
Abstract
Background
It remains unclear whether the Rho-kinase (ROCK) inhibition in combination with mechanical circulatory support (MCS) had a synergic protective effect on myocardial ischemia (MI)/reperfusion injury in therapeutic strategies for acute myocardial infarction (AMI). We report the results of an approach using a rat model consisting of a miniaturized cardiopulmonary bypass (CPB) and AMI.
Methods
A total of 25 male Wistar rats were randomized into 5 groups: (1) Sham: a suture was passed under the left anterior descending artery (LAD) creating no MI. A vehicle solution (0.9% saline) was injected intraperitoneally. (2) Myocardial ischemia (MI) + vehicle (MI + V): LAD was ligated for 30 min and reperfused for 120 min, followed by administration of vehicle solution. (3) MI + fasudil (MI + F): the work sequence of group 2, but the selective ROCK inhibitor fasudil (10 mg/kg) was administered instead. (4) MI + V + CPB: CPB was initiated 15 min after the ligation of the LAD to the end of the reperfusion, in addition to the work sequence in group 2. (5) In the MI + F + CPB group, the work sequence of group 4, but with fasudil administration (10 mg/kg).
Results
Measurements of cardiac function through conductance catheter indicated that the drop of + dP/dt after reperfusion was moderately limited in MI + F + CPB (vs. MI + V, dP/dt p = 0.22). The preload recruitable stroke work was moderately improved in the MI + F + CPB (p = 0.23) compared with the corresponding control animals (MI + V). Phosphorylated protein kinase B expression in the MI + V + CPB and MI + F + CPB was higher than that in MI + V (p = 0.33).
Conclusion
Therefore, fasudil administration with MCS resulted in a moderately better left ventricular performance.
Keywords
Introduction
Currently, ischemic heart disease is a significant cause of morbidity and mortality, and in particular, acute myocardial infarction (AMI) is a common acute condition with a high mortality rate. 1 Despite substantial basic and clinical research in the past, the mortality rate of patients who develop cardiogenic shock caused by AMI remains as high as 40% to 50%. 2 Although early revascularization results in better survival in patients with AMI complicated with cardiogenic shock, 3 20% to 30% of patients with AMI ultimately develop heart failure. 4 The process of restoring blood flow to the ischemic myocardium can further aggravate the amount of myocardial injury even after successful revascularization. This phenomenon, termed as myocardial ischemia/reperfusion (I/R) injury, can paradoxically reduce the beneficial effects of myocardial reperfusion. Increasing evidence suggests that multiple factors are involved in I/R injuries, such as calcium ions (Ca2+) overload, oxygen-free radical injury, cytokine production, and neutrophil infiltration. 5 The transmission of extracellular stress signals into an intracellular response has been reported to involve small guanosine-59-triphosphate-binding proteins such as those of the Rho family. Rho-kinase (ROCK) has been identified as a downstream effector of Rho. According to the emergence of the role of the ROCK pathway, the indications of ROCK inhibitors have been expanding in cardiovascular medicine.6–9
Underlying clinical background for application of extracorporeal circulation
Currently, extracorporeal life support is indicated in various intensive treatments for patients with the circulatory collapse that is refractory to conventional treatment.10,11 This therapeutic strategy also provides beneficial results in patients with severe progressive cardiogenic shock after AMI with global myocardial involvement. 12 With regard to balancing the risk of cardiac death, these outcomes might be attributed to the function of mechanically secured circulation with ventricular unloading and controlled reperfusion. Therefore, a therapeutic strategy of cardiopulmonary bypass (CPB)-assisted primary revascularization has a potential benefit in this clinical setting. However, a considerable proportion of patients, who still have prolonged myocardial impairment after cardiac revascularization, require lifelong mechanical circulatory support (MCS), for example, ventricular assist device implantation, or inotropic agents. 13
This study aimed to explore whether the ROCK inhibitor in combination with MCS immediately after the onset of the AMI had a synergic protective effect on myocardial I/R injury and contributed to maintaining myocardial contractility. 14
Materials and methods
Ethics
This study was approved by the responsible third-party belonging to the local authority LANUV (Landesamt für Natur, Umwelt und Verbraucherschutz NRW, Germany) (AZ84-02.04.2017. A289) and conducted in accordance with the valid German and European guidelines for laboratory animal care.
