
Abstract
A national study of clinical directors examined professional development (PD) focused on mental health provided to professionals in juvenile justice facilities for adjudicated youth. A total of 85 clinical directors responded to a mail survey (45% return rate). The survey questions related to (a) topics of staff training and the basis for choosing topics, (b) which professionals participated in each PD topic, (c) training format and frequency of PD, (d) recommended attributes of PD, (e) methods of evaluating PD, and (f) adequacy of PD and how can it be improved. For each topic, PD was typically provided once per year and face to face, rather than online. PD participation rates were commonly in the 30% and 40% ranges for professionals other than clinical directors and counselors, with teachers, correctional officers, administrators, and teaching assistants receiving PD the least. Rarely did PD include recommended attributes of PD, and it was commonly viewed as ineffective. Implications for research and practice related to PD and its relationship to youth reentry from juvenile justice facilities are discussed.
For many incarcerated youth, preparation and opportunities for eventual reentry and reintegration into school, community, and the workforce are complicated from the point of intake (Gagnon et al., 2018). The mental health characteristics of incarcerated youth provide a significant challenge to staff in juvenile justice (JJ) facilities. Prevalence studies have indicated that 70% of youth in JJ facilities, or about three times more than youth in the general population, exhibit a mental disorder (Shufelt & Cocozza, 2006). Specifically, 45% of JJ youth have a substance use disorder (McClelland et al., 2004). Shufelt and Cocozza also reported that almost 50% of JJ youth have conduct disorder and JJ-involved youth are two to four times more likely to have attention-deficit/hyperactivity disorder (ADHD) than youth in the general population (Fazel et al., 2008). In addition, 95% of JJ youth have experienced trauma (Becker & Kerig, 2011) and 25% meet criteria for posttraumatic stress disorder (PTSD; Dierkhising et al., 2013). Compared with youth in the community, higher percentages of JJ youth also have anxiety disorder (Wasserman et al., 2005) and depression (Shufelt & Cocozza, 2006; Weiss & Garber, 2013). In addition to mental disorders, JJ youth have troubled histories. For example, 30% have experienced physical abuse and 12% have suffered sexual abuse (Baglivio & Epps, 2016). Moreover, past-year suicide ideation and attempts by JJ youth are about double that of youth in the community (Teplin et al., 2015).
The U.S. Departments of Education and Justice (2014) have recognized the critical importance of understanding and addressing the social–emotional, mental, and behavioral health issues in preparing incarcerated youth for successful transitions out of JJ facilities. In facilities for adjudicated youth, a variety of JJ personnel have the daily responsibility of identifying and addressing the intense and complex mental health needs and histories of youth (Grisso & Vincent, 2005). For example, clinical directors, counselors, case managers, nurses, social workers, administrators, correctional officers (COs), teachers, and teaching assistants are all responsible for supervising, providing services to, and interacting with youth that have experienced major trauma (Becker & Kerig, 2011). Effective youth transition out of the facility is predicated on coordination and collaboration of professionals from multiple areas and systems within a JJ facility that have a common knowledge base of youth mental health needs and research-based approaches to intervening (Griller-Clark et al., 2016).
The significance of addressing youth mental health as a component of effective transition planning and services is well established. Externalizing mental health disorders and, specifically, conduct disorder, ADHD, and substance use disorder are associated with increased recidivism (Schubert & Mulvey, 2014; Wibbelink et al., 2017). Schubert and Mulvey (2014) also noted that comorbid internalizing and externalizing disorders were linked to recidivism (Wibbelink et al., 2017). Other researchers (Becker et al., 2012; Cottle et al., 2001; Mulder et al., 2011) have identified that anxiety, PTSD, and a history of physical and sexual abuse are also associated with recidivism.
Despite the importance of providing mental health supports to incarcerated youth, it has long been acknowledged that the inadequate training of professionals in JJ has stymied the provision of mental health services, ultimately inhibiting their reintegration (Federal Advisory Committee on Juvenile Justice, 2006; Gagnon et al., 2012; Mellin & Pertuit, 2009; Meservey & Skwyra, 2015). Granted, the preparedness of professionals certainly varies across disciplines and professions. For example, JJ clinical directors and counselors have an established knowledge base concerning incarcerated youth mental health. Similarly, social workers have the training and skill set to appropriately assist in providing evidence-based mental health interventions to incarcerated youth (de Saxe Zerden et al., 2019). In contrast, Stinchcomb (2001) noted that 88% of agencies hiring COs required that they have only a high school education. It is unsurprising that these professionals often rely on “excessively punitive or ineffective strategies that can unintentionally worsen a youth’s mental health symptoms” (Meservey & Skwyra, 2015, p. 3). COs, who have the most contact with youth and possibility for intervening regularly (Holt, 2011), have asserted their lack of mental health training, particularly concerning substance abuse, and reported that they are in dire need of professional development (PD) focusing on youth mental health needs (Penn et al., 2005).
Available evidence also suggests that school administrators, teachers, and teacher aides are unprepared to support youth with mental disorders and traumatic histories. Although there is no information concerning the previous mental health training of JJ facility administrators, limited research indicates that principal preparation does not typically address youth mental health needs (Caparelli, 2011). Similarly, although not specific to JJ, research indicates that teachers do not possess the knowledge or training to support youth mental health or even effectively implement behavioral interventions (Franklin et al., 2012). Moreover, JJ teachers are less qualified than their regular public school counterparts (Mason-Williams & Gagnon, 2017). JJ teaching assistants can be an important part of a treatment team and their many roles and responsibilities, particularly with providing direct support to youth, require a clear understanding of mental health–related topics. Again, available research is limited to public schools. However, Fisher and Peasants (2012) reported that teaching assistants obtained their training on the job, rather than formally. The authors also noted that 80% of teaching assistants had obtained only a high school diploma or passed the General Education Development (GED) test.
