
Abstract
Severe systemic right ventricular failure with tricuspid regurgitation is associated with poor prognosis. Here, we report a case of 49-year-old patient who experienced severe systemic right ventricular failure following atrial switch. We chose the surgical strategy for this challenging case using comprehensive four-dimensional imaging. The patient underwent tricuspid valve repair and cardiac resynchronization therapy and recovered with improved cardiac function and regulated tricuspid valve regurgitation.
Keywords
Introduction
Severe systemic right ventricular failure with tricuspid regurgitation (TR) has a poor prognosis. 1 Although heart transplantation is the gold standard for heart failure in adult congenital heart disease, its long-term prognosis is not necessarily satisfactory owing to several complications.
We describe a 49-year-old patient with severe systemic right ventricular failure who was successfully treated with tricuspid valve repair concomitant with cardiac resynchronization therapy defibrillator (CRT-D) implantation using four-dimensional (4D) imaging.
Case study
He was diagnosed with dextro-transposition of the great arteries with ventricular septal defect (VSD) just after birth. He underwent Mustard technique with a fenestrated VSD patch closure at the age of 14.
Recently, he presented with sudden ventricular fibrillation requiring extracorporeal cardiopulmonary resuscitation. Fortunately, he recovered and discharged home with a wearable cardiac defibrillator. Electrocardiogram (ECG) showed atrial fibrillation with an elongated and fragmented QRS complex to 148 