
Abstract
Background:
Absconding from psychiatric hospitals is of great concern for patients and caregivers. Absconding affects not only the treatment and safety of these patients but also patient’s caregivers and the community. Further investigation is needed to examine the pattern of this event and the characteristics of patients who abscond. Hence, our study was aimed to examine the sociodemographic and clinical profiles of inpatients who absconded from a psychiatric hospital in five years and to compare them with matched controls.
Methods:
A retrospective chart review of inpatients who absconded and matched control inpatients during the specified period of five years from January 2014 to December 2018 was done at a psychiatric hospital. Each control was matched with a corresponding absconding case on the following order: (a) admission ward, (b) admission period, (c) diagnosis, and (d) age. Results: Among 20,052 adult admissions during the specified period, 38 patients absconded, with a rate of 1.8 per 1,000 admissions. Most of them were male, from a younger age group, diagnosed with schizophrenia or mood disorder, and having comorbid substance use disorder, irritable affect, impaired judgment, and absent insight. Most of the events occurred within the first two weeks of admission. About 11% of them had a history of prior absconding from the hospital.
Conclusion:
Knowledge about the associated sociodemographic and clinical profile would help clinicians and mental health care professionals to prevent absconding. Further risk assessment using a patient’s profile would help to reduce absconding events from psychiatric hospitals in the future.
Methods
The study was conducted at a psychiatric hospital in India. Under adult psychiatry, the institute has three units for male patients, three units for female patients, and a dedicated unit for addiction psychiatry. Patients aged more than 18 years are admitted in these units. There is an open ward system, where the patients are admitted and managed with no/least restrictive measures. The institute has a boundary wall surrounding the campus and a main gate for entry and exit. The wards are adequately staffed with nurses and attendants across three fixed shifts of duty spanning over 24 hours. The staffing pattern is fixed for a type of shift (morning, evening, and night) across wards, based on the number of beds available for that ward. Each morning shift has 3–5 nursing personnel and 2–3 ward attendants, apart from the housekeeping staff, which is largely outsourced.
Approval was obtained from the Institutional Ethics Committee before collecting data. A separate register is maintained in the institute to record the absconding events. After an inpatient is reported missing in count from any ward during the mandatory headcount at the beginning and/or end of each shift, the information is passed to the treating team and hospital administration. A thorough search is conducted in the hospital premises. The local police station is also informed simultaneously. If the patient cannot be traced inside the hospital area and he/she fails to return to the hospital before midnight of the same day, either by himself/herself or by assistance, he/she is considered as absconding. Such events are recorded in the absconding register.
A list of case record file (CRF) numbers of patients who absconded between January 1, 2014 and December 31, 2018 was made from the register. Corresponding admission register of each case was accessed and searched for the admission period of that case. Parallelly, from other admitted inpatients of that admission period, a control was selected, matched with the diagnosis and age of the corresponding absconding case. Thus, each control was matched with the corresponding absconding case in the following order: (a) admission ward (admitted and residing in the same unit and ward as in each case of absconding) (b) admission period (the time period of admission during which the absconding case was admitted, (c) diagnosis, and (d) age. The method of chart review was followed for data collection. Sociodemographic information was recorded. Details for the event of absconding were collected. For clinical profiles, mental status examinations (MSE) done both during the admission and before the event of absconding were reviewed. As a part of the protocol of the institute, all the patients were examined regularly twice a day, in the morning and evening, and the clinical notes were recorded in CRFs. The MSE is structured and comprehensive in the case records. For cases, the most recent MSE before absconding was reviewed. For controls, the MSE most proximal to the date and time of absconding of the corresponding case was recorded. This was done to match immediate external factors around the event of absconding.
Statistical Analysis
Statistical analysis was performed, using the level of statistical significance of P < 0.05, in the Statistical Package for the Social Sciences (SPSS) version 22.0 for Windows. Sociodemographic characteristics and clinical profile of the sample were analyzed by descriptive statistics. Those records where either history was not available or MSE could not be elicited or did not specify psychopathology were excluded from the analysis. Chi-square test was used to assess discrete variables. Fisher’s exact test and Yate’s continuity correction was applied wherever applicable. After checking skewness, Student’s t or Mann–Whitney U test was applied for continuous variables.
