
Abstract
Elderly persons can get involved in the criminal justice system as victims or as perpetrators. The interaction of elderly persons with mental illness at various cross-sections of the judicial process needs thoughtful consideration. Through this review, the authors approach this less studied aspect of forensic psychiatry. Concerning the evaluation of a prisoner, three scenarios need focused consideration: evaluation for fitness to stand trial before a competent court, evaluations for an insanity defense, and fitness for sentencing. At the same time, incarcerated elderly who developed dementia or a severe mental illness at any point of time during the trial or in prison need specific approaches. In this article, the authors discuss the acts and case laws relevant to navigating these legal scenarios. We discuss existing mental health care provisions for protecting the health interests of elderly care in prison.
“During an NHRC inspection of undertrials in March 2005, a rapporteur stumbles upon a frail man who hasn’t spoken to anyone in decades quietly tending to the hospital garden. As it turns out, this man doesn’t remember why he was booked in the first place. The hospital authorities report that he was sent to the hospital to treat mental illness within weeks of arrest and was deemed fit to stand trial in 1967 itself. Still, the jail authorities didn’t pay heed, nor the trial court enquired about this man despite repeated reminders from the hospital. Originally arrested at the age of 23 years, on charges of voluntarily causing grievous hurt, which has a maximum sentence of ten years, this man, had served 54 years in custody.” This is the story of Machal Lalung, a legend back home whose family believed he was sacrificed in ritual for an under-construction bridge.
And this is not the only such case, the Supreme Court of India, taking notice from a news article published in the Indian Express in 2005, directed principal secretaries of all the prisons of the country for due compliance of section 330 of the Criminal Procedure Code, 1973 and section 30 of the Prisoners Act, 1900. Machal Lalung was released at the age of 77, with a compensation of 3 lakhs, only to die three years later of multiple physical ailments resulting from a long life in custody. 1
Criminal Responsibility
Criminal responsibility is a legal construct with two essential elements, both of which should be present for a person to be held responsible for an alleged criminal act
2
:
An actus reus (Latin for “guilty act”) A mens rea (Latin for “guilty mind”)
Actus reus refers to the specific voluntary criminal act. In contrast, mens rea refers to the level of intent necessary to commit the criminal act.
Before criminal responsibility arises, the law gives due consideration to whether a person is fit for participating in the judicial process. After the question of criminal responsibility is resolved, further judicial proceedings can get mediated at any stage by a question of the presence of mental illness.
Geriatric Population in Conflict with the Law
India’s elderly population is expected to increase threefold from 104 million in 2011 to nearly 300 million in 2050 (India Ageing Report, 2017). 3 According to the Prison Statistics India 2019 4 reports, 63,336 prisoners (13.2% of the total prison population) are above 50 years of age. An overall increase in the proportion of elderly among the general population, the trend toward stricter sentences, and the number of elderly being detained outnumbering releases have led to increased numbers of elderly persons in the prison system.4,5
Elderly persons frequently get involved in the criminal justice system as victims. Less commonly so they may come in conflict with the law as perpetrators. Once into the judicial system, the elderly with dementia may be an easy target for abuse by their peers in prison. The status quo in prisons may not be enough for the care and protection of these aging persons. Human rights and federal law find each other at crossroads in such situations. When psychiatrists are called upon to assess these elderlies, they must consider the geriatric population’s specific vulnerabilities when evaluating their fitness to stand trial or culpability. The elderly people with dementia exposed to the judicial system pose considerable challenges in respect to their placement. Dedicated forensic wards are scarce in our country 6 (in only a few tertiary settings such as NIMHANS, Bengaluru), and mental health establishments may not have adequate treatment facilities to cater to their comorbid medical illnesses. The community may be reluctant to place them in old age homes due to safety and risk considerations. 7 At the same time, prisons in their current format are not adequately equipped to care for elderly prisoners, especially those with complicated medical comorbidities, which are not rare in this population. 8
Mental health professionals offering care to elderly prisoners in the criminal justice system encounter apparent conflicts between the treatment interests of the elderly, the broader interests of these individuals, the legal rights of the individual, and the public interest. 9 Unfortunately, sparse published research is available regarding criminal behavior in elderly persons and the elderly in correctional settings from India. Western studies looking at elderly in prison7,10 report that elderly who come in conflict with the law are more often “uneducated, unemployed men with significant legal and psychiatric histories, including high rates of substance abuse (particularly alcohol abuse and dependence), recidivism, and multiple comorbidities.”
Problematic Behaviors in the Elderly
Certain problematic behaviors in the elderly may bring them in conflict with the law:
Disinhibitory behaviors are common in the elderly (included under the umbrella term of Behavioral and Psychological Symptoms in Dementia). These are often associated with frontotemporal dementia, Alzheimer’s disease and other neurocognitive disorders of diverse etiology. Neurocognitive disorders and substance use are the most common diagnosis bringing the elderly in conflict with the law.
10
Disinhibition may also be due to mental illnesses unrelated to aging, like mania, psychosis, delirium, substance intoxication, or medication side effect. These may result in theft, shoplifting, disrobing or urinating/defecating in public spaces, profanities or discussing inappropriate subjects in front of children, violation of social norms, including but not limited to problematic sexual behaviors. Paranoid ideations in the background of psychosis, delirium, and dementia may cause the elderly to become suspicious or fearful of the caregivers or neighbors and potentially result in violence and even murder in extreme cases. Agitation resulting from the psychiatric illness coupled with disinhibition may lead to poor anger control making the elderly more susceptible to act out on such aggressive impulses.