Animal model
Rats were intubated and administered inhalation anesthesia using isoflurane with a concentration of 4–5% for induction and 2–3% for maintenance, respectively.
We used a model creating a temporary ligation of the left anterior descending artery (LAD) via a small left thoracotomy at the fourth intercostal space. 15 A suture using 8-0 polypropylene was looped under the LAD, tied up for the induction of myocardial ischemia (MI), and released for the initiation of reperfusion. MI was conducted for 30 min followed by 120 min of reperfusion. To induce mechanical MCS and controlled coronary reperfusion, a miniaturized normothermic CPB was applied from 15 min after the completion of the MI to the end of the reperfusion.
Settings of CPB circuit
CPB in a rat model was established according to our previously published procedures.16,17 For the initiation of the extracorporeal circulation, a 14 G custom-made polyethylene cannula with multiple orifices was introduced into the right jugular vein after surgical cutdown and advanced into the right atrium and inferior vena cava, followed by a systemic administration of sodium heparin (400 IU/kg). A 20 G polyethylene cannula was also placed in the tail artery for arterial return. A continuous blood pressure measurement was achieved with a 22 G polyethylene cannula placed in the right femoral artery. The CPB circuit was primed with 10 mL of 6% hydroxyethyl starch (KabiPac, Fresenius Kabi GmbH, Bad Homburg, Germany) and a small volume of sodium heparin. Blood from the jugular vein flowed into the venous reservoir, which was slightly depressurized, and through the peristaltic pump into the membrane oxygenator (M. Humbs, Valley, Germany). The nominal flow of the CPB was calculated as 100 mL/min/kg. Using a heating mat and a heat exchanger in the CPB circuit, the body temperature was adjusted to 37°C.
Experimental groups and surgical procedures
Male Wistar rats weighing between 400 and 600 g (n = 25), purchased from Janvier Breeding Center (Le Genest-Saint-Isle, France), were randomly divided into 5 groups as follows: (1) Sham group (n = 5): cannulas were placed in each vessel without the initiation of CPB. A suture with 8-0 polypropylene was passed under the LAD without ligation. The vehicle solution (0.9% saline) was injected intraperitoneally continuously for 15 min. (2) MI + vehicle (MI + V) group (n = 5): cannulas are placed without the initiation of CPB. Temporary ligation of the LAD for 30 min was completed with a tourniquet technique. Intraperitoneal vehicle administration was started immediately after LAD ligature. Reperfusion of LAD was initiated by loosening the ligation 30 min after the completion of the ischemia and continued for 120 min without CPB running. (3) MI + fasudil (MI + F) group (n = 5): the work sequence of this group was performed in the same manner as in group 2 except for the administration of the selective ROCK inhibitor fasudil (10 mg/kg, dissolved in 0.9% saline; Asahi Kasei Corporation, Japan) instead of the vehicle. (4) MI + V + CPB group (n = 5): in addition to the work sequence in group 2, CPB was initiated 15 min after the ligation of the LAD. After the completion of 120-min reperfusion of the LAD with CPB support, animals were weaned from CPB. (5) MI + F + CPB group (n = 5): the work sequence of this group was performed in the same manner as in group 4 except for the fasudil administration (10 mg/kg) instead of the vehicle. A schematic presentation of the work sequences for all five groups is shown in Figure 1. No inotropic or vasoactive agents were applied in all five groups during the operation. The administration of drugs (vehicle or fasudil) was performed in a blind manner against the surgeon, who performed all operative procedures and intraoperative animal care.