Results
There was a total of 20,052 admissions in adult psychiatry in the specified period. During this period, 38 patients had absconded. Thus, the rate of absconding was 1.8/1000 admissions (0.18%).
Sociodemographic and Clinical Characteristics
Comparison of Sociodemographic Variables between Groups (N = 76)
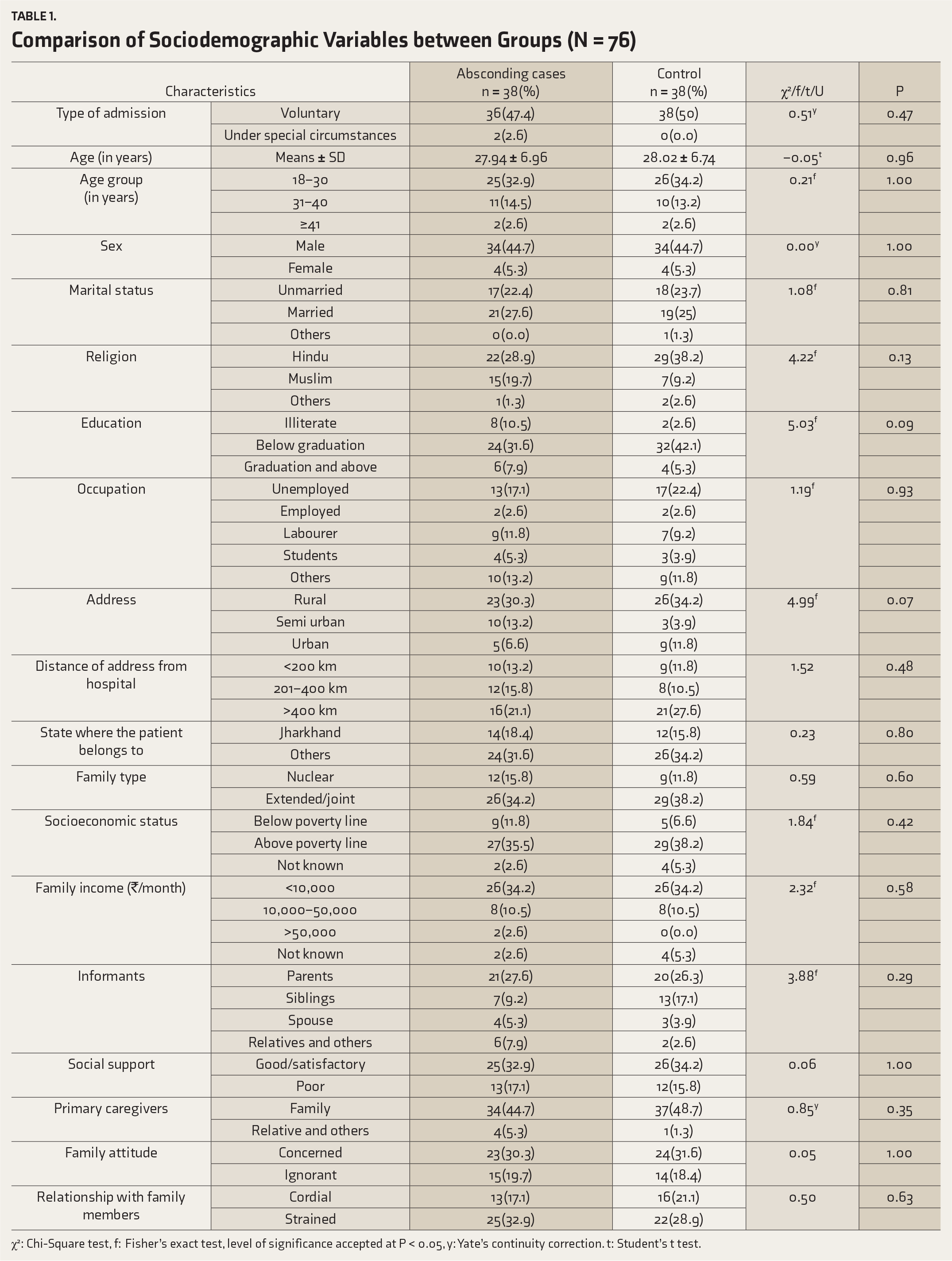
χ2: Chi-Square test, f: Fisher’s exact test, level of significance accepted at P < 0.05, y: Yate’s continuity correction. t: Student’s t test.