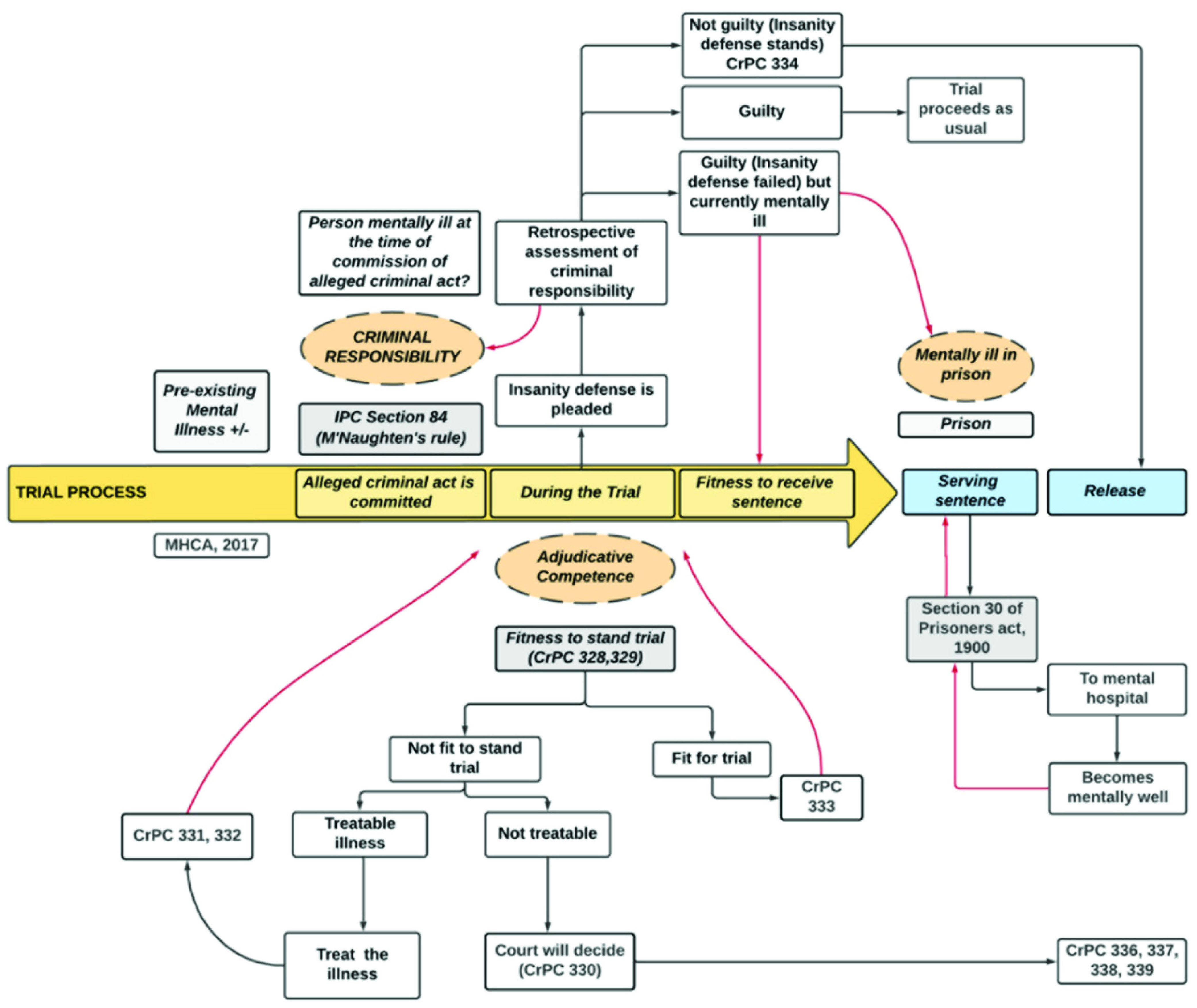
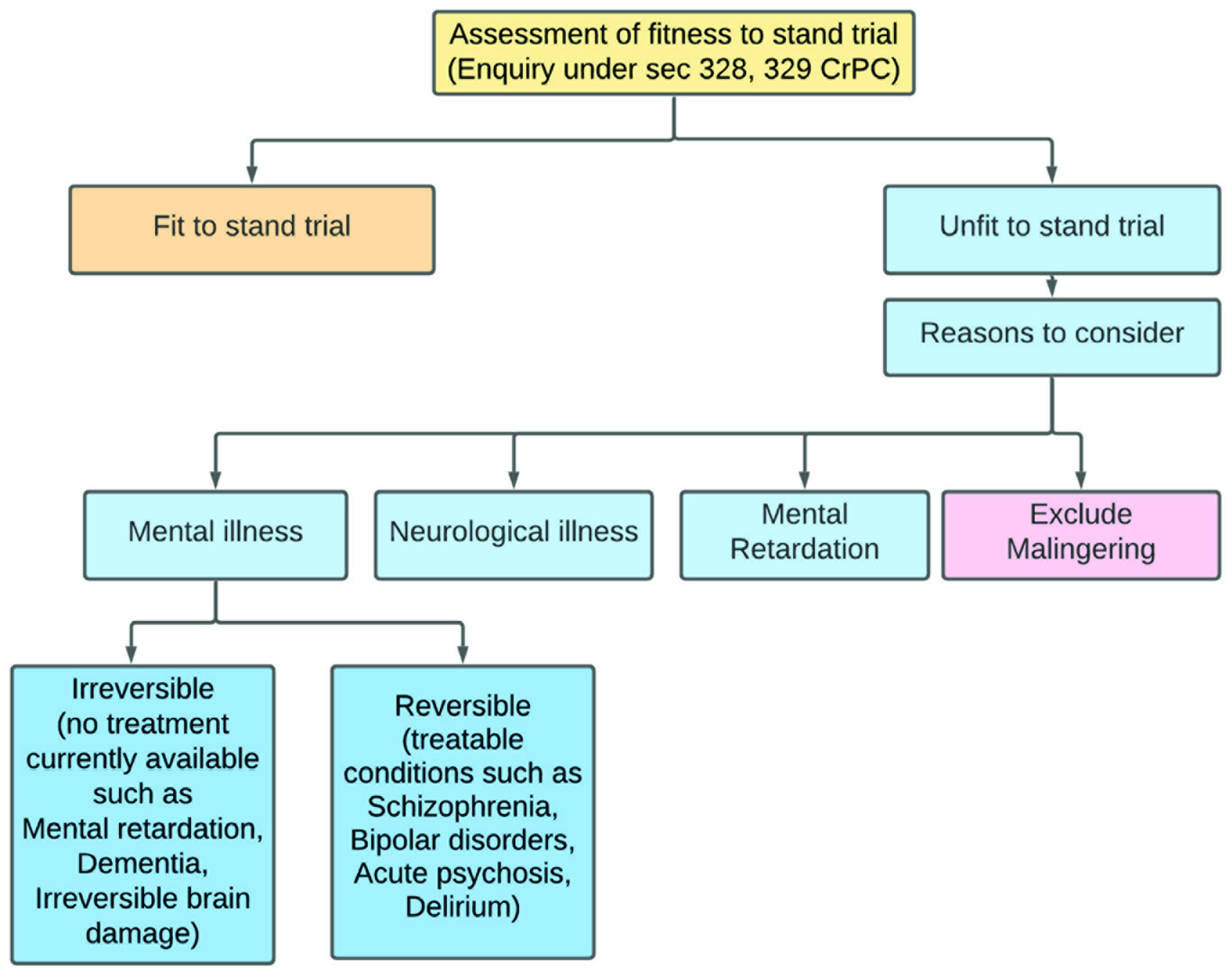
It is often difficult to ascertain the temporal relation of psychiatric illness with the alleged crime at various stages of the judicial process. However, careful consideration of circumstantial evidence and detailed forensic psychiatric assessment aids in arriving at a consensus. Table 1 and the flowchart in Figure 1 give the interaction between legal proceedings and mental illness at various cross-sections navigated by an elderly in conflict with the law.
Events and Cross-section with the Law
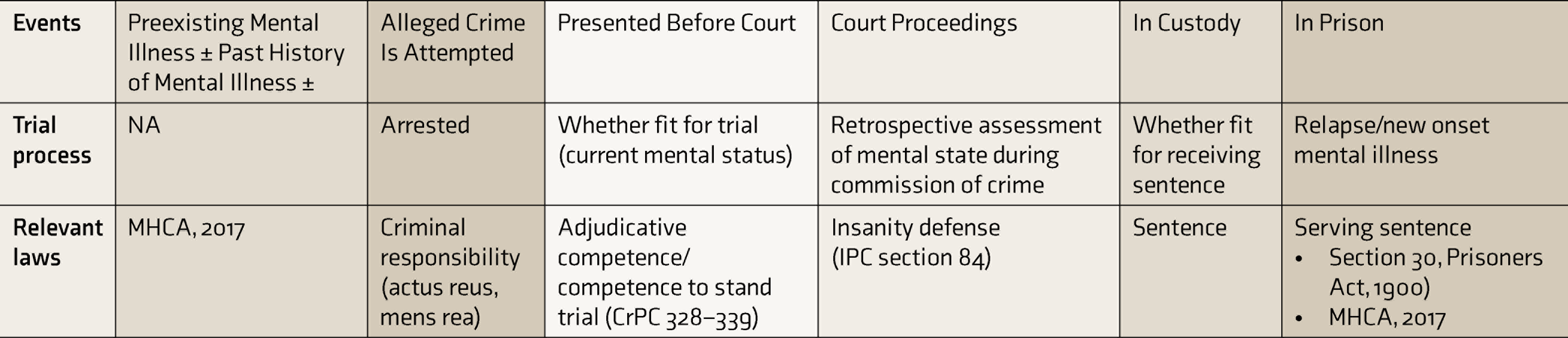
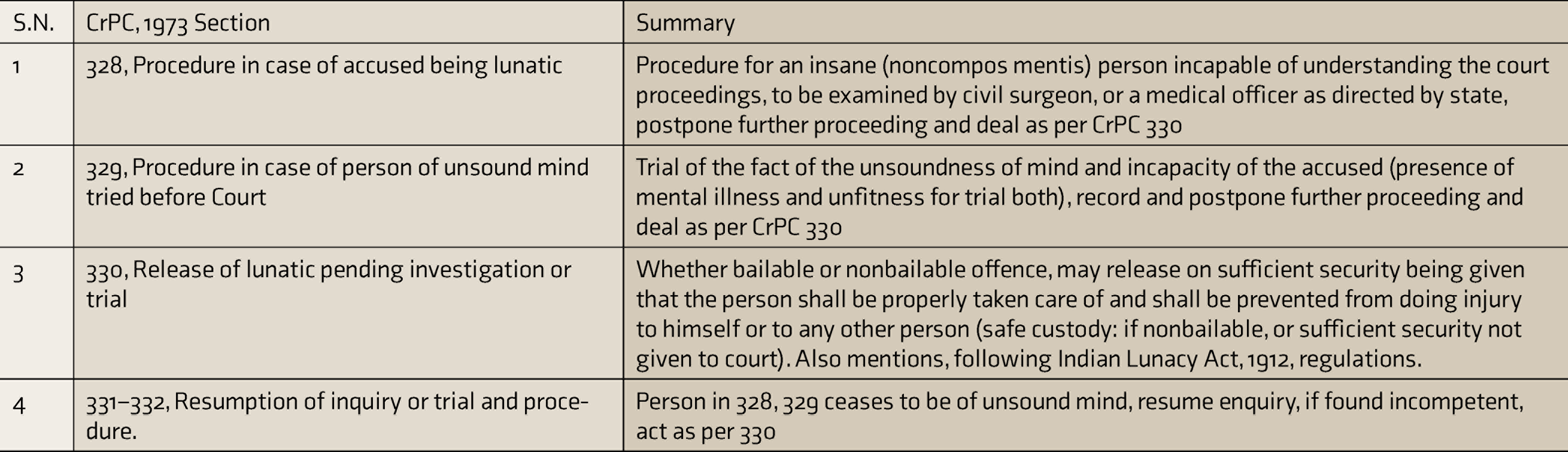
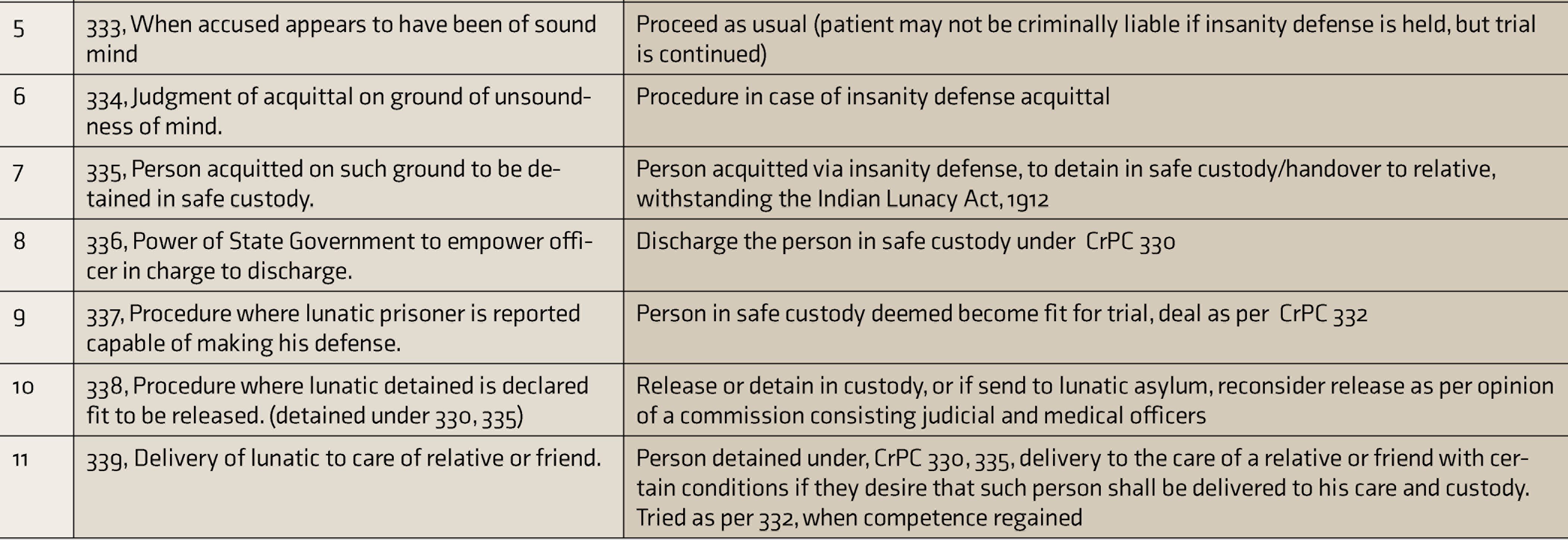
MHCA, 2017: Mental Health Care Act, 2017, CrPC: Criminal Procedure Code, 1973 section (see
Summary of CrPC Sections Relevant to Fitness to Stand Trial and Insanity Defense
