
Abstract
Background
We hypothesized that academic facilities and high-volume facilities would be independently associated with improved survival and a greater propensity for performing surgery in locally advanced esophageal cancer.
Methods
We identified patients diagnosed with stage IB–III esophageal cancer during 2004–2016 from the National Cancer Database. Facility type was categorized as academic or community, and facility volume was based on the number of times a facility's unique identification code appeared in the dataset. Each facility type was dichotomized into high- and low-volume subgroups using the cutoff of 20 esophageal cancers treated/year. We fitted multivariable regression models in order to assess differences in surgery selection and survival between facilities according to type and volume.
Results
Compared to patients treated at high-volume community hospitals, those at high-volume academic facilities were more likely to undergo surgery (odds ratio: 1.865, p < 0.001) and were associated with lower odds of death (odds ratio: 0.784, p = 0.004). For both academic and community hospitals, patients at high-volume facilities were more likely to undergo surgery compared to those at low-volume facilities, p < 0.05. For patients treated at academic facilities, high-volume facilities were associated with lower odds of death (odds ratio: 0.858, p = 0.02) compared to low-volume facilities, while there was no significant difference in the odds of death between high- and low-volume community hospitals (odds ratio: 1.018, p = 0.87).
Conclusions
Both facility type and case volume impact surgery selection and survival in locally advanced esophageal cancer. Compared to community hospitals, academic facilities were more likely to perform surgery and were associated with improved survival.
Introduction
Esophageal cancer is a relatively uncommon malignancy that is associated with significant mortality, as evidenced by a historical five-year relative survival of below 20%. 1 Approximately 18,500 new cases of esophageal cancer were diagnosed in the United States in 2020, with an estimated 33% of those patients having regional spread to the lymph nodes at the time of diagnosis. 1 Surgery as part of a multimodality approach has been associated with the best outcomes in selected patients with locally advanced esophageal cancer.2–4 Despite this, surgical treatment is likely underutilized in the management of such patients.5,6 In a previous National Cancer Database (NCDB) analysis, only 45% of stage II and 39% of stage III patients underwent surgical resection in 2013, with the rest receiving definitive chemoradiotherapy. 7 In particular, community centers were linked with a reduced likelihood of performing surgery for stage II and III disease (odds ratio for academic versus community centers: 2.42, p < 0.001). 7 Unlike surgery selection, survival outcomes have seldom been studied in the context of facility type in esophageal cancer. Additionally, although the positive correlation between facility volume and survival outcomes for patients with esophageal cancer is well-documented,8,9 whether this relationship holds true for both academic and community centers remains uncertain.
In the present study, we stratified academic and community facilities by case volume. This enabled us to address the primary objective of the study: to investigate the independent effects of facility type and case volume on surgery selection and survival outcomes in patients with locally advanced esophageal cancer. We hypothesized that academic facilities and high-volume facilities would be independently associated with a greater propensity for performing surgery and improved survival. We also hypothesized that patients undergoing surgery at high-volume academic facilities have superior perioperative outcomes compared to those undergoing surgery at high-volume community centers.
The NCDB is the largest cancer registry in the world that currently captures 72% of all newly diagnosed malignancies annually in the United States from more than 1500 Commission on Cancer-approved facilities. 10 We utilized this contemporary nationwide patient cohort to independently assess facility type and case volume in a specific, yet large subset of esophageal cancer patients. To the best of our knowledge, this is the first study on esophageal cancer to stratify facility type by case volume in order to investigate surgery selection, perioperative outcomes, and survival.
Patients and methods
Data source
The NCDB is a joint project of the Commission on Cancer of the American College of Surgeons and the American Cancer Society. Institutional Review Board exemption was granted for this analysis.
Selection of study population
In this retrospective cohort study, we queried the NCDB for patients diagnosed with American Joint Committee on Cancer (AJCC) clinical stage IB, II, or III esophageal cancer during the years 2004–2016, excluding those with cervical tumors. The AJCC staging edition applicable at the time of diagnosis (AJCC 6 or 7) was used to report clinical stage. We also excluded patients who were diagnosed and treated at separate facilities in order to attribute surgery selection and survival outcomes to the facility that treated the patient.
