
Abstract
Background
Though laser guided extractions of cardiac implantable electronic devices leads have become a routine procedure, the severe complications are associated with a high mortality. Here, we report our single center experience using uniportal video-assisted thoracoscopy for laser lead extraction and compare it to stand-alone laser lead extraction.
Methods
The intraoperative data and postoperative clinical outcomes of patients undergoing laser lead extraction with concomitant thoracoscopy (N = 28) or without (N = 43) in our institution were analyzed retrospectively.
Results
Neither the median x-ray time (612.0 s for the thoracoscopy group vs. 495.5 s for the non-thoracoscopy group, p = 0.962), length of the operation (112.5 vs. 100.0 min, p = 0.676) or the median length of hospital stay (9.0 vs. 10.0 days, p = 0.990) differed significantly. The mean intensive care unit stay was longer for patients in the non-thoracoscopy group (0.8 vs. 2.5 days, p = 0.005). The 30-day-mortality in the thoracoscopy group was zero, whereas five patients died in the non-thoracoscopy group. Furthermore, four patients in the non-thoracoscopy group had encountered haemothorax, while none were observed in the thoracoscopy group (p = 0.148).
Conclusions
The adoption of uniportal video-assisted thoracoscopy during laser-guided lead extraction of cardiac implantable electronic devices can be considered safe and does not lengthen the operating time or hospital stay. It might be useful in the detection of severe complications and, in experienced hands, possibly allow direct bleeding control.
Keywords
Introduction
Transvenous lead extraction (TLE) of cardiac implantable electric devices (CIED) is increasing with the aging population. 1 Extraction systems such as laser powered sheaths are often used for TLE of leads with long dwell times, and their use has been reported to achieve clinical success rates of up to 96%. 2 Major adverse events such as pericardial tamponade or massive bleeding due to laceration of the superior vena cava or the right atrium are rare (1–5%), but often end fatal, 3 and mortality rates of patients with vascular lacerations and consecutive massive bleeding are reported up to 40%. 4 Therefore, new strategies for improving the safety of laser assisted TLE (LTLE) are warranted. In 2014, we reported the successful use of right-sided unilateral video assisted thoracoscopy (UVATS) during LTLE in a series of five cases in our hospital. 5 The UVATS during LTLE allows direct visualization of critical structures (superior vena cava, right atrium, right vena subclavia) during the procedure and direct bleeding control. However, the feasibility and safety of UVATS during LTLE have not been evaluated in a larger patient cohort until today. We, therefore, report comparative results between the patients who underwent LTLE with and without UVATS in our institution during the past 5-years.
Patients and methods
Our institutional database was searched retrospectively for patients undergoing LTLE between January 2014 and December 2018 with (UVATS-group) and without UVATS (non-UVATS group). In accordance to the local guidelines of the ethics commission, no ethical application was needed for this retrospective study, and institutional review board approval, consent statement, and clinical trial registration were not required. All procedures were performed by the same experienced surgeon familiar with both cardiac and thoracic surgery. The decision for concomitant UVATS was made individually for each patient, based on risk factors such as dwell time of the leads, number of leads to be extracted, type of leads and frailty. The non-UVATS procedure was favored in patients with previous cardiac surgery, but not limited to, as it was assumed that adhesions from previous cardiac surgery would protect the patient from pericardial tamponade and bleeding. Our surgical protocol has been previously described in detail by Zardo et al. 5 Briefly, all procedures were performed under general anesthesia, cardiopulmonary bypass standby and, only for the patients in the UVATS group, with single lung ventilation. Right sided UVATS was performed by a 3–5 cm incision at the 4th or 5th intercostal space with a high-resolution 30-degree videoendoscope (EndoEye HD II, Olympous Corporation, Tokyo, Japan). The laser extraction was performed by the responsible surgeon using internal locking stilets and the SLS II laser sheath (Philips N.V., Amsterdam, Netherlands), while a second assisting surgeon was doing the VATS. At the end of the operation, a chest tube (28 French) was placed and the patients were referred to the intensive care unit after on-table-extubation whenever possible.