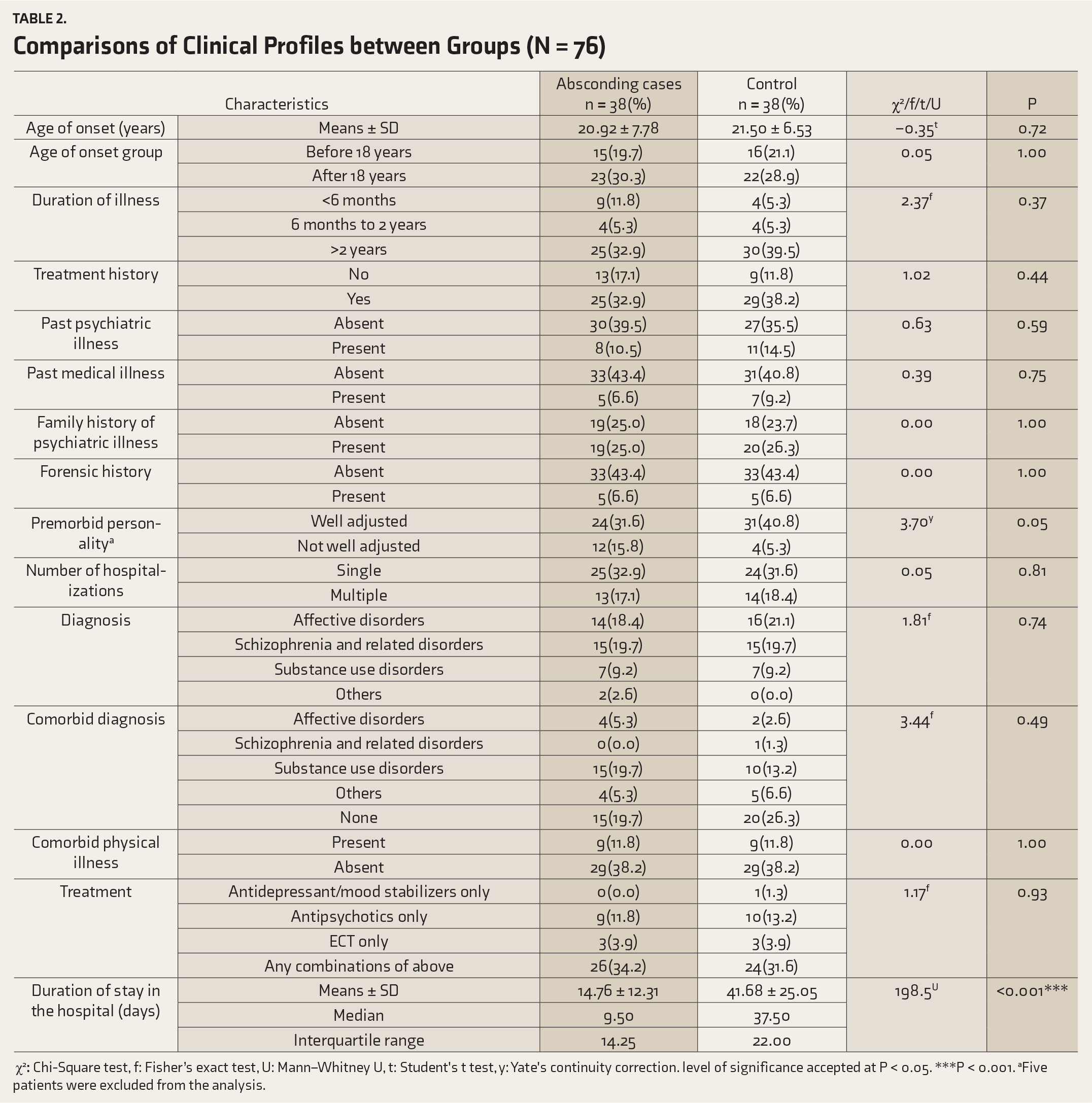
Comparisons of Clinical Profiles between Groups (N = 76)
χ2
Mental Status Examination at the Time of Admission
More cases of absconding had loud and overproductive speech (32.9%, n = 25) than controls (25%, n = 19). There was a significant difference in affect between the groups at the time of admission (P = 0.005). More absconding cases (22.4%, n = 17) than controls (9.2%, n = 7) had irritable affect. More patients in the control group (n = 13) than in the absconding group (n = 5) had perceptual abnormalities (P = 0.04). Most