
Abstract
Interdisciplinary collaboration is critical to address the multiple and varied needs of students with social/emotional and behavioral (SEB) challenges. Yet little is known about the nature of collaboration between two specialist groups who commonly support them: behavior analysts and mental health specialists. Considering expectations for collaboration, and the potential challenges unique to this partnership, we conducted a series of interviews in the U.S. state of Tennessee to explore these specialists’ experiences and perspectives around collaboration. We used a qualitative description approach, which led to identifying themes related to (a) specialists’ preparation to collaborate, (b) facilitators and barriers to effective collaboration, and (c) supports needed to collaborate more effectively in their current roles. Specialists from both groups felt their pre-service training inadequately prepared them to collaborate with one another. They identified several factors that impacted their ability to meaningfully collaborate and expressed needs for cross-discipline education, collaborative conversations, and training on “soft skills” to partner more effectively. We highlight distinct and overlapping perspectives within and across themes between behavior analysts and mental health specialists and discuss implications for improving the quality of these important partnerships.
Keywords
The expectation for collaboration among school professionals is ubiquitous, from establishing school-wide universal supports to implementing Individualized Education Programs for students with disabilities. Yet beyond interprofessional collaboration, a need for interdisciplinary collaboration has become more apparent as students encounter multiple barriers—both academic and nonacademic—to learning (Mellin, 2009; Willner et al., 2016). Interdisciplinary collaboration is defined by an integration of professionals’ knowledge and expertise toward a common goal through shared responsibility and decision-making (D‘Amour et al., 2005; Mellin, 2009). Conceptual frameworks for interdisciplinary collaboration emphasize various characteristics (e.g., interdependence, flexibility), contextual factors (e.g., professional identity, organizational attributes), and processes (e.g., communication, cross-disciplinary training) that interact to impact collaboration outcomes (Bronstein, 2003; Lemieux-Charles & McGuire, 2006; Mellin, 2009). Growing evidence from the school mental health literature points to positive impacts of interdisciplinary collaboration—particularly those between school and community providers—on access to services (Anderson-Butcher & Ashton, 2004; Bates et al., 2019; Reaves et al., 2022). However, less research has focused on specific interdisciplinary partnerships within the school setting to support certain student populations.
Specialists Who Support Students With Social/Emotional and Behavioral Challenges
The need for school specialists with expertise in social/emotional, behavioral, and mental health domains has grown in response to the prevalence of students with co-occurring externalizing and internalizing behavioral difficulties (Willner et al., 2016). These students—students with social/emotional and behavioral (SEB) challenges—include those who receive special education services (e.g., emotional disturbance) as well as those who are at risk for developing disabilities based on their lack of response to preventative or targeted supports (Cullinan et al., 2003; Gresham, 2005). Regardless of special education eligibility, students with SEB challenges often need intensive interventions across behavioral and mental health domains.
With respect to behavioral expertise, board certified behavior analysts (BCBAs) are increasingly employed by school districts to support assessment and intervention for students with severe or persistent challenging behavior (Behavior Analyst Certification Board [BACB], n.d.; VanDerwall & Poling, 2021). These master’s- (and in some cases, doctoral-) level specialists have training in Applied Behavior Analysis (ABA)—an applied science devoted to (a) understanding how environmental variables impact socially significant behaviors and (b) using this information to create environments that promote positive behavior change (Cooper et al., 2019). BCBAs commonly lead or oversee functional behavior assessments (FBAs) and behavior intervention plans (BIPs) for students with intensive intervention needs. Due to caseloads spanning multiple schools, most district-employed BCBAs consult with classroom teachers and other school personnel rather than provide direct student support (Giangreco et al., 2021; Shepley et al., 2017).
A range of qualified mental health specialists also play key roles in supporting students with SEB challenges. School psychologists, for example, are masters’-, specialist-, or doctoral-level clinicians whose expertise falls at the intersection of education and psychology. Their roles include psychological assessment and evaluation, behavioral assessment and intervention (including FBAs and BIPs), and consultation with school personnel and families to address a range of academic, social/emotional, and behavioral difficulties (Flaherty et al., 1998; National Association of School Psychologists [NASP], 2020; Zabek et al., 2023). School counselors and social workers are typically master’s-level clinicians who focus on the connection between the school, family, and community. They provide direct and indirect services to students and families, including individual and group counseling, social/emotional skill instruction, parent education, consultation with teachers and families, and referrals for additional services in or outside the school system (American School Counselor Association [ASCA], 2019; Flaherty et al., 1998; National Association of Social Workers [NASW], 2012; Zabek et al., 2023). Schools also commonly contract with qualified mental health providers to deliver school-based mental health services (National Center for Education Statistics, 2022). These professionals can hold a variety of credentials, including licensure as clinical social workers or professional counselors (Every Student Succeeds Act, 2015). Finally, the emergence of trauma-informed care has set the stage for new educator positions that specialize in promoting trauma awareness in schools, as well as integrating practices aligned with trauma-informed care in the classroom (e.g., trauma specialists; Perry & Daniels, 2016).
Collaboration Between BCBAs and Mental Health Specialists in Schools
BCBAs and mental health specialists are expected to collaborate in schools for a host of reasons. First, in addition to overlapping caseloads, their roles within the school have several points of intersection. Both groups of specialists are involved, to varying degrees, in evaluations, assessments, and interventions for students with SEB challenges (Wilczynski et al., 2002; Zabek et al., 2023). Moreover, both groups commonly have roles in multi-tiered systems of support; consult with classroom teachers and families; and help respond in crisis situations (Flaherty et al., 1998; Splett et al., 2017; VanDerwall & Poling, 2021; Zabek et al., 2023). Such shared responsibilities and mutual goals are defining features of collaborative relationships (D‘Amour et al., 2005; Mellin, 2009).
Second, professional guidelines for BCBAs and school mental health specialists alike emphasize the importance of cross-discipline collaboration in service provision. Expectations for behavior analysts to provide services in collaboration with other providers have been made explicit in professional standards dating back to 2010 (BACB, 2010, 2017). The current ethics code for behavior analysts states they must “collaborate with colleagues from their own and other professions in the best interest of clients and stakeholders” (BACB, 2020, p. 11). Collaboration and interdisciplinary teaming feature even more prominently in professional standards for school psychology, school counseling, and school social work (ASCA, 2019; NASP, 2020; NASW, 2012) and have long been endorsed in school mental health (e.g., Michael et al., 2014). Thus, in addition to expectations to collaborate from within the school system, BCBAs and mental health specialists are also professionally bound to do so in the service of the students they support.
Third, the distinct areas of expertise and skillsets brought by BCBAs and mental health specialists present strong potential for interdisciplinary collaboration. Bringing together people with diverse perspectives and expertise is not only a defining feature of interdisciplinary collaboration (Mellin, 2009), but has been identified as a facilitator of successful outcomes for collaborative teaming (Choi & Pak, 2007; Reaves et al., 2022). To illustrate, BCBAs focus on observable and measurable aspects of both behavior and environment, making them well-equipped to assess and intervene on externalizing behaviors and aspects of the classroom context that may contribute to these behaviors. Although mental health specialists attend to classroom environments, they also focus on factors that are not as readily “seen” in the classroom. These include potential stressors outside of school, as well as the thoughts and emotions that intersect with behavior and potentially contribute to difficulties at school (ASCA, 2019). Their training in mental health equips them to address the internalizing symptoms that often co-occur with challenging behavior (Willner et al., 2016). These distinct yet complementary areas of expertise make these specialists uniquely suited to collaborate to support students with SEB challenges.