Work sequence of the operative procedures for each experimental group. MI: myocardial ischemia; V: vehicle; F: fasudil; CPB: cardiopulmonary bypass; LAD: left anterior descending artery.
Hemodynamic measurements and laboratory parameters
Left ventricular (LV) performance was evaluated by the conductance catheter technique from simultaneous LV volume and pressure measurements. A 2 F pressure-volume catheter (SPR-878, Millar, Inc., Houston, TX) was inserted directly into the right carotid artery and advanced into the LV guided by online pressure and volume signals, which were continuously recorded at a sampling rate of 1000/s using an MPVS Ultra System (Millar, Inc., Houston, TX) coupled to a PowerLab 8/35 data acquisition system (ADInstruments Pty Ltd, Castle Hill, Australia). A rat insulator-type calibration cuvette provided by the manufacturer was applied to convert the raw conductance signals to the units of capacity. A small volume of hypertonic saline (10%) was injected into the right jugular cannula to determine a parallel conductance of the myocardium, and the offset was subtracted to obtain absolute blood volume. A calibration series was performed to adjust the results according to the hematocrit level.18,19
The hemodynamic assessment included mean arterial pressure (MAP), heart rate (HR), LV end-diastolic pressure (LVEDP), LV ejection fraction (LVEF) according to the LV end-systolic and end-diastolic volume (EDV), and LV pressure maximum rise and fall rate (±dP/dt). These parameters were continuously monitored throughout the experimental procedures, digitally processed in LabChart 8 for Windows (ADInstruments Pty Ltd, Castle Hill, Australia), and collected at each time point: before thoracotomy for LAD ligation (T1: baseline), 30 min after LAD ligation (T2: just before reperfusion), and 150 min after LAD ligation (T3) (Figure 1). All hemodynamic measurements were made under stable circulatory conditions, and data were accumulated in the mean value of consecutive 20 cardiac cycles at each measurement. The respirator was stopped during data acquisition to avoid respiratory-mediated hemodynamic fluctuation. In addition, a blood gas analysis (BGA) was performed just before each time point. The remaining blood samples were immediately centrifuged. The supernatant was harvested and stored at − 80°C for further analysis in the Central Institute for Clinical Chemistry and Laboratory Medicine of the University Hospital of Düsseldorf to detect troponin-T at each time point.
Sacrifice of the animals and confirmation of the ischemic region in myocardium
Animals were sacrificed by blood extraction immediately after T3; the death of animals was confirmed by the direct inspection of the cardiac mechanical activity and the record of the conductance catheter at least for 5 min. Simultaneously, organs were flushed systemically with 0.9% saline infused through the arterial cannula and drained from the venous cannula. After saline perfusion, the original LAD ligation was tied up again and the aortic root was pressurized using Evans blue dye to confirm whether the proximal LAD had been definitely occluded during the operation (Figure 2). Then, tissue samples were taken from the nonstained region of the myocardium.

Confirmation of proximal LAD occlusion via Evans Blue staining.
Western blot analysis
Western blots of heart tissue samples were performed to investigate changes in protein levels induced by I/R injury. Unstained portions of the myocardium were removed from the heart. Snap-frozen myocardial samples were powdered, then suspended in Mammalian Protein Extraction Reagent buffer (Thermo Fisher Scientific, Waltham, MA) containing protease and phosphatase inhibitors, and finally homogenized. Samples were centrifuged at 15,000 × g for 15 min and supernatants were collected. Moreover, 50 µg of protein was separated using 7% and 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis gels and transferred by blotting to nitrocellulose membranes. Primary antibodies for phosphorylated protein kinase B (p-Akt), Akt, phosphorylated STAT3 (p-STAT3) and STAT3 (all Cell Signaling Technology, Inc., Danvers, MA) were diluted according to the manufacturer's instruction. The membranes were blocked with 5% bovine serum albumin (BSA) followed by incubation overnight at 4°C with primary antibodies. Secondary goat antirabbit horseradish peroxidase (HRP) antibody (Jackson Immuno Research Labs, West Grove, PA) was applied for 1 h diluted at 1:5000 in 5% BSA in Tris-buffered saline with 0.1% Tween 20 detergent. Chemiluminescence signal (Quantum chemiluminescent HRP substrate; Advansta Inc., Menlo Park, CA) was recorded using a CCD Bioimaging System (UVP, LLC, Upland, CA). Image J 1.51 (Wayne Rasband, National Institutes of Health, USA) was used for densitometry.