of the cases in both the groups had impaired judgment and poor insight about illnesses at the time of admission. Table 3A shows the comparison of MSE findings between the groups at admission
Comparison of Mental Status Examination at the Time of Admission between Groups (N = 76)
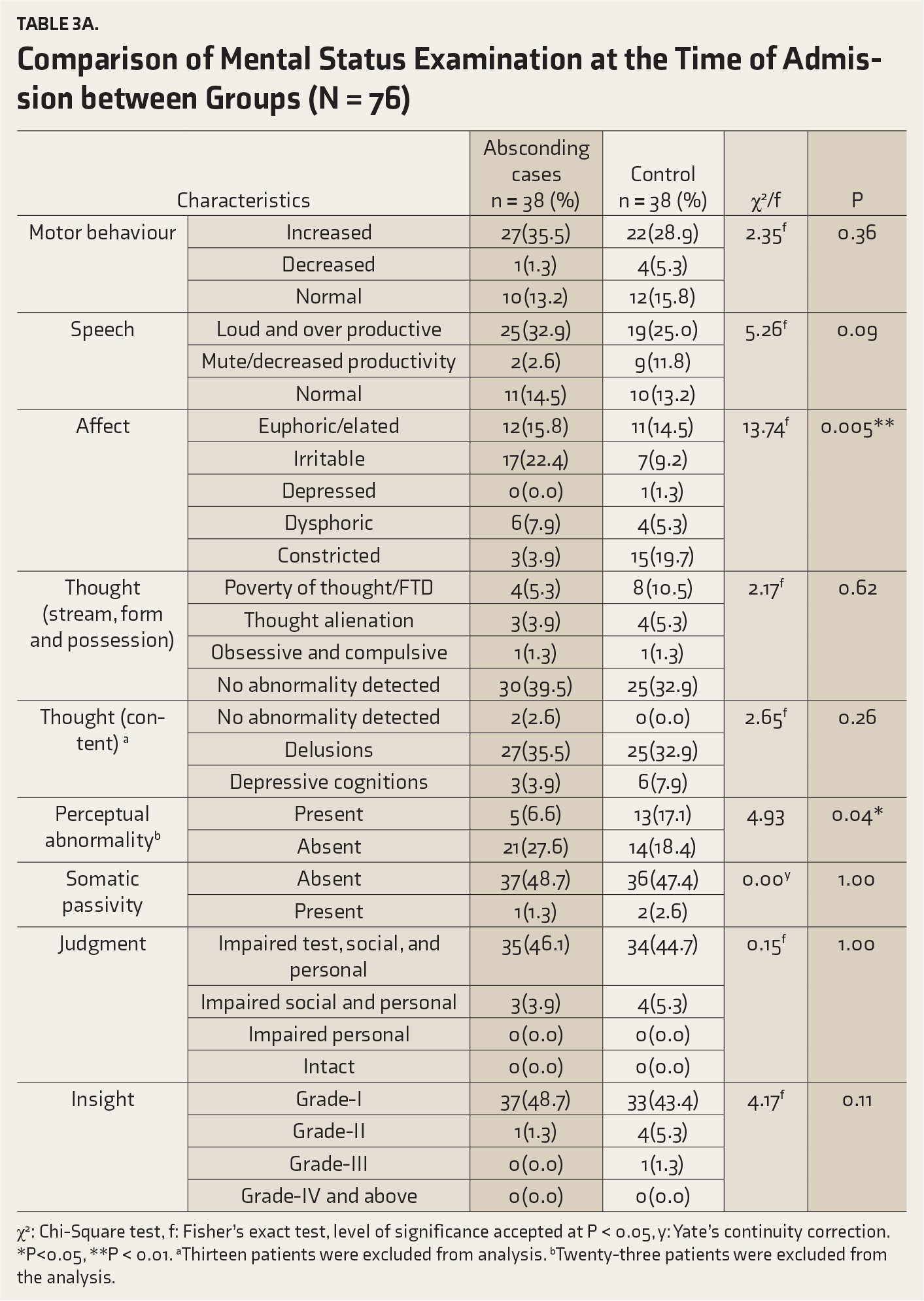
χ2: Chi-Square test, f: Fisher’s exact test, level of significance accepted at P < 0.05, y: Yate’s continuity correction. *P<0.05, **P < 0.01. aThirteen patients were excluded from analysis. bTwenty-three patients were excluded from the analysis.
