
Abstract

Sir,
Despite several criticisms, adjustment disorder (AD) continues to be a commonly diagnosed condition in several clinical settings. 1 A wide variety of pharmacological and psychological interventions have been tested in patients with AD. 2 Not surprisingly, antidepressants and benzodiazepines are the most widely studied psychotropic medications in patients with AD.2,3 The previous studies on the prescription pattern of psychotropic medications did not report the findings on AD as a separate category. For instance, the Indian Psychiatric Society multicentric study revealed that antidepressants and benzodiazepines were prescribed in more than 70% of patients with neurotic, stress-related, and somatoform disorders. 4 The above study did not report the prescription pattern in AD separately. The follow-up pattern of patients with AD is also of clinical interest due to the condition’s transient nature. A previous study reported that more than half the patients diagnosed with AD dropped out after the first visit. 5 In this context, the present analysis was conducted to determine the prescription and follow-up patterns in psychiatric outpatients with AD.
The present analysis was part of a larger study conducted in a tertiary care teaching hospital in South India. This retrospective observational study was approved by Institute Ethics Committee. The records of all the new patients evaluated in the psychiatry outpatient department from January 1, 2019 to August 31, 2019 were reviewed. Patients of both sexes with a documented diagnosis of AD were included. Those with grossly incomplete records were excluded. All the data were collected from the Hospital Information Management System. Data on sociodemographic parameters and clinical details were abstracted. Subsequently, the prescription details, including the names and number of psychotropic medications prescribed, frequency of drug use, and duration of the first prescription, were obtained from the first prescription issued to the patient. The follow-up pattern was assessed by counting the number of times the patient visited the psychiatry outpatient department during the six months from the date of the first evaluation. Frequencies and percentages were used to summarize categorical data. Continuous variables were represented as means and standard deviations.
A total of 880 outpatient records were screened, 39 (4.43%) patients had a documented diagnosis of AD, out of them, 16 (41%) had an education of graduate level or above and 10 (25.6%) were unemployed. Only one patient was admitted, and the rest were managed on an outpatient basis. A total of 36 (92.31%) patients received some form of pharmacotherapy (Table 1). The remaining 3 (7.69%) were referred to the clinical psychologist for psychotherapy. Escitalopram and clonazepam were the most widely prescribed psychotropic medications. Notably, 27 (69.23%) patients dropped out after the first consultation.
Sociodemographic Details, Prescription Pattern and Follow-up Pattern in Patients with Adjustment Disorder
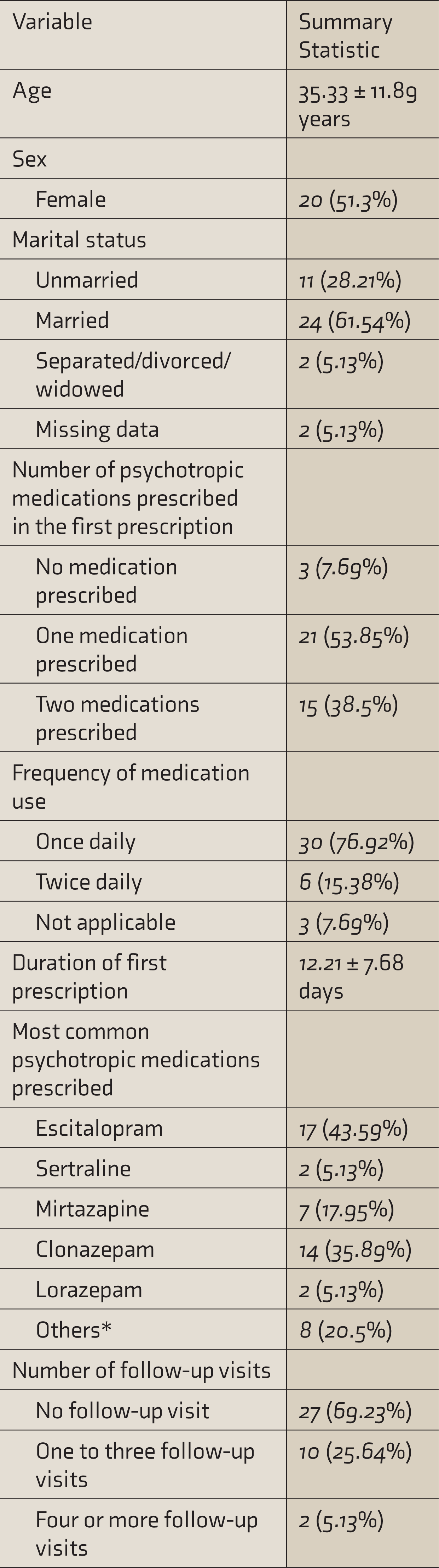
*Included duloxetine, amitriptyline, dothiepin, trazodone, and propranolol.
We found that less than 5% of the psychiatric outpatients received a diagnosis of AD. This relatively low rate could be explained by the fact that the study was conducted in a tertiary care teaching hospital. Our findings indicate that clinicians prefer pharmacotherapy over psychotherapy in patients with AD. This could be attributed to time constraints and limited availability of resources in a general hospital setting to conduct psychotherapy. Alternatively, brief counselling or supportive psychotherapy may have been given in many cases but was not documented in the outpatient records. Not unexpectedly, antidepressants and benzodiazepines were the most widely used. These findings are consistent with a study from Germany that reported that more than 80% of the inpatients diagnosed with AD received antidepressants, antipsychotics, and/or tranquilizers. 6 A study conducted in primary care settings in the United Kingdom reported that 37% of patients with AD had a psychotropic prescription. 7 The drop-out rate of 69% after the first visit in the present study is relatively more than the rate of 55% reported in an earlier study conducted in a tertiary care center in North India. 5 The high dropout rate is likely due to many factors, including the transient nature of the illness, dissatisfaction with pharmacotherapy, distance from the hospital, and socioeconomic factors.
The retrospective nature of the study ensured that real-life prescription pattern in AD was assessed-knowledge about an ongoing study of this nature would have influenced the prescription patterns of the clinicians. Due to the study’s retrospective nature, standard diagnostic instruments were not used and instead, the diagnosis documented in the case records was considered valid. A small proportion of patients may have continued treatment in another clinic or hospital, which could have contributed to an over-estimation of drop-out rate.
To conclude, pharmacotherapy with escitalopram and/or clonazepam was the preferred treatment modality for most patients with AD. Two-thirds of the patients dropped out after the first visit. The present study highlights the current prescription pattern and the drop-out rate in patients with AD, thus filling the existing knowledge gap in the Indian literature.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.