
Abstract
Background
The bidirectional Glenn (BDG) shunt operation serves as temporary surgery for the treatment of single-ventricle physiology with the eventual Fontan procedure. In some cases, the procedure can be performed without the support of a cardiopulmonary bypass (CPB) machine. In this study, we present the surgical outcomes of off-pump BDG operation with the use of a temporary veno-atrial shunt to decompress the superior vena cava (SVC) during clamping time.
Methods
A cohort of 23 patients underwent off-pump BDG operations at Cardiovascular Center, E Hospital. All patients were operated on using a veno-atrial shunt to decompress the SVC.
Results
Satisfactory results with mean oxygen saturation increased from 79.6 ± 11.2% to 87.2 ± 4.7%. The SVC clamping time was 14 ± 2.4 min (ranging from 12 to 21 min). Among 23 patients, only six patients required blood transfusion, 17 patients had BDG without blood transfusion. No neurological complications or deaths occurred after the surgery, and the post-operative period was uneventful.
Conclusions
The use of veno-atrial shunts to decompress SVC during off-pump BDG operation is safe with good surgical outcomes and can avoid the deleterious effects caused by CPB. It is easily reproducible, at low cost and economically effective.
Keywords
Introduction
Bidirectional Glenn (BDG) shunt institution is often indicated as the initial step in the treatment of functional single-ventricle physiology before the completion of the Fontan procedure. The purpose of this surgery is to provide balanced venous blood flow into two pulmonary arteries for the oxygenating process instead of mixed arteriovenous blood as in Blalock–Taussig shunt surgery (aortopulmonary shunt) while avoiding the volume overload of the left ventricle. The BDG operation is conventionally performed with the support of cardiopulmonary bypass (CPB) at the expense of higher costs and disadvantages of CPB. Therefore, in the world, there has been a variety of reports on BDG operations without CPB. 1 However, there have been no official reports on this issue in Vietnam. In this study, we present the surgical protocol to perform off-pump BDG operation using the superior vena cava-right atrium (SVC-RA) pressure lowering system and the early outcomes of this newly applied technique.
Patients and methods
Subjects
Patients who had indications for BDG operation without any intracardiac defects requiring correction: pulmonary artery (PA) plasty, atrial septal extension, atrioventricular valvuloplasty, etc. The patient underwent a thorough clinical workup: Clinical examination (evaluating the severity of heart failure using NYHA classification, the level of cyanosis), SpO2 and medical history.
Laboratory testings
− Routine blood tests, electrocardiography (ECG), chest x-ray,
− Echocardiography: evaluate left ventricular function, abnormal wall motion, chambers size, the functional status of heart valves and PA size.
− Cardiac catheterization: measure PA size, anatomy, pressure and resistance.
Definitive diagnosis was established based on physical examination, Doppler echocardiography, cardiac catheterization, blood tests, ECG and chest x-ray. Surgical consultation, hospital admission and preoperative medical therapy were provided for the patient. When preoperative conditions had been assured, the patients underwent surgery according to the same protocol in anesthesia, operative techniques and post-operative resuscitation. In the operating room, hemodynamic parameters were monitored and recorded.
Surgical procedure
General anesthesia, intubation
The patients were premedicated with Midazolam, Fentanyl and Rocuronium. Patients were on controlled mechanical ventilation with Vt = 150 mL and a respiratory rate of 18 per minute. The anesthesia was maintained by Isoflurane, Fentanyl and Rocuronium. A femoral vein catheter was placed for drug use and monitoring the right atrial pressure. A right internal jugular vein catheter was inserted for SVC pressure monitoring. An invasive arterial pressure line was also put in place.
Surgical procedures
Whole body antiseptic application, from the chest to two legs
Median sternotomy
Dissect the SVC and ligate the azygos vein
Dissect the right branch of PA, measure PA pressure
Set up the system to decrease SVC-PA pressure
All of the patients underwent the Glenn procedure with an internal shunt (veno-atrial shunt), in which a shunt was established between the distal SVC and the RA. A cannula of standard size, matched to the patient's age and weight, was used by the surgeon for the procedure.
