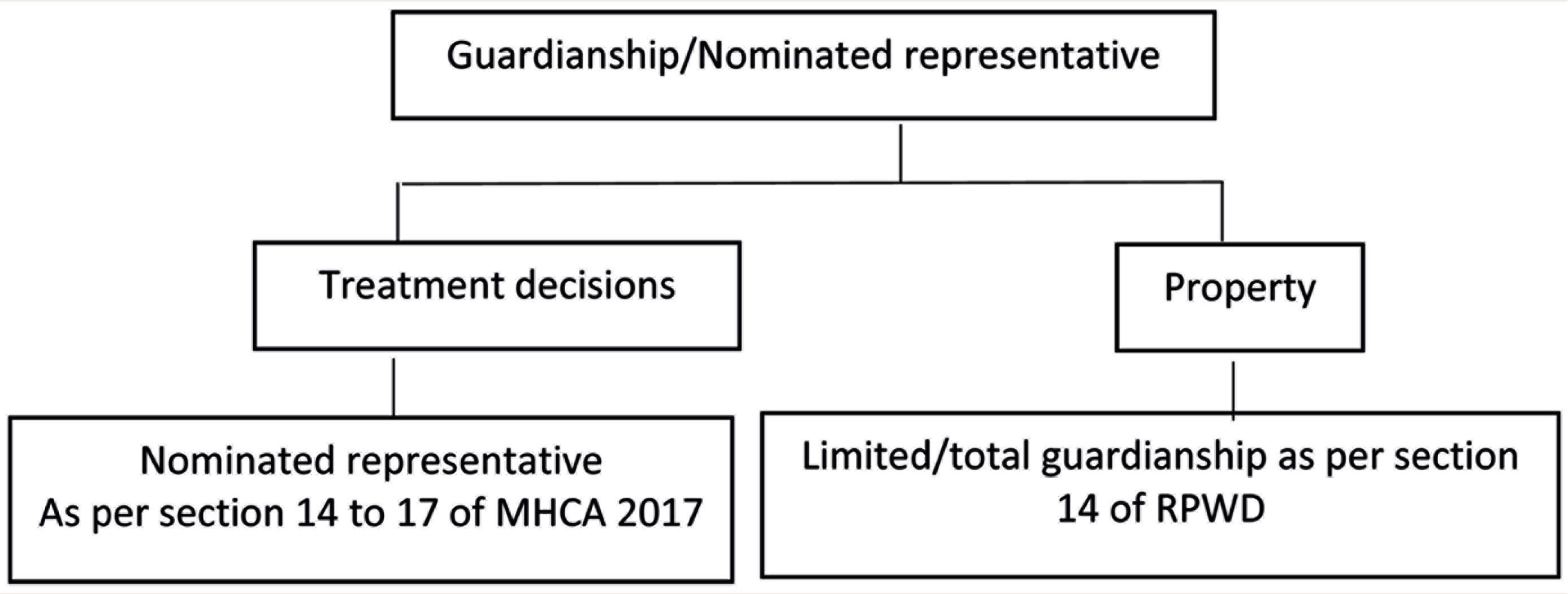
Guardianship Under Various Acts
Figure 1 describes the provisions for guardianship under various acts. Guardianship under RPWDA, 2016 [Section 14], is provided when a person with a disability (PWD) cannot make a legally binding decision despite being provided adequate and appropriate support. This is applicable for 21 different types of disabilities alike, such as long-term sensory impairments, chronic neurological conditions, mental illnesses, intellectual disability, locomotor disability, multiple disabilities, and so on. The RPWDA, 2016, has introduced the concept of limited guardianship. Limited guardianship is the guardianship provided for a specific situation and decision for a specific period and is a joint decision of the legal guardian and the PWD. 10 The decision made by the representative should be in the best interest of the individual who has lost the capacity. In situations where conflict arises between the guardian and the PWD, the PWD has the right to change his guardian. The guardianship under the Mental Health Care Act, 2017 (MHCA), is provided in a nominated representative under Chapter 4 of the Act. 11 It reflects a combination of best interests and a supported decision model for treatment-related indications. A psychiatrist might be requested to assess an individual’s capacity and accordingly opine if there is a need for the appointment of a guardian.