Despite compelling reasons why BCBAs and mental health specialists should collaborate to support students with SEB challenges, there are also factors that add complexity to this particular partnership. One complicating factor is that the roles of BCBAs in schools are relatively new and still changing (Layden, 2022). In fact, ABA training programs vary widely with respect to the settings in which preservice behavior analysts are trained to practice (Brodhead et al., 2018). And regardless of context, BCBAs have reported receiving very little preparation on collaboration in their training programs (Kelly & Tincani, 2013). This suggests many BCBAs might enter school districts with limited understanding of school-based service delivery and inadequate preparation to collaborate within this system. While school mental health specialists are trained to practice in schools, and on collaboration and consultation models in particular (Michael et al., 2014; Zabek et al., 2023), they may be unfamiliar with BCBA roles and responsibilities. These factors might represent barriers to effective partnerships between BCBAs and school mental health specialists, as mutual understanding of roles, responsibilities, and context-specific challenges can impact the effectiveness of interdisciplinary collaboration (Mellin, 2009; Weist et al., 2006).
Another complicating factor specific to this partnership is a tradition in ABA of discrediting “mentalistic” explanations for behavior—instead relying on observable, measurable, and often proximal aspects of the person’s environment to explain why targeted behaviors are happening (Cooper et al., 2019). While divergent perspectives are in some way essential to interdisciplinary collaboration, discipline-driven philosophical differences (e.g., why challenging behavior happens and how it should be addressed) can also present challenges (Mellin, 2009). In fact, there is some evidence to suggest BCBAs are reluctant to collaborate with or seek input from professionals outside their discipline (Kelly & Tincani, 2013). This challenge is exacerbated by limited opportunities for BCBA professional development in interdisciplinary collaboration (Slim & Reuter-Yuill, 2021). However, there is also reason to believe tides may be shifting toward a new, and potentially more collaborative, approach to ABA (Hanley, 2021; Rohrer et al., 2021). An updated set of professional standards for behavior analysts directs them to “identify and apply interpersonal and other skills (e.g., accepting feedback, listening actively, seeking input, collaborating) to establish and maintain professional relationships” (BACB, 2022, p. 2). Additionally, recent calls to integrate trauma-informed care (Rajaraman et al., 2022), compassionate care (Taylor et al., 2018), and interdisciplinary teaming (LaFrance et al., 2019) into behavior analytic practice suggest a shift toward valuing mental health perspectives.
To our knowledge, no prior empirical studies have focused on collaboration between BCBAs and mental health specialists in schools. In light of the clear expectations for these specialists to collaborate; their potential to partner to address the multiple needs of students with SEB challenges; and the factors that could bring complexity to this partnership, an exploration of BCBAs’ and mental health specialists’ experiences and perspectives on collaboration is needed. Such research has potential to inform strategies for improving the quality of these collaborations, and in turn, the impact of intensive intervention services for students with SEB challenges.
Qualitative Inquiry as a Starting Point
Qualitative inquiry is uniquely suited to studying people’s perspectives, experiences, and impressions in a particular context (Patton, 2015). The open, inductive nature of qualitative inquiry is also of value when there is little empirical research on a topic such that the aim is to explore and discover rather than to predict, test, and confirm (Patton, 2015). For the present study, we chose qualitative inquiry, given the absence of empirical research focused on collaboration between BCBAs and mental health specialists; our interest in these specialists’ perspectives and experiences on collaborating in schools; and our motivation to study collaboration as a necessary step towards improving the quality of interventions for students with SEB challenges. We conducted a series of interviews with BCBAs and mental health specialists to explore, in depth, their contextualized experiences and perspectives on collaborating with one another to support these students. We addressed the following questions: RQ1. To what extent and how did specialists learn to collaborate to support students with SEB challenges? RQ2. What factors did specialists identify as impacting their ability to collaborate effectively? RQ3. What did specialists report needing to better equip them to meaningfully collaborate in their current professional role?
Method
We addressed our research questions by conducting a descriptive qualitative study that involved inductive thematic analysis of standardized open-ended interviews (Patton, 2015). Among the many qualitative approaches, qualitative description offers clear and straight-forward descriptions of a phenomenon as reported by those directly experiencing it (Bradshaw et al., 2017; Sandelowski, 2000). Drawing from naturalistic inquiry, qualitative description allows researchers to “stay close to their data” (Sandelowski, 2000, p. 334). Although all qualitative research is interpretive, qualitative description allows researchers to focus on conceptualizing and reporting themes without making interpretations bound to a specific theory or framework. Importantly, our use of inductive thematic analysis within a descriptive qualitative study aligns with our pragmatic paradigm, which meant our goal was not just to interpret results to understand a phenomenon but to improve practice in the field (Sullivan-Bolyai et al., 2005). More specifically, we made decisions about sampling, data collection, and data analysis based on our desire to gain practical understanding about interdisciplinary collaboration as a real-world issue so that this knowledge could then be used to inform action (Patton, 2015).
Related to positionality, the research team included two faculty members and six graduate students in a department of Special Education with an ABA training program. The first and second authors led data analysis. Both were BCBAs with previous experience providing and evaluating intensive interventions for students with SEB challenges. They brought to this work a belief that BCBAs cannot address the distinct and varied needs of students with SEB challenges alone, and that interventions incorporating multiple domains will have farther-reaching effects than those focused solely on externalizing challenging behavior. Other team members brought varied professional experiences (i.e., supporting students with challenging behavior across a range of settings) and levels of expertise to the coding process. Of note, the second faculty member (last author) specialized in qualitative methods in a distinct area of scholarship (interventions for students with intellectual and developmental disabilities and complex communication needs). Bringing these different vantage points to various stages of the research process was valuable for reflexivity and understanding and addressing potential bias.
District and Participants
Participants were recruited from a large, urban, southeastern school district serving more than 78,000 students. Forty percent of students in the district were Black/African American; 29% were Hispanic; and 26% were White. The district had a substantial number of students who were considered economically disadvantaged (41%) and who were English Language Learners (26%); 12% of students had disabilities (Tennessee Department of Education Report Card, 2020). Two teams of BCBAs (17 total) were employed by the district to support students with behavioral concerns; the larger of the two teams solely served students without disabilities. The district employed more than 400 mental health specialists, yet numbers varied widely by professional role. For example, while there were at least one or two school counselors for each school building, there were only seven trauma specialists across the district.
Twenty-four school specialists participated in this study—nine BCBAs and 15 mental health specialists. The 15 mental health specialists—all of whom were responsible for providing mental health–related supports for students with SEB challenges—represented professionals in a variety of roles within the school mental health service domain. These specialists included four mental health providers (i.e., master’s-level clinicians contracted through the district to provide individualized, clinical mental health supports), three school counselors, three school psychologists, three trauma specialists (i.e., master’s-level professionals responsible for supporting classroom teachers in implementing practices aligned with trauma-informed care), and two school social workers.
Most participants were White (91.7%), female (95.8%), and had master’s degrees (87.5%). These demographics mirror national patterns of over-representation of professionals who identify as White and female in the fields of ABA and psychology/mental health (BACB, n.d.; Goforth et al., 2021; Salsberg et al., 2017). All BCBAs served in a district-level position, in which they supported a regional cluster of schools in the district in a consultative role. In addition to board certification as behavior analysts, two BCBAs reported holding certification as special education teachers. Mental health specialists served in both district-level (n = 6; 3 trauma specialists, 2 school psychologists, 1 social worker) and school-level (n = 9; 4 mental health providers, 3 school counselors, 1 school psychologist, 1 social worker) positions. All but four mental health specialists reported holding relevant certification and/or licensure (e.g., Licensed Clinical Social Worker, National Certified Counselor). Of the four mental health providers, three were Licensed Clinical Social Workers and one was a Licensed Professional Counselor. Most mental health specialists offered both direct and consultative services, excluding mental health providers who only provided direct student support. Participants had served in their current professional role for an average of 5.9 years (range, 1–22). On average, mental health specialists had served in their current roles longer than BCBAs (7.2 and 3.6 years, respectively).
With respect to students supported, seven of nine participating BCBAs reported serving only students without disabilities (one reported serving only students with disabilities and one reported serving both). Eight BCBAs reported providing Tier 3 (i.e., individualized) support. Thirteen of 15 mental health specialists reported serving both students with and without disabilities and 14 reported providing Tier 3 support. Thus, the majority of participating specialists collaborated to support students receiving Tier 3 intervention who were not yet receiving special education services.