Fitness to Stand Trial
An elderly approached by police officers as a possible criminal suspect has to navigate various legal tasks throughout the trial process that will impact the rest of his life. These tasks range in complexity, requiring different abilities depending on the legal scenarios being faced by the elderly. This involves assessing for adjudicative competence, that is, fitness to stand trial or competence to stand trial (we have used these terms interchangeably in the following text).
The concept of competence refers to a person’s cross-sectional (time-specific) ability to make decisions relevant to a particular task or issue. In contrast to the criminal responsibility evaluations (which rely on retrospective analysis of a defendant’s mental state at the time of committing the crime and is thus, static), fitness to stand trial evaluations’ focusses on the person’s present ability to defend themselves. Hence, this mental state may change over time and be considered dynamic.
In the eyes of the law, a person is presumed fit/competent to stand trial unless proven otherwise. However, the defense, prosecution, or the judge can request an evaluation of a defendant’s competence at any point before or during the trial (section 328–329 of the Criminal Procedure Code (CrPC), 1973). 11 A judge, or sometimes a jury, finally determines a defendant’s competence or fitness to stand trial. Here, the burden of proof of incompetence to stand trial lies with the defendant as per the preponderance of evidence standard. The preponderance of evidence standard requires a level of proof which is more likely than not, that is, more than 50% chance. If found incompetent to stand trial, the trial is usually postponed until competency restoration. 12
Melton et al.