The upper and lower catheters were connected to a three-way connection. After clamping the SVC, the SVC was decompressed by opening the three-way connection, allowing blood to flow passively due to the pressure gradient. However, if the SVC pressure increased above 40 mm Hg, a 50-mL syringe was connected to the three-way connection with sterile precautions to avoid air. Blood was actively aspirated from the upper catheter and injected into the lower catheter around 10–20 times per minute. These maneuvers were performed carefully to avoid any air and effectively lowered the SVC pressure (Figure 1).
Trial right PA clamp for several minutes to check the changes in transcutaneous oxygen saturation (SpO2). Systemic heparin with a dose of 1 mg/kg to achieve the ACT of more than 200 s. Set up the system to decrease SVC-PA pressure with the head of the patients elevated 15°, inject methylprednisolone (20 mg/kg) intravenously, SVC clamp to anastomose with right PA, maintain the difference between mean arterial pressure and mean SVC pressure during clamping higher than 40 mm Hg. During surgery, hemodynamic stability was maintained by fluid replacement and inotropes: adrenaline 0.1 mcg/kg/min and milrinone 0.3 mcg/kg/min.
Make end-to-side SVC-PA anastomosis by 7.0 prolene suture
Remove cannula, achieve hemostasis, insert drains, electrodes and close the pericardium if possible.
Close the sternotomy by steel suture, soft tissue was closed using running suture or interrupted absorbable suture in patients with high risks of infection.
Post-operative care
In the intensive care unit, echocardiography and routine laboratory tests (complete blood count, electrolytes, arterial blood gases, …) were done. All complications and actions taken were recorded. After the ICU stay, patients were transferred to Pediatric Cardiology Department for further treatment until discharge.
Results
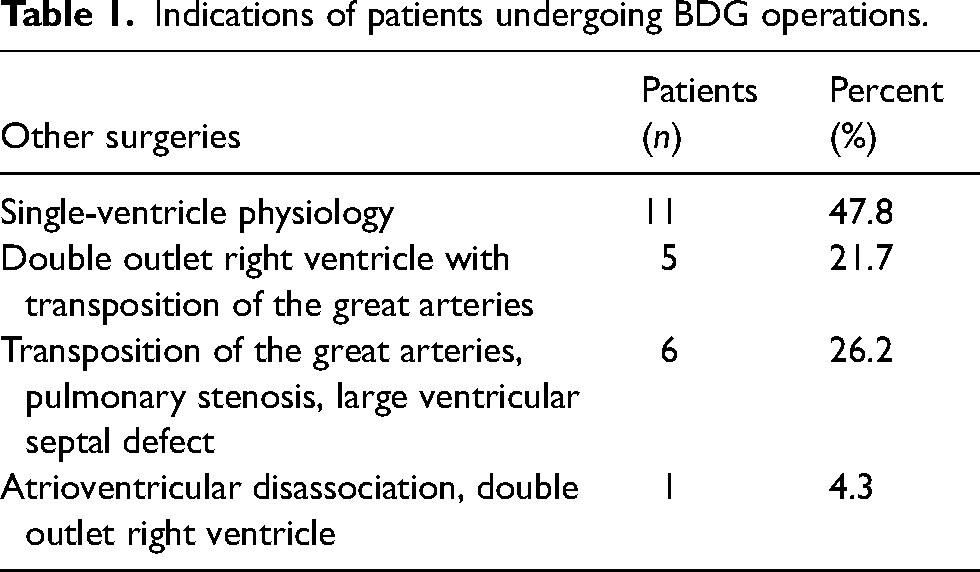
The study consists of 23 patients who underwent off-pump BDG operation at E Hospital, Hanoi, Vietnam. Among 23 patients, only six patients required blood transfusion, 17 patients had BDG without blood transfusion. The mean age was 48 months (range 5–180 months). The mean SVC clamp time was 14 ± 2.4 min (ranging from 12 to 21 min). During clamping, the mean central venous pressure ranged from 24 to 40 mm Hg (average 31.5 ± 6.1 mm Hg). Preoperative PA pressure was 11–25 mm Hg (average 16.3 ± 3.2 mm Hg). There was no conversion to the CPB machine. Indications of patients undergoing BDG operations are summarized in Table 1.
Indications of patients undergoing BDG operations.