Variables
A) Covariates
We included the following variables in our analysis: age at diagnosis (<50, 50–59, 60–69, 70–79, ≥80), sex (male, female), race (white, black, other), Charlson-Deyo comorbidity score (0, 1, 2, ≥3), insurance status (private, government, none), AJCC clinical stage (IB, II, III), tumor histology (squamous cell carcinoma, adenocarcinoma, other), county of residence (metropolitan, urban, rural), type of treatment received (upfront surgery ± adjuvant chemotherapy/chemoradiotherapy, induction chemotherapy/chemoradiotherapy + surgery ± adjuvant chemotherapy/chemoradiotherapy, definitive chemoradiotherapy, no treatment, other treatment), type of operative approach (minimally invasive, open, no surgery, unknown), and type of diagnosing facility (academic, community, Integrated Network Cancer Program).
The NCDB categorizes facilities into 10 different program types but includes the four largest ones in the available participant user file: Community Cancer Program, Comprehensive Community Cancer Program, Academic/Research Program, and Integrated Network Cancer Program. We dichotomized cases from Academic/Research Programs, Community Cancer Programs, and Comprehensive Community Cancer Programs into academic and community facility types. We included Integrated Network Cancer Programs in the overall cohort but did not categorize them as either academic or community facilities since it is not clear whether these facilities are academic or community facilities from the definition given by the NCDB (Supplemental Table 1). 11
B) Outcome measures
Outcome measures included surgery selection, which was defined as the odds of undergoing surgery, either alone or as part of a multimodality approach, and survival, defined as the odds of death. Perioperative outcome measures included positive surgical margins (defined as the presence of microscopic or macroscopic residual tumor), examination of ≥15 lymph nodes during surgery, 30-day mortality, 90-day mortality, and unplanned readmission within 30 days of surgical discharge.
Statistical analysis
We used SPSS Statistical software version 25 (IBM SPSS Statistics for Macintosh, Version 25.0; IBM Corp, Armonk, NY) for all statistical analyses. We used the default, listwise deletion, for missing data. We calculated summary statistics to determine baseline characteristics according to the type of treatment facility. We determined univariate differences between those being treated at academic facilities and those treated at community facilities using the Pearson chi-square test for categorical variables. We also used the Pearson chi-square test to assess group differences between patients included in the analysis (who underwent treatment at the diagnosing facility) and those excluded from the sample (who underwent treatment at an alternate facility).
We used multivariable logistic regression to compare surgery selection between academic and community facilities. We included the following variables in the logistic regression model on the basis of a priori hypotheses: age at diagnosis, sex, race, Charlson-Deyo comorbidity score, clinical stage, tumor histology, insurance status, and residence county. We also performed multivariable logistic regression to compare survival, with death as a dichotomous variable, between academic and community facilities. We included the following variables in the logistic regression model on the basis of a priori hypotheses: age at diagnosis, sex, race, Charlson-Deyo comorbidity score, clinical stage, tumor histology, insurance status, residence county, type of treatment received, and type of operative approach.
A) Impact of facility case volume on surgery selection and survival
In order to investigate the impact of facility case volume on surgery selection and survival, we separately dichotomized academic and community facilities into high- and low-volume subgroups using the cutoff of 20 esophageal cancers treated per year. This cutoff has been used previously by others and has been associated with mortality in esophageal cancer.12–14 We based facility case volume on the number of times a facility's unique identification code appeared in the dataset. We fitted multivariable logistic regression models to compare surgery selection and survival between high- and low-volume academic facilities and between high- and low-volume community facilities after adjusting for the previously mentioned potential confounders.
B) Impact of facility type on surgery selection and survival
In order to investigate the impact of facility type on surgery selection and survival, we performed similar adjusted analyses to compare surgery selection and survival between academic high-volume facilities and community high-volume facilities. We also utilized multivariable logistic regression models to compare perioperative outcomes between surgically treated patients at high-volume academic and high-volume community facilities. A p-value of less than 0.05 was used to declare statistical significance.
Results
Baseline characteristics according to the type of diagnosing facility
Our study included 22,485 patients with clinical stage IB, II, or III esophageal cancer. Compared to community hospitals, academic facilities had a greater proportion of younger patients and black patients. Academic facilities also had a greater proportion of those with stage III disease, squamous cell carcinoma, a Charlson-Deyo comorbidity score of 0, private insurance, patients residing in metropolitan counties, and patients undergoing surgery (Table 1).
Comparison of baseline characteristics of locally advanced esophageal cancer patients according to the type of diagnosing facility.
