
Abstract
Background:
Rising population of elder people and associated rise in health problems, frailty and disabilities have significant socioeconomic and health care implications. Mental health related disability contributes significantly in the global disability statistics and is an important health and quality of life indicator. Assessment of disabilities in elderly is essential part of routine evaluation, further it also helps the clinicians in identifying current functional status and choosing and monitoring therapeutic interventions and need for social welfare schemes.
Methods:
In order to understand the process of disability assessment in geriatric psychiatry and to gather information about social welfare schemes a literature review in Google Scholar and PubMed electronic database, and website of various ministries under Government of India was done, using developed key search terms for articles published up to February 2021. The identified eligible articles were reviewed for ideas and concepts, which were then integrated and categorized under broader themes. Finally, the broad categories were discussed briefly based on the above framework.
Results:
Review findings are summarized under the following headings: concept of ageing and disability, assessment of disability, process of certification, and social welfare schemes.
Conclusions:
The process of disability assessment comprises of comprehensive clinical evaluation, use of standardized rating instruments and disability certification wherever warranted or asked for. It is now being acknowledged worldwide by provisions of various social welfare benefits, that living with disability and increased care needs should be an integral part of definition of successful ageing.
Elderly population is the fastest growing age segment worldwide due to increasing life expectancy and associated population ageing. Globally, they constitute about 11.5% of the world population. By 2050, it is projected to increase to about 22% and will outnumber children below 15 years of age. 1 Approximately 46% of elders have some or other disabilities and more than 250 million older people experience moderate to severe disability. 2 Around 5% of the elders in India are affected by some kind of disability, based on 2011 census. 3 However, individual studies and analysis have reported this figure to be higher ranging from 17.9% to 47% using different tools and methodology.3–9
Old age is frequently associated with health-related problems, due to decline of various normal bodily functions, exposing the individual to an array of diseases and disabilities including mental health problems. 10 As per World Health Organization (WHO) data, approximately 15% of elderly above 60 suffer from a mental disorder; and mental and neurological disorders contribute to 6.6% of the total disability (DALYs, i.e., Disability Adjusted Life Years) for this age group. 11 Considering Indian data, the recent National Mental Health Survey, 2016, has reported lifetime prevalence of overall mental morbidity in people above 60 years of age to be around 15.1% (14.9%–15.3%) and prevalence of common and severe mental disorders to be 13.64% and 1.93% respectively. 12
Disability can adversely affect the quality of life of elderly and is a significant health indicator that has heavy social, economic and health care implications. 13 The assessment of functional abilities and or disabilities in elder people comprises of comprehensive assessment to determine the independence in performing activities of daily living (ADL) and quantification of various specific disabilities when present. This assessment helps the clinicians in detecting existing decline in functional abilities, planning and monitoring therapeutic interventions, and need for social welfare schemes. 14 In this review, the disability assessment in geropsychiatry in context of social welfare schemes is discussed.
Materials and Methods
A scoping review, using PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-analyses extension for Scoping Reviews) was done for articles published up to Feb 2021 (PubMed and Google Scholar) relevant to the topic under review. 15 Scoping review was chosen as the purpose is to identify knowledge gaps, scope the available literature and clarify relevant concepts. 16 Many research questions were framed for the study (Table 1) and the following search terms were used: using terms like “disability in elderly,” “disability assessment,” “geriatric assessment,” “social welfare schemes elderly” in various combinations. Additionally, tables of content of online issues of various psychiatric journals published from India like Indian Journal of Psychiatry, Indian Journal of Psychological Medicine, Journal of Geriatric Mental Health were specifically searched for studies evaluating the topics under review. Further for information on various social welfare schemes for elderly and for mentally ill, websites of various ministries and departments like Ministry of Social Justice and empowerment, Department of Disability Affairs, and National Program for the Health Care of the Elderly, etc., were searched.
Research Questions
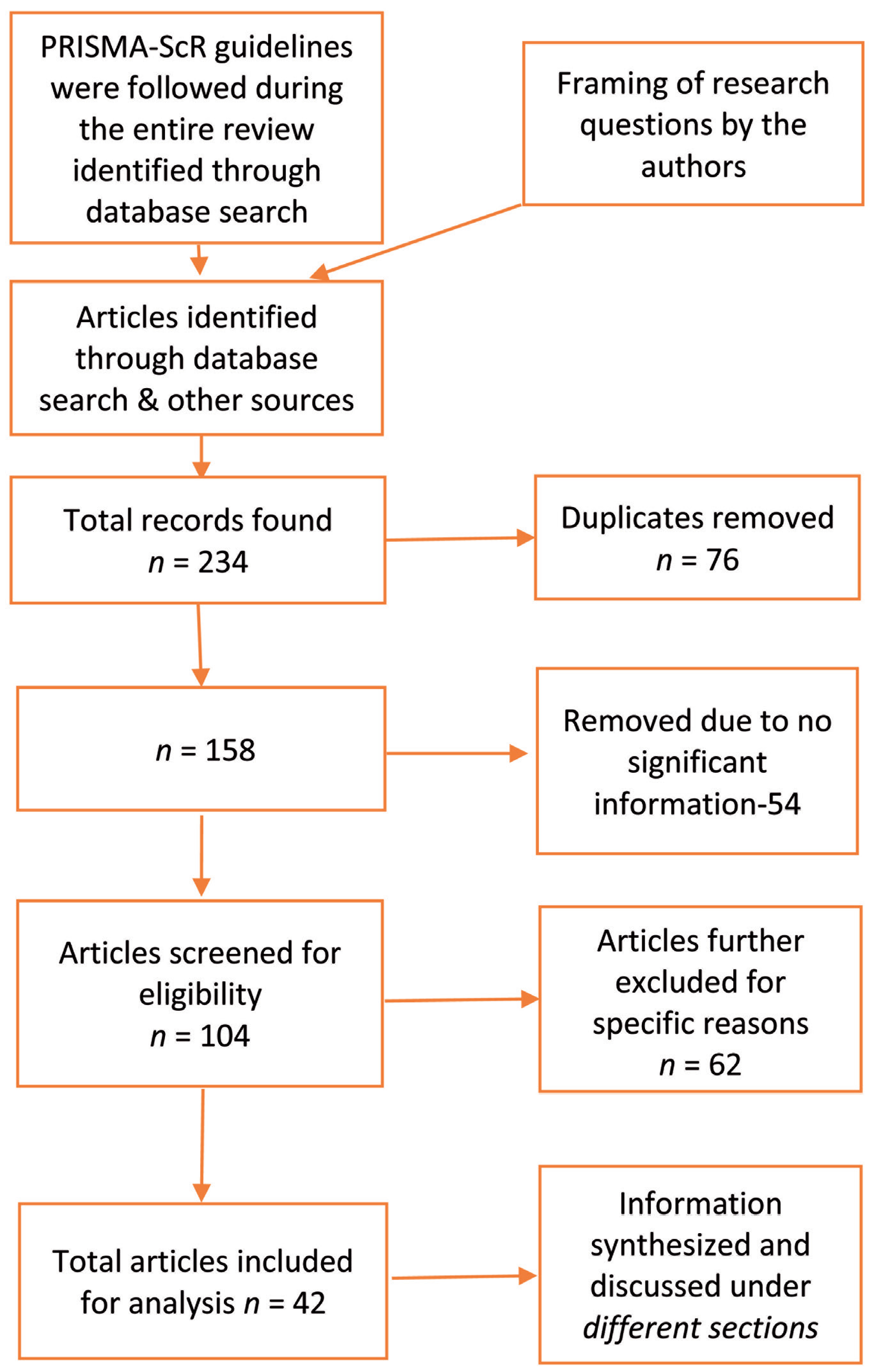
Initially, the authors independently identified 234 peer-reviewed articles and other articles from government websites published in English were selected. After screening those 76 duplicate articles and 54 articles that did not give any relevant information were removed. Further after screening the full text articles 42 articles were further excluded and a total of 62 articles were included for analysis. Information was retrieved from these articles as concepts. The concepts were then discussed under different predefined sections, based on the research questions. A framework of these sections was used to integrate the information into the final review of knowledge (Figure 1).