The mean ventilator time after surgery was 2.6 ± 1.2 h (1–6 h), the ICU length of stay was 13.2 ± 3.1 (10–18 h), and no death occurred. Echocardiography evaluation at discharge showed no anastomosis stenosis and post-operative ECG revealed no arrhythmia. The mean post-operative PA pressure was 13.6 ± 2.5 mm Hg.
The hospital length of stay ranged from 6 to 9 days (average 7.1 ± 1.3 days). Echocardiography showed no significant pressure gradient through the SVC-RPA anastomosis with good velocity of blood flow, ECG showed normal sinus rhythm in all patients, and no neurological complications were recorded.
Comments
Off-pump BDG operation without a temporary shunt to decompress the SVC will cause the elevation in cerebral blood volume, leading to increased intracranial pressure and eventually resulting in reduced blood flow to the brain and damage to the neurological system. Several studies documented the decrease in oxyhemoglobin in brain tissue, a 50% reduction in blood flow in the middle cerebral artery with significant changes in encephalography. Rodriguez proved that clamping the SVC would decrease the systolic pressure of cerebral arteries and subsequently decrease the oxygen supply to the brain.2–4 To avoid such disadvantages, there were many reports on the use of a temporary shunt to decompress the SVC and improve the perfusion of the brain.
Table 2 is the summary of studies in the past 15 years of authors from all over the world on BDG operations without CBP. Lamberti polished his research on seven patients in 1990 and after that, there were a series of studies by other authors on off-pump BDG surgery.1,5,6 Until now, there have been no official reports on this technique in Vietnam.
Researches on off-pump BDG surgery.
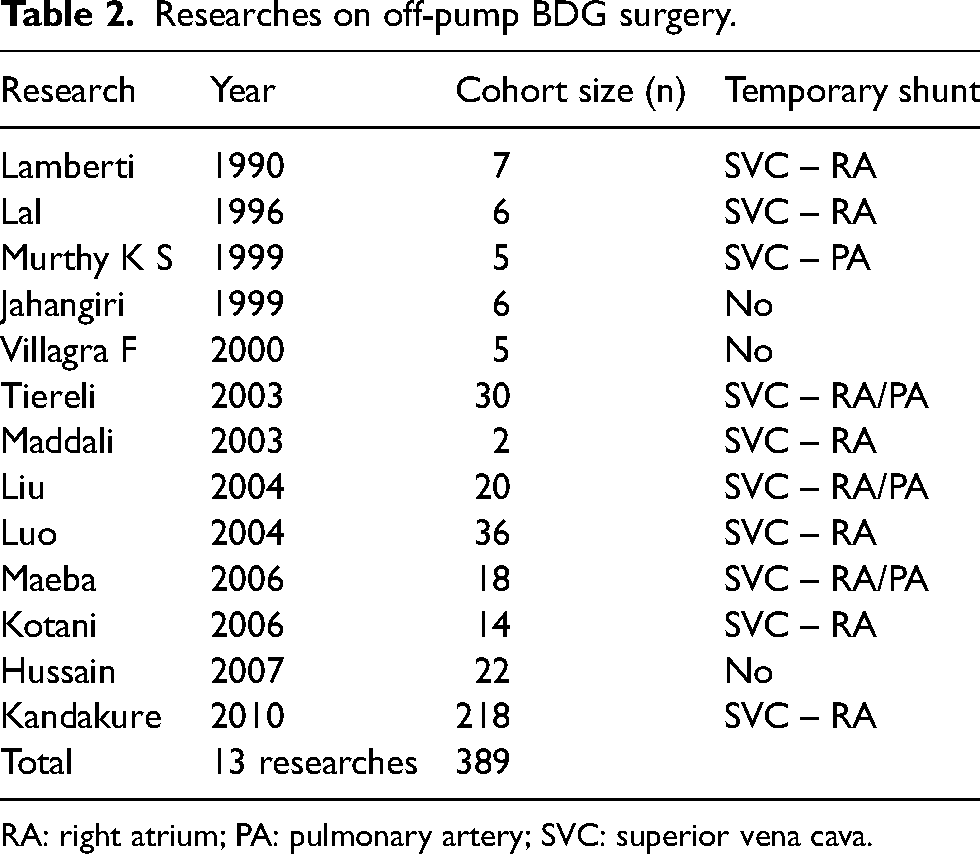
RA: right atrium; PA: pulmonary artery; SVC: superior vena cava.