Recruitment
To be eligible to participate, participants were required to be a behavior or mental health specialist who (a) provided direct support to students in grades K-8 with SEB challenges or (b) oversaw others in supporting these students. Eligibility was determined based on self-report, and no participants were excluded based on these criteria. We stratified our recruitment efforts to understand both sides of the collaborative relationship (behavior and mental health) and to involve relatively equal numbers of participants in different professional roles within the mental health domain (i.e., at least two per professional role). However, we did not restrict the sample; all specialists who indicated interest were invited to participate.
After receiving research approvals from the district and the university’s Institutional Review Board, the second author sent recruitment emails to 11 district representatives (e.g., behavior support team leads, mental health support coordinators) whose email addresses were publicly available. Recruitment emails were later sent to two school principals for targeted recruitment of school counselors. In these emails, we requested permission to send a study invitation email to behavior specialists (all of whom in this district were BCBAs) or a subset of mental health specialists in the district/school. Seven of the contacted leaders responded and were given the option of sharing a list of email addresses with the research team or forwarding the invitation themselves to potential participants. Because most representatives chose to forward the invitation themselves, we were unable to identify the total number of specialists who were invited to participate.
Interview Protocol Development
We used an iterative process to develop a standardized open-ended interview protocol. The protocol addressed a series of research questions related to collaboration between behavior analysts and mental health specialists, three of which are the focus of this study. This type of interview presents the same open-ended questions in the same sequence to all participants, yet allows flexibility with respect to follow-up questions and probes based on individual responses (Patton, 2015). The interview protocol was also pragmatic, in that we intentionally developed straight-forward questions to gather information with direct practical utility (Patton, 2015). In addition to our research questions, the initial draft of the protocol was informed by (a) existing literature on interdisciplinary collaboration in ABA (e.g., Brodhead, 2015; Kelly & Tincani, 2013; LaFrance et al., 2019) and school mental health (e.g., Mellin, 2009; Splett et al., 2017; Weist et al., 2006); (b) a previously published semistructured interview protocol designed to explore collaborative relationships among school personnel (Biggs et al., 2016); and (c) feedback from a faculty member with experience conducting qualitative interview studies (last author). Table 1 depicts the subset of interview sections and questions aligned to the research questions for this study. The full interview protocol is available in the online supplemental materials.
Interview Protocol Content Aligned to Each Research Question.
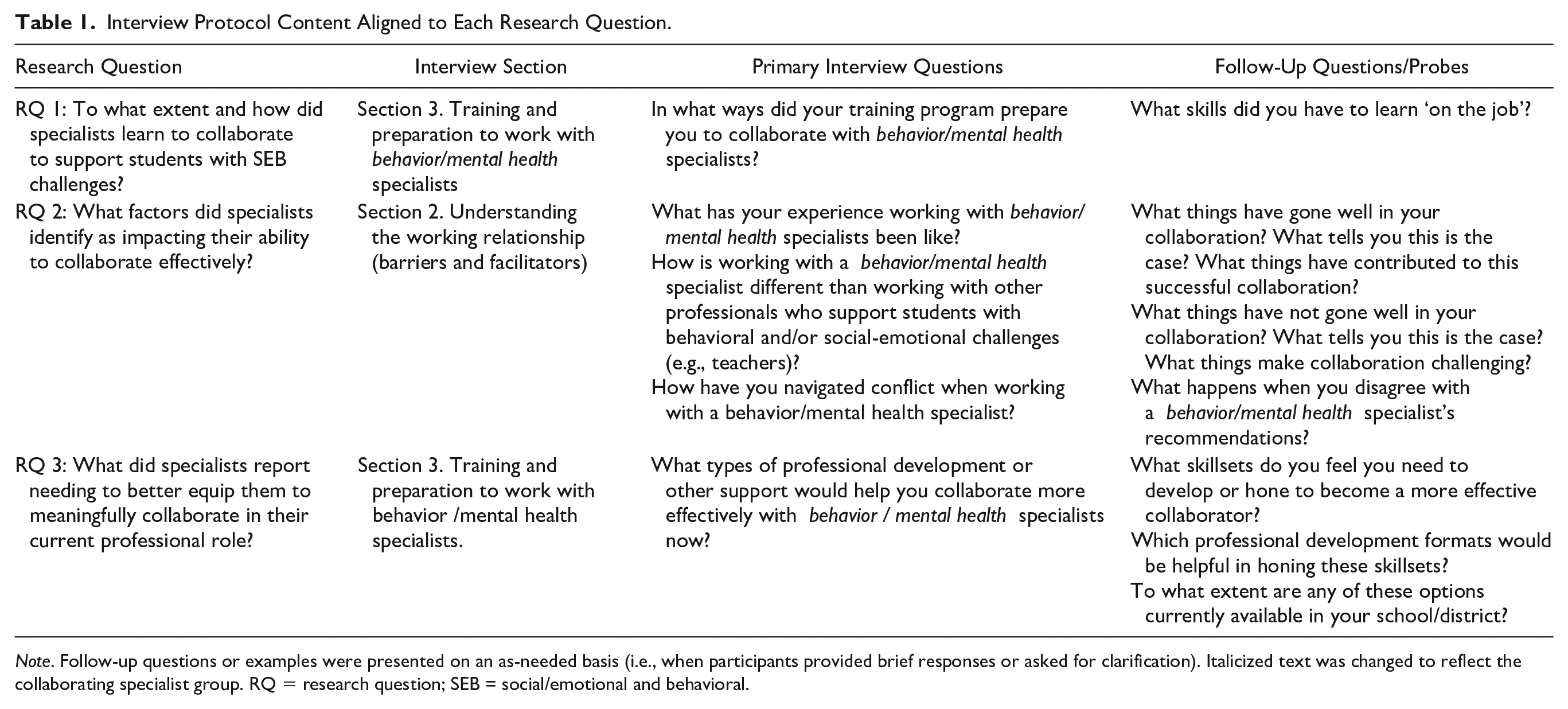
Note. Follow-up questions or examples were presented on an as-needed basis (i.e., when participants provided brief responses or asked for clarification). Italicized text was changed to reflect the collaborating specialist group. RQ = research question; SEB = social/emotional and behavioral.
We solicited and incorporated feedback on the interview protocol from each of two professionals with strong behavioral and mental health backgrounds. One was a clinical faculty member in counseling, with a school counseling background; the other was a BCBA with extensive experience leading district behavior support teams. We then piloted the interview protocol with a university staff member (i.e., Licensed School Counselor) with experiences providing both behavioral and mental health supports in public school settings. We refined the protocol based on their feedback and our own impressions of the interview (e.g., added opportunities for participants to share additional comments on a given topic before moving to the next section). Finally, after reviewing methodological field notes from the first three participant interviews, we made minor protocol refinements, which included adding reminders for the interviewer to the introductory notes as well as potential follow-up questions.
Procedures
After obtaining informed consent via a secure electronic form, we asked each participant to complete a brief online questionnaire for the purpose of gathering background information on participant demographics and their professional roles. We reviewed questionnaire responses in preparation for each interview, noting any specific follow-up or clarification questions based on their entries. Participants then attended one interview via remote video conference with one to two members of the research team. The first author facilitated the majority of interviews (n = 21). The second author facilitated two interviews, and a third member of the research team (doctoral student) facilitated one interview. Mean interview duration was 64.8 min (range, 35–110). All interviews were completed between May 2020 and April 2021, and we noted specialists were working from home (due to the COVID-19 pandemic) in most interviews.
After each interview, the interviewer completed a reflection guide (i.e., field notes; Phillippi & Lauderdale, 2018), where they summarized the main themes they heard from the interview and wrote notes about (a) the context of the interview and its impact on interview quality; (b) the affect of the participant throughout the conversation; (c) any comments that surprised the interviewer and/or challenged their own experiences or expectations; and (d) suggestions for future interviews. These field notes were used for documentation and later reference; the first and second authors discussed any suggestions for future interviews and reached consensus on whether additional adjustments to the interview protocol (e.g., adding example follow-up questions) were warranted.