Mental Status Examination Before the Event of Absconding
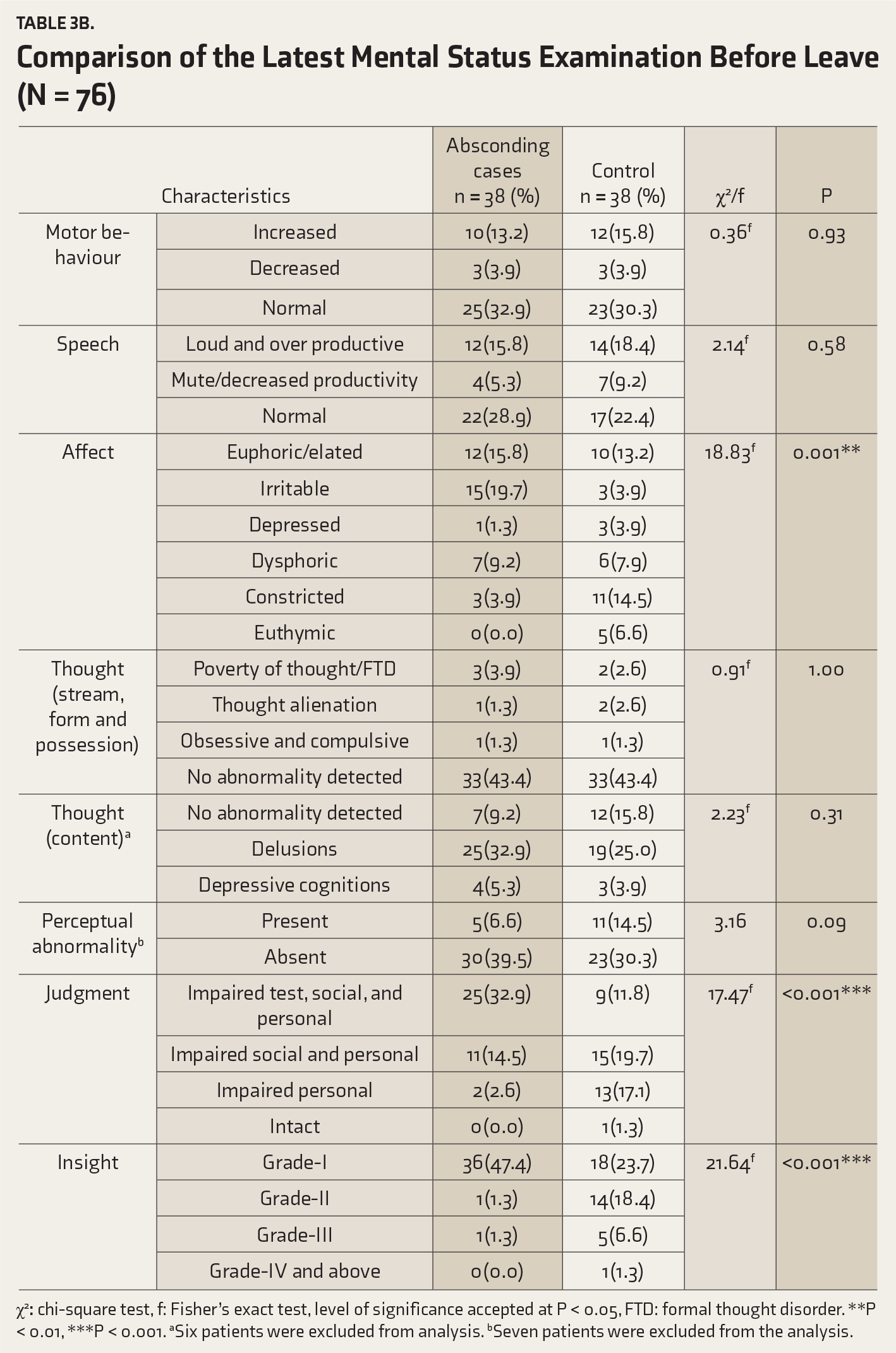
There was a significant difference in affect between the groups (P = 0.001). Affect was found irritable among more cases of the absconding group (19.7%, n = 15) than the controls (3.9%, n = 3), while a higher proportion of constricted and poorly communicable affect was found in the controls (14.5%, n = 11) than the absconding group (3.9%, n = 3). A trend toward higher perceptual abnormalities was noted in the control group (P = 0.09). There was a significant difference between the groups in relation to judgment and insight (P < 0.001). Impaired test, social, and personal judgments were found more in the absconding group (32.9%, n = 25) than the controls (11.8%, n = 9). Most of the patients in the absconding group had no insight (47.4%, n = 36). Table 3B shows the comparison of MSE findings between the groups before the time of absconding.
Comparison of the Latest Mental Status Examination Before Leave (N = 76)
χ2
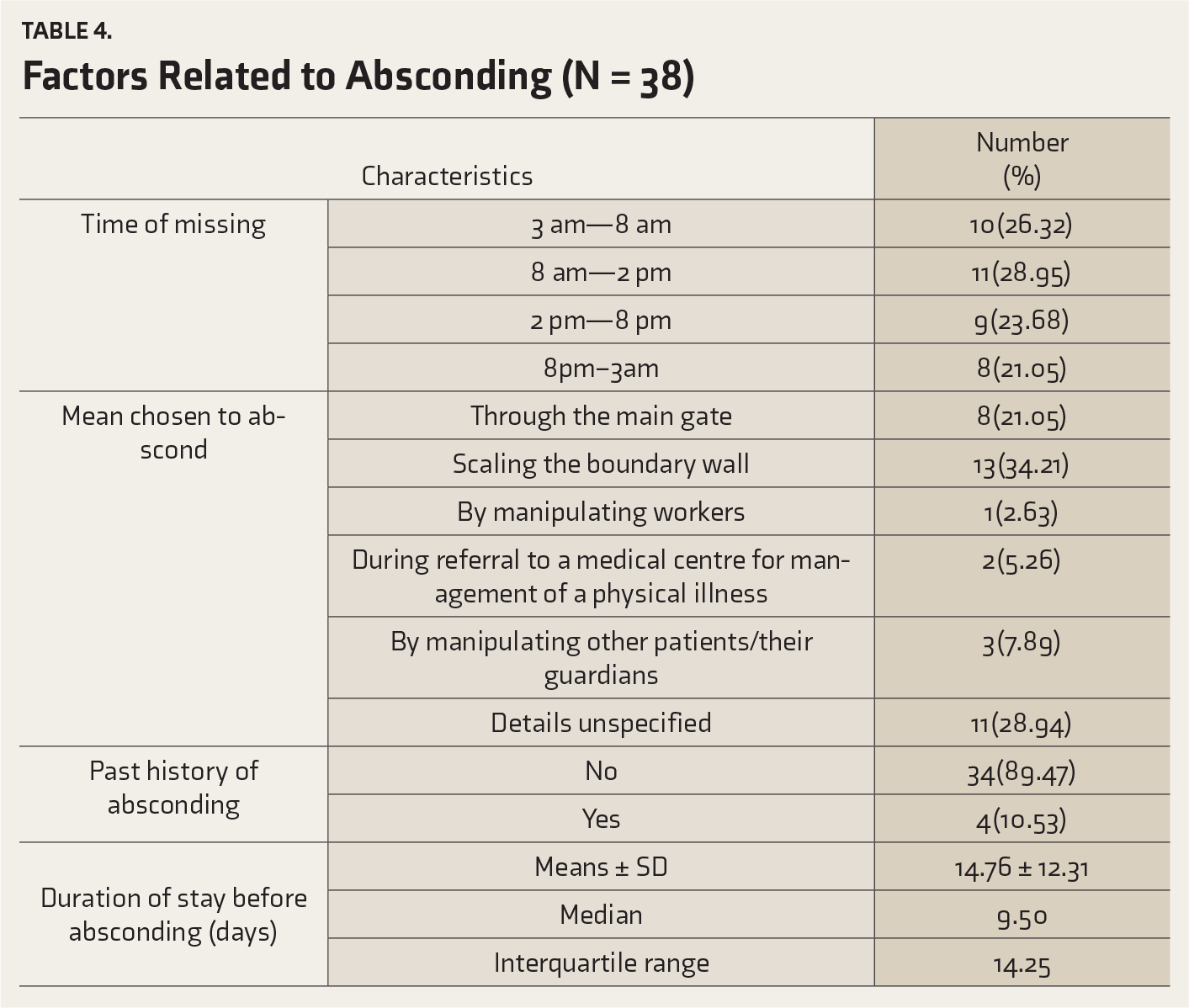
Factors Related to Events of Absconding
Table 4 shows various factors related to the absconding behavior. The mean duration of stay till the date of absconding was 14.76 ± 12.31 days. The most common timing was 8
Discussion
Our study examined all the absconding events from the inpatient care of a psychiatric hospital over a period of five years. The strengths of our study were not missing any cases of absconding and close matching between the cases and controls. Admission period and admission ward were matched, as these might influence immediate environmental factors such as, level of supervision, security level, and clinical management protocols. As psychiatric diagnoses are often heterogeneous in nature and dependent upon a constellation of psychopathologies, matching diagnosis helped us examine several clinical factors, including psychopathologies not attributable to the