13
have outlined the essential components based on the US Supreme court’s Dusky Competence to Stand Trial standard.
14
As per Melton’s proposition, the adjudicative competence has two essential prongs:
The defendant’s rational and factual understanding of the criminal justice process. The defendant’s current ability to assist his or her lawyer in the defendant’s defense.
Source. Adapted from Math et al., 2011, with permission.
In addition to the Dusky standard, Math et al.
15
have reviewed multiple other international guidelines and Indian case laws relating to competence to stand trial and outlined five basic requirements for considering a person fit for trial. If any one of these is absent, the person may be deemed unfit for trial:
Comprehending the charges framed against them Realizing the seriousness of the penalties if proven guilty Following the proceedings of the court Helping their lawyer to defend their case Appropriate behavior in the court (Readers are advised to read the article on fitness to stand trial
15
for a comprehensive review of the topic)
In the elderly, neurocognitive disorders, both major and mild, can alter the elderly’s abilities needed for decision-making in terms of competence and consent due to the impairments of attention, memory, executive function, and abstract thinking. Unlike persons with severe forms of dementia, milder neurocognitive problems may go unnoticed during the judicial process. However, they can still be susceptible to dysfunction due to poor executive function, social cognition, and judgment, thus necessitating assessment for competence. 16
Assessment of Fitness to Stand Trial
The level of competence required for a task is valued in proportion to its consequences. For fitness to stand trial, the defendant is expected to have a reasonable degree of understanding, not an absolute or perfect competence. In one of the past studies, most defendants found unfit to stand trial had some form of psychosis, but almost one-thirds of those found competent to stand trial were also found to suffer from psychosis. 7 Thus, mental illness is an important factor in determining a person’s trial competence, yet it is not the sole criteria. The psychiatrist must demonstrate and record the mental illness to be causing a defect of reasoning to render the defendant incompetent to stand trial. In the Delhi High Court case, taufiq vs. state 17 judgment, the court held that though the person (accused of rape) was suffering from Bipolar affective disorder, currently hypomanic, but he was able to comprehend the charges and circumstances as per the opinion of the medical board and hence deemed fit for trial.
In Geeg Singh vs. The State of Raj, 18 Mr. Geeg Singh was charged with murder and sentenced to life imprisonment by the trial court. During appeal proceedings in the high court, he was found unfit for trial due to schizophrenia, and hence treatment was initiated in a mental hospital as per CrPC 329. Upon regaining competence (while still suffering from schizophrenia), he was tried as per section 332 of the CrPC. Since the circumstantial evidence pointed toward the accused’s unsoundness of mind at the time of the commission of the alleged murder, he was acquitted under IPC 84 via CrPC 334. The court further advised releasing the appellant in the custody of a relative if he is medically fit or retain in prison or mental hospital as deemed fit by the state.
Defendants cannot be involuntarily hospitalized lifelong to restore competence to stand trial alone. The US supreme court verdict in Jackson vs. Indiana, 1972 19 states that they should not be held for more than the reasonable period necessary to determine whether the person will regain competence to stand trial in the foreseeable future. However, when mentally ill patients are sent to prison for safe custody, the outcomes of such cases are poorly monitored, and there are numerous instances where the mentally ill prisoners outstay their sentences or are entirely forgotten. The case of Machal Lalung vs. Union of India, 20 mentioned in the introduction, is a testimony where neither the trial courts considered whether this undertrial prisoner could be released nor his friend or relative came forward with sufficient security and sought release under the said provision.
When a person is being evaluated for fitness to stand trial, the evaluator should know the charges faced by the defendant, the police information report, the statements of any witness of the alleged offense. This information is helpful in the assessment of the defendant’s understanding of the legal process. It also provides clues to the individual’s mental state, and its plausible relationship to trial incompetence, if any. In addition to this information, prior psychiatric records, prior criminal records, jail treatment records, medical records, educational records may be helpful to establish the context further. Along with reviewing these records, the evaluator should enquire about any difficulties that the defendant’s lawyer noted in the client’s ability to assist them.
An impairment of a person’s comprehension, appreciation, reasoning, and communication can result from various psychiatric illnesses rendering a person unfit for trial. Cognitive impairment, especially dementia and delirium in the elderly and various psychoses, are the most common diagnoses associated with incompetence to stand trial. 7 However, mere amnesia for the criminal act (which may result from an underlying organic cause, for example, dementia) does not necessarily mean the person is unfit for trial.
The Wilson factors
21
for evaluating the impact of amnesia on fitness to stand trial take the following into account:
The effect of amnesia on the abilities of the defendant to consult/assist their lawyer Their ability to testify How well the evidence could be externally reconstructed The possibility that if not for the amnesia, the accused could have established an alibi or defense Other facts indicative of a fair trial
As in all criminal cases, malingering has to be ruled out. A refusal to participate in competence assessment alone does not indicate trial incompetence, which can come off as an easy way to delay prosecution. Objective causal evidence should be sought to relate or rule out noncooperation with a mental illness. Similarly, a person providing inadequate answers about the legal process due to a lack of knowledge about the criminal justice system does not equate with adjudicative incompetence. The evaluator is expected to invariably educate the defendant and later ascertain whether the defendant can learn and retain the information long enough to decide.