PRISMA Flowchart for Scoping Review
Results and Discussion
Based on research questions, the review consists of two broad categories: (a) concept of ageing and disability, assessment of disability (psychiatric) and its certification, and (b) social welfare schemes and provisions pertaining to elderly in India.
Concept of Ageing, Frailty, and Disability
The term ageing is frequently associated with chronological ageing process and is commonly linked to reduction in faculties and hence sickness, frailty, and disability. Though there is no universally accepted definition, frailty can be defined as “a state of increased vulnerability for adverse health conditions, including disability, dependency, falls, need for chronic medical care, and mortality.” Though it is used interchangeably with disability, differentiating the two conditions may improve our understanding of ageing process. Conceptually we can say that frailty is a physiologic state of diminished physiologic capacities, and even dysregulation of some systems resulting in difficulty maintaining homeostasis in the time of adversities like acute illnesses, extreme temperature and malnutrition, etc., which increases the risk of developing disabilities. 17 Although there is no universally accepted criterion, Canadian Initiative on Frailty and Aging (CIF-A) developed Edmonton Frail Scale (EFS), consisting of domains like cognition, general state of health, functional independence, social support, medication use, nutrition, humor, continence, and functional performance. 18
Recently, the concept of cognitive frailty has also been introduced, which represents concomitant physical frailty with cognitive decline in absence of overt dementia. 19 There is evidence that frailty, functionality, and emotional regulation have a complex interaction with each other making it imperative to talk about frailty while dealing with disability in elderly. 18
Physical health has an impact on mental health, and the reverse is true as well, e.g., older adults having health conditions like cardiac illness have high rates of depression; and untreated depression can negatively affect the outcome of such illness. 20 Physical functional limitations, pain, low social support, and low sense of mastery, which are often accompaniments in old age, contribute and aggravate the psychological distress.21,22
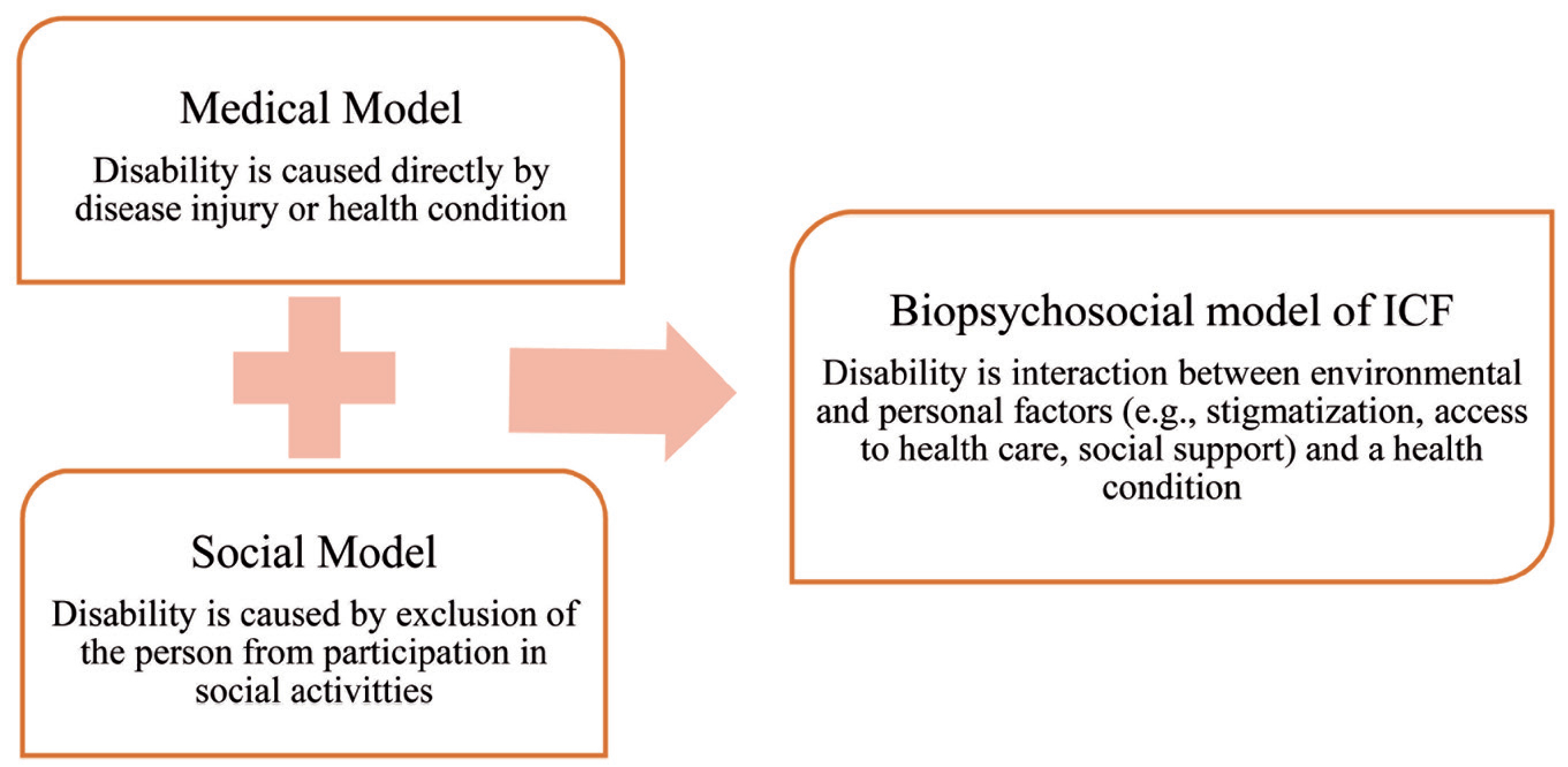
While conceptualizing ageing in context of disability, it is prudent to look at it as a process rather than an event. According to a recent “life course” approach, ageing categories are dynamic in nature and change as per the prevailing cultural and social changes. 23 It argues that both disability and ageing categories are produced in society as they are often excluded from work either due to old age/retirement or disabilities. Life course approach has been more relevant in analyzing ageing and disabilities than chronological categories. 24 The contemporary model of disability further supports this view. The biopsychosocial model (Figure 2), which forms the basis of current International Classification of Functioning, Disability, and Health (ICF), defines disability as, “the interaction between environmental and personal factors (e.g., stigmatization, access to health care, social support) and a health condition (e.g., schizophrenia, cardiovascular disease)” (Figure 3). 25 This is in contrast to the classic “medical model,” which emphasizes solely on disease, trauma, or other health condition, or the “social model,” which takes into account only the effect of contemporary social organization.