We completed member checks (Creswell & Miller, 2000; Leko et al., 2021) within 1 week of each interview. We contacted participants via email to share back a summary of main themes from their interview; ask their input on whether they believed these themes accurately described what they talked about; and invite them to share any additional reflections they had since the interview. The purpose of these member checks was to enhance credibility and trustworthiness by providing participants an opportunity to validate, correct, or expand on our interpretations of their responses. Seventeen of the 24 participants (70.1%) responded to the member check, all of whom agreed the main themes we identified accurately reflected their experiences and perspectives. One participant added information that was not captured during the interview, which we added to the corpus of data for analysis.
Data Analysis Procedures
Audio recordings of each interview were transcribed, checked for accuracy, and de-identified. The first round of coding consisted of structural coding (Saldaña, 2021), which refers to flagging excerpts with category-like codes that correspond with research questions. To do this, three doctoral students and a faculty member (the first four authors) first independently reviewed a unique subset of transcripts that included both specialist types, focusing on generating a potential list of structural codes. Each team member then reviewed one another’s lists of potential codes before meeting to collaboratively develop the set of structural codes that would be applied to the full data set. The first author then imported the transcripts into a qualitative data analysis software program (Dedoose, 2022) and two other team members independently coded excerpts from each interview that aligned with each structural code. The structural codes were (a) collaboration preparation, (b) facilitators and barriers, and (c) professional development needs.
The second round of coding involved open coding, during which we used an iterative, collaborative process to further analyze the excerpts within each structural code. Specifically, we used a constant comparative method of data analysis, in which each unit of data was constantly compared to previously coded units (Corbin & Strauss, 2015). This coding round involved several steps. First, each research team member independently reviewed the excerpts flagged within the structural code to generate a preliminary list of open codes (i.e., ideas) based on participants’ comments (Corbin & Strauss, 2015). Examples of preliminary open codes included (a) “no formal training” and “fieldwork” (collaboration preparation structural code), (b) “open-mindedness” and “communication” (facilitators and barriers structural code), and (c) “collaboration skills” and “learning about other specialties” (professional development needs structural code). Second, we met as a team to discuss the preliminary open codes and synthesize each individual’s ideas into one comprehensive set of codes (i.e., an initial codebook draft) that would then be applied to the full data set. Third, one member of the research team took a first pass at applying open codes to the excerpts in Dedoose (2022). For this step, the unit of analysis was a paragraph, although more than one open code could be applied to the same paragraph if multiple themes were identified. The member of the research team who took the first pass updated the codebook if any excerpt contained any ideas not already captured or any content (e.g., descriptions, illustrative examples, salient quotes) that helped define, clarify, or demonstrate the properties and dimensions of an existing open code (Corbin & Strauss, 2015). Fourth, another team member reviewed the coded excerpts, adjusting both the codebook and the codes applied to excerpts in Dedoose (2022) where necessary.
The third round of coding focused on data reduction via examination of connections across the open codes. The first and second authors collaboratively reviewed the codebook and excerpts, synthesizing open codes into themes. We kept an audit trail to document changes to codebooks throughout the coding process (Brantlinger et al., 2005). Finally, our fourth round of coding included full transcript reviews, where we reviewed all transcripts in full to search for confirming and disconfirming evidence for each theme (Leko et al., 2021). Two team members (the first or second author and another team member) independently reviewed each transcript in full, examining coded excerpts and searching for participant comments that addressed the research questions but (a) were not captured in the codebook or (b) contradicted the contents of the codebook. The first and second authors met to discuss outcomes from this coding round and made updates to the codebook as necessary. Specifically, we added one new theme for Research Question 1 (Training Experiences Discouraging Collaboration) and expanded the descriptions of several existing themes. We did not find evidence in opposition of any themes. A list of the final themes is presented in Figure 1.
Representation of Themes by Research Question and Specialist Group.
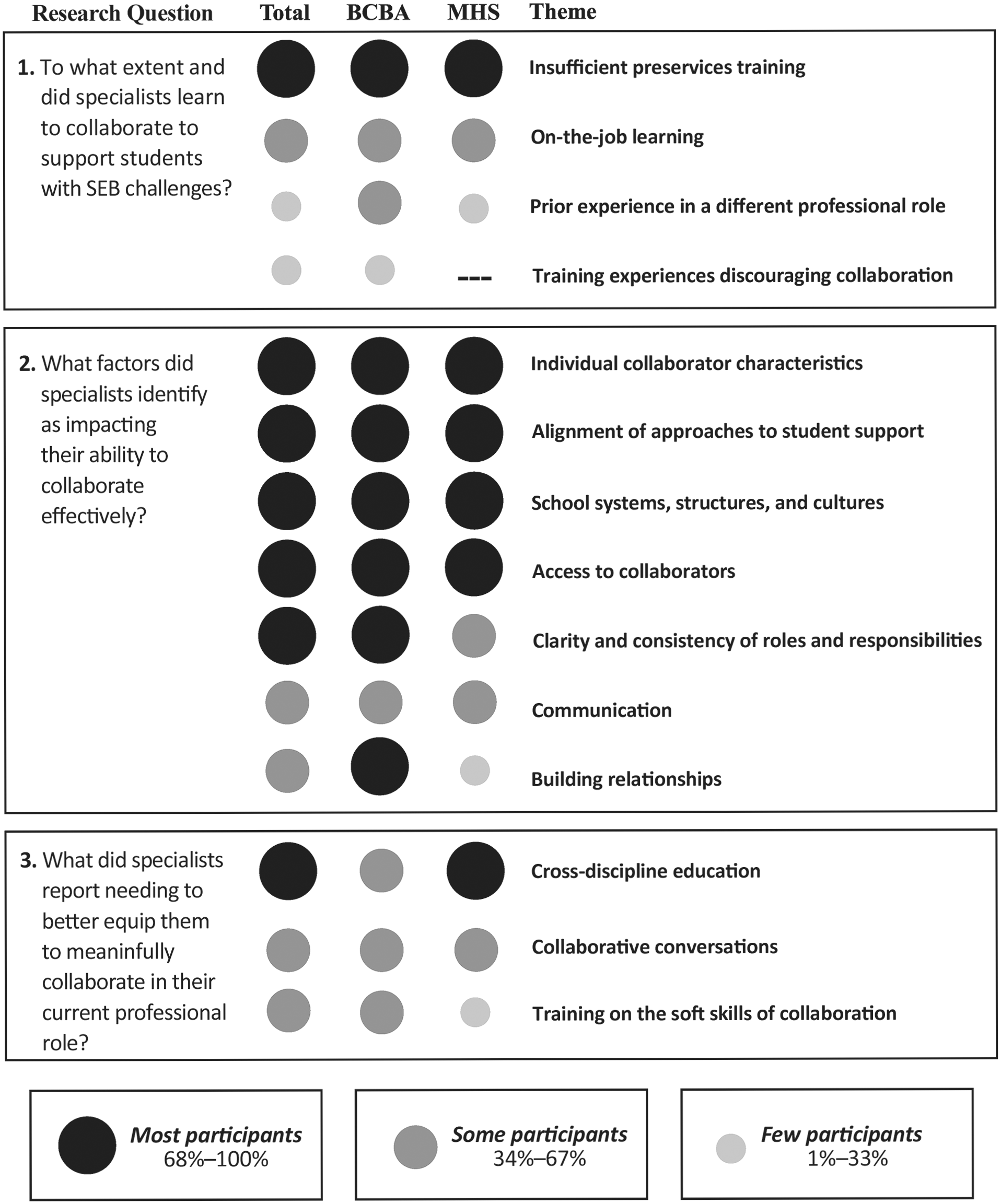
After qualitative analysis was complete, we sought to describe the extent to which each identified theme was mentioned within and across specialist groups. We calculated the number and percentage of mental health specialists, BCBAs, and all participating specialists who made at least one comment that was coded to a given theme. To facilitate appropriate interpretation of these quantitized data (i.e., describing patterns without the intent to generalize percentages to a broader population; Sandelowski et al., 2009), we created a visual summary displaying the portion of specialists within and across groups who mentioned each theme (see Figure 1).