Although there is no research on the educational training of JJ case managers, the Council for Accreditation (n.d.) identifies only that case managers should be, “qualified by a bachelor’s degree in a social or human service field, and experience working with youth” (p. 31). Similarly, information on the specific training of JJ nurses does not exist. However, it is clear that nurses within public schools and in JJ are an informed and crucial resource for the identification and provision of mental health supports to youth (Bohnenkamp et al., 2015).
Mental Health–Related PD
Given concerns with the formal mental health–related training of JJ staff, there is increasing interest in the PD opportunities provided in JJ. In a recent national study, lead clinical JJ staff overwhelmingly reported that training was the greatest barrier to implementing evidence-based mental health interventions and ensuring that youth mental health needs are adequately met (Swank & Gagnon, 2016). Underwood and Washington (2016) also noted that inadequate PD in JJ is a serious barrier to providing youth with the mental health services and supports they need. One major initiative for providing mental health–related PD in JJ is the Mental Health Training Curriculum for Juvenile Justice (MHTC-JJ). “MHTC-JJ is a one-day training for juvenile justice staff that focuses on adolescent development, mental health disorders and treatment, the critical role of families, and practical strategies for engaging and interacting with youth” (Campaign for Youth Justice, 2014). Although important, concerns remain that a single day of training is insufficient in terms of the breadth and depth needed for JJ professionals with varied backgrounds to obtain the knowledge and skills necessary to assist incarcerated youth.
PD Topics
When considering the PD topics related to youth mental health, it is critical that professionals understand aspects of and interventions for the aforementioned mental disorders that are prevalent in the JJ youth population. Additional mental health–related topics may also inform the approaches that JJ professionals take to assist youth. For example, the National Research Council (2013) emphasized using developmentally informed practices. When practices in JJ are not informed by adolescent development, they may interfere with youth cognitive, social, and emotional growth and maturity, as well as educational attainment, which may increase factors leading to juvenile crime (Steinberg, 2009). Available evidence suggests that few JJ professionals provide programs designed to meet youth developmental needs (Henderson et al., 2007). Similarly, although positive and proactive behavioral interventions are among the most beneficial approaches in JJ settings (Lipsey, 2009), few professionals are knowledgeable of effective behavioral interventions (Gagnon et al., 2018; Oliver & Reschly, 2010). No research has evaluated the extent to which JJ PD focused on these topics.
Additional PD topics are relevant to JJ professionals. In light of the high percentage of JJ-involved youth that have experienced trauma or have a conduct disorder, it is not surprising that youth are at substantial risk for being perpetrators or victims of aggression and harming themselves or others (Archer et al., 2010; Teplin et al., 2002). As such, JJ professionals need PD on helping youth with anger management (Griffin et al., 2012). Also, there are ongoing concerns with youth inability to reintegrate into school, the community, and workforce (Gagnon & Barber, 2019). As such, it is important that JJ professionals have PD on implementing programs and interventions focusing on developing youth life skills and anger management in preparation for reintegratation. No information is available on the existence of PD on these topics.
Three other areas for PD are particularly relevant to JJ professionals themselves, to ensure that they can provide the best possible support and safety for youth. For those professionals that work with incarcerated youth, there are often competing demands to maintain a distance from youth and providing the appropriate support and guidance to promote their reintegration into society (Chan & Henry, 2014). PD designed to promote the ability of professionals to appropriately build supportive relationships with youth is even more critical, given that few JJ-involved youth have a history of trusted relationships with adults (Todis et al., 2001). JJ professionals also have a high-stress job with the potential for physical harm, as well as day-to-day interactions with youth with serious behavioral and mental health needs (Ford & Blaustein, 2013; Meservey & Skwyra, 2015). The researchers noted that PD focusing on self-care and burnout has the potential for providing important coping strategies. Again, no research has addressed the existence of PD for JJ staff on these issues.
In addition to the actual topics of PD, there is no available information concerning who decides on PD topics in JJ settings. There is some evidence that staff selection of PD topics, in general, can improve motivation and implementation (Lyon et al., 2011).
Recipients of PD
Professionals, including clinical directors, counselors, case managers, nurses, social workers, administrators, COs, teachers, and teacher assistants, must all have PD on essential topics if they are to collaborate and support incarcerated youth effectively (Gagnon et al., 2012; Houchins et al., 2012). Collaboration is a cornerstone of effective transition planning for incarcerated youth (Griller-Clark et al., 2016). Advocates strongly support the facility-wide training of JJ professionals to ensure a common understanding of youth and critical issues that relate to educating and rehabilitating them (de Azúa, 2018), especially given that some JJ professionals may have only high school education and no knowledge of how to meet the complex mental health needs of youth (Stinchcomb, 2001). However, there are no national data indicating which professionals in JJ receive mental health–related PD.
Training Format and Frequency of PD
There is a long-standing concern that professionals in JJ settings are isolated from other professionals in their fields and have inconsistent access to PD (Gagnon et al., 2013). Moreover, difficulties may exist with the logistics of providing JJ professionals from multiple departments within the facility the necessary time to participate in PD, let alone opportunities for facility-wide training. Although there is no available research on the use of online, face-to-face, or blended (i.e., combined online and face-to-face) PD in JJ, research in other settings indicates that there is no appreciable difference in learning outcomes when comparing online and face-to-face PD (Fishman et al., 2013). Moreover, online PD may provide needed flexibility to maximize learning and the time professionals have for face-to-face PD (Nelson et al., 2010). There is a need for information on the extent to which JJ facilities rely on face-to-face, blended, or online PD, and if there are certain topics for which a certain approach is more commonly used.