Models of Disability 25
ICF Model of Disability
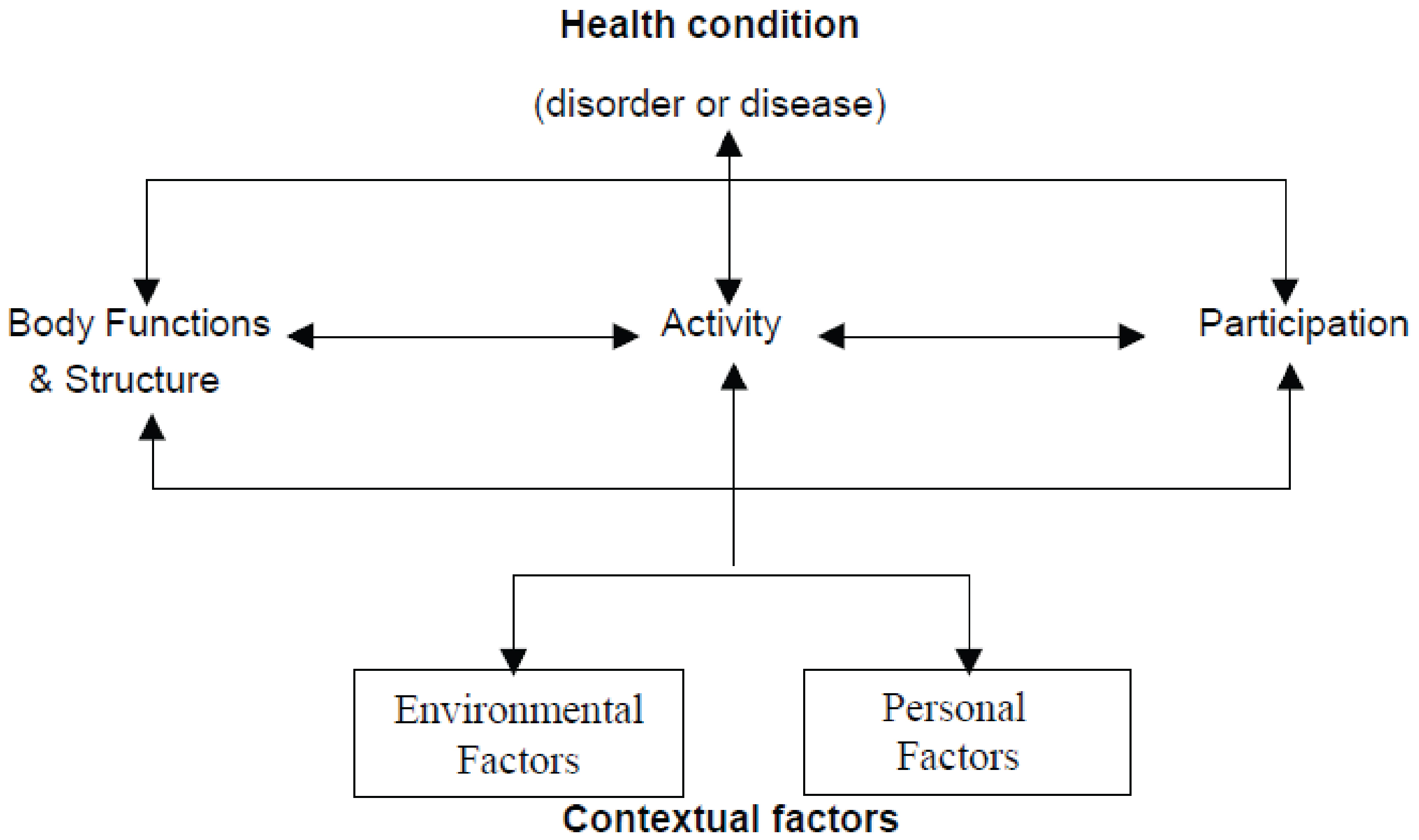
World Health Organization. The International Classification of Functioning, Disability, and Health.