difference in the diagnosis between the groups. A similar matching protocol had been adopted by research that investigated absconding from an inpatient setting and other uncommon hospital events like inpatient suicide.8, 15, 25–29 As the controls were matched for the admission ward and admitted under the same unit of the corresponding absconding case, both the groups became matched for sex too. Another strength was that we reviewed the MSE at two time points.
The rate of absconding in our study was 1.8 incidents per 1,000 admissions. This rate is low compared to previous studies, where the rate ranged from 1.85% to 17.2%.20, 22, 23, 30, 31 A systematic review found the rates to be substantially lower for locked wards (1.34/100 admissions) compared to open wards (7.96/100 admissions). Despite being an open ward system, comprehensive management, including continuous risk assessment, monitoring, and supervision by treating teams consisting of a psychiatrist, clinical psychologist, psychiatric social worker, psychiatric nurse, and ward attendants might have reduced absconding, accounting for the lower rate in our study. Different rates across the world might be due to a difference in the type of security measures, type of hospital care, the presence of forensic patients, legal measures, and multiple other factors. 3
Most of the total sample in our study was admitted as voluntary admission under Mental Health Act 1987 and subsequently as independent admission under Mental Healthcare Act 2017 in both the cases and the control group. In contrast to this, most studies have demonstrated an increased prevalence of involuntary admission among inpatients who abscond.4, 7, 13, 32 A recent study by Gowda et al., 24 at a psychiatric hospital, also showed that most patients who absconded had involuntary admission. However, a case-control study by Bowers et al. 5 did not demonstrate the above finding and instead suggested that the escaping