Various tools help to do a structured assessment of the competence to stand trial. However, these tools are not validated for the Indian legal system. None are considered the gold standard but can provide good anchor points for final decision-making while assessing trial competence. Some of these tools are as follows:
Competence Assessment for Standing Trial for Defendants with Mental Retardation.
22
Georgia Court Competency Test: Screening instrument includes a picture of courtroom layout.
23
MacArthur Competence Assessment Tool—Criminal Adjudication: Semistructured interview format with 22 items utilizes a hypothetical vignette to assess a defendant’s psycholegal abilities.
24
Evaluation of Competency to Stand Trial—Revised.
25
Methods to Restore Competence
Attempts to restore competence involve the following interventions:
Use of medication or pharmacotherapy. This may be voluntary or involuntary. The Sell criteria (Sell vs. the United States 2003) outline conditions where involuntary treatment can be permitted. The court must find the involuntary medication to significantly help the person regain competence, be the least intrusive measure, and have demonstrated efficacy for the particular ailment. 26 Upon treatment and regaining the competence for trial, the patient may refuse the involuntary treatment. However, it can be further continued given the fulfillment of Sell’s criteria and the necessity of medication for the patient’s safety or others.
Psychosocial interventions. In the form of educational modules and programs used in the competence-restoration curriculum and educating patients about their rights in a correctional setting.
Legal counseling. In the form of educating the defendant regarding the legal proceedings, pleas, charges, sentencing, and how to assist their lawyer in planning the defense using a variety of individual or group activities, for example, role plays of courtroom procedures.
Insanity Defense and the Elderly
As mentioned earlier, a variety of problematic behaviors in the elderly may lead to legal conflicts. However, the law does not punish a person who is non compos mentis (not of sound mind) at the time of commitment of a criminal act. Insanity is a legal rather than a psychiatric term. IPC 84 in India defines legal insanity and is essentially an adaptation of the M’Naghten standard, that is, “To establish a defense on the ground of insanity, it must be proved that at the time of the committing of the act, the party accused was laboring under such a defect of reason, from the disease of the mind, as not to know the nature and quality of the act he was doing, or if he did know it, that he did not know that it was wrong.” 27
Legal insanity revolves around knowledge of the act’s consequences and awareness of wrong or unlawful acts. This includes the comprehension of the act, the possible consequences of the act, and the awareness that it is unlawful or wrong. Not all mental illnesses cause such a loss of reasoning.
As per section 334 of the CrPC, 28 the time at which legal intensity is to be proved is the time of attempting the unlawful act, also reiterated in the Dahyabhai Chhaganbhai Thakker vs. State of Gujarat case. 29 So the state of mind during the commission of the crime is considered static and hence assessed retrospectively. If the defense is established on the ground of insanity, further course of action will be determined based on section 335 of the CrPC, 1973, which says a person can be put to safe custody or delivered under the care of a relative or friend.
Even when known to cause a defect of the reason, the mere presence of a psychiatric illness is not enough for the insanity defense. Various circumstantial evidence is needed to prove that as a result of the psychiatric illness, at the time of committing the crime, the person had such an unsound mind as not to know the nature of his act or its reasonable consequences. In Hari Singh Gond vs. State of Madhya Pradesh, 30 the supreme court of India held that the accused assaulted the victim and had later run away. Even when his behavior appeared unusual and no motive for such behavior was evident, mere mental illness was not held as a ground for an insanity defense, and a bail plea was refused.
The elderly, especially those with severe dementia, psychosis, delirium, or mental retardation, will need be carefully evaluated to assess to what extent their mental condition influenced reasoning and behavior. 31 As for the fitness to stand trial, amnesia for the alleged crime is usually not considered a defense of insanity. 32 In the Bapu alias Gajraj Singh vs. State of Rajasthan, 33 the Supreme Court of India has detailed the insanity defense rationale. If not shown as related to the defect of reason at the time of the commission of a crime, the existence of a preexisting mental illness cannot be ground for the insanity defense.
Assessment of Criminal Responsibility
Assessment of criminal responsibility involves an in-depth understanding of psychiatric diagnoses and how a diagnosis may diminish a person’s criminal culpability. With the increasing numbers of individuals with mental illness entering the criminal justice system, mental health professionals play an increasingly prominent role in assessing criminal responsibility, diminished capacity, and appropriateness for diversion of offenders from punishment to community treatment.
The psychiatrist should consider admitting the defendant for a global evaluation of the accused. The psychiatrist has to educate the court, clarify psychiatric problems and provide an objective opinion based on factual data and sound reasoning. NIMHANS Detailed Workup Pro forma for Forensic Psychiatry Patients 34 can be used for semistructured assessment of forensic psychiatric cases. This pro forma is modified periodically as per the clinical evaluation and legal requirements. The review article, Insanity defense: Past, present, and future by Math et al., 2 comprehensively covers the assessment of criminal responsibility. Readers are requested to go through the article for further reading.
Fitness for Receiving the Sentence
A person who has committed a crime and developed dementia or delirium at some stage during legal proceedings (which sometimes may take years) may be referred for fitness to stand trial evaluation. Circumstantial evidence may indicate the person was of sound mind when attempting the crime (the time frame relevant to insanity defense) but is not so at the time of presentation in court. Such persons are termed as guilty but mentally ill/ postconviction mentally ill and maybe deemed unfit for standing a trial or receiving a sentence as the case may be.