Based on this concept ICF classifies disability as the following
26
:
Impairments: structural or functional problems of body Activity limitations: problems when attempting to carry out an action or task Participation limitations: problems in dealing with real life situation (e.g., social, occupational)
Assessment of Disability
India signed the United Nations Convention on the Rights of Person with Disabilities (UNCRPD) and subsequently ratified the same on October 1, 2007. And further to comply with the recommendations, amended the Persons with Disabilities (PwDs) Act 1995 and replaced it with The Rights of PWD Act, 2016. 27 The prelude of this act clearly expresses efforts to protect the dignity of every PwD and prevent discrimination of any form. It also promotes acceptance of people with disability and strives for complete participation and inclusion in the society. The act defines PwD as “any person with long-term physical, mental, intellectual, or sensory impairments which on interacting with barriers hinder effective and equal growth in the society.” 28
“Mental illness” has been defined by Mental Health care Act 2017 as any mental disorder which is a “substantial disorder of thinking, mood, perception, orientation or memory that grossly impairs judgment, behavior, capacity to recognize reality or ability to meet the ordinary demands of life, other than mental retardation, which is a condition of arrested or incomplete development of mind of a person, specially characterized by sub normality of intelligence.” 29 The RPwD further defines “Person with Benchmark Disability” as a person with not less than 40% of specified disability, which is a minimum eligibility to claim various disability benefits. Among the various disabilities included in the act, of concern to psychiatrist are mental illness, intellectual disability, specific learning disability, autism spectrum disorder and dementia. 27
Assessment for disability. Disability assessment in context of geropsychiatry can be a part of routine evaluation during comprehensive assessment for detecting existing decline in functional abilities, planning and monitoring therapeutic interventions, and need for social welfare schemes. 14 Disability assessment is usually carried out under following subheadings: clinical assessment, use of standardized instruments and/or use of IQ testing wherever applicable. 30
Clinical assessment: In addition to the routine psychiatric evaluation as in adults, a Comprehensive Geriatric Evaluation (Figure 4) is generally recommended, which is a process of assessing multiple problems of older persons, their resources and strengths, the need for services and development of an integrated plan of focused intervention. 31
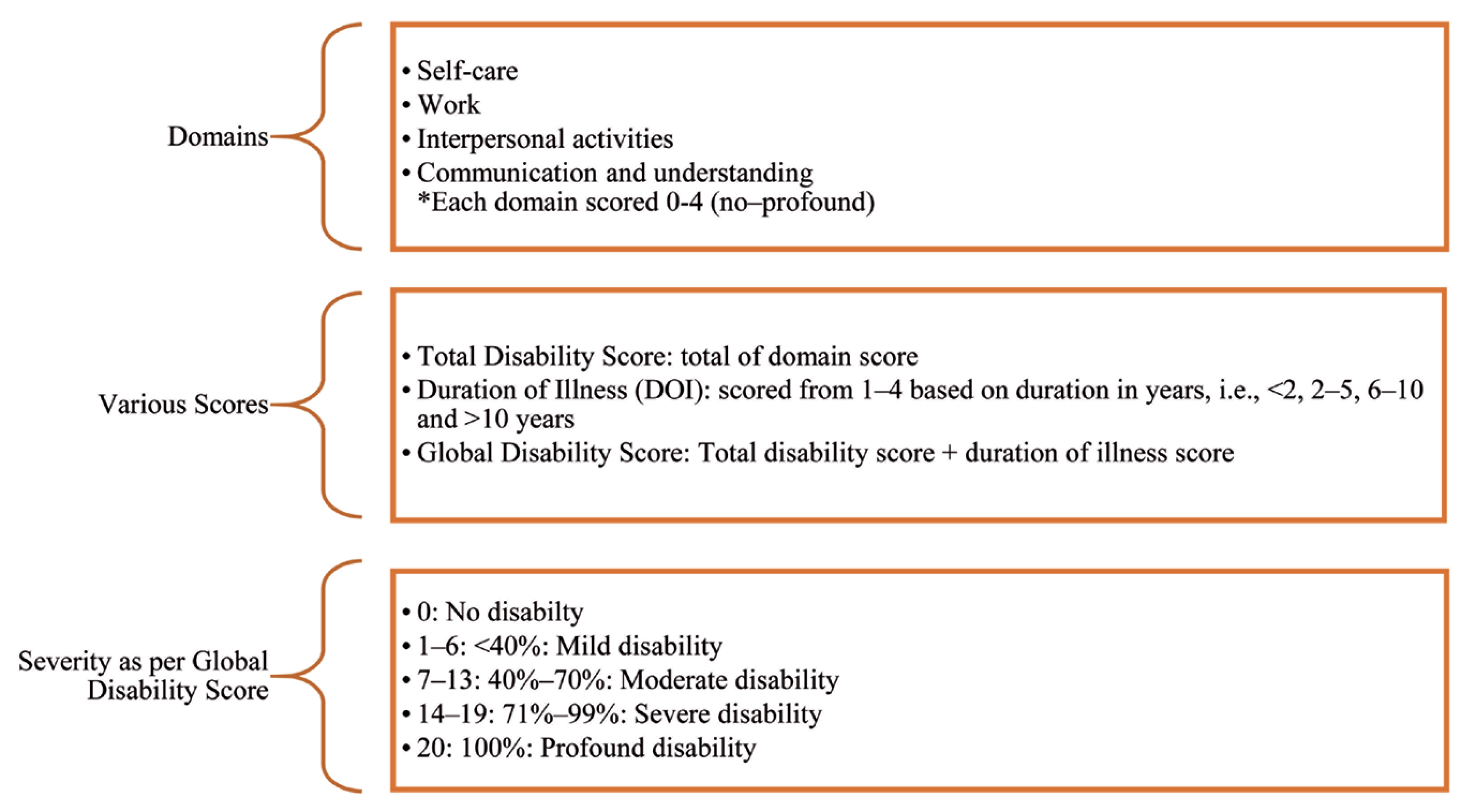
Total disability scores: 3 × 4 = 12
DOI weightage for four years: 2
Global Disability Score: 12 + 2 = 14 (which corresponds to “severe” disability)
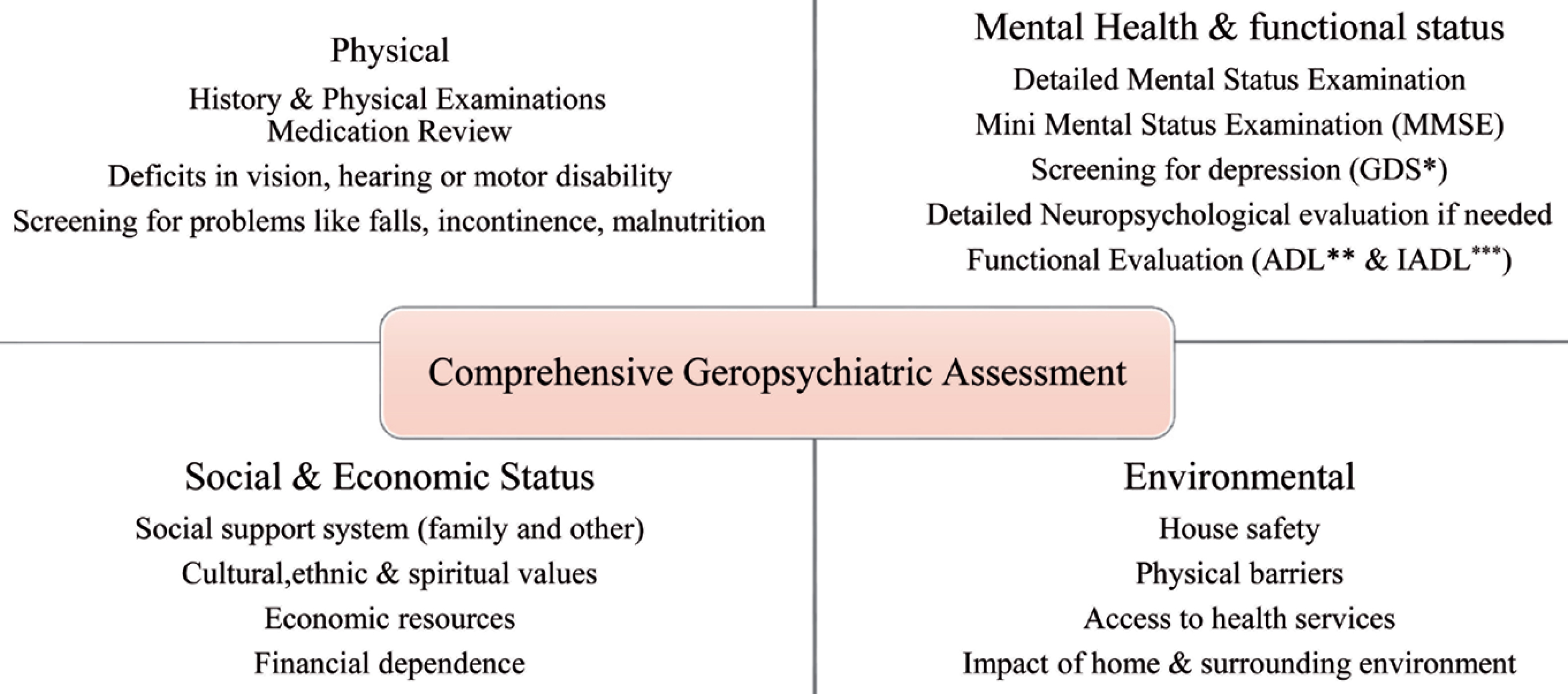
*GDS: Geriatric Depression Scale, **ADL: Activities of Daily Living, ***IADL: Instrumental Activities of Daily Living.