Although there are no national studies on the frequency of mental health–related PD in JJ facilities, reports indicate that PD in these settings is typically limited to a single day (Campaign for Youth Justice, 2014; Gagnon et al., 2013) and staff feel that the length of training is often inadequate (Meservey & Skwyra, 2015). Stand-alone mental health workshops lasting a few days or less are typically ineffective (Beidas & Kendall, 2010; Lyon et al., 2011). There is a need for information on the frequency of PD for important topics related to the mental health of incarcerated youth.
Recommended Attributes of PD
Although there is a dearth of research on PD in JJ, researchers have recommended four attributes that increase the likelihood that PD will be effective and useful. For example, researchers (Houchins et al., 2012) recommend training focus on evidence-based practices (EBPs). However, there is no known research identifying the extent to which JJ mental health–related PD focuses on EBPs. Also, providing multidisciplinary PD is important for facility-wide implementation of skills and practices learned during PD. Researchers (Leone & Weinberg, 2010) identified multidisciplinary training as an important initial step to promoting communication and collaboration among professionals from different departments within JJ. It is also critical that PD move beyond “one-shot” and brief trainings, and provide sufficient opportunities for professionals to generalize interventions to various situations (Gagnon et al., 2013). Finally, to support staff implementation of new knowledge and skills, follow-up support and assistance with implementation are critical (Mathur et al., 2009; Nelson et al., 2010).
Evaluating and Adequacy of PD
Despite the importance of evaluating PD, it is one of the most common components that is omitted from the PD process (Gagnon et al., 2012; Mathur et al., 2009). Although there is a need for national research to identify approaches used in JJ settings to evaluate training, it is also important to identify the extent to which training is viewed as adequate and what is needed to improve PD within JJ facilities.
Study Purpose
Given the need for and lack of national information concerning mental health–related PD in JJ settings, we solicited responses from JJ clinical directors to six questions: (a) Which topics are included in PD and what is the basis for choosing certain topics? (b) Which staff participate in PD? (c) What is the training format (i.e., face-to-face, online, combined) and frequency of PD? (d) What recommended attributes are used when providing PD? (e) What approaches are used to evaluate PD? (f) What is the adequacy of PD and how can it be improved?
Method
This is a cross-sectional descriptive survey study designed to provide a snapshot of PD in JJ settings. As no previous research has examined mental health–related PD for staff in JJ and given the limitations of survey research, the goal was to provide a broad, initial understanding of PD.
Participants
The target population consisted of clinical directors working at JJ settings throughout the United States. Eligible participants included the clinical director at each secure JJ setting that serves adjudicated youth or a combination of adjudicated and detained youth. Facilities serving only detained youth and wilderness camps were excluded. An existing list of facilities was used that the authors had previously identified (see Swank & Gagnon, 2016, 2017). The initial list was derived from the 2012 Directory: Adult and Juvenile Correctional Departments, Institutions, Agencies, and Probation and Parole Authorities (American Correctional Association 2012), as well as website reviews and phone call verifications with state JJ departments. In addition, for this study, a research assistant contacted each state JJ department by phone, and their websites were reviewed to ensure the list of facilities was current. The research assistant verified that each facility had a clinical director that was not shared with other facilities to ensure that duplicate surveys were not completed by any clinical director.
No published research identifies the primary person responsible for mental health–related PD in JJ. As such, the choice to survey clinical directors was based on two factors: (a) the first author’s extensive work with JJ facilities and (b) example job descriptions for JJ clinical directors in Colorado (State of Colorado Job Opportunities, 2019) and Massachusetts (NFI Massachusetts, 2019), which included duties to plan for and direct PD.
A total of 189 facilities were identified that met the inclusion criteria for the study. Staff at 85 facilities completed the survey, a 45% response rate. Facilities in 37 states and the District of Columbia participated in the study. Regarding the number of youth at each facility, 2.35% (n = 2) housed one to 10 youth, 8.24% (n = 7) housed 11 to 20, 31.77% (n = 27) housed 21 to 50, 27.06% (n = 23) housed 51 to 100, 15.29% (n = 13) housed 101 to 150, 5.88% (n = 5) housed 151 to 200, and 9.41% (n = 8) housed more than 200. There were 11.8% (n = 10) of facilities that reported serving only females, 61.2% (n = 52) only males, and 27.0% (n = 23) serving both females and males. With regard to the age of youth in the facilities, youth ages ranged from (a) 12 to 18 (n = 28); (b) 13 to 18 (n = 24); (c) 12 to 17 (n = 5); (d) 14 to 18 (n = 11); (e) 15 to 18 (n = 1); (f) 16 to 18 (n = 5); (g) 13 to 17 (n = 3); (h) 18-year-olds (n = 1); and (i) youth more than 18 (n = 7).
In total, 81.7% (n = 67) of facilities identified as being public, 7.3% (n = 6) as private nonprofit, and 11.0% (n = 9) as for-profit. Regarding accreditation, 25 programs reported having American Correctional Association accreditation, 13 reported National Commission on Correctional Health Care accreditation, 0 reported Joint Commission on Accreditation of Healthcare Organizations accreditation, and 28 reported no accreditation. In addition, participants had the opportunity to indicate additional accreditations: Four facilities listed Performance-based Standards for Youth Correction and Detention Facilities, two listed Commission on Accreditation of Rehabilitation Facilities, one listed substance abuse overlay, one listed North Central Association for Colleges and Schools, one listed Center for the Application of Substance Abuse Technologies, and three listed state accreditation. Furthermore, 48.2% (n = 41) of the facilities reported serving one or more special populations, including 31 serving youth with substance abuse, 24 serving sexual offenders, 16 serving youth with mental health needs, one serving violent offenders, and one serving youth with developmental disabilities.