All data were recorded in Excel spreadsheets (Microsoft, 2016) and analyzed using IBM SPSS Statistics (IBM Corp. Released 2019, IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp). While categorical variables are presented as absolute values and percentages, continuous variables were tested for normality and are presented as median (Q1; Q3), as non-normality was found for all continuous variables. Mean values and standard deviation were given as additional information when the median was zero. The variables were compared with Mann-Whitney-U test, Pearson's chi-squared test or Fisher's exact test according to group size and type of variable.
Results
During the observed timeframe, seventy one LTLE procedures were identified (Table 1). The baseline characteristics of patients in the two groups did not differ significantly, despite significantly more patients had undergone previous cardiac surgery in the non-UVATS group (51% vs. 25%, p = 0.028). The two groups were comparable for age of the extracted leads and the number of extracted leads per patient (Table 2). However, patients in the UVATS group had significantly more often single chamber pacemaker systems (14% vs. 0%, p = 0.021) and less often ICD single chamber systems (14% vs. 42%, p = 0.014), while significantly more ICD dual coil leads were extracted in the non-UVATS group (54% vs. 29%, p = 0.039).
Patient's demographics.
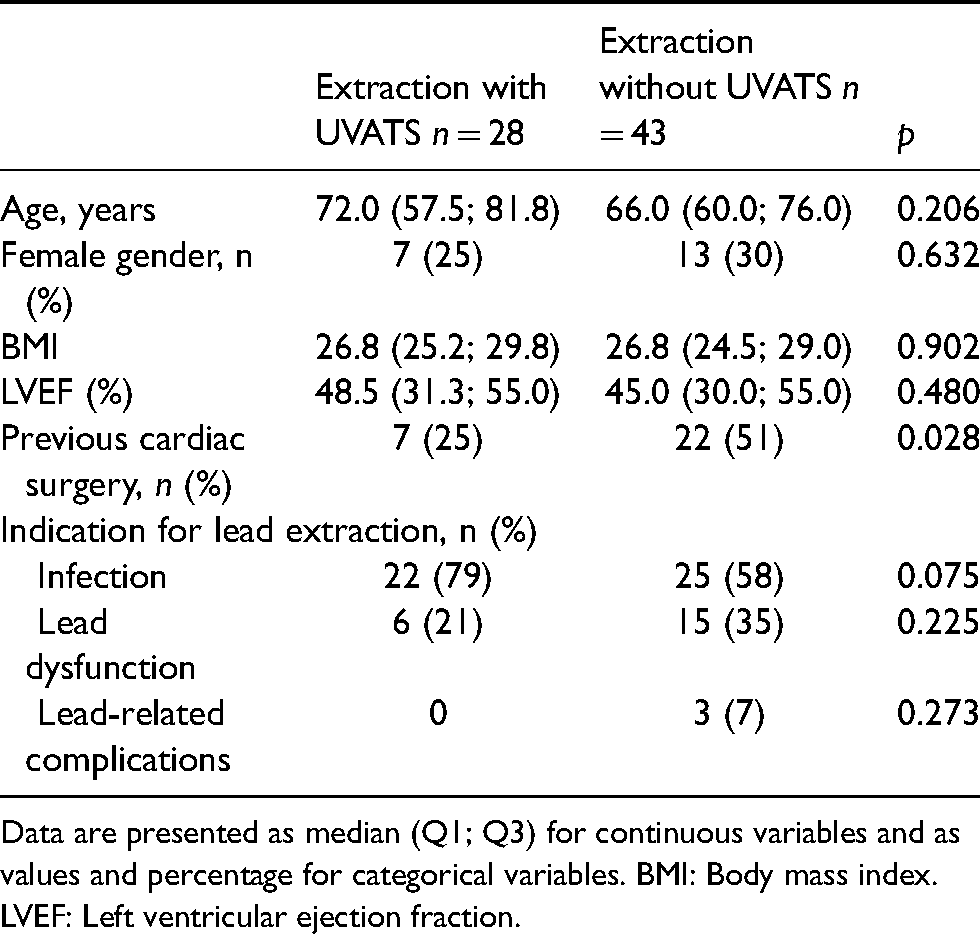
Data are presented as median (Q1; Q3) for continuous variables and as values and percentage for categorical variables. BMI: Body mass index. LVEF: Left ventricular ejection fraction.