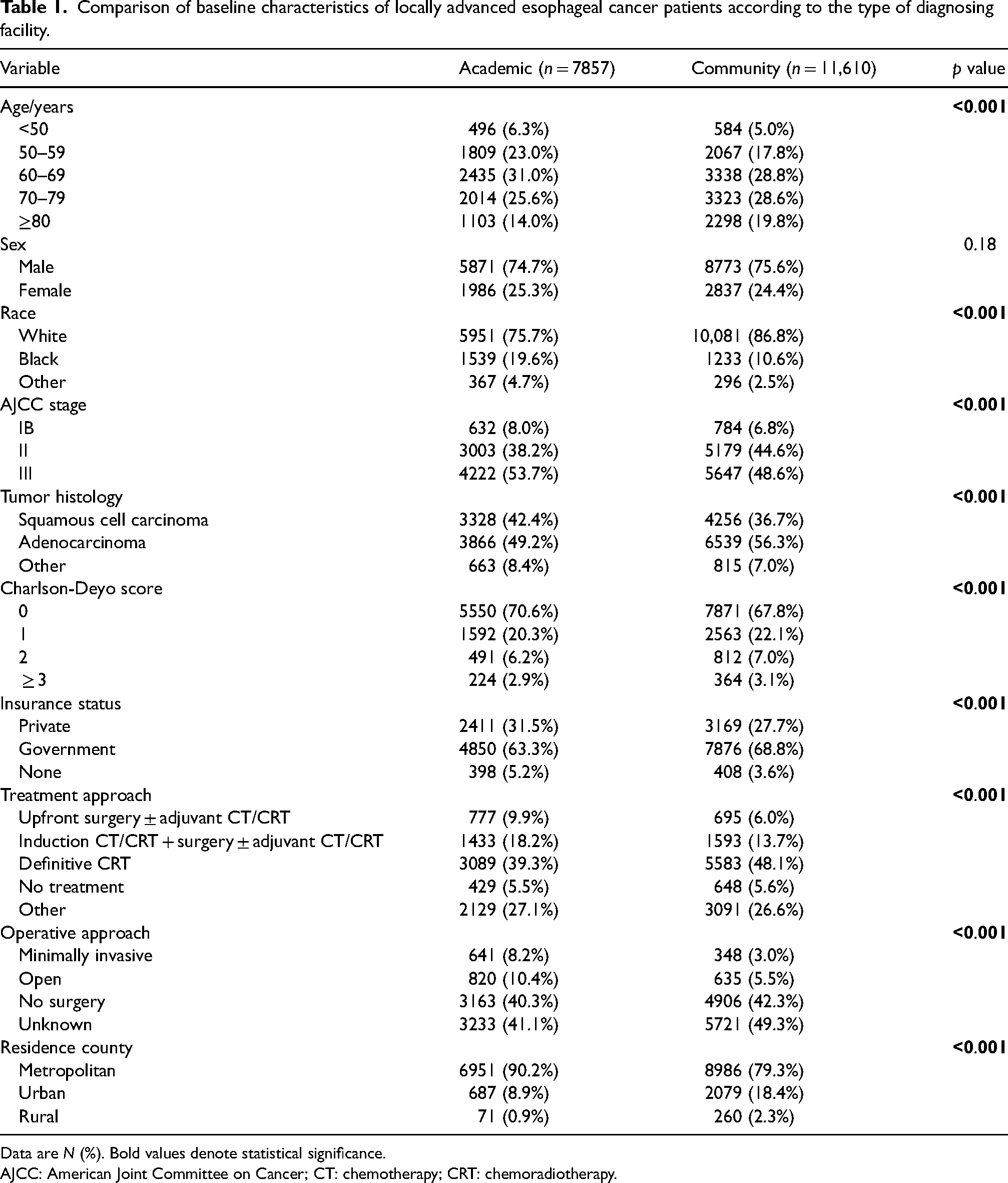
Data are N (%). Bold values denote statistical significance.
AJCC: American Joint Committee on Cancer; CT: chemotherapy; CRT: chemoradiotherapy.
Predictors of surgery selection and survival in the whole cohort
Compared to academic facilities, community hospitals were less likely to perform surgery (adjusted odds ratio [aOR]: 0.550, p < 0.001). Compared to academic facilities, community hospitals were also associated with greater odds of death (aOR: 1.230, p < 0.001) (Table 2).