incidents might be more officially reported among involuntary patients than the voluntary ones. In our study, the mean hospital stay for the absconding group was 14.8 days. Though a recent study found that a longer duration of stay is predictive of absconding, 31 other studies found that most absconding occurred during the first two weeks following admission. This may be because, during the initial two weeks of inpatient care, adjusting to the hospital environment happens and the illness is often most acute.19, 33
We did not find any significant difference regarding marital status between the groups. A recent case-control study by Khammarnia et al. 15 showed no significant difference between those who absconded and those who did not, in terms of age and marital status. A few studies have found a higher rate of absconding among unmarried inpatients.4, 33 Our study did not find any difference in religion between the groups, which is consistent with the findings from other studies.4, 21 However, some studies have a different finding.5, 34–36 Like other studies, most of the absconding cases in our study were male and from a younger age group.15, 22, 24, 30, 33 Similarly, John et al. 30 also found a smaller proportion of females than males and speculated that the low rate among the women might be due to the culturally inculcated restrictions among Indian women. On the contrary, Khisty et al. 19 and Dickens and Campbell 4 did not find any significant difference between absconding cases in men and women. Cultural shift over time or difference in the setting might have caused this finding. 19
While Gowda et al. 24 found that most patients who absconded belonged to lower socioeconomic status, our study did not find any such difference between the groups. In our study, most of the patients in the absconding group belonged to joint or extended family. In contrast, Gowda et al. 24 had found that most of them belonged to a nuclear family.