Results
Research Question 1: To What Extent and How Did Specialists Learn to Collaborate?
Specialists’ reflections on their preparation to collaborate revealed four themes: (a) insufficient preservice training; (b) on-the-job learning; (c) prior experience in a different professional role; and (d) training experiences discouraging collaboration. The top panel of Figure 1 shows the portion of participants (within and across specialist groups) who mentioned each of these themes.
Insufficient Preservice Training
All participants (n = 24; 100%) described their preservice training programs as insufficient with respect to preparing them to collaborate with the other specialist group. Some specialists said they lacked any formal training on interdisciplinary collaboration. For example, a mental health provider said, “I don’t remember ever taking a class on collaboration.” (M03). A BCBA shared a similar sentiment, noting that the lack of preparation for collaboration she experienced was common across behavior analytic training programs: “I’ve been in a couple [training] programs and [I] supervise students from different programs, and there’s not really anything that’s teaching us how to be . . . that collaborative person.” (B15). Another BCBA portrayed her training program’s instruction on collaboration as superficial, describing it as “focused on not being a know-it-all [expletive] . . . rather than really understanding the training these [related service providers] have and how they might be approaching [their work]” (B11).
Some mental health specialists acknowledged aspects of their preservice training program (e.g., coursework and field experiences) addressed collaboration in general, but did not focus on specific professional roles. A mental health provider described her training in the area of collaboration as “just very general, you know, teaching you how to collaborate with anybody that you might be working with . . . communicating and cooperating and being part of a team” (M02). Importantly, none of the mental health specialists reported any formal preparation to collaborate specifically with behavior specialists. One school psychologist shared, “In my graduate program we had a collaboration class where we collaborated with general education teachers . . . but we never collaborated with BCBAs. . . . In my behavior class—where we actually did FBA and BIP—there was no collaboration whatsoever” (M19). In fact, several mental health specialists noted that behavior analysts were not mentioned as potential collaborators in their preservice preparation. As one school psychologist put it, BCBAs were not “even someone we talked about existing when I was in my training program” (M17). Similarly, a mental health provider commented “I didn’t even know what a behavior specialist was during my actual training” (M02). And a trauma specialist with a master’s degree in social work said, “until I worked in a school, I don’t think I had any understanding of what behavior specialists did or do—and I really wish I had more understanding” (M06).
On-the-Job Learning
Eleven specialists (44.4% of BCBAs; 46.7% of mental health specialists) emphasized they learned collaboration skills while on the job. A BCBA, who was previously a special educator, said, Even going to school as a special education teacher—like when I had to plan IEP [Individualized Education Program] meetings—it was all new—nobody taught me any of that stuff. And then, for ABA, I mean, I feel like it [learning to collaborate] is all on-the-job. (B13)
Another BCBA described her experience as “trial by fire,” saying: “I’ve never really been trained [to collaborate]. . . . It’s really just been this process of working with all these different professionals. . . . And everyone plays different roles . . . so it’s like, how do I fit in on this team?” (B24). Mental health specialists offered similar sentiments. A school counselor described not learning to collaborate until “I started having challenging kids and I needed to connect them to somebody that was outside my scope of practice” (M08). When asked how she learned to collaborate with behavior specialists, a mental health provider said, “I think most of it I’ve learned by trial and error” (M03).
Some specialists—mostly those in mental health—described taking purposeful actions while on the job to learn how to collaborate in their current role. For example, a trauma specialist mentioned shadowing other team members; a school psychologist talked with colleagues and read books on collaboration; a social worker actively built relationships with interdisciplinary team members; and a school counselor worked to stay abreast of what other specialists were doing with students on her caseload.
Prior Experience in a Different Professional Role
Seven specialists (55.6% of BCBAs; 13.3% of mental health specialists) reported that prior experience in a different professional role (e.g., classroom teacher) or work context helped prepare them for collaboration. One BCBA who previously worked as an early childhood specialist shared how that role helped prepare her for collaboration: “You’re really looking at the whole team—the parent, the child, the teacher . . . and you’re bringing them together as a team” (B25). Another BCBA reflected on her previous experience on a grant-funded project implementing the Pyramid Model (Hemmeter et al., 2021) in Pre-K classrooms. As part of that project, she partnered with a social/emotional learning coach, which shifted her entire approach: I went from being . . . very individual, working on my own island, to really just . . . inviting everybody in. . . . I didn’t do that before. I was the expert. . . . I wrote behavior plans in my office without hardly any input from anybody. (B26)
A mental health provider said, “I was a certified teacher so I think that probably gave me more guidance on collaboration than my social work background” (M03). She went on to say, I think my training in teaching middle school and my work with middle schoolers helps me collaborate better in the classroom and understand what is difficult for a teacher to incorporate in a classroom . . . because sometimes the plans that they [BCBAs] wanted to do are just impossible for teachers. (M03)
Training Experiences Discouraging Collaboration
Three BCBAs mentioned learning to collaborate with mental health specialists in spite of their formal ABA training, which emphasized perspectives that were inconsistent with—and sometimes actively opposed to—mental health perspectives. One BCBA suggested her training program discredited the field of mental health by suggesting she should “stay away from that zone” (B25). She identified this aspect of her training as contributing to her mindset when she entered the field, which she described as “I’m not even going to be open to some of that [mental health] stuff” (B25). Another BCBA reported questioning their instructors’ stance on mentalism during training: “Going through the BCBA coursework, I remember talking about mentalism and how that’s not measurable. . . . And I remember sitting there going, are you kidding me?” (B24). A third BCBA described how her approach to collaboration had changed dramatically since her training: We laughed at counselors . . . we’re like “it’s not science, and there’s not real data.” . . . and that’s the perspective I had originally. . . . It took some rounds of having really positive experiences with psychologists . . . and counselors and social workers to say, “Oh, you do have lots of value to add into this; I need to listen to you . . .” . . But I was literally not primed for that and taught something opposite than what is actually true. (B15)
Research Question 2: Facilitators and Barriers to Effective Interdisciplinary Collaboration
We identified seven factors that were perceived to facilitate and/or inhibit collaboration: (a) individual collaborator characteristics; (b) alignment of approaches to student support; (c) school systems, structures, and cultures; (d) access to collaborators; (e) clarity and consistency of roles and responsibilities; (f) communication; and (g) building relationships. The middle panel of Figure 1 shows the portion of participants who mentioned each of these factors.
Individual Collaborator Characteristics
Twenty-three specialists (88.9% of BCBAs; 100% of mental health specialists) reported their ability to collaborate effectively depended on individual characteristics of their collaborator. The word “open” was repeatedly used by BCBAs and mental health specialists to describe what facilitated more effective collaboration, including: “open minded” (M09; B24); “open to collaboration” (B26); “open to feedback” (M07); “openness and understanding” (M05); “open to bring us in” (M06); “open to being wrong” (M18); “open to the fact that you don’t know” (M19); “open dialogue and open communication” (M29); “open to ideas . . . open to everyone’s input . . . open to other strategies . . . open to changing practices” (B25). Other characteristics framed as facilitators (and mentioned across specialist groups) included being respectful, a team player, knowledgeable, competent, transparent, a good listener, empathetic, curious, and willing to learn. Mental health specialists also mentioned characteristics as facilitators that were not addressed by BCBAs, including: available, humble, flexible, innovative, inviting, and insightful. With respect to characteristics framed as barriers, both specialist groups mentioned being closed-minded, disrespectful, difficult to work with, unapproachable, and territorial. Other characteristics perceived as barriers were only mentioned by BCBAs (i.e., defensive, unreliable, unresponsive, unwilling to learn new things, negative) or by mental health specialists (i.e., condescending, rigid, unaware).