Statistical analysis
For the sample size calculation, a type I error of 0.05 and type II error of 0.1 were considered acceptable for an animal study. Based on a previous study, 20 the positive effect of fasudil on cardiac contractility evaluated by ± dP/dt was chosen as the primary endpoint in our study. The G*Power 3 (University of Düsseldorf, Germany) was used for the sample size calculation, which resulted in n = 5 per group. The data were expressed as mean + standard error values (n = 5 animals per group). Only non-parametric tests were applied to evaluate the statistical difference between study groups; in Tables 1, 2, and 3, priori Kruskal–Wallis test and subsequent post hoc testing via the Steel–Dwass test were performed for pairwise comparisons between individual groups. In Figures 5 and 6, the Steel–Dwass test was also performed for pairwise comparisons between individual groups without priori test Two-way repeated measures ANOVA calculated the effects of the group and timepoint in the transition of the troponin-T and subsequent post hoc testing via the Tukey test was applied for pairwise comparisons between individual groups. JMP 9.0.2 for Windows (SAS Institute, Cary, NC) was used for all data analyses.

Effects of fasudil and CPB on LVEF and ± dP/dt. LVEF and ± dP/dt were assessed using the conductance catheter technique. (A) Comparison of absolute changes of left ventricular ejection fraction (LVEF). ΔLVEF indicates the difference in LVEF between T1 and T3. *: Because of a missing value of LVEF, the number of animals in the MI + F + CPB group was 4. (B) Comparison of absolute changes of + dP/dt. Δ + dP/dt indicating the difference of + dP/dt between T1 and T3. (C): Comparison of absolute changes of −dP/dt. Δ−dP/dt indicates the difference of −dP/dt between T1 and T3. (D) Comparison of preload recruitable stroke work at T3. †: Because of a missing value of EDV, the number of animals in the MI + F + CPB group was 4. MI: myocardial ischemia; V: vehicle; F: fasudil; CPB: cardiopulmonary bypass; T1: baseline; T3: after reperfusion; PRSW: preload recruitable stroke work, EDV: end-diastolic volume. Data are presented as mean + SE (n = 4–5 animals per group).

Impact of fasudil and CPB on activation of Akt and STAT3. Myocardial protein expression of (A) total Akt and phosphorylated Akt (P-Akt) as well as (B) total STAT3 and phosphorylated–STAT3 (p-STAT3) was assessed by Western blot. Data are presented as mean + SE (n = 5 animals per group).
BGA and hemodynamic parameters at baseline (T1).

BGA: blood gas analysis; MAP: mean arterial pressure.
BGA and hemodynamic parameters 30 min after ischemia (T2).

BGA: blood gas analysis; MAP: mean arterial pressure.
*p = 0.0011.
p = 0.041.
p = 0.028.
p = 0.0076.
p < 0.0001 compared to the sham, MI + V and MI + F animals.
BGA and hemodynamic parameters after reperfusion (T3).