The absconding patients and the controls did not differ in the age of onset, duration of illness, history of past treatment, history of psychiatric or medical illness, history of family illnesses, or the presence of forensic history.
Factors Related to Absconding (N = 38)
A significantly higher proportion of patients who absconded had irritable affect both at the time of admission and around the time of absconding. Also, those who absconded had less perceptual abnormalities than controls at admission, which could explain the absence of perceptual abnormality among the absconding cases at the time of absconding too. This is consistent with Khisty et al. 19 who speculated that being more guarded than controls might be the reason why they were less likely to report hallucinations.
There was a significant difference in judgment and insight around the event of absconding between the groups. Patients of the absconding group had grade I insight around the time of absconding, while the patients of the control group had shown improvement to have grade II or better insight (P < 0.001). A recent study from a psychiatric hospital in India also found a higher prevalence of absconding among patients who had an absent insight. 24
About 10% of cases had a history of prior absconding from the hospital in the previous admissions. This proportion is less than what was found by Meehan et al., 40 who found that one-third of those who absconded had a similar history in their previous hospitalizations. The reason behind this discrepancy might be the improvement in the psychiatric management of inpatients, including the physical structure and environment of the psychiatric care facility.
Most of the events occurred during the daytime and early morning or evening hours, as compared to early morning clustering observed in another study. 40 Khisty et al. 19 found that most incidents occurred during the daytime (09:00 hr to 18:00 hr) Several factors might contribute to this. Leaving the hospital ward may be easier during the daytime because at that time, almost in any hospital, much more people move around or visit, thereby making it less difficult to make way for the exit. Dickens and Campbell 4 reasoned that often, at nighttime, even open wards are locked by night staff, which seems to be relevant in our study too. A literature review 3 did not find any common patterns, which might be due to the variations in the hospitals, organization of shifts among hospitals, settings, hospital protocols, and countries.
The most common mean chosen for absconding was scaling through the boundary wall, followed by escaping through the main gate, manipulating other patients or their guardians, during a referral to other medical centers for physical illness, and by manipulating the workers. A study by Yasini et al. 33 found that high numbers of absconding take place from the main door of the hospital, followed by other sites (walls, windows, etc.). Agreeing with previous researchers, we speculate that increased staffing would help by improving the monitoring and observation of inpatients and the understanding of their psychological and nursing care needs.33, 41
Our study suffered from a few limitations. For about one-third of the absconding cases, the means chosen to abscond were not shared by the patients and hence could not be recorded. Reasons for absconding have not been examined as well in our study. Qualitative information could not be examined. We included a modest period of observation of five years only. Limitations of a retrospective design based on CRF review need a mention.
Conclusion
Most of the inpatients who absconded were male, from a younger age group, from joint or extended family, diagnosed with schizophrenia or mood disorder, and having comorbid substance use disorder, irritable affect, impaired judgment, and absent insight. Most incidents of absconding happened during the first two weeks following admission. About one-tenth of those who absconded had a similar history. Most of the events occurred during daytime and early morning or evening hours, and the most common means chosen were scaling the boundary wall and passing through the main gate. Our study adds to the existing sparse literature on the nature and pattern of absconding and the profile of those inpatients who abscond from a psychiatric hospital. Further research should focus on this event with a longer period of observation and should include qualitative design. This would lead to a more effective risk assessment in psychiatric inpatient care and facilitate reintegration into the community.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.