Instrument
The authors used an iterative process to develop a survey focusing on the mental health PD provided to professionals (i.e., clinical directors, counselors, case managers, nurses, social workers, administrators, COs, teachers, and teacher assistants) within JJ, as well as to obtain basic facility and student demographics. An initial survey was drafted based on a review of research, professional expertise in JJ, and through consultation with professionals with expertise in JJ and mental health. Consistent with Swank and Gagnon (2016), we provided the initial draft to three researchers with expertise in JJ. Next, three clinical staff from JJ facilities reviewed the revised drafts. Finally, two experts in survey development provided feedback and final revisions were completed. Similar to previous national survey research on exclusionary schools, each group provided recommendations regarding, “(a) layout of the survey; (b) ease of directions; (c) clarity of questions, (d) consistency between research questions and survey categories and questions; (e) importance of the categories and specific questions; and (f) recommendations for additional categories or questions” (Gagnon & McLaughlin, 2004, p. 265).
Survey content validity was assessed using Item Content Validity Index (I-CVI). Consistent with recommendations from Armstrong et al. (2005), a panel of seven experts reviewed the survey and rated the relevance of each item using a four-point ordinal scale (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, 4 = highly relevant). Polit et al. (2007) suggested that item-level CVI (I-CVI) values of .78 and lower are evidence for item revision or deletion. For four questions, the I-CVI was .71 (i.e., Is PD provided focusing on bipolar disorder? Do trainings promote collaboration and conversation across disciplines? Do trainings include the presentation of case studies? Do trainings include dialogue/discussions?), and these questions were deleted.
Although three other questions were also at .71, they were not deleted. Specifically, experts ranked the inclusion of conduct disorder as a PD topic rather low. However, given that 50% of JJ youth have conduct disorder (Shufelt & Cocozza, 2006), this topic was maintained. Next, whether each training topic was adequate (Choices: disagree, neutral, agree) and the frequency that PD addressed each topic (Choices: once, once per year, twice per year, three or more times per year) were asked for each PD topic. Survey length prevented the possibility of more detailed question choices for participants and the general nature of the responses resulted in low I-CVI. The limitations of including these questions with very broad response choices is acknowledged, but these questions and choices were maintained to provide at least an initial query into topics that have not been addressed in previous research.
The remaining items had I-CVIs of either .86 (n = 4) or 1.00 (n = 26). In addition, Polit et al. (2007) recommended calculating scale-level CVI, universal agreement (S-CVI/Ave), by averaging all item-level CVIs. Values of .90 and higher are considered acceptable evidence of content validity. In this study, S-CVI/Ave was .96.
In addition to questions on facility characteristics (e.g., facility size, public or private, accreditation, if the facility served specialized group of youth) and youth characteristics (e.g., gender served, ages of youth), the survey included five major sections: (a) training topics provided to staff; (b) who receives training; (c) planning, delivery, and evaluation of training; (d) training attributes; and (e) quality of training.
Clinical directors were directed to respond concerning the mental health training provided at the facility and not on outside training in which staff may participate. To identify training topics, the authors first reviewed the prevalence data of common mental disorders and histories of incarcerated youth and identified eight topics (e.g., addictions [drugs/alcohol], ADHD, anxiety, conduct disorder, depression, physical/sexual abuse, suicide risk/prevention, trauma/PTSD). In addition, some broad approaches to youth mental health and behavioral concerns that have been recommended by experts in the field were included (e.g., adolescent development, behavioral approaches, anger management, life skills development, relationship building with youth), as well as staff self-care and burnout. These served as the PD topics included in the survey. Next, we identified key facility staff that are likely to come in contact with youth and need a degree of understanding of youth and appropriate interventions (e.g., administrators, teachers, teaching assistants, clinical directors, counselors, social workers, case managers, COs, nurses). Study participants could mark on the survey if each professional received PD on each topic. A specific time frame for participation in PD was not identified.
The next section of the survey queried respondents on the planning, delivery, and evaluation of PD. Specifically, four survey questions were included that focused on (a) the methods upon which PD topics were decided (e.g., state/federal requirements, accreditation requirements, address facility issues, staff suggestions, component of program evaluation process); (b) whether PD for each topic was provided face-to-face, online, or combined; (c) the frequency that each PD topic was provided (e.g., training is provided once, once per year, twice per year, three or more times per year); and (d) the methods for evaluating PD (e.g., written evaluation, evaluations linked with program outcomes, evaluating implementation, not evaluated).
The final survey also included sections on the presence of recommended training attributes and respondent views on the quality of PD. In terms of training attributes, respondents rated that (a) trainings are focused on evidence-based/best practices in working with adolescents in correctional facilities; (b) trainings are multidisciplinary; (c) trainings provide sufficient PD to generalize interventions to various situations; and (d) there is a plan to assist personnel in implementing new knowledge and skills following training. Available responses were not at all, some of the time, or most of the time. Concerning the quality of PD, participants were asked to indicate their agreement that PD on each topic was adequate (disagree, neutral, agree) and, if the PD was inadequate, what was needed for improvement (more training, resources, follow-up/support).
Data Collection and Management
Institutional review board (IRB) approval was obtained prior to initiating the study. The survey, consent form, a small incentive (US $2 bill for the first mailing and a US $5 gift card for the second mailing), and a return envelope with postage paid was mailed to the clinical director at each facility. Participants also received a link for the online version of the survey constructed through Qualtrics that resembled the hard copy version. Thus, participants had the opportunity to complete the printed or online version of the survey. Three survey mailings were conducted.