Testamentary Capacity
The capacity of an individual to make a Will is called testamentary capacity. The guiding principles for capacity assessment are derived from a popular case of Banks v. Goodfellow. 12
Provision of Guardianship Under Various Acts
The Banks v. Goodfellow criteria:
Understanding the nature of the act and its effects, Knowledge of the nature and extent of one’s assets, Knowledge of persons who have a reasonable claim to be beneficiaries, Understanding of the impact of the distribution of the assets of the estate, A confirmation that the testator is free of any delusion that influences that disposition of the assets; and Ability to express wishes clearly and consistently in an orderly plan of dispositions.
Role of a Psychiatrist
The goal of assessment is to check if the six points mentioned above are getting fulfilled. The mere presence of psychiatric illness does not make a person incapable of executing a valid will.
Process of assessing testamentary capacity 12 : The psychiatrist should get a letter from the solicitor detailing the legal tests. A thorough physical, neurological, and psychiatric examination should be done, and all the responses should be recorded verbatim. Facts such as the extent of assets, potential beneficiaries, previous Will should be explored as per the Banks v. Goodfellow criteria.
A detailed evaluation by the psychiatrist: A detailed evaluation for the cognitive and physical impairment must be done. Cognitive impairments like difficulties in attention and information processing, language difficulties, and memory impairment can affect testamentary capacity. It commonly occurs in cases of advanced dementia, mood disorders, delusions of persecution or poverty, and when under the undue influence of others or substances. Physical impairment like hearing difficulty, impairment in language, speech, and difficulty in execution needs assessment.
Screening tools to assess cognitive impairment: The Mini-mental Status Examination and the Draw a Clock test are the commonly used screening tests for cognitive functioning. 13
Reporting: Based on the detailed evaluation, the psychiatrist should opine if the individual can execute a valid will. If the capacity is present, advise the individual to execute the will within the next seven days and re-evaluate capacity within seven days of executing the will. This way, one can reduce the chances of future litigations.
Banking Facilities for the Senior Citizens and Persons With Disability
Aging produces various physical, mental, and psychosocial adversities that also hamper a person’s financial autonomy. The Reserve Bank of India in 2017 provided guidelines for the provisions of various facilities for the senior citizens and PWD accounting for their unique needs.
14
These facilities have been enumerated below:
There should be identifiable dedicated counters at the bank. There should not be undue delay in credit of pension. Banks should not insist on the physical presence of the account holder to issue checkbooks. A fully Know Your Customer (KYC) compliant account should be automatically converted into a “Senior Citizen Account” based on the available date of birth. Doorstep banking facility for senior citizens more than 70 years of age and PWD such as pick up of cash and instruments against receipt, delivery of cash against withdrawal from the account, delivery of demand drafts, submission of the KYC documents and Life Certificate at the residence of such customers.
As mental health professionals, it would be vital to educate the elder about these provisions as a part of their psychosocial rehabilitation. Joint ownership of bank account between elderly and caregiver can be considered with standing instructions on operating it.
Right to Legal Aid
The elderly are vulnerable to getting their rights violated because of various factors such as physical illnesses, financial constraints, poor social support, physical abuse, and emotional abuse, thereby leading to the development of multiple mental health issues. Article 21 of the Indian Constitution gives the right to life and liberty, including living with dignity. Furthermore, article 41 and article 46 mandates state to ensure that senior citizens lead their life with dignity and are protected from social injustice and exploitation. 15 In line with the above-mentioned constitutional provisions, the Legal Services Authority Act was framed in 1987. Under which a senior citizen is entitled to free legal aid (in case of civil or criminal litigation) if his annual income is less than the ceiling limit of the prescribed rules of the respective state government as per section 12 of this act.