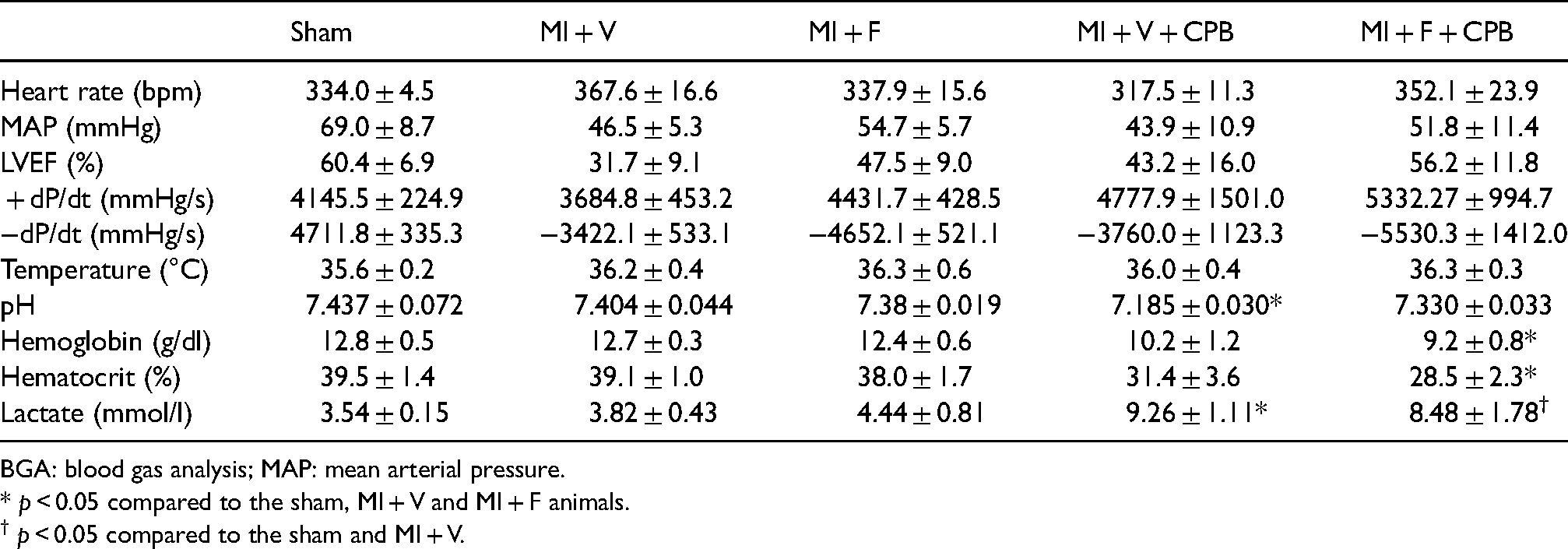
BGA: blood gas analysis; MAP: mean arterial pressure.
* p < 0.05 compared to the sham, MI + V and MI + F animals.
† p < 0.05 compared to the sham and MI + V.
Results
Survival of the animals
In addition to the 25 animals included in this analysis, 5 more animals were treated but died from AMI intraoperatively; of these, 2 animals died immediately after the completion of LAD ischemia before randomization (drug administration) and 3 other animals died before the completion of the reperfusion (2 in the MI + V group and 1 in the MI + F group). No intraoperative cardiogenic death was observed in the course of animals that were supported by CPB. All 10 animals in the MI + V + CPB and MI + F + CPB groups were successfully weaned from CPB without any support from catecholamine and other vasoactive agents.
Assessment of myocardial injury
In this experiment, the serum concentration of troponin-T peaked at the end of the operation. Serum troponin levels in each group at the beginning (T1) and at the end of the operation (T3) are shown in Figure 3. Troponin concentrations were higher in all groups subjected to MI than before, except for the sham group, confirming the efficacy of LAD occlusion and the extent of MI.

Impact of fasudil and CPB on the myocardial injury. Serum concentrations of troponin-T were quantified using automated analyzers. White bar indicates the serum concentration of troponin-T measured at T1 (baseline) and gray bar indicates that at T3 (after reperfusion). MI: myocardial ischemia; V: vehicle; F: fasudil; CPB: cardiopulmonary bypass. Data are presented as mean + SE (n = 5 animals per group). Longitudinal change within the same animal was significant (p = 0.0001). *: p > 0.05 in pairwise comparison between each group.