Specific procedures were implemented for data entry to minimize nonsampling errors introduced by data transfer. The research assistant received training in data entry and was provided ongoing feedback, corrective measures, and additional training, as needed. Three approaches to checking for coding errors in the data entered were implemented, consistent with De Vaus (1995). First, a valid range check was completed. Second, filter checks were conducted. The first author reviewed the database to ensure that no contingency-question items were answered if not appropriate. Third, logical checks were conducted to review the data entered and identify illogical codes (e.g., a letter was used instead of a number). Data were examined for patterns within missing data.
Data Analysis
Given that the goal of the current survey was to obtain a broad snapshot of the state of mental health–related PD in JJ, the analysis consisted of descriptive statistics (i.e., frequency, percent). In cases where participants were asked to “check all that apply” (e.g., barriers to providing quality PD; see Table 4), only frequency was calculated.
Results
Topics of PD and Basis for Choosing Topics
Regarding the selection of PD topic areas and the basis for choosing them, topics were typically decided by state/federal requirements (n = 68), facility issues that need to be addressed (n = 64), or staff suggestions (n = 51). Fewer facilities relied on accreditation requirements (n = 38), or topics associated with a program evaluation process (n = 30). Respondents reported which PD was provided at their facility. The percentage of facilities providing PD on a given topic was in the 70% and 80% range (see Table 1, Column 1). The most commonly offered PD was suicide risk/prevention (100%) and behavioral approaches (90.6%). The PD topic offered least was self-care and burnout (61.1%).
Professional Development: Number of Facilities Covering Topics and Participating Staff.
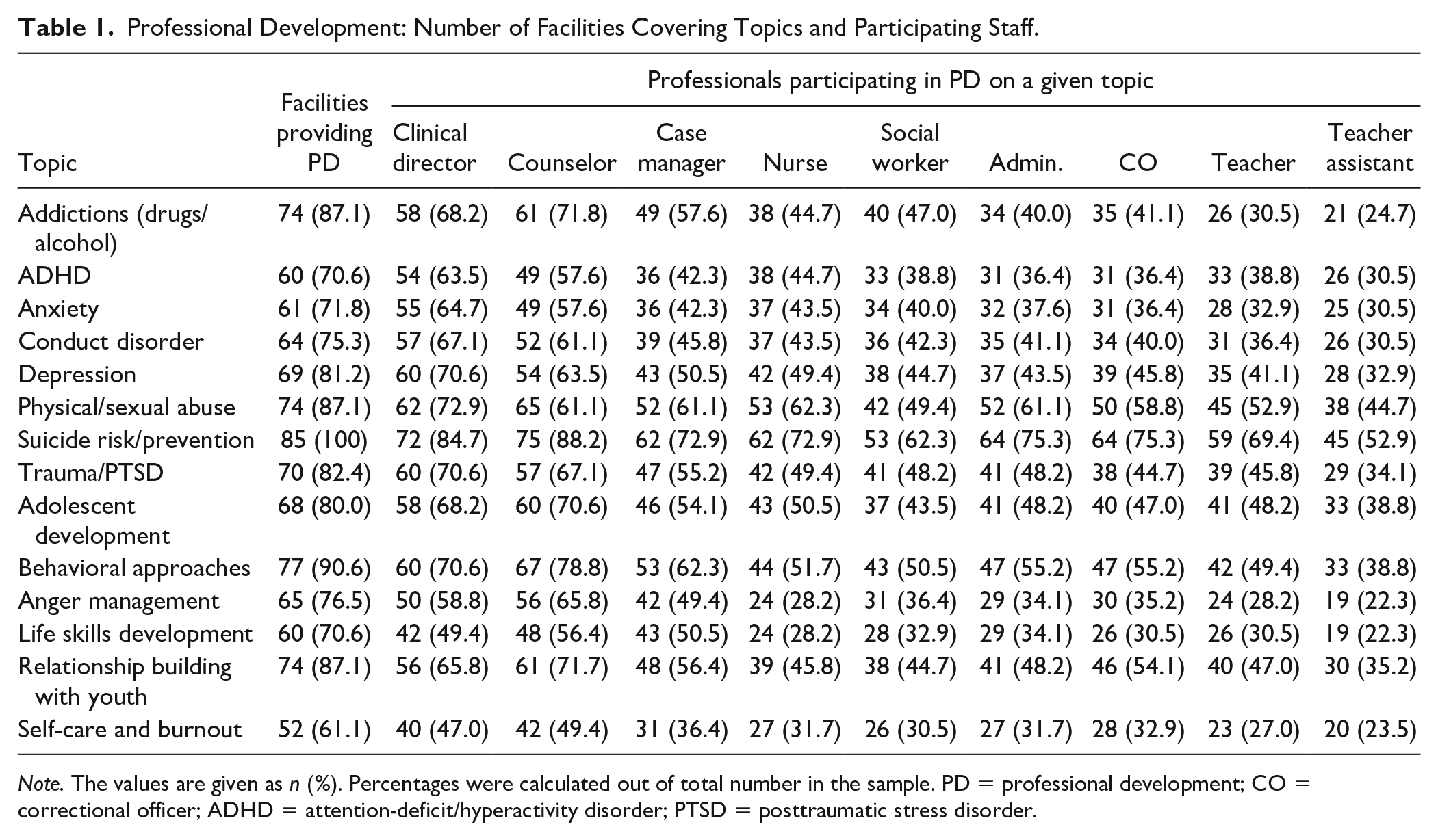
Note. The values are given as n (%). Percentages were calculated out of total number in the sample. PD = professional development; CO = correctional officer; ADHD = attention-deficit/hyperactivity disorder; PTSD = posttraumatic stress disorder.