Results of the multivariable logistic regression showing predictors of surgery and predictors of death in locally advanced esophageal cancer.
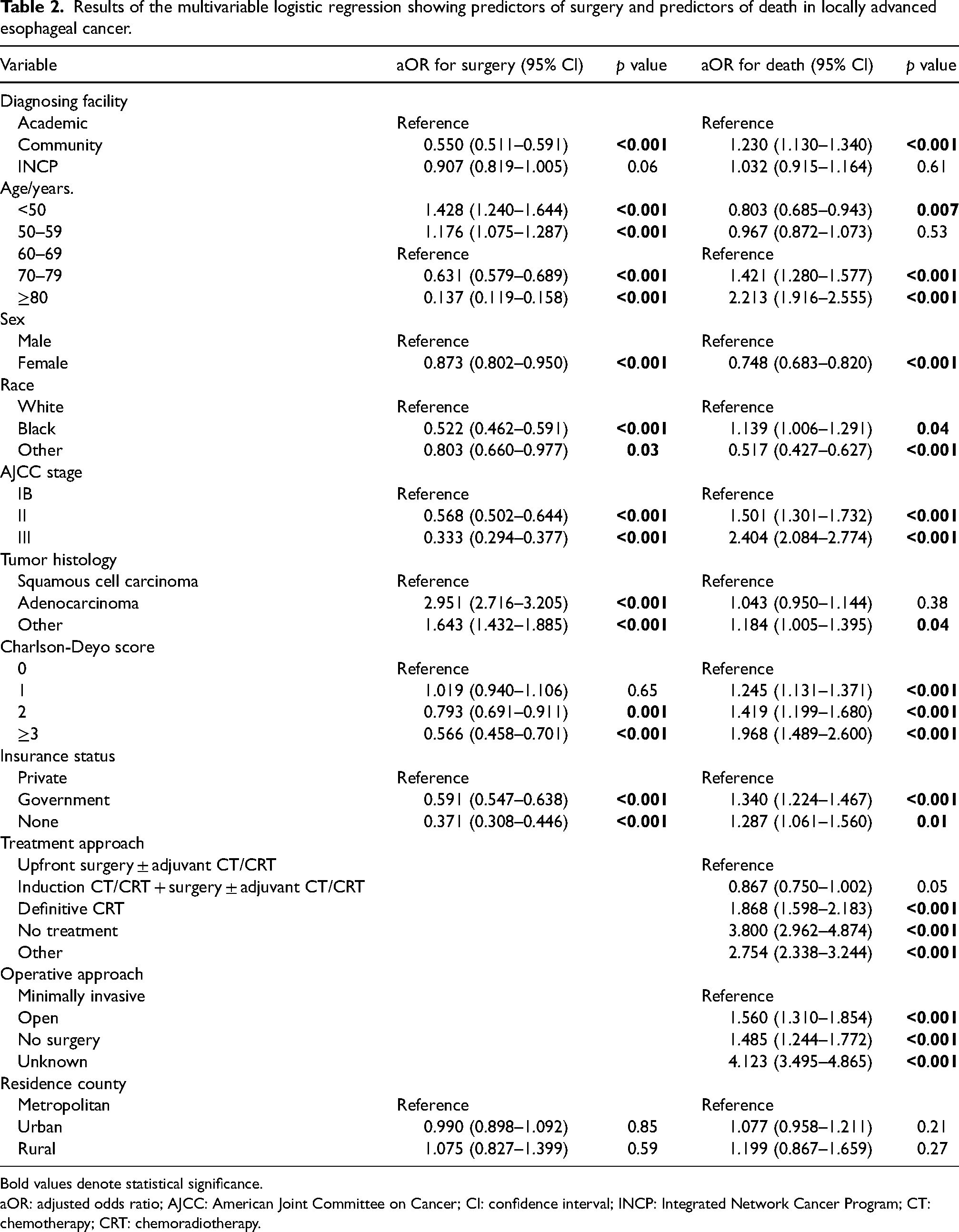
Bold values denote statistical significance.
aOR: adjusted odds ratio; AJCC: American Joint Committee on Cancer; CI: confidence interval; INCP: Integrated Network Cancer Program; CT: chemotherapy; CRT: chemoradiotherapy.