Alignment of Approaches to Student Support
Twenty-one specialists (100% of BCBAs; 80.0% of mental health specialists) explained that a factor impacting collaboration was the degree of alignment between approaches to supporting students. Several specialists expressed that having distinct and complementary approaches facilitated collaboration. For example, one mental health provider said, It’s like the Venn diagram. . . . There’s definitely some overlap there, but whereas I might be more focused on teaching the child some self-calming down or grounding skills. . . the behavior specialist’s goal is [to] get the kid back in a classroom doing their work and support the teacher in doing so. (M04)
A BCBA described it as “We sharpen each other’s saws so much . . . making each other better” (B26). Similarly, a social worker noted “the collaboration is so key because we both do different things. But when we marry them, they work really well together” (M28). Alternatively, one trauma specialist described instances of “territorialism” and “feather ruffling” when approaches overlapped too much, “because we were trying to figure out where we best fit in” (M09).
Some BCBAs also noted that having different approaches to student support could inhibit collaboration, particularly when they disagreed with other specialists about the extent to which a given approach was considered “best practice,” aligned with their field’s ethical guidelines, or considered feasible for classroom implementation. For example, one BCBA offered an example about disagreeing with a mental health specialist’s recommended response to challenging behavior: A certain regulation activity may go against what the function of behavior is, and in my mind [it] may be reinforcing the [challenging] behavior. But [according to] . . . a trauma specialist, we have to use that to regulate the student first. (B25)
Another BCBA felt some resistance from colleagues to the scientific approach underlying ABA: Most of the time I feel like people are willing to hear my perspective or understand the behavioral perspective, but they have to believe in the science of behavior. . . . Some don’t. Some think that reinforcement should not be happening. (B15)
School Systems, Structures, and Cultures
Twenty specialists (88.9% of BCBAs; 80.0% of mental health specialists) suggested aspects of the broader system, structure, or culture in which they worked inhibited their ability to collaborate effectively. With respect to staff shortages and unmanageable workloads, a counselor put it bluntly: “I don’t think we can truly collaborate well with anyone until they reduce the workload on teachers, social workers, counselors, and behavior specialists” (M29). Others echoed this sentiment, noting “we just don’t have enough people” (B23). Specialists also pointed out problems related to who the policy-level decision makers were in the district. A school counselor indicated such decisions are made by “people who have been outside of the classroom for too long, not working with students, not working with teachers” as opposed to “the people who have an understanding of what’s happening . . . in the trenches” (M10). Other specialists referenced structural issues with district- and school-level referral systems, as well as structural barriers between teams supported by different sources of district funding.
Other aspects of this theme focused on the extent to which district and school leadership fostered a culture of collaboration in their schools—starting with communicating expectations to collaborate and providing the guidance and supports to do so. For example, one mental health provider reported that as a therapist, “we’re not required or expected to really have any collaboration . . . it’s up to us whether we want to collaborate” (M07). Other specialists indicated disconnects between expectations and available supports to collaborate. For example, a BCBA noted “It’s just interesting they [district administration] talk about collaboration, yet they don’t give us the fundamentals to collaborate—to do our job.” (B12). Several specialists underscored the impact school-level administrators can make on the collaboration process. A social worker summed it up this way: I think so much of it depends on the administration in a building—how good of a communicator they are; how good of a relationship builder they are; and how effectively they are able to support their staff. And organize when there’s a lot of need. (M28)
Behavior analysts echoed this sentiment, with one saying “I think as [school] administrators, they need to foster that feeling or sense of community—to really give a sense that this is a team approach” (B12).
Access to Collaborators
Limited access to collaborators was identified as a barrier by 19 specialists (88.9% of BCBAs; 73.3% of mental health specialists). Although this barrier was mentioned by both specialist groups, it concerned limited access to BCBAs in particular. Mental health specialists noted BCBAs are “spread very, very thin” (M04), while BCBAs acknowledged the same, describing their own caseloads as “out of this world” (B20). Several mental health specialists lamented the impacts of these large caseloads across multiple schools, with one school counselor stating, “they’re just not around . . . they swoop in, they observe the kid, and then they swoop out” (M29). A positive comment by a school psychologist underscored the rarity of accessing BCBAs, noting how helpful it was to “actually see the behavior specialist” (M17). Some mental health specialists also expressed feeling excluded from contexts where collaboration could take place. One mental health provider shared, I was constantly being left out of IEP meetings, manifestation meetings, even after being there for several years. . . . That’s a common frustration among all school-based therapists for sure. . . . They know we’re working with this kid and they don’t invite us to IEP meetings . . . it’s very frustrating. (M07)
Similarly, a BCBA expressed a desire to include mental health specialists in more decision-making meetings: I almost wish that . . . for every process or every meeting, there would at least be one person—trauma . . . specialist or a social worker or someone—that would be at those meetings. . . . Because I think every student would benefit from having ideas brought to the table from those specialists. (B25)
Clarity and Consistency of Roles and Responsibilities
Seventeen specialists (88.9% of BCBAs; 60.0% of mental health specialists) described how the clarity and consistency of their and their colleagues’ professional roles impacted collaboration. This factor was primarily framed as a barrier related to a lack of understanding of what different specialists—primarily BCBAs—do. According to a behavior analyst, “Some people still don’t know what we do and it’s really discouraging. I feel like sometimes we aren’t being used appropriately” (B12). Mental health specialists shared a similar sentiment, with one trauma specialist noting, “When I got hired, no one was like, ‘here is exactly what the BCBA does and what their role is in a school.’ . . . I just kind of had to figure that out” (M06). A social worker echoed this experience, saying “I didn’t know what a BCBA was. . . . I kind of had to, like, build a relationship with our BCBA to figure out what they do and . . . how best to engage them when we had a need” (M28).
Both specialist groups also acknowledged that roles and responsibilities varied widely by district, school, and individual specialist—another factor that can make collaboration difficult. A BCBA noted that “one of the big struggles is there’s no uniformity . . . in terms of what these roles and responsibilities need to be” (B20). Another BCBA described it as “everybody just brings their own individual kinds of experiences . . . [or] their bag of tricks to the situation” (B24). A trauma specialist said, “it feels like the social workers, the counselors, the school psychologists —their roles differ from school to school based on how the school wants to use them” (M06).
Communication
Fourteen specialists (55.6% of BCBAs; 60.0% of mental health specialists) emphasized the impact of communication on collaboration, framing communication as both a facilitator and a barrier. Frequent communication was perceived to make collaboration easier. A school counselor felt that “regular communication is really important—especially in a school setting” (M29). Another counselor described her positive experience with behavior analysts being “fantastic about checking in. And seeing about, not only the progress of a student . . . but checking in with our staff to make sure the process is working for them” (M10). One BCBA felt frustrated about infrequent communication by mental health specialists, stating “they’re just not communicating quick enough” (B15).
Specialists also emphasized the importance of communication quality. Both mental health and behavior specialists identified behavior analytic jargon as a barrier to effective communication. One BCBA questioned the helpfulness of using such technical language: “What’s our ultimate goal? Sounding smart? Sounding like, super technical? Or is it to actually see change? . . . I’ve talked to some [mental health specialists] that feel really intimidated by people on our team” (B26). Along the same lines, mental health specialists viewed the tone of many behavior specialists as a barrier. For example, one counselor said “I think sometimes the way they [BCBAs] talk to us can be kind of condescending. . . . It’s more like they’re instructing versus collaborating” (M29). Similarly, according to a school psychologist, I’ve had experiences [collaborating] that have not been good, but it is generally . . . the behavior analyst’s communication style. I appreciate you being an expert in this area, but don’t think that I’m not. I don’t care for that. (M19)
The same school psychologist offered the following advice to BCBAs: “You might know a lot about your field of study, but you do not have a whole picture. . . . Be open to the fact that you don’t know and allow others to enlighten you” (M19).