Staff Participation in PD
The percent of professionals that received PD on any given topic (see Table 1, Columns 2–10) was low, with only suicide risk/prevention exceeding 80% and then only for clinical directors and counselors. Every professional participated most frequently in PD on suicide risk/prevention, and for all but two professionals (i.e., counselors, case managers), physical/sexual abuse. Excluding suicide risk/prevention and physical/sexual abuse, behavioral approaches was the most frequent PD topic for teaching assistants (38.8%), teachers (49.4%), COs (55.2%), administrators (55.2%), social workers (50.5%), nurses (51.7%), case managers (62.3%), and counselors (78.8%). For clinical directors, three topics tied at 70.6% (i.e., depression, trauma/PTSD, behavioral approaches).
Participation in any PD topic was low for all professionals and can be divided into five general categories. Clinical director and counselor PD participation for specific topics tended to be in the 60% (n = 7) and 70% (n = 4) ranges. For case managers, they typically participated in the 40% (n = 4) and 50% (n = 6) ranges. Nurse participation was somewhat varied, but they most commonly participated in the 40% (n = 7) range. Administrators, COs, and teachers most commonly participated in the 30% (n = 4, n = 5, n = 5, respectively) and 40% (n = 6, n = 5, n = 5, respectively) ranges. Teacher assistants participated in PD the least of all professionals, with participation in the 20% (n = 4) and 30% (n = 8) ranges.
Characteristics of PD Provided
Results are presented in two categories: (a) training format and frequency of PD; and (b) the use of recommended attributes when providing PD.
Training format and frequency of PD
Table 2 provides information on the frequency and percent of respondents that reported their facility used face-to-face, online, or combined approaches to PD by each training topic. Respondents were asked to respond in general, rather than for each type of professional. In terms of the training format, most topics were presented in a face-to-face format, with 10 topics in the 70% range and five in the 60% range. Rarely did facilities provide PD solely online. For two topics, the percentage of facilities that provided combined face-to-face and online training exceeded 30% (i.e., addictions, physical/sexual abuse). In terms of frequency that a given PD topic was covered (see Table 2), the questions were also designed to provide a broad indicator of the frequency that PD on a given topic was provided (i.e., once, once per year, twice per year, three or more times per year). The question did not ask participants to identify frequency for each professional, but in the aggregate. The most common response was once per year for all but two topics (i.e., adolescent development, anger management), where the PD was provided once. The provision of PD on a given topic twice per year only exceeded 10% for relationship building with youth (11.8%). The frequency that PD was provided three or more times per year exceeded 10% for nine topics (addictions, physical/sexual abuse, suicide risk/prevention, trauma/PTSD, adolescent development, behavioral approaches, anger management, life skills development, relationship building with youth) and never rose above 16.2%.
Approach to Training and Frequency.
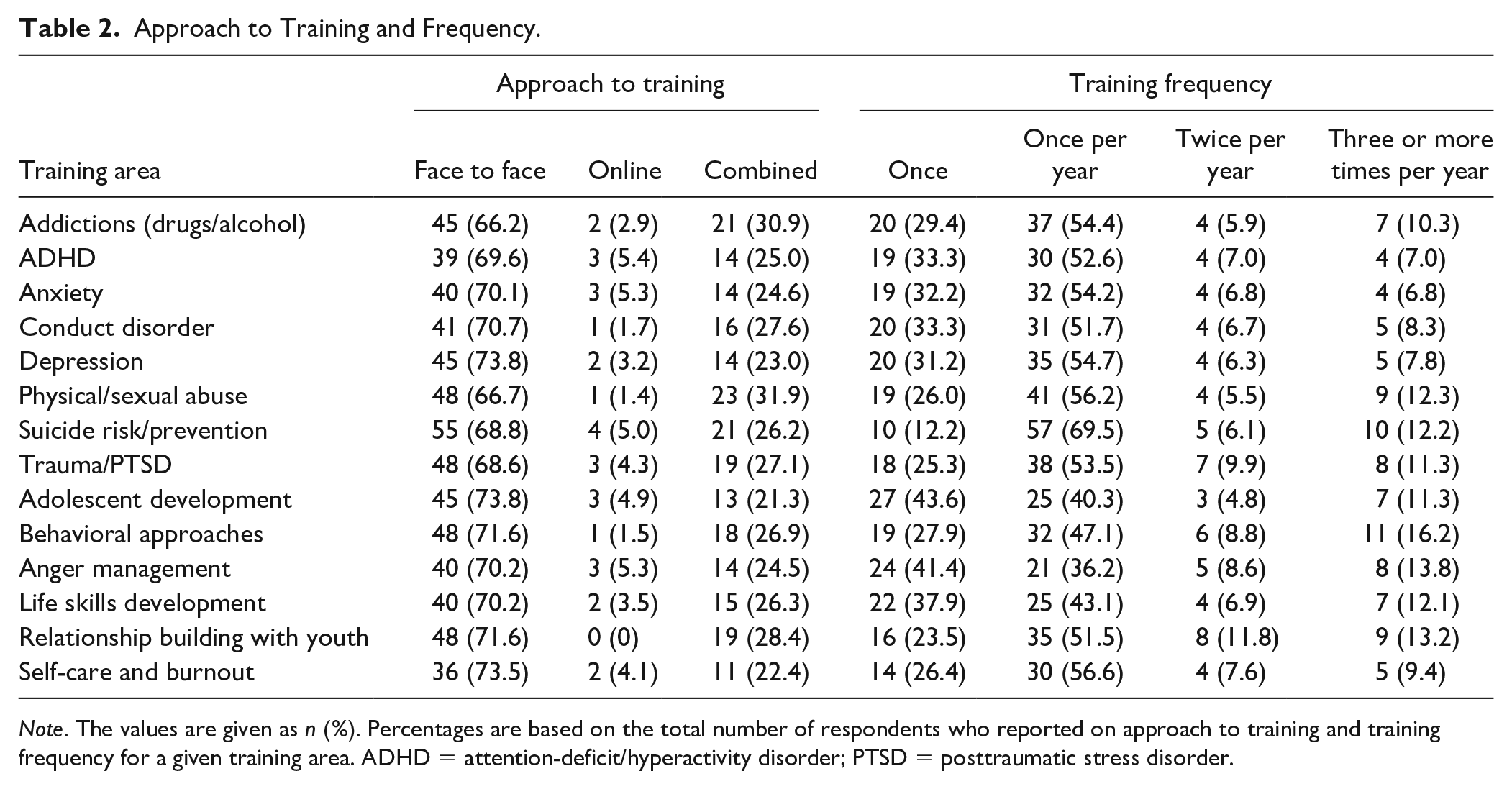
Note. The values are given as n (%). Percentages are based on the total number of respondents who reported on approach to training and training frequency for a given training area. ADHD = attention-deficit/hyperactivity disorder; PTSD = posttraumatic stress disorder.