Impact of diagnosing facility case volume on surgery selection and survival outcomes
The composition of the study population stratified by type of diagnosing facility and case volume is shown in Table 3. The results of the multivariable logistic regression showed that high-volume facilities were independently more likely to perform surgery than low-volume facilities for both academic and community facilities after controlling for hypothesized confounders (p < 0.05) (Table 4). Compared to low-volume academic facilities, high-volume academic facilities were associated with lower odds of death (aOR: 0.858, p = 0.02). However, there was no statistically significant difference in the odds of death between high- and low-volume community facilities (aOR: 1.018, p = 0.87) (Table 4).
Composition of the study population stratified by type of diagnosing facility and case volume.
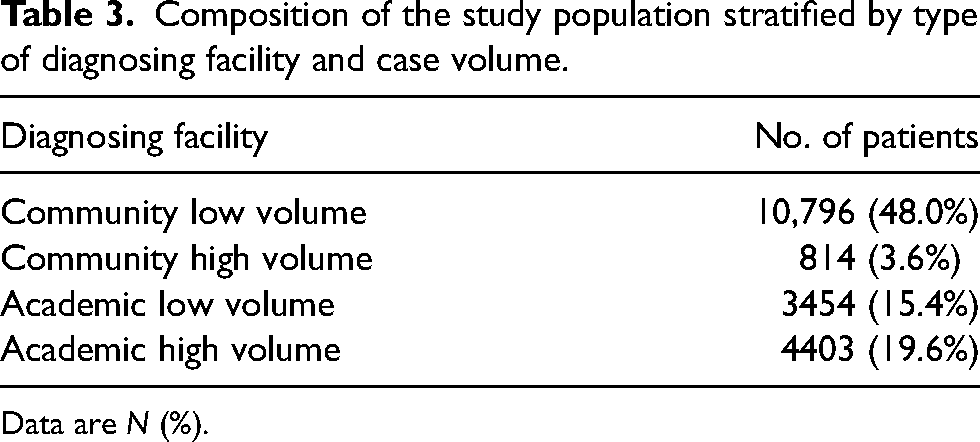
Data are N (%).
Adjusted odds ratios of performing surgery and adjusted odds ratios of death for high- vs. low-volume facilities for each type of diagnosing facility.
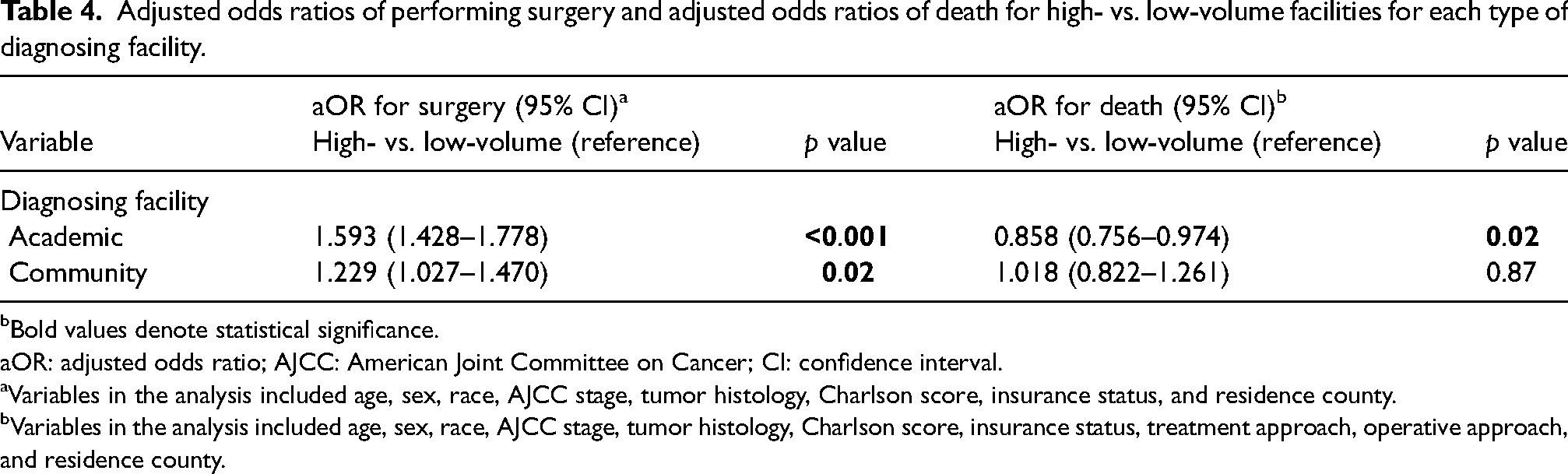
Bold values denote statistical significance.
aOR: adjusted odds ratio; AJCC: American Joint Committee on Cancer; CI: confidence interval.