Indian Disability Evaluation and Assessment Scale (IDEAS): The WHO Disability Assessment Schedule (WHO-DAS 2.0) has been amended for Indian setting by the Rehabilitation Committee of the Indian Psychiatric Society into a tool called the IDEAS. It is a simple yet comprehensive instrument (GDS: Geriatric Depression Scale, ADL: Activities of Daily Living, IADL: Instrumental Activities of Daily Living) for measuring mental illness associated disability. IDEAS was advised for only four psychiatric disorders: schizophrenia, bipolar disorders, OCD, and dementia. However, further the Ministry of Social Justice and Empowerment, Government of India, gazetted its use to evaluate disability for all mental disorders, on five dimensions: self-care, work, interpersonal activities, communication and understanding, and duration.32,33 The scale has been field tested across the country, involving 1,078 patients and was found to have good internal consistency, face, content and criterion validities easier to administer and requires less training and time for administration and hence more suited to the Indian setting. 34 It is being used in India for disability assessment in mental disorders.34,35
The domains and scoring of IDEAS are explained in Figure 5. For example, a patient who is suffering from Dementia and has severe disability (score of 3) in each of the four defined domains, calculated based on the manual of IDEAS and has a duration of illness of four years, the calculation of disability will be as follows:
Domains and Scoring in IDEAS 28
However, IDEAS has limitations such as its not suited for disorders other than mental illnesses and it is difficult to calculate duration of illness in episodic disorders like bipolar disorder. 28
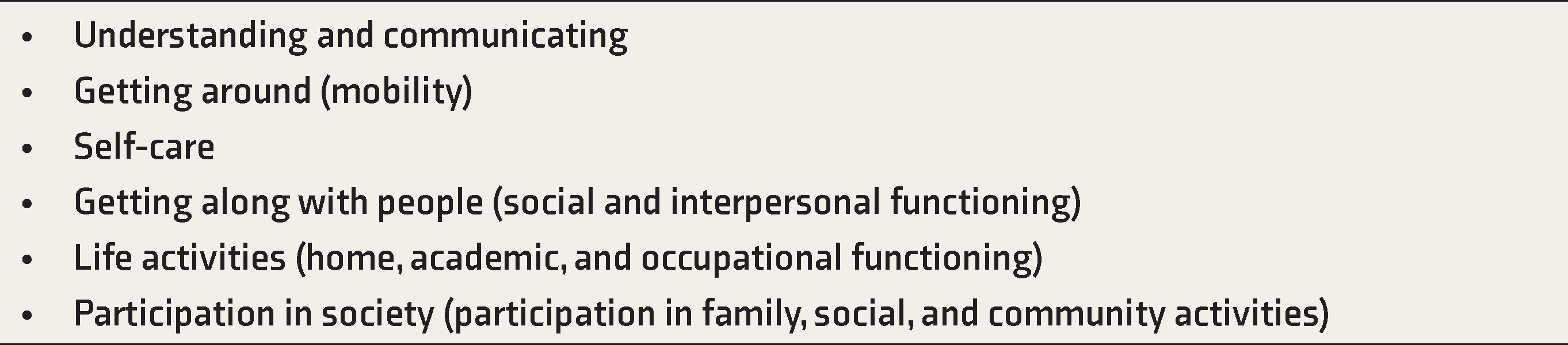
Other Scales: WHODAS 2.0 has its conceptualization that underlies the tenets of WHOs family of International Classifications, and ICF that the final mechanism for any disorder physical or mental to cause disability, is by limitation of activities and behaviors and restrictions on participation in social life. It is a self-report tool that evaluates patient’s ability to perform activities in six domains of functioning (Table 2) in last one month, giving a score of global disability. 33
Domains of WHODAS 2.0 33
It has both manual and computerized scoring options; the earlier one is suitable for clinical purpose. It is reliable, sensitive, culture neutral and applicable across the globe. It has also shown strong psychometric properties across a range of psychiatric and physical disorders. 36 This scale though, takes time and training for administration 27 ; the manual scoring system does not have normative data and it is a self-report tool without any indices to assess validity of response. Nevertheless, according to the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders) Disability Study Group, it is the best instrument available currently for disability assessment in routine clinical use and recommends it to be included in DSM-5. 36
Another less commonly used global measure of disability is “Global Assessment of Functioning Scale” which clinician-rated scale to quantify symptom severity or psychological, social, and occupational functioning over a specified time period, on a range from mental health (score 100) to mental illness (score 0) and was a part of DSM since its third edition. 37
Other Assessments in Elderly