Pacemaker system and lead characteristics.
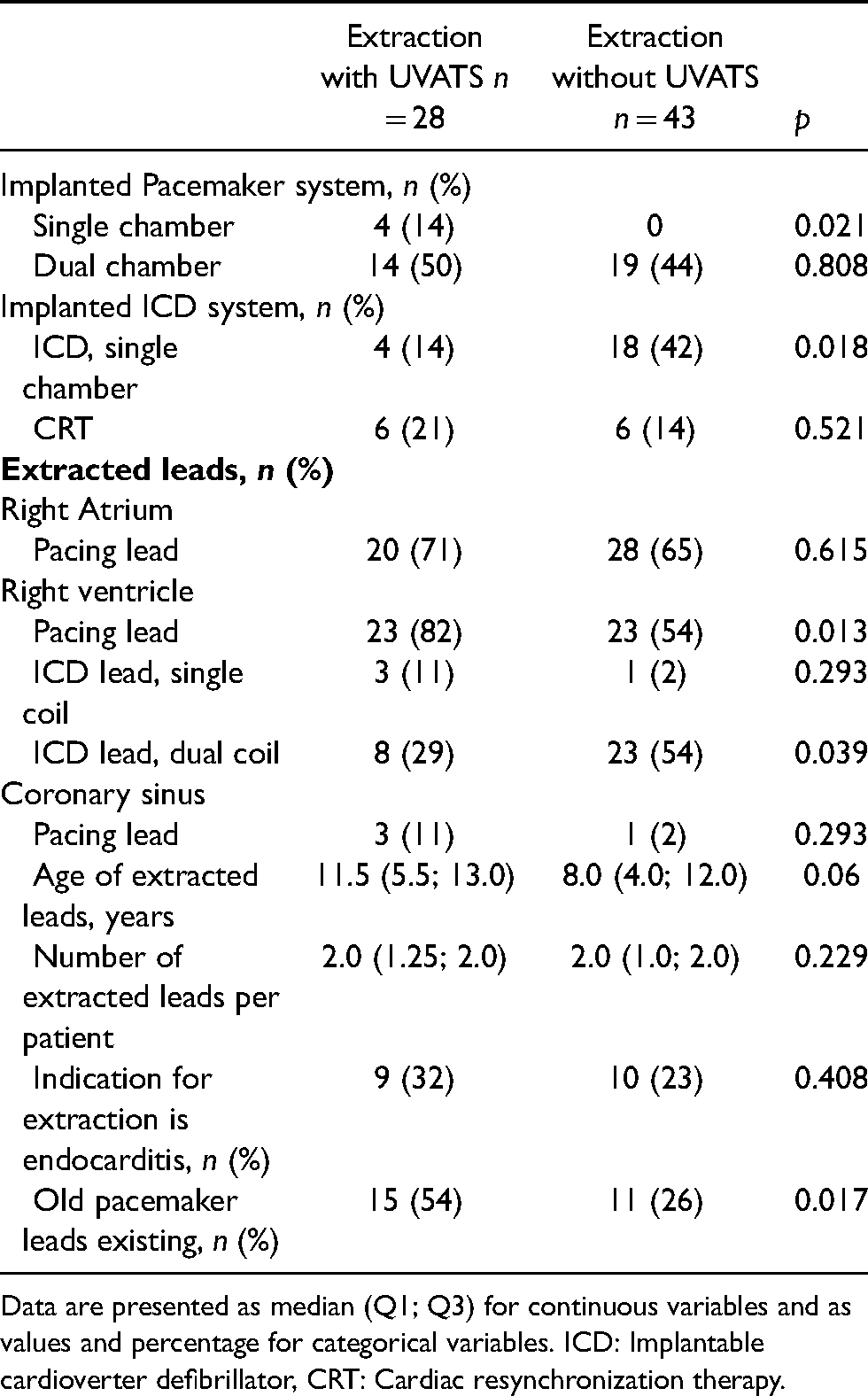
Data are presented as median (Q1; Q3) for continuous variables and as values and percentage for categorical variables. ICD: Implantable cardioverter defibrillator, CRT: Cardiac resynchronization therapy.