In the study of Ulisses Alezandre Crotti, 7 the mean age of the on-pump group was 66 months and that of the off-pump group was 50 months (p = 0.17 using the Mann–Whitney test). This result means that the differences in age, gender, weight and types of defects between the on-pump and the off-pump groups are not important factors in choosing the use of peripheral circulation.
The choice of a temporary shunt to establish depends on the experience and the ability of the surgeons, anesthesiologists and the settings of each surgical center. Our technique uses the temporary veno-atrial shunt with the following steps: place a venous graft at the junction of the SVC and azygos vein, which effectively decrease the pressure of the clamped SVC and avoid the possibility of SVC stenosis. In addition, the head-elevated position during operation facilitates the adequate decompression of SVC and provides enough space for the surgical field.
According to our experience, with the veno-atrial shunt, SVC pressure after clamping did not exceed 40 mm Hg. Post-operative chylothorax and dysfunction of the diaphragm with low incidences because with our technique, the dissect field of SVC was short; avoid the injury to the phrenic nerve and the surrounding lymphatics. Performing Glenn operation on patients who already had a Blalock–Taussig shunt or patent ductus arteriosus (PDA) was more convenient due to the aortopulmonary shunt continuously supplying blood for the lungs during the reconstruction of Glenn anastomosis and maintaining the good stable oxygen saturation. The choice of SVC and atrial cannula size was based on the size of the patients’ SVC and RA, besides size choosing according to the patient's weight, and skin area in CPB. During surgery, the cooperation between surgeons and anesthesiologists is the key to a successful off-pump BDG operation. 8
During SVC clamping, the blood flow to the brain is reduced, therefore, to maintain good cerebral perfusion during off-pump BDG surgery, the authors proposed the concept of transcranial pressure, which is the difference between mean arterial pressure and mean SVC pressure during SVC clamping (transcranial pressure = mean arterial pressure – central venous pressure). 9 This pressure had to be maintained at a minimum of 30 mm Hg during SVC clamping to assure adequate cerebral perfusion. Veno-atrial shunt reduced SVC pressure and improved cerebral perfusion.3,4 In addition, during the procedure, the SVC is clamped and the proximal pressures can rise as high as 40 to 55 mm Hg. This impairs blood flow to the brain and judicious use of inotropes to increase the mean arterial pressure was indicated. Maintaining the transcranial pressure greater than 30–40 mm Hg was expected to maintain adequate cerebral perfusion. 10
Elhaddad compared the result of the external shunt with the result of the internal shunt (veno-atrial). In group I, using the veno-atrial shunt, the results during clamping show that the mean SO2 was 71.3 ± 1.5, the mean SVC pressure before opening the shunt was 40.4 ± 3.4, while after opening the shunt 28.5 ± 3.8. The result in group E was nearly similar to group I, the mean SO2 was 69.6 ± 3.1, the mean SVC pressure before opening the shunt was 37.6 ± 4.5, while after opening the shunt was 26.4 ± 2.1 and there were no post-operative neurologic complications. 11
Monitor parameters of brain function to provide additional information about hemodynamic effects on the brain tissue of SVC clamping could be based on transcranial Doppler ultrasound, near-infrared spectroscopy and encephalography. 8 However, these tests are not routinely available; therefore, the monitoring of brain function was mainly based on the mean arterial pressure and central venous pressure.
The use of corticosteroids aimed to minimalize brain edema and neurological insults. Body temperature was kept at approximately 33–34°C in order to reduce the metabolism of brain cells to adjust with the reduced pressure of cerebral blood flow due to SVC clamping. Inotropes and crystalloid replacement were used to maintain adequate cerebral blood flow and a transcranial pressure higher than 30 mm Hg during SVC clamping. 12
Hypoxia was regulated by the increased fraction of inspiratory oxygen (FiO2), and mean arterial pressure was also increased by using inotropes and providing enough circulating fluid. Therefore, the blood flow to the lung was secured.