Functional Assessment
As described earlier, clinical assessment and administration of IDEAS remains same for elderly. Apart from global measures, some specific instruments that can be used in elderly are measures of functional capacity by assessing ADL, which are basic activities of personal care and IADL required to live independently in community. 38
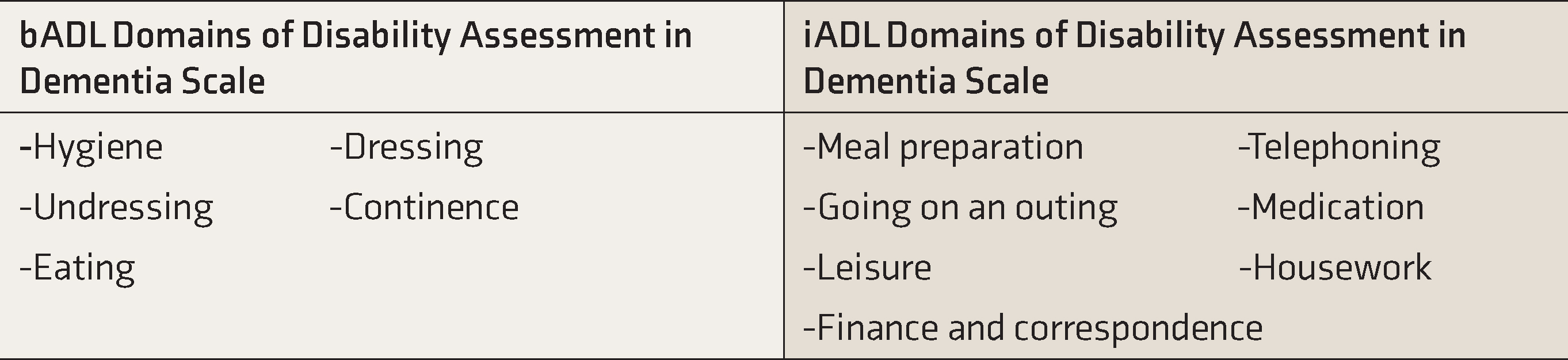
Disability assessment in Dementia (DAD) is one such instrument, which has 17 items that assess basic ADL (bADL) and 23 questions for instrumental ADL (iADL) and leisure activities (Table 3). 38
Domains of Disability Assessment in Dementia (DAD) 38
In addition, separate scales are also available for assessing ADL and IADL like Katz Index of Independence in ADL 39 for bADL and the Lawton-Brody Instrumental Activities of Daily Living (IADL) Scale for IADL. 40
Assessment of Competence
Competence, which in general, is the ability to act in the circumstances, including ability to work, or to reason or make decisions. Its assessment is of particular relevance in patients who have a cognitive dysfunction or suffer from a psychotic illness that makes it difficult for them to provide consent for treatment or legal procedures. Though competency per se is legal terminology, it is task-specific and may vary for different circumstances. Some common procedures where the assessment of competency is mandated are as follows:
Medical treatment and surgical procedures Power of attorney and will Consent by advance directives for research and withdrawal of life support systems
31
Process of Certification for Mental Illness as per Rights of Persons with Disability Rules, 2017
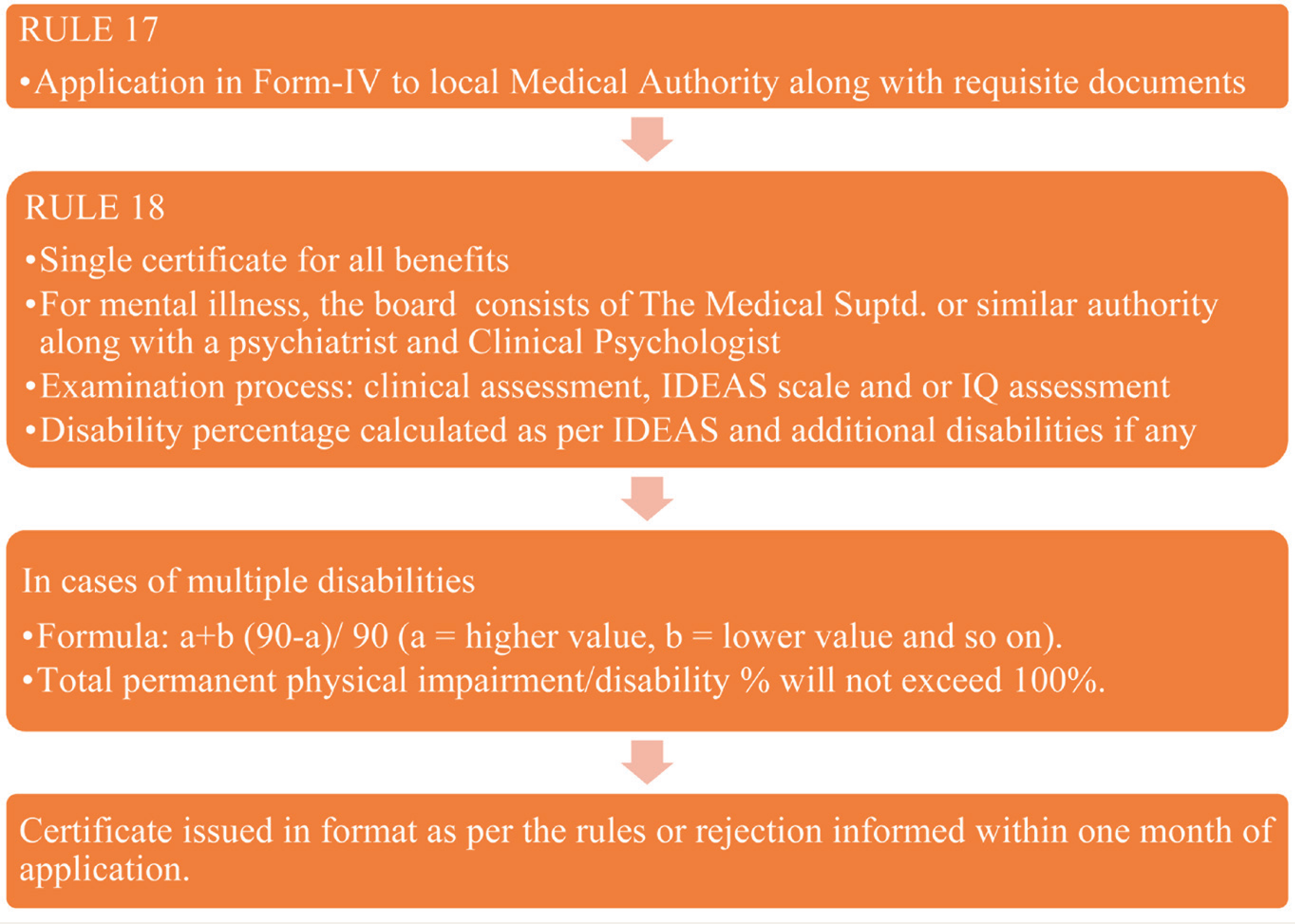
Rule 17: Describes the process of certification in which any person with specified disability or their legal guardian can apply in Form-IV and submit the application to a medical authority in the district as per the proof of residence along with copy of proof of residence, two recent photographs and Aadhar number, if any.
Rule 18: The authority shall issue certificate of reason of rejection thereof within a month of the application. The certificate will either be permanent if there is no chance of variation or improvement over time or temporary if change is expected. This certificate is deemed valid for all purposes like government facilities, benefits, and concessions, etc.
As stated before, the examination process consists of clinical assessment, IDEAS scale and/or IQ (intelligence quotient) assessment where intellectual disability is suspected. If only IDEAS is required, the same is administered and disability quantified as explained above. If only one test does not quantify the disability properly and intellectual disability is also suspected both IQ and IDEAS shall be used and the one showing higher disability be the disability score of the person. 29 In cases where other limitations coexist, they are assessed separately as per the guidelines and the final disability % calculated using the formula: a + b (90 – a)/ 90 (a = higher value, b = lower value). Total permanent physical impairment/disability % will not exceed 100% (Figure 6). 41
Process of Disability Certification as per RPwD Rules 2017 30
Social Welfare Schemes and Provisions for Elderly
The United Nations Geneva Assembly 1991 identified and encouraged nations to follow and promote certain principles in relation to senior citizens.