The intra- and postoperative characteristics of both groups were comparable (Table 3). In both groups, the length of the procedure and x-ray time did not differ significantly. Patients in the UVATS group were significantly shorter on the ICU (mean 0.8 vs. 2.5 days, p = 0.005), but the median hospital stay did not differ significantly (9.0 vs. 10.0 days, p = 0.990). In a further subanalysis, the median length of hospital stay was significantly longer for patients who underwent TLE due to infection compared to all other patients (12 days, Q1–7; Q3–16.0 vs. 5 days, Q1–4; Q3–11, p = 0.004), irrespective of concomitant UVATS. No significant differences were observed in major and minor complications, but a trend for a lowered complication rate was seen in the UVATS group, where no mortality was observed. In the non-UVATS group, five patients died during the 30 days follow-up (Table 4). Three patients experienced a laceration of the superior vena cava (SVC) that corresponds to a rate of 4% compared to the overall cohort of seventy one patients. The two patients that experienced mass bleeding and emergency sternotomy in the operation theater died within the operation. Only one perforation of the SVC could be handled, but the patient died in the further postoperative course due to cardiogenic shock after additional, interventional mitral valve repair.
Procedural details and outcome.
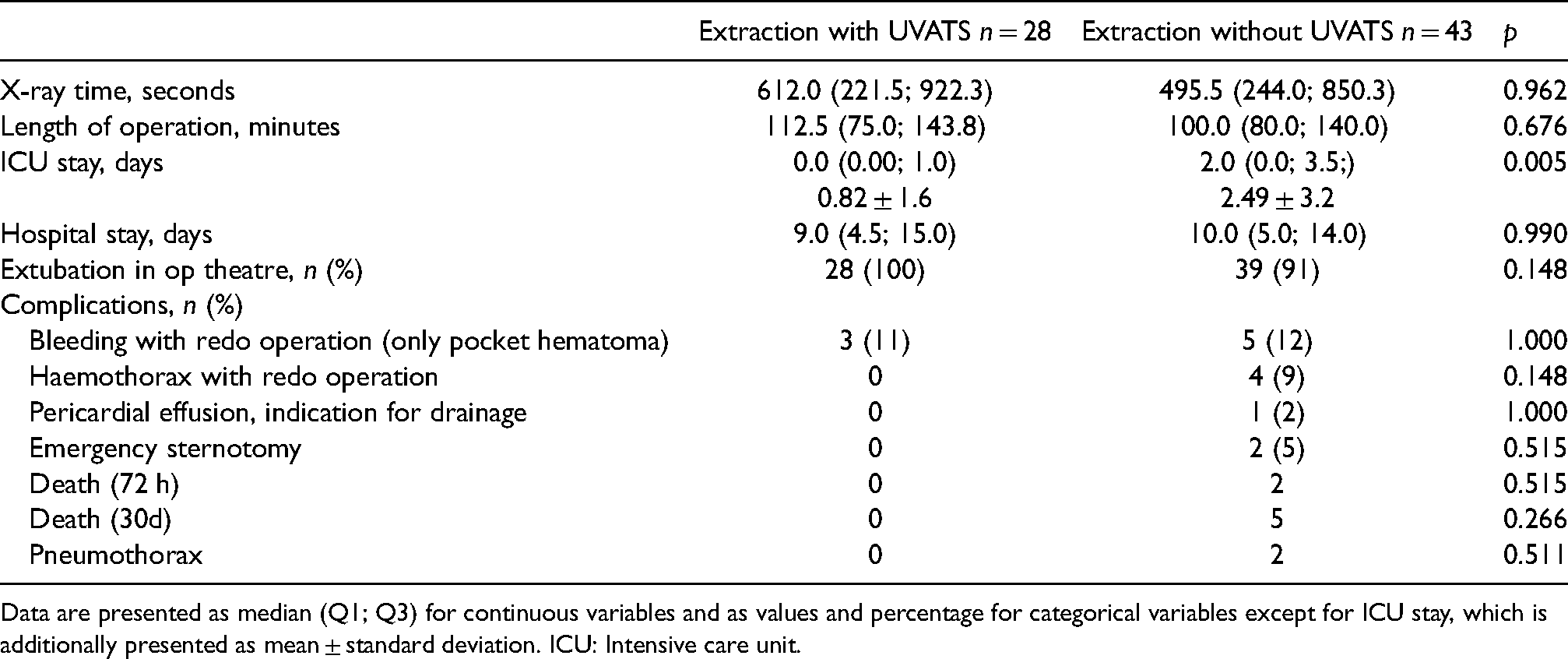
Data are presented as median (Q1; Q3) for continuous variables and as values and percentage for categorical variables except for ICU stay, which is additionally presented as mean ± standard deviation. ICU: Intensive care unit.