BGA and hemodynamic parameters
The values of HR, MAP, rectal temperature, and parameters of BGA at T1, T2, and T3 are presented in Tables 1, 2, and 3. There were no significant differences among the groups in HR, rectal temperature, and parameters of BGA at baseline. Because of the hemodilution induced by the CPB circuit, hemoglobin and hematocrit levels in the groups treated with CPB (MI + V + CPB and MI + F + CPB) at T2 and T3 were significantly lower than those of other groups. In addition, the MI + V + CPB and MI + F + CPB groups had a higher blood level of lactate at T3. Further evaluating hemodynamics, MAP proved to be most stable in the sham group over the course of the entire experiment, but still demonstrated a slight but steady decrease from T1 to T3 (Figure 4). At T2, mean MAP was significantly different among the 5 groups with the highest mean MAP in the MI + V + CPB group and lowest in the 2 groups receiving fasudil (MI + F and MI + F + CPB) and the 2 control groups receiving vehicles exposing intermediate mean MAP values (Table 2, Figure 4). Accordingly, ± dP/dt in the 2 groups receiving fasudil, which were influenced by the afterload, was lower at T2, which was contradictory to LVEF at T2 (Table 2). However, at the end of the experiment after 120 min of reperfusion (T3), mean MAP values in both groups receiving fasudil were higher than in-vehicle controls. LVEDP in the MI + F and MI + F + CPB groups showed a greater dropping trend than other groups without CPB (Figure 4, B) at T3, indicating a reduction of the LV volume load.

Effects of fasudil and CPB on MAP and LVEDP. MAP and LVDEP were assessed using the conductance catheter technique. (A) Change of mean arterial pressure (MAP) between T1 and the other time points. (B) Change of left ventricular end-diastolic pressure (LVEDP) between T1 and the other time points. MI: myocardial ischemia; V: vehicle; F: fasudil; CPB: cardiopulmonary bypass; T1: baseline; T2: before reperfusion; T3: after reperfusion. Data are presented as mean + SE (n = 5 animals per group).
Comparison of LV performance
Comparing the experimental groups without CPB, rats with MI but without fasudil administration (MI + V) had a greater tendency to have decreased LVEF during the experiment (T1 to T3) than those receiving fasudil administration (MI + F), but without a statistical significance (p = 0.83). This effect of fasudil was less pronounced between experimental groups with MCS via CPB (MI + V + CPB vs. MI + F + CPB; p = 1.0) (Figure 5, A). With regard to the transition of LVEF through the experimental protocol, a greater drop of LVEF at T3 was observed in rats without fasudil administration, and this tendency was neutralized by the application of CPB (MI + V vs. MI + F, p = 0.83; MI + V + CPB vs. MI + F + CPB, p = 1.0). A similar tendency to the transition of LVEF was also observed in the transition of + dP/dt. MCS by CPB tended to minimize the AMI-associated drop in + dP/dt regardless of fasudil administration (MI + V vs. MI + F, p = 0.45; MI + V + CPB vs. MI + F + CPB, p = 1.0). The + dP/dt drop at T3 in MI + V group was up to 40%. Compared with this control group, the maintenance of + dP/dt in MI + F + CPB was stronger than that in MI + V, and the combination of fasudil and MCS via CPB was effective in the rescue of + dP/dt (MI + V vs. MI + F + CPB; p = 0.22) (Figure 5, B).
–dP/dt was measured at T3 to evaluate postischemic diastolic function. Interestingly, at the end of the experiments, –dP/dt showed some decrease as a consequence of the operative treatment and anesthesia, as observed in the sham group. In the MI groups, fasudil led to a partial preservation of –dP/dt in both study arms, with or without MCS, respectively (Table 3). However, the difference in the transition of –dP/dt showed less tendency between experimental groups; the experimental group with fasudil administration and MCS support showed a slightly better tendency than that of vehicle control (MI + V vs. MI + F + CPB, p = 0.59) (Figure 5, C). The systolic pressure increment ( + dP/dt) is a classic contractility parameter, which is dependent on preload changes. The analysis of the relation of stroke work (SW) to EDV allowed a comparison of the preload recruitable SW (PRSW) among groups at a given EDV. Compared with the corresponding control animals (MI + V), the PRSW was moderately improved in the MI + F + CPB group (p = 0.23), indicating a preserved systolic function during I/R injury (Figure 5, D).