ms, and echocardiography revealed moderate tricuspid valve regurgitation due to coaptation failure in the anteroseptal commissure and annular dilatation (Figure 1(a) and (b)). The systemic right ventricular function was severely impaired with dys-synchrony with contraction delay (Figure 2(a)). Furthermore, 4D flow magnetic resonance imaging (MRI) revealed severe systemic right ventricular failure: ejection fraction of 37.3%; end-diastolic volume index of 147.4 ml/m2; end-systolic volume index of 92.5 ml/m2; and cardiac index of 2.40 L/min/m2, but no flow acceleration on the Mustard route (Figure 3(a) to (c)). Contrast-enhanced ECG-gated computed tomography (CT) revealed that the noncoronary sinus of the transposed aortic root was firmly adherent to the sternum. Considering the extreme risk of resternotomy, prior cardiopulmonary bypass was initiated with right femoral arterial perfusion and right internal jugular and femoral venous drainage.
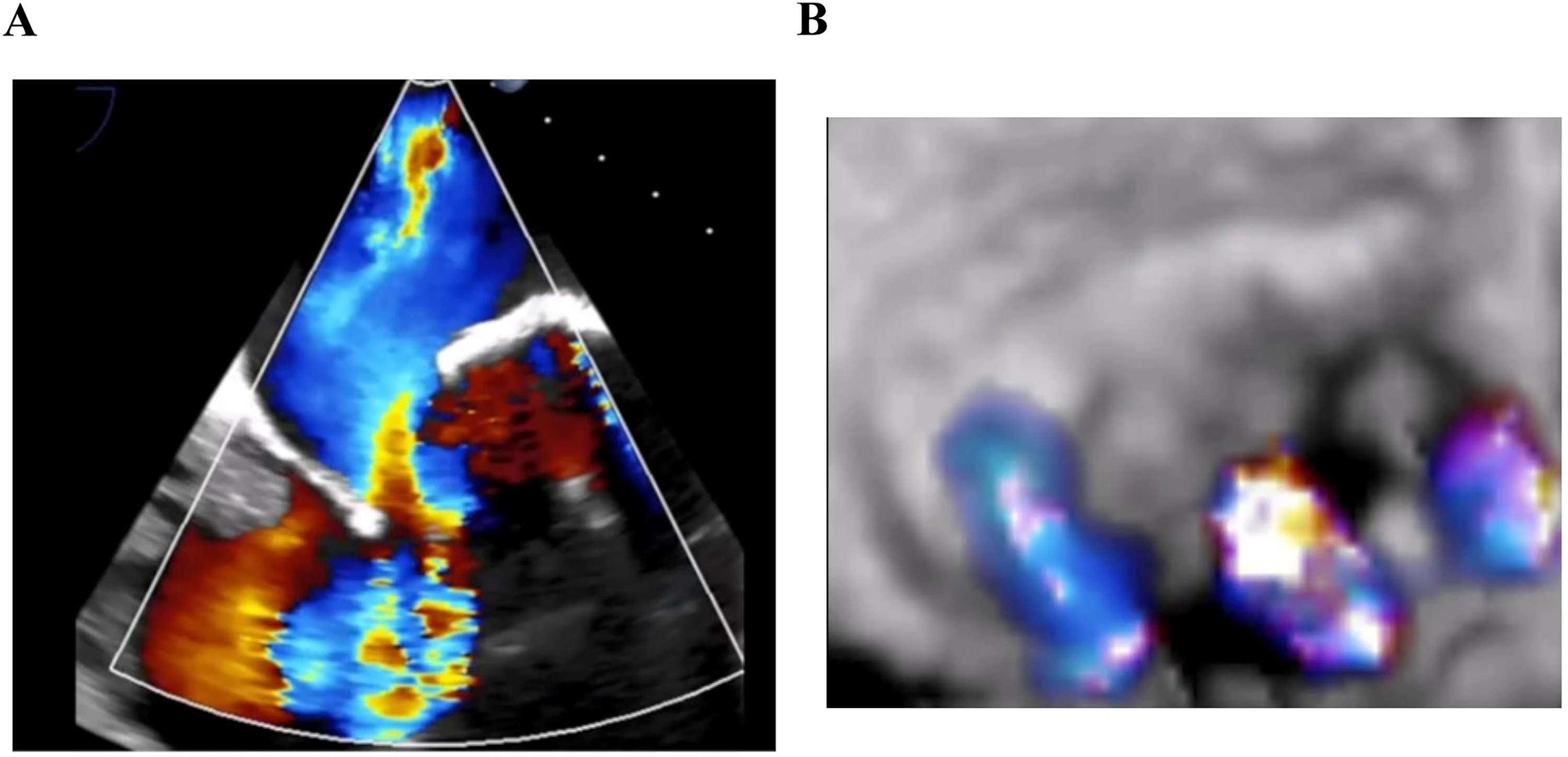
(a) Preoperative echocardiography shows moderate to severe systemic tricuspid regurgitation with prolapse. (b) Systemic tricuspid valve of preoperative three-dimensional echocardiography.
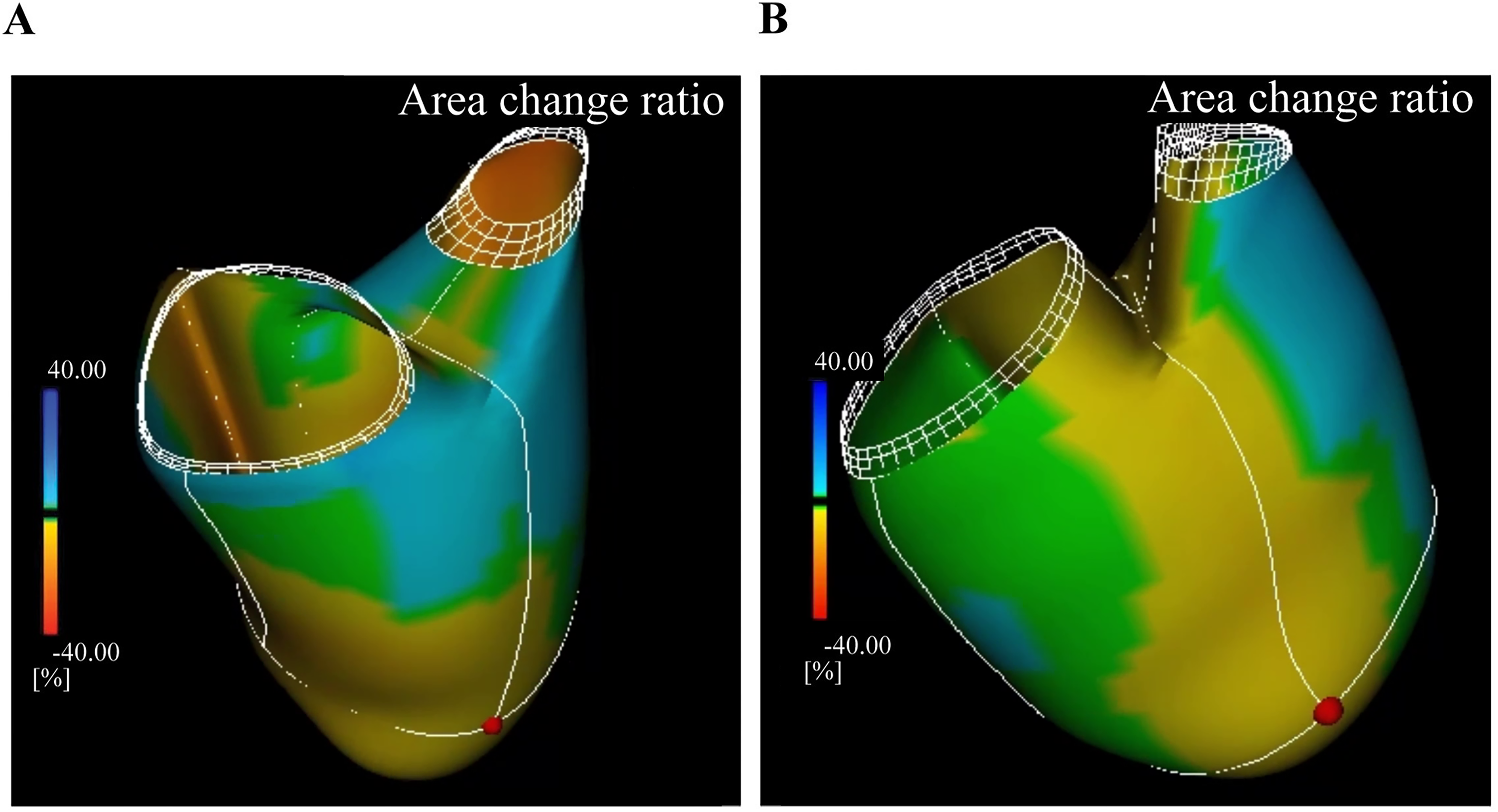
(a) Color map of preoperative speckle tracking echocardiography shows systemic right ventricular function was severely impaired with dys-synchrony. (b) Color map indicate the propagation of the contraction site, which successfully resynchronized after the cardiac resynchronization therapy (CRT) pacing.
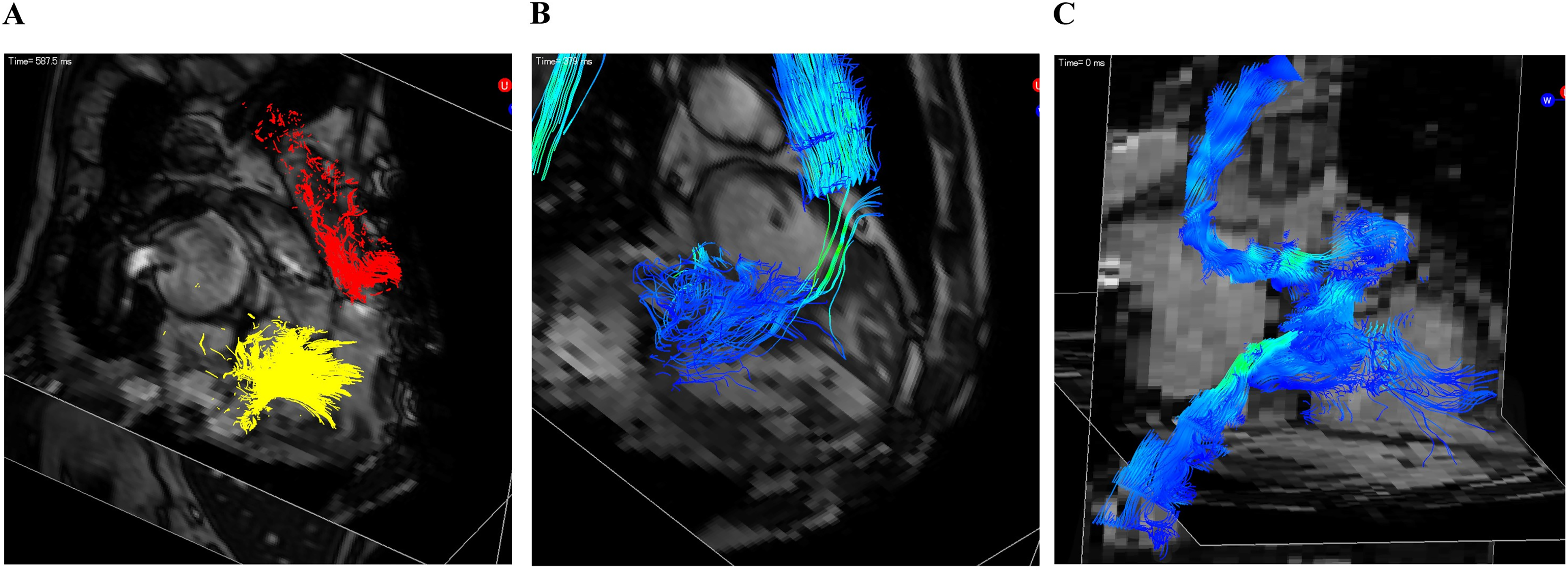