Characteristics of deceased patients.
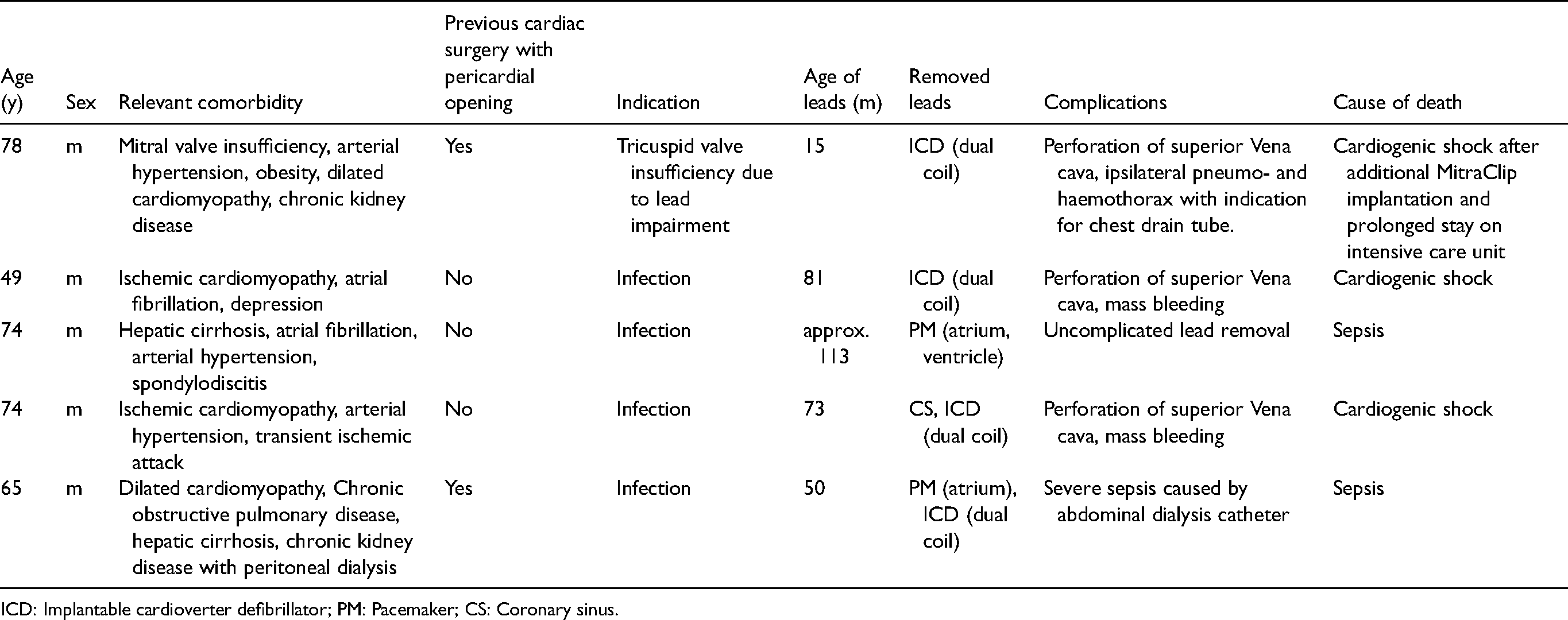
ICD: Implantable cardioverter defibrillator; PM: Pacemaker; CS: Coronary sinus.