Variables in the analysis included age, sex, race, AJCC stage, tumor histology, Charlson score, insurance status, and residence county.
Variables in the analysis included age, sex, race, AJCC stage, tumor histology, Charlson score, insurance status, treatment approach, operative approach, and residence county.
Impact of the type of diagnosing facility on surgery selection and survival
High-volume academic and high-volume community facilities were compared to investigate the impact of facility type on surgery selection and survival. Compared to high-volume community facilities, high-volume academic facilities were more likely to perform surgery (aOR: 1.865, p < 0.001) and were associated with lower odds of death (aOR: 0.784, p = 0.004) after controlling for hypothesized confounders (Table 5).
Adjusted odds ratio of performing surgery and adjusted odds ratio of death for academic high-volume vs. community high-volume facilities.
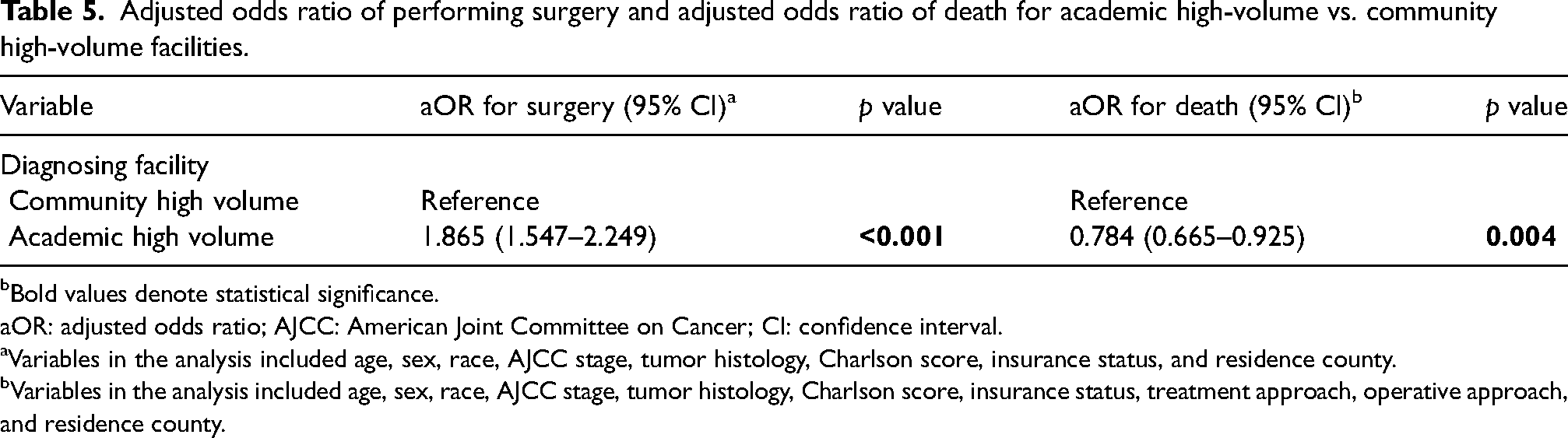
Bold values denote statistical significance.
aOR: adjusted odds ratio; AJCC: American Joint Committee on Cancer; CI: confidence interval.
Variables in the analysis included age, sex, race, AJCC stage, tumor histology, Charlson score, insurance status, and residence county.
Variables in the analysis included age, sex, race, AJCC stage, tumor histology, Charlson score, insurance status, treatment approach, operative approach, and residence county.
Impact of the type of diagnosing facility on perioperative outcomes
We compared outcomes between surgically treated patients at high-volume academic and high-volume community facilities after controlling for hypothesized confounders (Table 6). Compared to those treated at community facilities, patients at academic facilities had lower odds of death within 30 days of discharge (aOR: 0.564, p = 0.04), while academic facilities were more likely to examine ≥15 lymph nodes during surgery (aOR: 1.572, p < 0.001). There was no statistically significant difference in the likelihood of death within 90 days of discharge, unplanned readmission, and positive surgical margins (p > 0.05).
Multivariable logistic regression analysis of the cohort of surgically treated patients showing adjusted perioperative outcomes for high-volume academic versus high-volume community facilities (reference).
