
Abstract

The National Mental Health Survey of India showed that the use of opioids is widely prevalent across the country and that there is an increased prevalence in certain localized geographical areas. 4 Uttarakhand, a predominantly hilly state in the northern India, also has seen a rise in the prevalence of OUD over the past few years. 5 According to a recent nation-wide survey, the prevalence of opioid use in Uttarakhand is 0.8%, which is slightly higher than the national prevalence of 0.7%. 6 As a result, the OST has also been scaled up for the effective treatment of patients in this region. 7 The main OST service available in Uttarakhand is dispensing buprenorphine–naloxone combination (BNX) tablets. The majority of this service in this area is provided by private teaching hospitals where the supply of BNX is via private dealers.
This article depicts the experience of a private teaching hospital after its stocks of BNX were exhausted due to the restrictions placed due to the COVID-19 outbreak. This hospital has been providing OST for the past five years. This is the only OST center that caters to the suburbs of the Dehradun city with no other OST center in a 30-kilometer radius. To sum up the situation, the authors made a review of the patients visiting the psychiatry outpatient department around the time the COVID-19-related lockdown started. The patient records were reviewed and compared in three important time frames (
Phase I (from February 25, 2020 to March 24, 2020): Before the onset of the lockdown
Phase II (from March 25, 2020 to April 22, 2020): After the onset of the lockdown and till the stock of BNX was available in the pharmacy
Phase III (from April 23 to May 4, 2020): After the stocks of BNX were exhausted while the lockdown continued
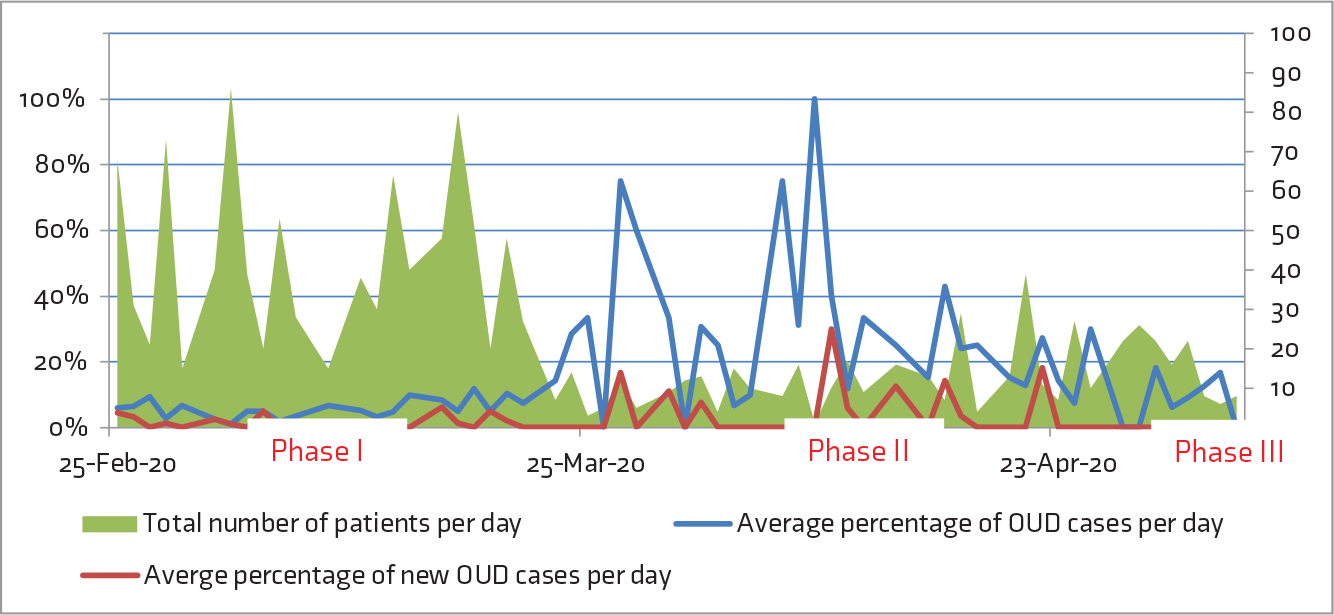
OUD: Opioid use disorder.
It was found that due to the lockdown, the total number of patients attending the psychiatry OPD diminished drastically (Mean±SD attendance per day in Phase I: 42.5 ± 23.07, Phase II: 12 ± 8.44, and Phase III: 15.5 ± 8.2). But, after the onset of lockdown, there was a sharp rise in the percentage of OUD patients attending the clinic. Average percentage of OUD per day in the three phases were as follows: Phase I—5% (n = 56), Phase II—24% (n = 71), and Phase III—9% (n = 15). However, this rise immediately vanished after the non-availability of BNX. Similarly, there was also a rise in the number of new patients of OUD attending the clinic, which vanished after the non-availability of BNX. Average percentage of new OUD per day in the three phases were as follows: Phase I—1% (n = 14), Phase II—4% (n = 16), and Phase III—0.2% (n = 1) (
We believe that this experience shows a very interesting trend. It is evident that the lockdown had caused an increased influx of patients of OUD to the hospital. The reason behind this could be the non-availability of illicit opioid substances. The increase in the number of new patients can be explained by the care-seeking attitude precipitated by having to spend more time amongst the family members. However, the sudden decrease in the number of patients, coinciding with the exhaustion of BNX, raises an uncomfortable question.
One possibility is that the patients started indulging in reckless activity (like stealing) to continue their opioid use. Another possibility is that they restarted intravenous drug use or are diverting other opiate drugs prepared for medicinal purposes. In both the cases, opioid overdose remains a very worrying complication. 8 Furthermore, the tendency to continue drug use alone (enforced by lockdown and to prevent sharing) may also further delay emergency help-seeking if required. To summarize, a sudden exhaustion of BNX may predispose an already vulnerable population to greater dangers. To estimate the potential danger, we have to look at the existing literature, which shows, for example, that in Russia, banning of methadone led to an increase in OUD and HIV infection, which ultimately spiraled out of control into an epidemic. 9
We hypothesize that the current phenomenon reflects the unpreparedness of an already taxed healthcare delivery system. Understandably, the COVID-19-related lockdown is probably the most significant public health emergency we saw in our lifetime. But still, patients with OUD should not be low down in the priority list of emergency services. We should be better prepared to mend the broken supply chain of OST to prevent a disastrous outcome in such patients. 10
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.