Legal Services to Senior Citizens Scheme 2016 16
The objective under this scheme include creating awareness about the rights of senior citizens, improving the legal aid and representation at different levels, promoting the establishment of authorities and institutions under the Maintenance and Welfare of Parents and Senior Citizens Act (MWPSCA) 2007, promoting the establishment of old age homes and their supervision, etc. State legal services authorities (SLSAs) are mandated to conduct regular visits to old age homes to ensure adequate facilities. The senior citizens boarding at the old age homes are treated with dignity. In the premises of every tribunal and appellate tribunal and old age homes, there should be a legal service clinic that SLSAs will establish. Any senior citizen seeking legal aid can approach these legal services clinics. 15
Gift Deeds
An interesting provision under the MWPSCA is regarding gift deeds [Section 23]. 17 It describes certain instances where the transfer of property is considered void. It broadly includes circumstances when the transferee fails to provide the basic amenities and basic physical needs to the transferor, in which case the transfer of property is considered through fraudulent means and coercive and deemed void. This was also held in Karnataka High Court in the writ petition. WP(C) No. 8193/2014.
Elderly and Voting
Voting rights are given by the constitution of India to every citizen of India. As per section 16, Representation of the Peoples Act 1950, any person with unsoundness of mind is disqualified from registering in the electoral roll. The common illnesses in the elderly which can lead to unsoundness of mind include dementia and delirium. The exact prevalence rates of these illnesses vary from place to place. Indian studies have reported the prevalence of dementia in people aged more than 65 as 2.5% and delirium in medical wards as 11%–40%.18,19
As per the Election Commission of India, there were about 10 crore people aged more than 65 years in the year 2014. 20 Considering the prevalence of dementia to be around 2.5%, around 25 lakh people are suffering from dementia, and we don’t know if they can cast their votes. The research in this area is sparse. There are few studies from developed countries in this regard but none from India.21,22 There is a structured assessment tool, the Competence Assessment Tool for voting (CAT-V), to determine the capacity to vote; but using it to assess the voting capacity of all the elderly in India is impractical.
Persons with dementia require some level of assistance in casting their vote (deciding which candidate to vote for), which the spouse or other caregivers generally do. While doing so, there is always a chance that the person who is assisting might influence the voter’s decision. On the flip side, disqualifying all people with dementia from voting can lead to deprivation of their rights and a sense of lowered self-esteem. Another issue of the elderly is accessing the voting polls; they might not be physically fit and might not be having the caregiver assistance to reach voting polls. There are no provisions made in the electoral process, such as postal vote or assistance by the electoral commission in setting up a ballot near old age homes, age-sensitive ballots, etc. 23
Driving License and Geriatric Population
The ability to drive is a part of one’s identity and helps an individual to meet his needs and connect socially. However, with aging, health issues emerge (decline in vision, reflex, hearing, and cognition), which might hamper their driving skills, making them vulnerable to encountering road-traffic accidents (RTA). Despite the increased vulnerability, the elderly drivers experience fewer accidents than their younger counterparts, as they tend to obey traffic rules and drive slower, taking more precautions. 24 But elders are more likely to die from the injuries of the accidents than the younger drivers. 25 As per data released by the Ministry of Road Transport and Highways, 4.35% and 3.59% of the deaths in drivers in RTA were elders of age > 60 in the year 2016 and 2019, respectively.26,27
In India, Motor Vehicles Act, 1988, section 9 deals with the grant of driving license, and section 15 deals with renewal of driving license. The initial license given by the Transport Authority is valid up to the age of 50 years; after that, the renewal must be done every five years. There is no upper limit on the applicant’s age for renewal. Still, hearing, eyesight, and health must be certified by a medical officer after the attainment of the age of 40 years. 28
Dementia needs special emphasis while discussing elderly driving, as it causes a decline in cognitive functioning, which declines the ability to drive safely and its awareness. Drivers having Alzheimer’s disease are at an increased risk of involvement in an RTA by two to five times. 29 This is probably due to the fact that, unlike patients with visual or motor impairments who are aware of their declining abilities, dementia patients may lack awareness and drive even when it might not be safe for them. 30 Therefore, it becomes important to assess patients with dementia for their ability to drive safely in mild cognitive decline. Those with moderate to severe dementia might need to avoid driving when it poses a high risk causing harm to themselves and others.