Post-operative treatment was aimed at decreasing pulmonary vascular resistance and increasing blood return to SVC. Pulmonary dilation medications (milrinone, iloprost …) helped to decrease pulmonary arterial pressure and end-diastolic left ventricular pressure. 1 Prolonged mechanical ventilation time resulted in increased intrathoracic pressure and negatively affected the blood return to SVC and blood flow through the shunt, early weaning and extubation helped to avoid the above-mentioned disorders. The mean time on the ventilator in our study was 2.6 ± 1.2 h (1–6 h), which is comparable to other studies. 1 Short ventilatory time is also a big advantage of off-pump BDG operation compared to conventional BDG surgery with CPB.2,3,13 The mean duration to extubation of the off-pump group was 3 h and that of the on-pump group was 11 h (p = 0.83). The mean length of stay in the ICH was 3 days and 5 days in the on-pump and off-pump groups, respectively (p = 0.29). The average hospital length of stay of the former group was 9 days, of the latter group was 5 days and of the whole study group was 7 days.
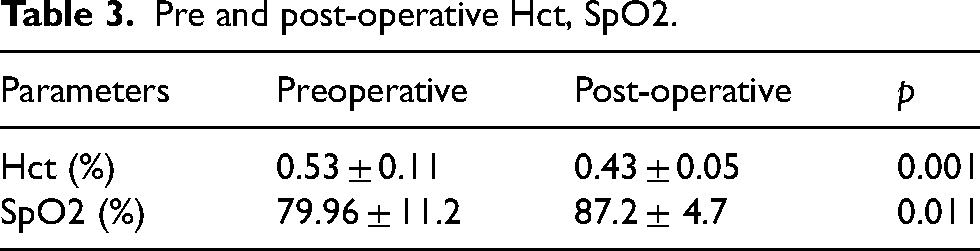
In this study, all cases had shunt that supplied blood to the lungs: PDA, collaterals, aortopulmonary shunt (Blalock–Taussig) had the shunt ligated to avoid the increased left ventricular afterload, improve cardiac function and decrease the severity of atrioventricular valve regurgitation. 6 The mean post-operative pulmonary arterial pressure was 13.6 ± 2.5 mm Hg, which was the ideal pressure after BDG operation. According to Tables 2 and 3, the oxygen saturation was significantly improved after surgery (p < 0.011), and the hematocrit decreased substantially post-operatively (p < 0.001). In 23 studied subjects, there were six cases with early post-operative complications, accounting for 26.1% (Table 4), and one case with more than one complication. According to Chang et al., 6 the incidences of post-operative complications such as SVC syndrome, low cardiac output syndrome and arrhythmia were high, while in research in our center and by other authors, 14 the incidences of the above-mentioned complications were very low. There was no bleeding event that required reoperation in our study, in other studies, this complication occurred in 6% of cases. There was a case that required reoperation: 3 days after BDG surgery, facial edema occurred and echocardiography revealed thrombi inside SVC. In reoperation, we found that there were thrombi along with the central venous catheter and at the Glenn anastomosis. The thrombi were removed and the central venous catheter was replaced. The reason for thrombi formation may be in the previous surgery, during the separation of SVC we cut a part of the central venous catheter that lies in the RA (a catheter that is too long will cause difficulty for operation and cannot measure SVC pressure). In general, the incidences of post-operative complications in our study are comparable to or lower than other studies.13,15
Pre and post-operative Hct, SpO2.
Post-operative complications.
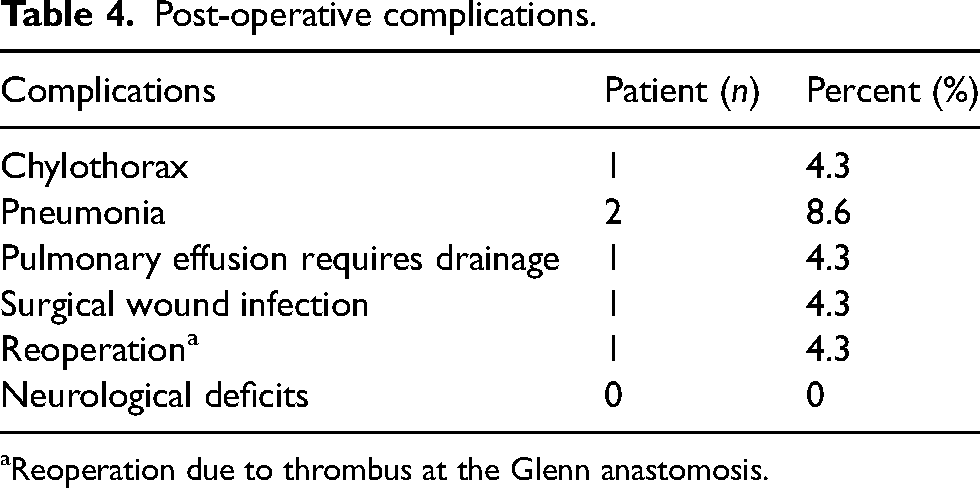
Reoperation due to thrombus at the Glenn anastomosis.