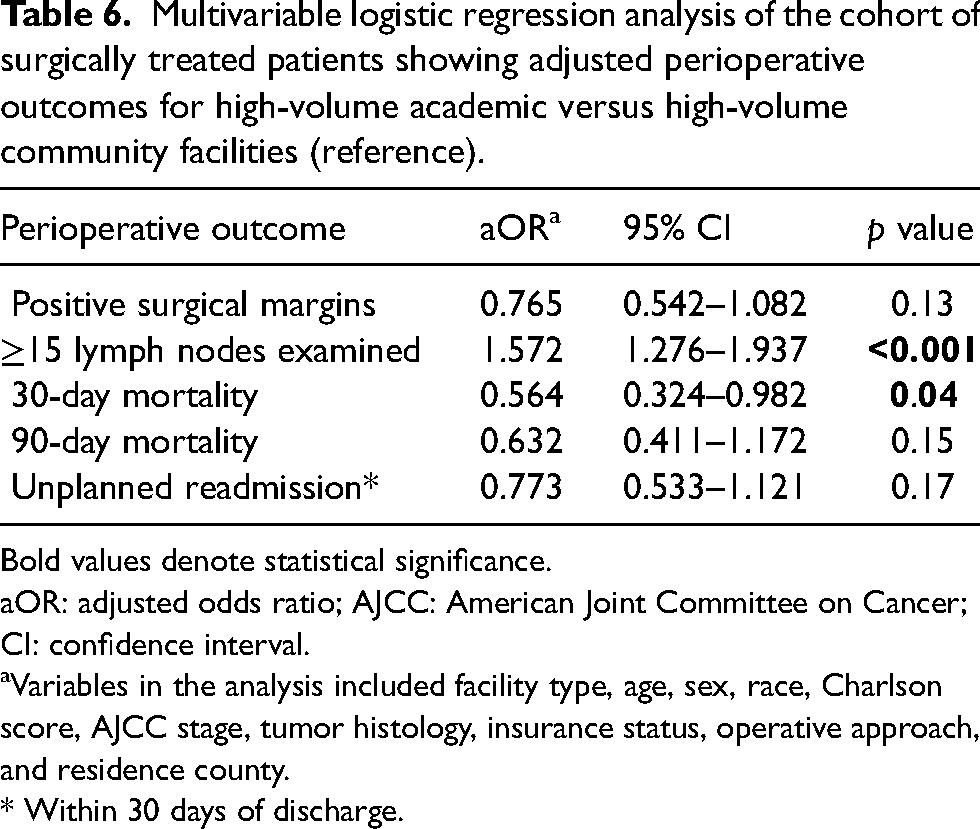
Bold values denote statistical significance.
aOR: adjusted odds ratio; AJCC: American Joint Committee on Cancer; CI: confidence interval.
Variables in the analysis included facility type, age, sex, race, Charlson score, AJCC stage, tumor histology, insurance status, operative approach, and residence county.
* Within 30 days of discharge.
Group differences between patients treated at diagnosing facility and those diagnosed and treated at separate facilities
Supplemental Tables 2–5 show the results of the analyses assessing group differences between those treated at the diagnosing facility and those who were excluded from the study cohort as they were diagnosed and treated at separate facilities. The group of patients that was excluded had a greater proportion of patients diagnosed at academic facilities and high-volume facilities.
Discussion
Several previous studies have cited higher facility case volume alone as the primary driver for superior outcomes in esophageal cancer.8,9,15 The results of the current study suggest that patients with locally advanced esophageal cancer presenting at academic facilities are more likely to undergo surgery and experience superior survival outcomes compared to those presenting at community hospitals. Our results are significant, in that these findings persisted at high-volume centers and indicate that teaching facility status of the diagnosing facility independently impacts surgery selection and survival. Patients diagnosed at academic facilities experienced better outcomes that were independent from simply being more likely to undergo surgery. This was evidenced by favorable perioperative outcomes in the group undergoing surgery at academic facilities compared to those undergoing surgery at community hospitals. Lastly, the case volume of the diagnosing facility was an independent predictor of survival for academic facilities, but not for community hospitals.