Myocardial activation of STAT3 and Akt
Western blot analyses of myocardial tissue samples were performed to investigate changes in protein expression and activation of salvage pathways. Mean relative activation of p-AKT showed a remarkable difference between the groups with and without CPB support during the reperfusion. Mean relative activation of p-AKT was increased by 96% and 121% in animals receiving CPB support with or without fasudil administration, respectively (p = 0.33) (Figure 6, A). There were no remarkable tendencies in p-STAT3 expression between the groups regardless of CPB application during reperfusion (Figure 6, B).
Discussion
This study examined the effect of ROCK inhibition and MCS in the setting of I/R injury in the rat heart. There were several findings observed in this model. First, rats supported by CPB during the reperfusion phase exhibited better LV performance after reperfusion, especially regarding contractility after I/R injury. Correspondingly, myocardial activation of Akt was increased in CPB-supported animals, indicating that MCS reduces I/R injury and improves LV performance through the activation of the reperfusion injury salvage kinase (RISK) pathway. However, in rats with MCS, fasudil administration did not additively improve LV contractility or significantly increase the activation of the RISK pathway during reperfusion.
Role of ROCK inhibitor in I/R injury
Myocardial I/R is a complex pathological process. The reperfusion phase of I/R injury is particularly deleterious to the mitochondria through the opening of the mitochondrial permeability transition pore (MPTP) that causes the release of cell death–inducing proteins.21,22 Moreover, deleterious nucleotide depletion and mitochondrial Ca2+ overload are further critical determinants of lethal reperfusion injury. 23 Owing to the release of mitochondrial proteins and the loss of ATP-generating capacity, the opening of MPTP also induces both apoptotic and necrotic cell death. Phosphatidylinositol 3-kinase (PI3K)/Akt and nitric oxide (NO) signaling, which is called the RISK pathway, has been identified as an essential system protecting against I/R-induced cell death. 24 ROCK is a family of serine/threonine protein kinases, stimulated by G protein–coupled receptor activation of small plasma membrane–bound GTP-binding proteins. ROCK activation has been implicated in infarct development after myocardial I/R through the mechanism of reduced endothelial NO synthase activity and PI3K/Akt signaling in the heart.25,26 ROCK inhibition protects the myocardium against I/R injury through a mechanism dependent on constitutive PI3K/Akt and NO signaling. 24 Fasudil, a ROCK inhibitor, has been reported to inhibit ROCK activity by competing with ATP for the ATP binding site in the ROCK catalytic domain.27,28 In recent years, fasudil is also becoming more extensively used in the cardiovascular field. In the acute phase of myocardial I/R injury, the effect of fasudil to reduce the further loss of myocardial tissue and prevent ventricular remodeling through the RISK pathway was demonstrated in several animal models.29–31 However, to the best of our knowledge, there has been no in vivo model to demonstrate the effect of fasudil on LV performance in the absolutely acute phase of I/R injury. However, such an acute scenario of MI and consecutive hemodynamic instability despite myocardial revascularization (be it operative or via catheter intervention) is frequently encountered in the clinical setting. The present model was designed to investigate whether myocardial contractility may be protected by the administration of the fasudil in the setting of acute myocardial I/R injury and whether there may be a synergistic effect of ROCK inhibitor and MCS during an ongoing I/R injury of the myocardium.