In India, no law mandates the psychiatrist or physician to identity drivers with physical or mental impairment during routine clinical duty. Comparing it with other countries, like many states in the United States, it is mandatory to report if a physician has reasons to believe that their patient has an impairment that might affect his/her driving. 31 Failure to report may lead to physician liability if the patient is involved in an RTA. There is a downside to mandatory reporting as it involves a breach of confidentiality, and there can be honest disagreement about the degree of risk. However, it’s also important for the psychiatrists and physicians to be involved in voluntary reporting as it involves public safety, especially if the risk is marked and outweigh the consequence of reporting on patient care.
Organ Donation and Elderly
There exists a major disparity in the supply and demand in the field of organ donation and transplantation. Many countries have made it easier for elders to participate in organ donation. Despite variable outcomes with the use of elderly donors because of age-related decline in the function of the organs and increased comorbidities, the guidelines encourage routine use of elderly donors to meet the increasing demand. 32 With this, the average age of donors in kidney and liver transplants, most commonly transplanted organs, has increased over the years. As per World Health Organization, India ranks third globally with 12,660 organs being transplanted in 2019. 33 In India, the Transplantation of Human Organs (THO) Act, 1994, further amended in 2011, deals with organ transplantation. The THO Act permits transplantation between near relatives such as parents, siblings, and children. New rules made in 2014 under the THO Act have added grandparents as near relatives. 34
Many western countries follow presumed consent, as per which every person is supposed to have agreed to organ donation at the time of birth unless he/she opts out of the system. In India, we require consent for cadaveric transplant, which requires a person to pledge their organ donation. Only then will the deceased person’s family be approached after their death for organ donation. 35 Similarly, for living donors, it is essential to have an application to grant approval by both the donor and recipient jointly. The THO Act allows for living organ donation from a near relative after approval by the competent authority. Whenever the donor is not a near relative, the authorization committee of the hospital can look if any undue monetary considerations are involved. 36 However, there exists a possibility of the elderly agreeing because of “undue influence.” Undue influence occurs in a continuum, and it is often difficult to assess. A sense of guilt, emotional pressure from family members, may influence the elder’s decision to donate. So, it becomes important for psychiatrists to assess the voluntariness and advocate for them. Additionally, the physician’s role is to ensure that the consent to living donation is morally robust and that the individual can make this decision. Capacity assessment here would be done on similar grounds as discussed earlier in the section on decision-making capacity.
Conclusion
Mental illness in the elderly may lead to diminished capacity, which limits their participation in civil duties and makes them vulnerable to abuse. A clinician does the capacity assessment, and it is task and time-specific. It has to be differentiated from incompetence, which is decided by the judiciary and invalidates all further legal proceedings by that person. Also important is the risk of coercion and abuse, interfering with the elder’s right to vote, banking, organ donation, and even neglect after a property transfer. There are provisions to overcome it through legislatures such as free legal aid clinic in section 27 of MHCA, Legal services to Senior Citizens Scheme 2016, and provisions to revoke property transfer in MWPSCA. Despite having various systems in place, we still grapple with challenges, including poor legal literacy and problems translating awareness into assistance. Improving legal literacy among various stakeholders like health professionals, the elderly, and their family members might be an important step toward tackling this issue.
Footnotes
Declaration of Conflicting Interests
This article being submitted has not been published, simultaneously submitted, or already accepted for publication elsewhere. The manuscript does not infringe upon any copyright or property right of any third party, to the best of the author’s knowledge.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.