Four-dimensional (4D) flow magnetic resonance imaging (MRI) enable comprehensive assessment of hemodynamics and cardiac function including chamber size, valve regurgitation, and abnormal flow acceleration in systemic and pulmonary circulation. (a) Systemic pathline of preoperative 4D flow MRI shows reverse flow in trans tricuspid flow (TR flow). (b) Systemic streamline of preoperative 4D flow MRI shows the site and extent of accelerated flow. (c) Pulmonary streamline of preoperative 4D flow MRI shows no flow acceleration on the Mustard route.
Because the anteriorly located ascending aorta was densely adhered to the sternum, and injured during resternotomy, the aorta was smoothly clamped and repaired using a bovine pericardial patch and replaced with the Dacron graft under the circulatoyr arrest (Figure 4(a)). Through right-sided atriotomy, edge-to-edge commissuroplasty was performed with the annuloplasty using a 27-mm Tailor flexible ring (St Jude Medical, Inc., St Paul, MN, USA) to control the TR (Figure 4(b)). Preoperative 3D speckle tracking echocardiography was used to confirm synchronicity and positional adjustment of the epicardial pacing for the biventricular pacing, and a shock lead to the left atrial roof on the right side of the aortic root (Figure 4(c)). Cardiopulmonary bypass was weaned with intra-aortic balloon pumping support.
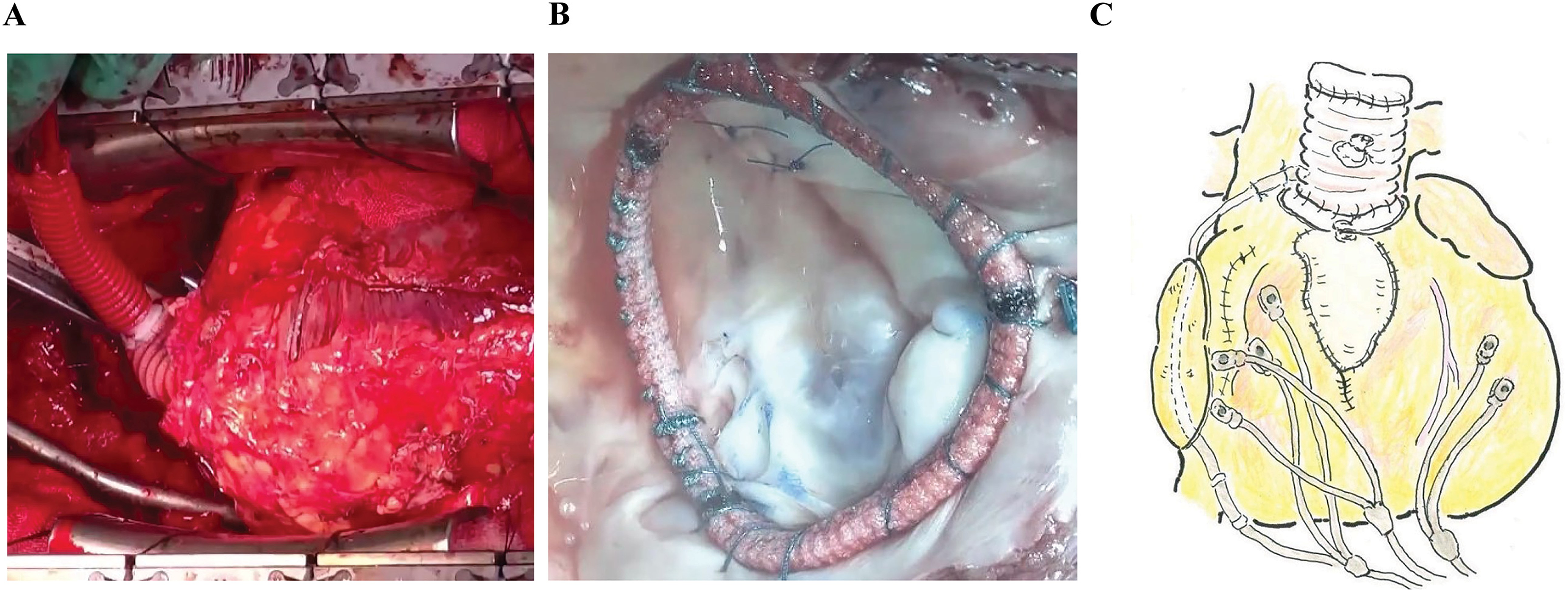
(a) Intraoperative photography. The injured nonfacing sinus was repaired using a patch and artificial graft. (b) Intraoperative photography of the systemic tricuspid valve; annuloplasty performed with artificial ring. (c) Surgical schema.