Recommended attributes of PD
For two of the four recommended attributes of PD (i.e., trainings focus on evidence-based/best practices in working with adolescents in correctional facilities, trainings are multidisciplinary), about two-thirds of the facilities included the attributes most of the time and about one-third included them some of the time (see Table 3). About half of the facilities reported providing sufficient PD to generalize interventions to various situations most of the time, and about 40% included them some of the time. Only about one-third of the facilities reported that there is a plan to assist personnel in implementing new knowledge and skills following training most of the time, and about half included them some of the time.
Effective Attributes of Professional Development.
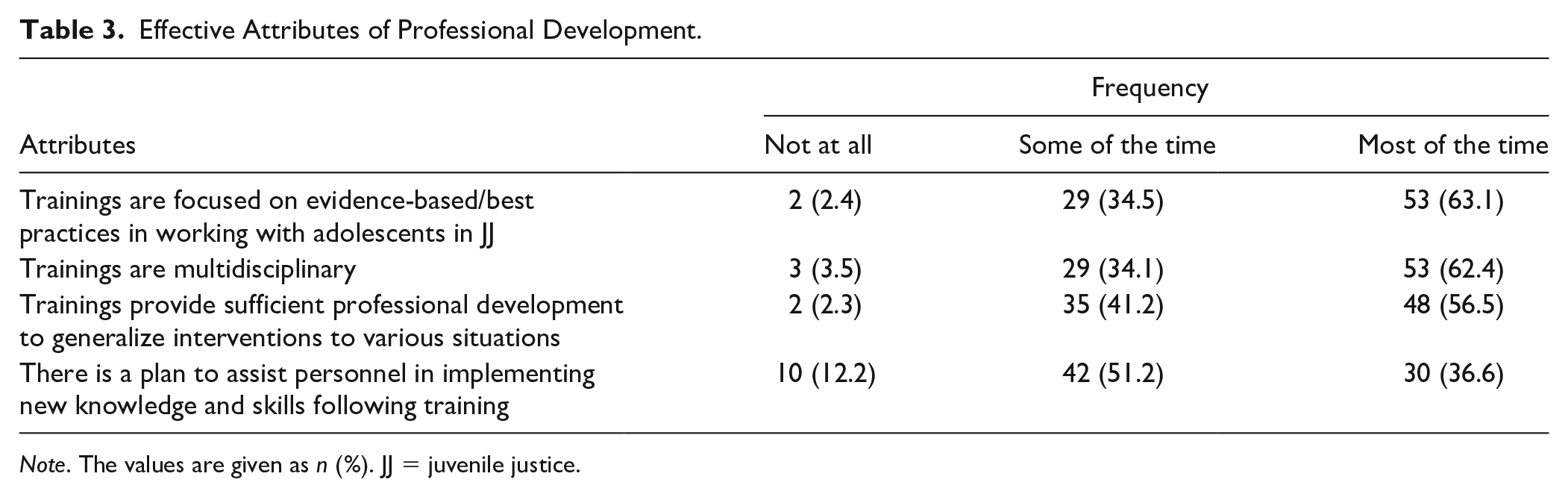
Note. The values are given as n (%). JJ = juvenile justice.
Approaches Used to Evaluate PD
Participants were asked to “check all that apply” concerning which methods that were used to evaluate PD. Training was most often assessed by written evaluation (n = 70), with relatively few facilities evaluating actual implementation (n = 11) or linking PD and program outcomes (n = 19). Eleven respondents reported that PD was not evaluated.
Adequacy of and Barriers to Providing Quality PD
Respondents noted the extent to which PD was adequate for each topic, as well as the barriers to providing quality PD for each topic (i.e., need for more training, resources, follow-up/support; see Table 4). Note that participants were able to “check all that apply” concerning the barriers for each topic and no percent was calculated. For only suicide risk/prevention did more than 70% of respondents report that PD was adequate. For three other topics (i.e., physical/sexual abuse, adolescent development, relationship building with youth), about 50% of participants reported that PD was adequate. PD related to professional self-care and prevention of burnout was the topic area most participants least rated as adequate (27.7%). ADHD (31.3%) was the other topic most rated as inadequate.