42
These are as follows:
Independence: Older persons should have access to basic amenities, safe environment, work and other opportunities. Participation: They should be integrated to society, having active participation in movements affecting their well-being and serve as mentors to the young. Care: They should receive family and community care, and access to health care. Self-fulfilment: They should be able to pursue opportunities and have access to educational, cultural, spiritual, and recreational resources of society. Dignity: They should be able to live in dignity and security; should be free from exploitation and discrimination.
With aforementioned principles in mind Indian elder people are protected and promoted through following provisions:
Constitutional approach
Article 41 of the Constitution provides that “the State shall within the limits of its economic capacity and development, make effective provision for securing the right to work, to education and to public assistance in cases of unemployment, old age, sickness and disablement, and in other cases of undeserved want.”
43
Article 46 deals with promotion of educational and economic interests of and other weaker sections; however, does not mention elderly in specific.
44
The above two are under Part-IV of Indian Constitution, which deal with Directive Principles of State Policy (DPSP) and are the basis of policy formation and enacting laws, but are not the fundamental rights of an individual. There are no national or local specific laws in India that directly address age discrimination. However, Article 14 of the Constitution of India provides for equality before the law or equal protection of the laws within the territory of India.
45
Legislative approach
Personal laws: Religion also finds that children are responsible for maintaining their parents and in some cases their elderly relatives also. This has been put forth in statutory provisions under Hindu Adoption and Maintenance Act, 1956, and Muslim law.46,47 Criminal law: Chapter 1X of Section 125 of Code of Criminal Procedures makes provisions that the children provides maintenance to their parents, if proof of neglect or refusal to maintain them is found.
48
The maintenance and welfare of parents and senior citizens act, 2007: The act obligates the children and grandchildren to maintain their parents, grandparents, and older relatives, if they are unable to take care of themselves, which includes food, health care, recreation centers, security, medical assistance, and other necessary amenities.
49
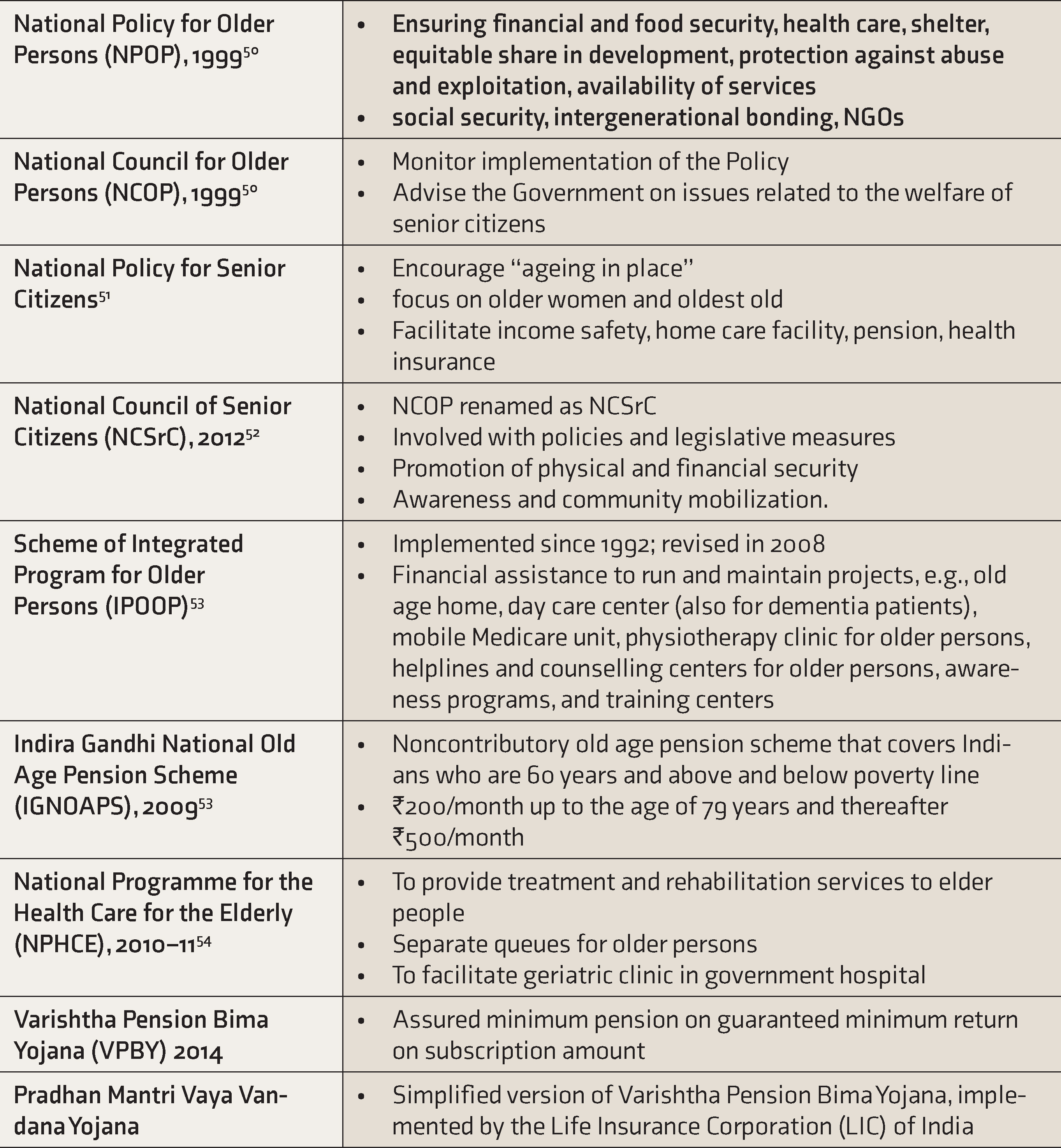
Government approach and policies: The Ministry of Social Justice and Empowerment is mainly responsible for welfare of senior citizens and has launched various programs and policies for the promotion and empowerment of the senior citizens. Table 4 presents a summary of these programs.