In our study, there were no deaths in the off-pump group and two deaths in the on-pump group. There were no cases of chylothorax in the off-pump group but eight patients in the on-pump group suffered from this complication. Only two patients in the off-pump group had early complications and the number in the on-pump group is 14. One advantage of the Glenn procedure without peripheral circulation is the significant reduction in post-surgical complications compared to the on-pump group. The rates of hemorrhage requiring reoperation in the two groups are significantly different (p = 0.044); the rate of chylothorax in the on-pump group is significantly higher than that of the off-pump group (p < 0.01). The early mortality rates of the on-pump and the off-pump groups are 0% and 4%, respectively. The causes of death in the on-pump group were low cardiac output syndrome, heart failure and neurological complications. Comparing the results from this study, we concluded that the off-pump group had a better post-operative recovery, shorter time on the mechanical ventilator, shorter length of stay in ICU and in the hospital and fewer post-surgical complications compared to the on-pump Glenn procedure.
Without CPB, patients can avoid unwanted effects: increased pulmonary vascular resistance, blood dilution, air embolism and other undesirable effects. Tireli et al. 16 in 2003, in his research, confirmed that in off-pump BDG operations, pulmonary arterial pressure was lower and the hospital length of stay of the off-pump group was shorter than the on-pump group. All patients were on heparin in the first 24 h, and aspirin was used subsequently. Patients were monitored regularly and all of them maintained good oxygen saturation, no neurological complications occurred.
It is still unclear that performing the BDG without the use of CPB can provide protection to the brain. Jahangiri and associates described seven patients who underwent placement of BDG without the use of CPB or any form of decompressing shunt. Rodriguez and coworkers found the blood flow velocity in the MCA decreased by 50% with clamping of the SVC. In a second study, Rodriguez and associates also found significant electroencephalogram changes during SVC clamping.9–17
Clamping the SVC without of temporary shunt can lead to decreased cerebral blood flow and put the brain at risk. Therefore, a temporary shunt is not only necessary during the procedure but also a suitable size cannula is needed to avoid higher SVC pressure. The clamping time should also be kept as brief as possible. Additionally, BDG without CPB is reasonable if SVC pressure is less than 40 mm Hg and clamping time is less than 30 min.
Medical cost is always a concern of every healthcare system. According to the Syed Tarique Hussain report in India in 2007, the cost of an on-pump BDG surgery is 1200 USA and that of an off-pump BDG operation is only 250 USA. 12 To date, the cost of a BDG shunt institution with CPB (2500$) is 7 times higher than that of the same operation without CPB (300$) at our Cardiovascular Center. The off-pump BDG operation technique reduced the cost by avoiding the use of CPB, decreasing the use of blood products, and the suctioning system is reusable after sterilization according to the protocol. The post-operative period and hospital length of stay were shorter, the rates of pulmonary effusion, chylothorax and diaphragm paralysis were lower and no neurological complications were documented.
Conclusions
The study investigates the safety and post-operation results of 23 patients who underwent off-pump BDG shunt, at Cardiovascular Center—E Hospital, we concluded that off-pump BDG operation using veno-atrial shunt to decompress the SVC was safe with satisfactory early surgical outcomes. This technique can avoid the complication caused by CPB, significantly improve oxygen saturation, improve the quality of life and reduce mortality rate after the Fotan procedure, easily reproducible and have high cost-effectiveness.