Role of MCS and ventricular unloading in I/R injury
Current knowledge supports the role of CPB or other circulatory support systems in the setting of AMI with hemodynamic instability to compensate for decreased cardiac output and to reduce preload of the ventricle accordingly. In this framework, CPB decreases preload by withdrawing blood from the right atrium, accordingly reducing the pulmonary venous return to LV, and it also increases LV afterload by augmenting the arterial perfusion volume. Therefore, the impact of CPB on the relationship between pressure and volume of the LV depends on the balance between decreased preload and increased afterload. The fundamental pathophysiology that leads to the formation of infarcted myocardium is a mismatch between oxygen supply and demand. Saku et al. 4 reported that totally unloading LV assist device (LVAD) could suppress LV oxygen consumption, thus improving hemodynamics and reducing infarct size in a canine model. The underlying mechanisms, how the mechanical unloading could save myocardial tissue, were explored previously. With regard to I/R injury, Kapur et al. 32 reported that infarct size could be reduced by LV unloading, which involves the activation of the RISK pathway, thereby protecting the myocardium from apoptosis in the porcine heart. A similar result was achieved by Tamareille et al., 33 suggesting that LVAD unloading before reperfusion reduces the release of endothelin 1 and inhibits Ca2+ overload and subsequent myocardial apoptosis. As another mechanism affecting the rescue of the myocardium, collateral blood flow could play an important role during MCS. Because collateral blood flow is elevated by increased arterial diastolic pressure and decreased LVEDP,34,35 the improvement of collateral flow by CPB may contribute to the reduction of the infarct size. A potent vasodilator effect of fasudil could also contribute to this process. Furthermore, CPB could compensate for the hemodynamic instability caused by the vasodilatory effect of fasudil.
Limitations
First, owing to the small sample size (n = 5 per group) and any p-value achieved from comparisons of the randomized groups, this work represents a preliminary study. Second, the optimal timing of fasudil administration is also controversial. In the study by Kitano et al., 36 a positive effect of fasudil was observed in reducing infarct size after an earlier application. However, it was very unlikely in a real-world clinical setting to apply fasudil 60 min before the onset of ischemia. To apply the results of this investigation to clinical settings, we should apply fasudil or mechanical unloading after the onset of ischemia. The lack of a dosage trial is certainly a limitation of this study. Initially, we administered 10 mg/kg of fasudil intravenously, and then we switched to an intraperitoneal injection of 20 mg/kg. However, a vasodilating effect was too strong in the fasudil group to reach the end of the experimental protocol because of the hemodynamic deterioration. The data of the dosage trial were unfortunately not available because of the incompleteness of the study protocol. We believe that the current dosage (10 mg/kg, intraperitoneal injection) was the safe limit not to lead to hemodynamic instability. Third, the lack of an estimation measuring the size of the infarction area limits us from further drawing conclusions on the mechanism underlying the potential effect of fasudil in combination with mechanical unloading. Finally, despite the fact that rats supported by CPB exhibited better LV performance and increased myocardial RISK pathway activation after I/R in our study, application of CPB also induced a significant increase in serum lactate as a side effect. However, this was our first study using CPB in a normothermic setting which, compared with hypothermia, is characterized by altered systemic perfusion conditions resulting in increased lactate levels. We will address this topic in future projects because we want to continue examining the cardioprotective effects of the ROCK inhibitor fasudil in combination with MCS.
Conclusions
Our preliminary results in a small animal model indicate that ROCK inhibition can reduce the myocardial damage caused by reperfusion injury although the sole application of ROCK inhibition cannot significantly preserve cardiac function. The combined application of ROCK inhibition and MCS may have a potential benefit for myocardial rescue in the setting of AMI. However, the true benefit of fasudil and its synergetic mechanism with MCS require further verification in subsequent studies to pave the way for the therapy that can lead to better outcomes after AMI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Susanne-Bunnenberg-Herzstiftung.
Ethical approval
This study was approved by a third party belonging to the local authority LANUV (Landesamt für Natur, Umwelt und Verbraucherschutz NRW, Germany) (AZ84-02.04.2017. A289) and conducted in accordance with German and European guidelines for laboratory animal care.
Informed consent
Not applicable.