Various Programs Initiated by Indian Government for Welfare of Elderly
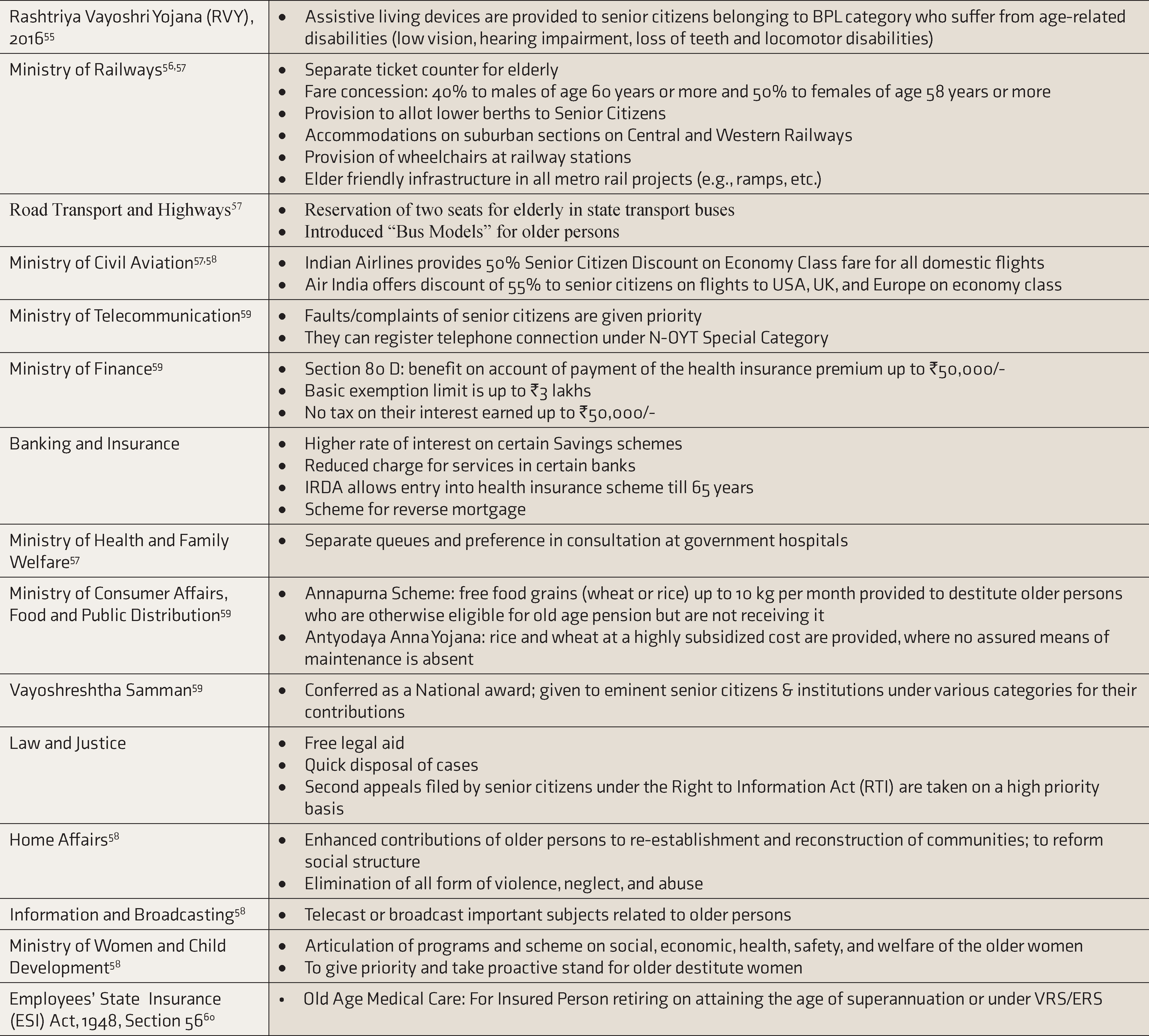
Under the aforementioned initiatives and also in addition to these, multiple provisions are made to support the elderly and improve their quality of life (Table 5).
Facilities and Benefits Provided in Different Areas to Elderly in India
Social Welfare Schemes for Elderly Persons with Psychiatric Disability
Acts and government agencies involved: The rights and welfare of the persons with psychiatric disability are mainly governed by (a) Mental Health Care Act (MHCA), 2017 and (b) Rights of Persons with Disabilities Act (RPWD), 2016. The subject of “Disability” figures in the State List in the Seventh Schedule of the Constitution, but the Central government has also been active in this area via Ministry of Social Justice and Empowerment. However, in view of the enormous number of responsibilities involves, it was stated in the 11th Five Year Plan that “The ‘Disability Division’ of the Ministry of Social Justice & Empowerment will be strengthened by converting it into a separate Department, so that it can liaise effectively with all the other concerned Ministries/Departments and fulfil its responsibilities towards the disabled,” and subsequently in 2012 Department of Empowerment of Persons with Disabilities (DEPwD) was constituted. 61
Benefits and initiatives for persons with psychiatric disability: The constitution and government of India are committed for the welfare of the persons with disability. There are numerous provisions for the inclusion, nondiscrimination and protection of PwD. They are entitled with various benefits by different government agencies in India which are similar to that for other age groups like disability pension, 62 concession in public transport,63,64 reservation in employment,65,66 income tax benefits, 67 financial assistance, 68 insurance schemes,69,70 and legal assistance, 71 etc. In addition, certain other government initiatives and schemes like Scheme for Implementation of Persons with Disabilities Act (SIPDA), Deendayal Disabled Rehabilitation Scheme (DDRS), 72 The National Action Plan (NAP) for Skill Training of Persons with Disabilities, 73 Awareness Generation & Publicity Scheme, 74 and District Disability Rehabilitation Centres, 75 etc., are also in place to fulfil aforementioned objectives.
Barriers to Utilization of Social Welfare Schemes in Elderly
In spite of the existence of these social welfare schemes for elderly in India, their utilization is still questionable due to multiple reasons. Firstly, there is inadequate awareness of these schemes, ranging from 46.4% to 86.9% as found by studies done in Northern India. 76 Another study found that lack of knowledge remains the most common barrier to access these benefits. Other common impediments are lack of clarity of procedure, lack of knowledge of facilities that can be availed using a particular scheme, tedious formalities, form rejections, corruption, and schemes not well implemented or advertised by the concerned authorities. Measures using newer technologies can be taken up to raise awareness about these schemes and to make the process more user friendly. Corruption should be dealt with severe punitive actions since it weakens the faith of elders in system and denies them of their rights.76,77
Conclusions
From the perspective of population science, the lifespan is increasing, thereby leading to increase in number of years spent in old age as well as disabilities. Considering this notion, the concept of successful ageing would include optimal living conditions and imbibes care needs including various strategies and resources for autonomy and improved quality of life. 78 Government, through its various schemes and provisions, has been trying to reduce day-to-day hassles, provide financial and other support to improve their quality of life and provide a sense of security. However, complexities in assessment of geriatric disability and barriers in utilization of available resources remains a challenge and also an underexplored area, at least in Indian subcontinent, requiring further research. We further support the notion that expanding the horizon of successful ageing to ageing with inclusion should be our way ahead.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.