It is of no use to execute a convict if he cannot understand the purpose of his death sentences at the time of sentencing. A person’s inability to take part in the sentencing process defeats the very reason for granting a deterrent punishment. In 2019, the Supreme court of India in the Accused X vs. the State of Maharashtra 35 case had laid the grounds for considering postconviction mental illness as a mitigating factor during sentencing. The supreme court considered “the aspect of postconviction mental illness as mitigating factor in the analysis of ‘rarest of the rare’ doctrine and had stated, Article 20 (1) 36 of the Indian Constitution imbibes the idea communication/knowledge for the accused about the crime and its punishment. This communicative element is ingrained in the sentence (death penalty), which gives meaning to the punishments in a criminal proceeding. The death sentence and the ensuing sufferance cause incapacitation and is idealized to invoke a sense of deterrence. Suppose the accused cannot understand the impact and purpose of his execution because of his disability. In that case, the raison d’être for the execution itself collapses. The supreme court, in this case, allowed the sentence of death awarded to the petitioner to be commuted to imprisonment for the remainder of his life sans any right to remission and offer appropriate mental health care as per the MHCA 2017” (verbatim from the Supreme court Judgment transcript).
Providing Care to the Elderly in Correctional Settings
Prisoners are more vulnerable to mental illness because of overcrowding, enforced solitary confinements, a lack of privacy, lack of engagement in meaningful activity, insecure prospects, and poor health services. Research on prisoners uniformly indicates that the stress of incarceration increases the incidence of mental illness in the country. 5 The recent case of Mr. Varavara Rao, 37 an 81-year-old poet accused of being part of the Elgar Parishad—Maoist link case, has reignited the often-overlooked concerns of cognitive dysfunction in a correctional facility. Mr Rao, during his stay at the prison, had developed delirium as a result of electrolyte imbalance and hemodynamic instability along with multiple other ailments. The lack of the current prison infrastructure to cater to the need of such individuals further came to light when Mr Rao later slipped and fell from his bed and sustained injuries on the forehead that required stitching. As a result of the complete absence of any qualified health care staff at the central prison hospital, Mr Rao moved back and forth from the prison hospital, tertiary care government hospitals, and superspecialty hospitals over the subsequent six months. After much debate and National Human Rights Commission’s involvement, the court adopted a humanitarian approach and decided to release Mr. Rao on bail, citing that continued incarceration was incompatible with his life. Correctional agencies have a clear constitutional duty to provide treatment for prisoners with SMIs and those in psychiatric crises, regardless of whether these illnesses and crises existed before incarceration or were caused or exacerbated by incarceration.
There are numerous elderlies in prison, similar to Machal Lalung, who remain in eternal waiting without a periodic medical check-up or periodic consideration by the relevant courts for fitness to stand trial. In India, Section 30 of the Prisoners Act, 1900 deals with provisions for mentally ill prisoners. This act directs the state machinery to notify and send a prisoner of unsound mind to mental hospitals for appropriate mental health care and discharge to safe custody, prison or release as per the remaining sentence term. Section 93 of Chapter 12 of MHCA, 2017 also says that state governments should remove all mentally ill persons from prisons to mental health establishments or another place of safe custody. The medical officer in charge of said mental health establishment must report all such mentally ill prisoners’ current health status every six months.
World over, prisons are considered stressful environments and have a significant impact on the mental health of individuals with identified syndromes like “Ganser syndrome or prison psychosis or hysterical pseudodementia.” In prisoners aged between 50 and 54 years, about 50% had mental health problems, and only one-thirds of these people would have adequate access to treatment during the time they were in prison. 38 In contrast to the 13% prevalence in the general US population aged over 65, the prisoner population in the same age range can have as high as 44% of persons living with dementia. 39 Studies on the same in India are lacking. Unique to this vulnerable population is cognitive decline and dementia, a normal part of aging, crosses the mark of normal physiology to pathology rather viciously, and deprives them of early identification and subsequent treatment.
The “punitive bifurcation” whereby those in prison stay in for longer sentences while the admission rates are growing less quickly is a plausible reality. 40 The overall increase in the sheer number of this demographic group compounded with increased incidence of life sentences over capital punishment and improved health care facilities also adds to the same. 41 The proportion of elderly people in prison (defined as 55 years and more in a recent review by Yarnell et al.) ranges from 1% to 30%. Studies have been limited by small sample sizes, selection bias, and nonstandardized assessment tools. 42
The prevalence of dementia in prison ranges from 0.8% to 18%. 43 Prison and cognitive impairment have a bidirectional interaction. An interesting hypothesis of people in prison is the concept of “accelerated aging,” which mentions that the prisoner’s physical health may be 10–15 years more advanced than their chronological age. 44 The people in prison will usually have several distal risk factors like difficult childhood experiences, disadvantaged families, low educational status, substance use disorders, poor nutrition, or head injuries after violence (which may lead to chronic traumatic encephalopathy)40,46, which can, in turn, interact with the many proximal factors like difficult and unstimulating physical environment in prison, the lack of privacy, isolation, and so on resulting in adverse effects on their cognitive capacities.
The commonest form in this age group is Alzheimer’s Dementia. 47 Still, the elderly prisoners are also at risk of developing vascular dementia as they have been often noted to have multiple medical comorbidities with poor coronary health. When the individual does develop the behavioral symptoms of dementia, the chances are that it may not be correctly recognized as a health problem but as a problematic individual resulting in punitive treatment. The other inmates may also have a higher propensity to maltreat or abuse this vulnerable sect of cognitively impaired individuals. The “deliberate indifference,” which entails knowing that an individual was at substantial risk of serious harm and disregarding the information, is an unpleasant reality in this population. 48
In the artificial environment of prison, the dysfunction caused by dementia may be masqueraded as benign forgetfulness as largely the instrumental activities of daily living involving executive brain functions may not be relevant for elderly prisoners. Thus, conventional cognition testing batteries like MMSE, HMSE, etc., may not be sensitive in picking up these cases. 47 Thus, the concept of prison activities of daily living (PADLs) becomes imperative including, dropping to the floor for alarms, standing for headcounts, ambulating to the dining hall for meals, hearing orders from staff, and climbing up and down from the top bunk.