Building Relationships
The importance of building relationships with colleagues was mentioned by 11 specialists (77.8% of BCBAs; 26.7% of mental health specialists). Specialists emphasized that to facilitate collaboration, relationships should be mutually beneficial, with colleagues meeting each other on equal ground. One counselor described it in these terms: For me, collaboration comes down to relationship. And it’s more than . . . I do for you, you do for me; it’s really about seeing the uniqueness and somebody’s ability to help you do the work that you do, and hopefully they learn from you, and you learn from them; and it becomes this process where it’s mutually necessary and rewarding for both of you. (M10)
Specialists also described how certain aspects of collaboration, such as navigating conflict or disagreements, are much harder when you do not have an established relationship to build on. A BCBA said, If I haven’t already put in a lot of time building a relationship with some of my counselors, then me trying to ‘call them out’ on something that’s reinforcing a behavior we don’t want to see . . . that usually goes south quickly. (B11)
A counselor highlighted a similar sentiment, stating “I don’t feel my relationship is strong enough with our [behavior specialist] to be able to voice any concerns” (M29).
Research Question 3: Supports for More Effective Collaboration
We identified three themes representing distinct categories of support specialists needed to better collaborate: (a) cross-discipline education, (b) collaborative conversations, and (c) training on the soft skills of collaboration. All specialists confirmed their proposed supports were not already available in their district, to their knowledge. The bottom panel of Figure 1 shows the portion of participants who mentioned each theme.
Cross-Discipline Education
Seventeen specialists (66.7% of BCBAs; 73.3% of mental health specialists) expressed interest in formal training opportunities to learn about their collaborators’ discipline. Specialists from both groups mentioned wanting to know more about their collaborators’ philosophies, how they were trained, and the ethical guidelines informing their practice. In particular, several mental health specialists expressed a need to better understand the roles BCBAs play. A mental health provider suggested “a training educating all of us school-based therapists on exactly what they [BCBAs] do, what their roles are” (M07). Another mental health provider said, “I’d like a presentation around, you know, this is what behavior specialists are trained in; this is how [they] think; this is how [they] function; these are the tools [they] use” (M04).
Some BCBAs expressed a desire to better understand the interventions and support strategies used by mental health specialists, including ones they could potentially incorporate in their own practice. For example, one BCBA said, “I definitely want to learn more about interventions for more traditional mental health issues; more strategies to help with anxiety. I see a lot of kids with anxiety, and a lot of times, traditional behavioral techniques don’t work with them.” (B24). Other BCBAs seemed more interested in understanding the evidence base supporting mental health interventions. For example, one BCBA commented, “I want them [mental health specialists] to tell me about the research . . . how they arrived to where they are . . . what their data says” (B11). In addition to the comments themselves, the tone used by these BCBAs seemed to call into question the validity of approaches used by mental health specialists: “I need to see the science, or I need to see proof” (B15).
Collaborative Conversations
Fourteen specialists (55.6% of BCBAs; 60.0% of mental health specialists) expressed a desire to bring both specialist groups together to share perspectives and problem-solve on equal footing (as opposed to one group training the other). One counselor said, I would love opportunities to sit down at a table with behavior analysts and understand a little bit more about where they’re coming from . . . I want to know what lenses [they] see through and then build from there. (M10)
Similarly, a BCBA described “bringing in a school psychologist, school counselor, behavior analyst, trauma specialist, restorative practice specialist, social-emotional learning specialist—all these layers that we have—with an end goal of: What are we going to do to support students?” (B26). Other specialists suggested the value of coming together to practice problem-solving based on hypothetical scenarios. For example, a trauma specialist described a hypothetical workshop that
gives us . . . scenarios, and I say how I would deal with it; you say, as a BCBA, how you deal with it, so we can get [your] perspective on things and also argue it out—like a safe place to talk. (M09)
Several specialists described these interactive learning opportunities as preferred over traditional lecture-style formats. For example, one BCBA described hands-on, collaborative learning activities as “more effective than sitting in a lecture hall, or someone throwing materials at me. I don’t find that to be an effective way for me to learn” (B16). Within the collaborative conversations theme, specialists also emphasized that these collaborative meetings should be done preventatively, proactively, and with consistency—as opposed to only calling such meetings in times of crisis.
Training on the Soft Skills of Collaboration
Nine specialists (55.6% of BCBAs; 26.7% of mental health specialists) expressed a need for support on the “soft skills” of collaboration. A BCBA suggested having “broader trainings on collaboration, like, here are some best practices . . . I think that as a district, a lot of people could really use training on how to collaborate” (B23). Another BCBA said, “I think more professional development on different modes of collaboration would be helpful. Just learning how to collaborate, what exactly does that look like? What kind of questions should I be asking? When are different modalities [needed]?” (B12). A few mental health specialists identified similar needs. For example, a school psychologist said, “We can all use more conflict management training, and just those soft skills of collaboration” (M18). A social worker emphasized the importance of self-awareness training:
I think we get a lot of professional development on strategies and approaches to address “a thing,” but—particularly with collaboration—to me, that first step is self-awareness . . . if you’re not aware of your approach [to collaboration], it’s much harder to differentiate it when you come across other people that it’s just not effective with. (M28)
Beyond the nine specialists who initiated the idea of needing training on these soft skills, several other specialists commented on the importance of interpersonal skills when they were asked what skills they felt they needed to hone. Specialists mentioned listening, turn-taking, asking the “right” questions, having difficult conversations, giving and accepting constructive feedback, compromising, and “diffusing high emotional situations” (M18). Specialists also identified navigating situations where they disagreed with colleagues as an area for growth. In particular, several specialists referenced struggling to advocate for what they thought was best for a student when their views were different from those of a collaborator. For example, a school counselor reported wanting to “work on being more assertive because I am still very quick to back down . . . I would like to be able to voice my opinions more” (M29). Similarly, a trauma specialist said “I don’t always speak up when I am not sure about something or when I disagree with something . . . I haven’t quite developed those skills, but that is something I hope to acquire” (M06). Behavior analysts also expressed a desire for supports embedded in their day-to-day practice. For example, one BCBA wanted an expert mentor to
come help me at an S-team [student support team meeting] and tell me, what could I have said differently? Or what questions could I have thought of? . . . Give me that feedback so that I’m able to build my skills. (B12)
Discussion
The goal of this study was to learn about behavior and mental health specialists’ perspectives on their preparation to collaborate with one another; the factors that affect the quality of these collaborations; and what supports they need to partner more effectively. We used a qualitative description approach and pragmatic research paradigm to collect and synthesize straight-forward responses about real-world issues with potential to inform practice (Bradshaw et al., 2017; Patton, 2015; Sandelowski, 2000). We highlight key findings from each research question and identify their implications for practice and research.
Overall, specialists reported that their preservice training programs came up short with respect to preparing them to collaborate with one another. However, distinctions emerged between BCBAs and mental health specialists. A repeated sentiment from mental health specialists was that, regardless of the extent to which their training program emphasized collaboration, there was no mention of BCBAs—or behavior specialists in general—as potential collaborators in schools. Behavior analysts, on the other hand, spoke more to a general lack of focus on interdisciplinary collaboration, regardless of professional role. The missing focus on collaboration in preservice training expressed by BCBAs (and to some extent, mental health specialists) is consistent with results of initial survey research focused on BCBAs and collaboration (Kelly & Tincani, 2013). However, our results revealed an additional barrier, in that some BCBAs reported experiencing active opposition to mental health perspectives as part of their training. This finding suggests there may be unique barriers to this particular partnership, especially for newly minted BCBAs who are trained in programs with limited emphasis on or access to school or other interdisciplinary settings.
The themes related to specialists’ preparation to collaborate point to several ways preservice training programs in ABA and school mental health domains might better prepare these professionals to collaborate in their future practice. First, open channels of communication between these professional groups should start in preservice training. Program faculty in each discipline might invite school-based practitioners from the other discipline to speak to their students, explaining who they are, what they do, and how their service provision intersects with the other specialist group (see Boivin et al., 2021). Such exposure might better equip preservice professionals to acknowledge and leverage the benefits of divergent philosophies around student support (Mellin, 2009). Second, regardless of the degree of theoretical overlap, ABA training programs should acknowledge mental health specialists as valuable partners, as many students who need intensive behavioral interventions also need and benefit from mental health supports (Fazel et al., 2014). Third, as evidenced by recent priorities among federal funding agencies and faculty who contribute to personnel preparation (e.g., Foxx & Anderson, 2020; Office of Special Education Programs, 2022), interdisciplinary programs that train future specialists side-by-side might help cultivate cultures of collaboration. In particular, interdisciplinary courses and fieldwork in local school districts or university-affiliated laboratory schools have potential to address gaps in preparation and pre-empt barriers to effective collaboration.