Discussion
Complications of LTLE are rare but often fatal due to massive bleeding. Intravasal approaches to deal with vasal lacerations, such as bridge occlusion ballons are promising, but improper placement and lacerations larger than the ballon limit their application. 6 Various hybrid approaches combining surgery with LTLE to reduce the intraoperative risk have been described, but evidence is low.7–9 Here, we present our 5-years experience with the UVATS approach. It was our hypothesis, that in case of laceration of the SVC or right atrium, the bleeding would be manageable by applying pressure on the laceration, e.g. with swabs, until thoracotomy is performed to repair the laceration after the establishment of CPB.
The feasability of this approach has been describe before in smaller case series. Bontempi et al. reported a case series, where monitoring the SVC and right atrium by UVATS or minithoracotomy helped to treat lacerations. 10 Furthermore, Azzarafiy et al. reported nineteen cases with left-minithoracotomy and VATS without complications. 7
In the present patient cohort, no major complications such as hemothorax, pericardial effusion with the need for drainage or emergency sternotomy were seen in the UVATS group. This benefit could likely be linked to the UVATS approach, because the operating surgeon has not only manual, but also visual feedback of the protrustion of the laser sheath. Whenever traction on the SVC or the right atrium is visible, the operating surgeon can slow down the protrusion for a more sensitive laser extraction.
The overall mortality in our cohort was 7%, and deaths were only seen in the non-UVATS group. This is above the rate of 0.23%−1.6% that is reported in larger registries for transvenous lead extractions.11,12 However, we are a tertiary referal center for laser lead extractions, so the patients in our cohort can be considered as selected high risk patients referred from surrounding hospitals, if complicated lead extraction would be expected.
Only two patients died due to intraprocedural complications, and both were operated due to infections of the system. It is known that especially in patients with infections, the mortaliy rate can rise up to 7.7%, as CIED infections and systematic inflammation can lead to multi-organ failure. 13 Furthermore, these two patients had both not undergone previous cardiac surgery (Table 4). Although we cannot prove the protective effect of pericardial adhesions as hypothesized by us, our hypothesis is at least supported by data from animal experiments, which report significant adhesions after previous pericardial opening in the area of the right and atrium and ventricle. 14 Thus, we would still suggest that prior cardiac surgery with pericardial opening might reduce the risk of fulminant pericardial tamponade after lead extractions and might therefore narrow the indication for perioperative UVATS, but should still not be considered as an exclusion criteria, as the protective effect is more hypothetical and not evidenced by data.
Our data indicates that UVATS can be performed without lenghtening the overall time of the operation, thereby excluding risks for complications associated with prolonged operation time, such as ventilator associated pneumonia. The median length of stay (LOS) reported in our cohort was 9.0 days for the UVATS group and 10.0 days for the non-UVATS group. This is longer than the typically reported 5–7 days in larger registries.11,12 However, 66% of the procedures were conducted due to infection, which requires extended antibiotic therapy and wound care. Large registries report a median LOS of 8 days for patients with TLE due to infection.15,16 This was in line with our sub-analysis, where we found that patients with infected CIED systems had a long median hospital stay (12 days), whereas all other patients were within the usually reported LOS (median 5 days).
This study has limitations. Dual coil ICD leads were more often extracted in the non-UVATS group group (54% vs. 29%, p = 0.039) and all patients with SVC injury had dual coil ICD extraction. As dual coil ICD leads are a known risk factor for major complications in TLE, the complications have to be attributed to the dual coil ICD leads and not to the missing UVATS procedure.
A further limitation is that the patients were not prospectively randomized and decision for UVATS was made as a case-to-case decision. Therefore, it is not possible to identify risk factors and indications for concomitant UVATS based on this study, and further data from larger cohorts or a randomized study protocols will be needed. However, based on the presented data, concomitant UVATS seems beneficial for high risk patients, where increased patient's age and frailty, age of the leads and dual-coil ICD leads could be considered as factors favoring UVATS.
In conclusion, the adoption of uniportal VATS during laser assisted CIED lead extraction is a safe and feasible method and may likely help to prevent or manage severe intra-procedural complications without lengthening the overall operation time or the hospital stay.
Footnotes
Authors’ Note
The results of this study were presented (oral presentation) on the 2021 Annual Meeting of the German Society of Cardiothoracic Surgery (online meeting).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.