Existing prison medical services have a strong focus on acute health care issues rather than long-term preventive measures. Effective health care provision in the correctional environment can be obstructed due to the routine of the prison, correctional staff unavailability, time constraints, and demands from prisoners. There are barriers for nurses to develop therapeutic relationships with those they care for due to correctional requirements and the physical environment, affecting nurse–patient relationship building. Prejudice of nursing staff about ASPD traits is an important barrier to health care. 48 Cognitive decline as a barrier to providing health care in prison from the help-seeking side is a further impediment.
Intervention for the Elderly Prisoners with Dementia
Dementia in prison remains “a hidden problem” for many reasons:
Prisoners are not screened for cognitive impairment when they enter the facilities Prison staff lack the skills to identify possible dementia Prisoners tend not to report any cognitive or physical symptoms for fear of repercussions The mental health services are often focused on other inmates whose behaviors are more challenging
Thus, the suffering of elderly prisoners with dementia can be mitigated by making changes at the individual, managerial, staff, and environmental levels. At the individual level formalizing the definition of the elderly prisoner and may include even individuals less than 55 years of age with cognitive impairment. Developing protocols for screening prisoners regularly for cognitive impairment and physical health with subsequent referrals and follow-ups of suspected individuals is required. Creating advanced directives for health care decisions may be encouraged early into prison days. Customized activities in the prison environment to stimulate the elderly along with training younger prison inmates to act as facilitators and caregiver for those who are unable to care for themselves and include: listeners, who are prisoners trained by the Samaritans to support fellow prisoners experiencing distress; insiders, who are prisoners who support new prisoners and provide practice advice, information, and reassurance; and hospice volunteers, who are prisoners trained to provide practical support, social and companionship to those who are terminally ill. 49 Develop protocols to facilitate discharge or release from prison into the community of individuals who may be incapacitated and debilitated and render palliative or hospice care. Rehabilitation centers open new vistas for the process of recovery and reintegration, considering the disability of the neurodegenerative disorder and progressively increasing intervention needs for these debilitated individuals. 50
Additionally, the compassionate release of the elderly with dementia from prison may be considered. There are four considerations in this connection: “the chance of recidivism, the rights of the victim, the costs involved in continued incarceration versus the cost of external health care, and the continued welfare of the prisoner with dementia” and addresses the ethical question of keeping an elderly prisoner with dementia in prison. The financial burden of taking adequate care of individuals with cognitive decline in the prison setting and logistic issues is a major concern, especially for the administrative personnel. The common principles followed include supporting age-appropriate regimens and accommodation, enhancing health and well-being, tailored age and interest-relevant programs, and building strong partnerships.
Section 31 of the MHCA, 2017 says that all medical officers of prisons should be trained in basic mental health care. Section 103 (3,4) of the MHCA, 2017 directs that medical officers of prison should send a quarterly report to the concerned mental health board that there are no mentally ill prisoners in prison or jail, which may be verified by the relevant board anytime. Better coordination between different stakeholders facilitating consultations and appointments enriching a multidisciplinary team approach, alongside specialist care, is recommended at the managerial and staff level. 51 Regular staff training on dealing with prisoners with cognitive impairment while helping identify and challenge all such conditions in the custodial setting can be implemented. Facilitating an elderly friendly prison physical environment by adopting design principles for persons with dementia could be the way forward. It can ease decision making, reduce agitation and distress, encourage independence and social interaction, promote safety, and enable activities of daily living by accommodating wheelchairs and walkers, proper lighting, ramps, etc. 52
Future Directions
Studies in this area are scant. There should be systematic studies done to assess the issues of the elderly in prison and the ways to address these issues. Studies should focus on other vulnerable groups like elderly women in prison. They are known to have relatively greater longevity than men and report worse self-rated health than men, the experience of many culturally diverse groups, and their unique requirements related to living with dementia. 53 Helping develop geriatric housing units to facilitate continuum care for elderly prisoners and linking former inmates to postrelease health care services to older persons is another untapped dimension. Increasing the research on dementia in prisoners specifically rather than identifying dementia as a secondary outcome of elderly prisoners and appreciating the difference between cognitive decline and dementia is imperative. Developing a screening and diagnostic tool sensitive and specific to pick up dementia in the prison setting would go a long way.
Evaluations in the area of geriatric forensic psychiatry vary significantly depending on factors in individual cases. Currently, there is a dearth of assistive tools and guidelines on forensic evaluations in the elderly population, and the law does not consider the age of a person in conflict with the law but the disability that comes with it. Therefore, as reflected in our review, consensus guidelines are required, which may be developed in liaison with psychiatrists, geriatric specialists, mental health law and policy stakeholders, and legal professionals.
Footnotes
Declaration of Conflicting Interests
This article has not been published or simultaneously submitted, or already accepted for publication elsewhere. The manuscript has been read and approved by all the authors, the requirements for authorship as stated earlier in this document have been met, and each author believes that the manuscript represents honest work. To the best of our knowledge, this work does not infringe upon any copyright or property right of any third party. There is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.