In postoperative echocardiography, TR was reduced to mild, and biventricular synchronicity improved, resulting in systemic right ventricular chamber reduction (Figure 2(b)). He recovered well and was extubated on postoperative day 4 and was discharged six weeks later. Four months after the discharge, he returned to work, and at the six-month follow-up, he worked fine with preserved cardiac function and regulated tricuspid valve regurgitation, without the recurrence of ventricular arrhythmia.
Discussion
We decided surgical strategy for this challenging case using comprehensive 4D imaging, including 4D flow MRI, ECG-gated enhanced CT, and echocardiography speckle tracking.
Four-dimensional flow MRI revealed the systemic right ventricular function and TR hemodynamics, in addition to the evaluation of the Mustard route hemodynamics. 2 Computed tomography provides anatomical information; therefore, it is useful for the assessment of reoperation, including resternotomy and cardiopulmonary bypass access, particularly drainage to the Mustard rerouting venous system and approach to the tricuspid valve. Although the limitation is that electrophysiological study was not implemented, resynchronization can be obtained by pacing both ventricles almost simultaneously based on echocardiography speckle tracking, compensating for the electrical delay.
Although the systemic tricuspid valve repair is considered slightly challenging with no high success rates, 1 appropriate patient selection of the valve status, particularly less cusp degeneration, failure of coaptation, and enough tethering height, is necessary. 3 Flexible rings can effectively reduce regurgitation without compromising valve leaflet mobility and can withstand systemic circulation for reliable durability.
In conclusion, CRT treatment and appropriate tricuspid valve repair can improve cardiac function.3,4 This can delay the timing of heart transplantation, thereby resulting in a better prognosis; therefore, our surgical strategy is a potent bridge treatment for heart transplantation.
Footnotes
Acknowledgements
The authors are grateful to Dr Yoshihiro Seo and Dr Shohei Kikuchi in the department of Cardiology, Nagoya City University Graduate School of Medical Sciences for their detailed assessment and advises in 3D speckle tracking echocardiography and electrophysiological study in the determination process of CRT pacing in the present case.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The corresponding author K.I. has a following conflicts of interest associated with this manuscript: A Stock Option from Cardio Flow Design Inc., which delivers blood flow imaging tools.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fundings from the Japanese governmental research grants for 4D imaging tools described in the present manuscript from the Japan Society for the Promotion of Science, KAKEN, from the Japan Agency for Medical Research and Development, AMED; and from the Japan Science and Technology Agency technology, JST.
Ethical approval
Not applicable.
Informed consent
Not applicable. The Institutional Review Board of Nagoya city university graduate school of medical sciences and medical school waived the need for individual ethical review and patient consent.