In the present study, academic facilities and high-volume facilities were independently associated with greater surgery selection. For academic facilities, improved survival outcomes were seen in facilities that had a higher likelihood of performing surgery. Despite this, our results showed an overall surgery rate of 28% for locally advanced esophageal cancer. A prior Surveillance, Epidemiology, and End Results (SEER) analysis of stage I–III esophageal cancer reported an overall surgery rate of 34%, 5 while Taylor and colleagues observed an overall surgery rate of 36% for clinical stage 0–III esophageal cancer. 7 Similarly, Merritt and colleagues observed a 26% surgery rate at community facilities and a 49% surgery rate at academic facilities. 16 The factors contributing to these low surgery rates are likely multifactorial. In addition to community facility status and low case volume, these factors may include a lack of awareness of guideline-concordant care, 7 reluctance to operate in older patients or those with multiple comorbidities, 6 socioeconomic barriers to ideal treatment, low individual surgeon case volume, 6 and the absence of subspecialists such as general thoracic surgeons and surgical, medical, and radiation oncologists.
In our study, advanced age and a higher Charlson score correlated with a lower likelihood of surgery, while social determinants such as race and insurance status also impacted surgery selection. Even after adjusting for these factors, academic facility type and high facility case volume remained independent predictors of surgical treatment. It is possible that these facilities offer greater access to experienced esophageal surgeons and advanced postoperative care, and this drives an increase in the number of esophagectomies performed. 16
Facility case volume was not an independent predictor of overall survival in our study. Although high overall case volume successfully correlated with a higher likelihood of surgery in both academic and community facilities, it was only associated with improved survival in academic facilities. Our results can be likened to those of Rodgers et al., who analyzed case volume as a predictor of inpatient mortality after esophagectomy in a review of the Nationwide Inpatient Sample. 17 The inclusion of surgeon volume in their multivariate analysis eliminated the independent effect of facility case volume on mortality, while in our study the stratification of facility type by case volume also suggests that facility case volume may not independently impact survival. Our findings indicate that teaching facility status has a greater influence on outcomes than case volume. Given the multidisciplinary nature of advanced cancer care, it is plausible that the addition of postgraduate oncology and surgery training programs at academic centers facilitates greater interdisciplinary coordination of care and contributes to better patient outcomes.18,19
There are several limitations to this study. The retrospective nature of the analysis is prone to selection bias that is difficult to fully control with the use of multivariable models. In addition, our conclusions only apply to patients who were diagnosed and treated at the same facility since we excluded patients who were diagnosed and treated at separate facilities in order to avoid attributing surgery selection and survival outcomes to a facility that diagnosed but did not treat the patient. We were also unable to investigate and adjust for individual surgeon case volume in our analyses since this information is not included in the NCDB, while important clinical information such as specific comorbidities, performance status, and results of pulmonary function tests were also unavailable and would have influenced surgery selection and survival. Another factor to consider is the impact of an intrathoracic versus cervical anastomotic leak on morbidity and mortality, which we were also unable to account for given the limitations of the database. The distribution of patients following the stratification of facilities by case volume was also disproportionate, ranging from 3% at high-volume community facilities to 48% at low-volume community facilities, which may limit the generalizability of our results. Lastly, although the NCDB provides time-to-death information, the assumption of proportional hazards was violated, which precluded any adjusted survival analyses.
Conclusion
Both facility teaching status and case volume of the diagnosing facility impacted surgery selection and survival in locally advanced esophageal cancer patients. Compared to community hospitals, academic facilities were more likely to perform surgery and were associated with improved perioperative outcomes and survival. Subsequent efforts to improve outcomes in patients with locally advanced esophageal cancer should be directed at better elucidating the factors responsible for the higher likelihood of surgery and improved survival at academic facilities and determining if these factors can be replicated in a community setting since the majority of patients presented to community hospitals in the present study.
Supplemental Material
sj-docx-1-aan-10.1177_02184923231215539 - Supplemental material for Impact of facility type and volume in locally advanced esophageal cancer
Supplemental material, sj-docx-1-aan-10.1177_02184923231215539 for Impact of facility type and volume in locally advanced esophageal cancer by Zaid Muslim, Stephanie Stroever, Kostantinos Poulikidis, Cliff P Connery, James R Nitzkorski and Faiz Y Bhora in Asian Cardiovascular and Thoracic Annals
Footnotes
Acknowledgements
The data used in the study are derived from a de-identified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigator.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board exemption was granted by Biomedical Research Alliance of New York (BRANY) (Investigator Initiated Protocol # 21-505/BRANY File # 21-15-213-337) for this analysis.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.