Results of this study also revealed a variety of factors that specialists identified as impacting their ability to collaborate effectively with the other specialist group—many of which align with conceptual models of interdisciplinary collaboration (e.g., Mellin, 2009). Some themes addressed systems-level factors that were primarily framed as barriers (i.e., School Systems, Structures, and Cultures; Access to Collaborators; Clarity and Consistency of Roles and Responsibilities). However, the most commonly identified factors were contextual influences (Mellin, 2009) related to the individuals with whom the specialist was collaborating (i.e., Individual Collaborator Characteristics; Approaches to Student Support). Specialists reflected that their ability to collaborate effectively depended on whether their collaborator was open-minded and was a reliable and respectful communicator. Specialists from both groups also alluded to advantages of partnering with colleagues who have complementary approaches to student support (e.g., perspectives and skillsets). This “Venn diagram” of training and expertise has been identified as an important component of interdisciplinary collaboration in both school mental health and behavior analytic literatures (e.g., Mellin, 2009; Summers et al., 2022). The importance of complementary approaches seems especially relevant for specialists who support students with SEB challenges, whose needs span multiple domains.
Reflections from a subset of BCBAs, however, seemed to focus on scenarios in which their approach to student support differed substantially from those of mental health specialists, leading to tension in the collaborative relationship. As several participating specialists alluded, some behavior analytic traditions have historically discredited “mentalistic” explanations of behavior (Hayes & Brownstein, 1986). This could point to an inherent challenge in integrating behavior analytic and mental health perspectives when supporting students with SEB challenges. Alternatively, such patterns might be indicative of a resistance to nonbehavioral perspectives and approaches unique to the BCBA community (Giangreco et al., 2021) or the programs in which they are trained (see Training Experiences Discouraging Collaboration). Indeed, we detected other signals of potential resistance among BCBAs across multiple themes and both specialist groups. For example, mental health specialists identified “rigidity” as a characteristic that inhibits their collaboration with BCBAs and described the tone of communication from some BCBAs as “condescending.” Additionally, when discussing needs for cross-discipline education, some comments by BCBAs seemed to question the evidence base informing certain mental health interventions. Although these signals of potential BCBA resistance were few and far between, they are worth acknowledging as they are consistent with prior discussion and preliminary evidence identifying resistance to nonbehavioral approaches as a unique barrier to collaboration in the field of ABA (e.g., Brodhead, 2015; Kelly & Tincani, 2013).
Finally, when asked what supports they needed to collaborate more effectively, specialists shared a variety of ideas. Given their insufficient preservice training, it was not surprising that many specialists expressed interest in learning more about their collaborators’ discipline (ABA or mental health), as well as the “soft skills” of collaboration. With respect to format, specialists from both groups expressed a desire for “non-traditional” professional development opportunities, including purposeful collaborative conversations with specialists from other domains and opportunities to practice collaborating with ongoing feedback from a coach or mentor. Specialists’ reflections also seemed to center around a need for experiential—as opposed to merely didactic—learning opportunities. These reflections mirror calls for collaborative, hands-on, and problem-oriented training for school-based personnel who support students with intensive intervention needs (Foxx & Anderson, 2020).
Limitations
Our results should be considered in light of the following limitations. First, though generalizable outcomes were not the goal of this qualitative study, characteristics of our study sample may have limited the breadth of perspectives shared. For example, our sample of specialists were homogenous with respect to gender and race/ethnicity—most were White women. Though we included more total mental health specialists than BCBAs, it is also worth noting our small number of BCBAs represented a larger proportion of all BCBAs in the district relative to proportions represented by any mental health specialist role. We purposefully sampled mental health specialists from a variety of professional roles because each played a part in SEB service provision (Zabek et al., 2023). In addition, our focus on specialists in a single school district also may have limited the breadth of experiences shared. However, unique features of this district allowed an in-depth exploration of varying experiences and perspectives within a system where opportunities for collaboration should be present. For example, this was a district with two behavior support teams, the larger of which served students without disabilities—likely maximizing caseload overlap with those of mental health specialists.
Results should also be considered in light of the qualitative description approach we took to this study, where we looked for straight-forward, unadorned responses to our research questions. Other approaches to qualitative inquiry, such as phenomenology, ethnography, or grounded theory, would have produced different—and perhaps more nuanced—findings. In addition, the voluntary nature of this study may mean participating specialists had a bias toward supporting collaboration. We did, however, capture a range of perspectives and experiences (both positive and negative) among our participants. Finally, to share back interview themes with participants in a timely manner, we completed our member checks before we formally and iteratively analyzed study data. Thus, while participating specialists had the opportunity to review and respond to a summary of themes from their own interview, they did not share input on how we coded, categorized, and summarized themes across specialists.
Future Research
The results and limitations of this study also point to several worthy avenues for future research. First, researchers might conduct larger-scale survey studies to investigate the generalizability of themes identified in this qualitative analysis related to preservice training, factors impacting collaborative practice, and desired in-service supports. Such studies might also help reveal distinctions among different mental health specialist professions or behavior specialists who are not BCBAs. Second, more interdisciplinary research is needed to better understand potential discipline-driven differences in philosophies and mindsets between BCBAs and mental health specialists, as well as other important collaborators (e.g., special educators, child psychiatrists), and how these differences impact collaboration and service delivery. Third, perspectives of classroom teachers who support students with SEB challenges should also be explored, considering they are often responsible for implementing practices recommended by collaborating BCBAs and mental health specialists. Understanding teachers’ experiences as the consultee in this professional triad would likely reveal additional avenues for making these collaborative partnerships more effective. Finally, intervention research related to interdisciplinary collaboration is needed (e.g., Bates et al., 2019). This includes both the development of systems that lead to stronger collaboration among various members of student support teams, as well as empirical evaluations of the impact of these collaborations on intervention outcomes for students with SEB challenges.
Conclusion
Interdisciplinary collaboration is a critical feature of service delivery for students who face emotional and behavioral barriers to learning. In this study, we explored partnerships between school-based BCBAs and mental health specialists to support students with SEB challenges. Research addressing this distinct partnership is needed to identify barriers and needs that may be unique to these two specialist groups and their focus on intensive intervention. On the whole, the BCBAs and mental health specialists we interviewed expressed a desire and willingness to collaborate with one another, even as they acknowledged the challenges and barriers they faced on a day-to-day basis. While representing specialists from a single district, results of this study point to ways we might better prepare, equip, and support school-based BCBAs and mental health specialists to collaborate effectively, and in doing so, increase the impacts of intensive intervention services for students with SEB challenges.
Supplemental Material
sj-docx-1-bhd-10.1177_01987429231225623 – Supplemental material for Perspectives of Behavior Analysts and Mental Health Specialists on Collaborating to Support Students with Intensive Intervention Needs
Supplemental material, sj-docx-1-bhd-10.1177_01987429231225623 for Perspectives of Behavior Analysts and Mental Health Specialists on Collaborating to Support Students with Intensive Intervention Needs by Marney S. Pollack, Blair P. Lloyd, Gabrielle E. Crowell, Matthew A. Santini and Elizabeth E. Biggs in Behavioral Disorders
Footnotes
Acknowledgements
The authors thank Emily Baran, Olivia Reznik, Ellie Hancock, and Cassie Gray for their assistance with data collection and analysis. They also thank the participating specialists who generously shared their time with them in the midst of an unprecedented school year. Marney S. Pollack is now at the A.J. Pappanikou Center for Excellence in Developmental Disabilities, University of Connecticut Health Center (mpollack@uchc.edu).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Support for this research was provided by the Office of Special Education Programs, U.S. Department of Education (Grant no. H325D170005), and a Student Research Grant from the Association for Positive Behavior Support (APBS).
Supplemental Material
Supplemental material for this article is available on the Behavioral Disorders website with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.