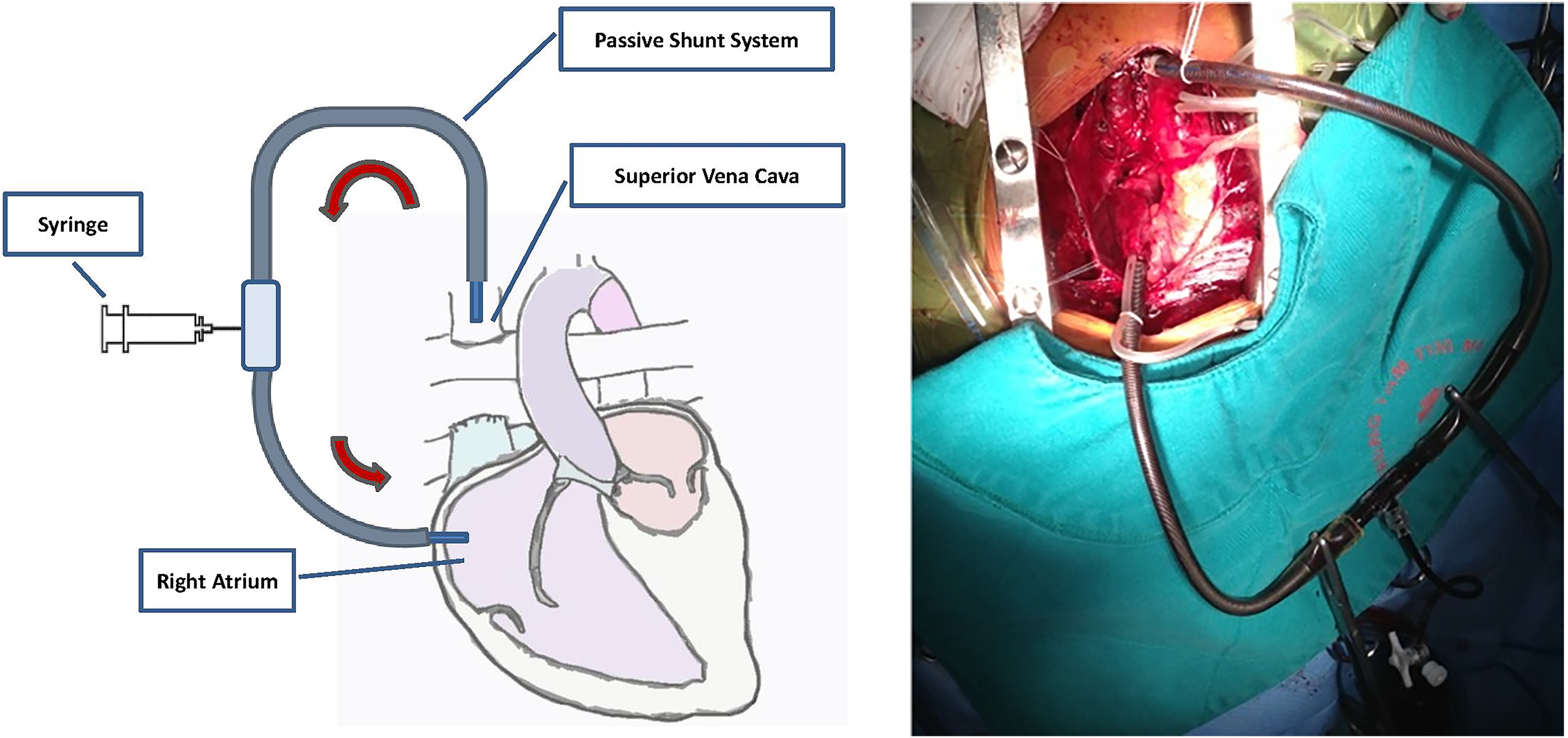
Description of a veno-atrial shunt used in our technique. SVC: superior vena cava; RPA: right pulmonary artery; LPA: left pulmonary artery; RA: right atrium.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the ethics committee of National E Hospital, Vietnam and was conducted in accordance with the Declaration of Helsinki.
Informed consent
The need for informed consent was waived by the ethics committee of National E Hospital, Vietnam. We have obtained written consent to publish from the patient to publish. No identifiable information was disclosed in any form.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.