Quality of Current Mental Health Training and Barriers to Providing Quality Training.
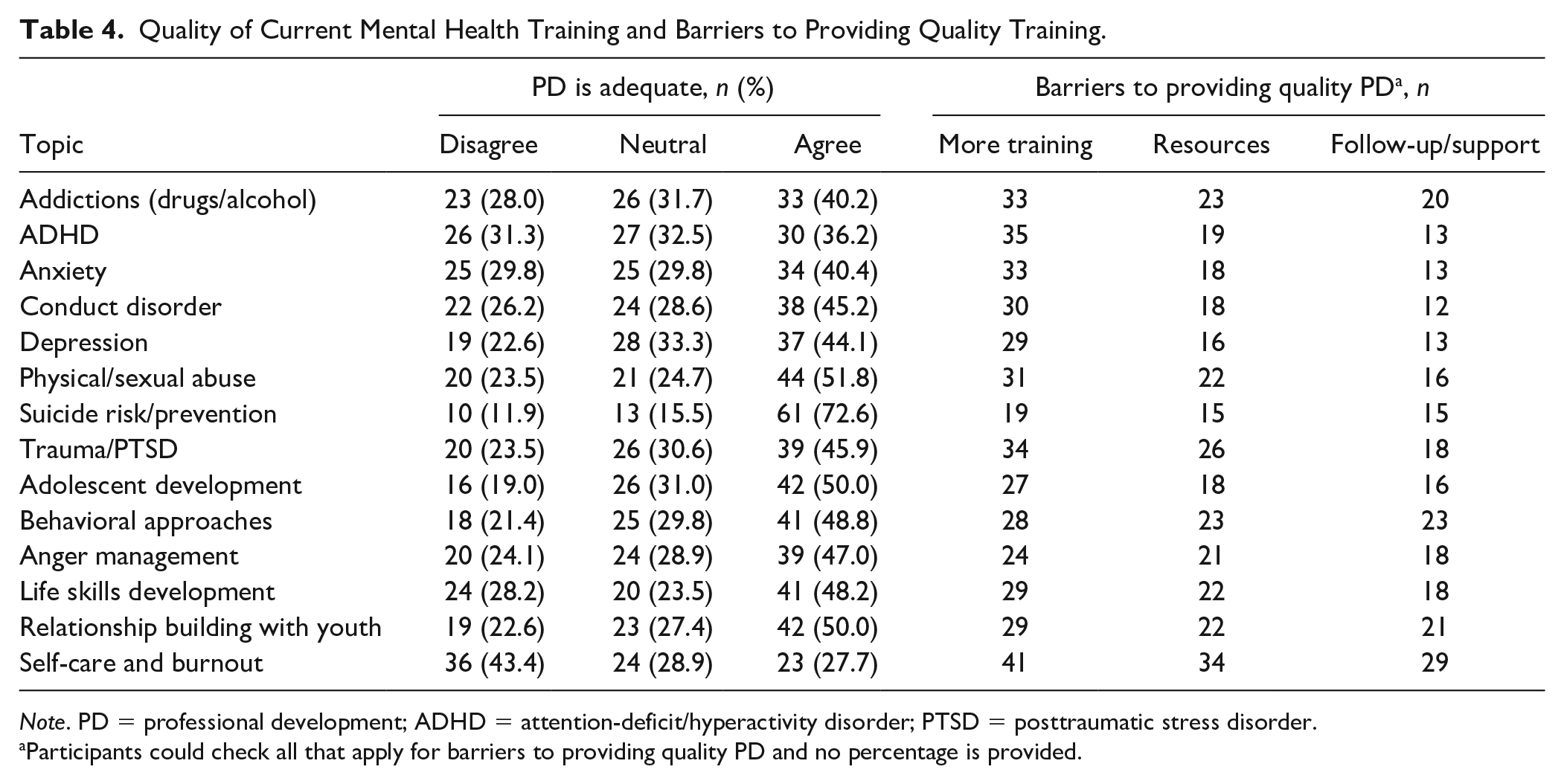
Note. PD = professional development; ADHD = attention-deficit/hyperactivity disorder; PTSD = posttraumatic stress disorder.
Participants could check all that apply for barriers to providing quality PD and no percentage is provided.
The need for more training was most frequently identified for every topic as necessary to improve PD. The need for resources was always the second most frequent needed improvement for PD, with two exceptions; follow-up/support was reported equally for suicide risk/prevention and behavioral approaches.
Discussion
This foundational research is the first national picture of mental health PD in JJ. Important implications for research and practice emanate from this study. However, additional research is needed to fully understand and ensure the successful implementation of PD in this complex setting.
Implications for Research
Topics of PD and basis for choosing topics
Interesting patterns exist concerning the frequency that PD is provided on specific topics. Although we did not query participants on the prevalence of mental health disorders in their facilities, previous research suggests that mental disorders are common in JJ facilities and can be justified as important topics for PD. It is encouraging that all respondents reported that their facility provided PD for suicide risk/prevention and 90.6% provided PD on behavioral approaches, given that these represent, respectively, a significant concern and a common approach to interventions for incarcerated youth (Lipsey et al., 2000; Teplin et al., 2015). However, 12.9% to 29.4% of facilities did not provide PD for each remaining topic. Previous research has identified high prevalence rates of mental disorders that are not the focus of PD in many facilities. For example, although researchers (Shufelt & Cocozza, 2006) noted that half of the JJ-involved youth have conduct disorder and youth are two to four times more likely to have ADHD (Fazel et al., 2008), only 75.3% and 70.6% of facilities provided any PD on these respective topics. Research is needed to identify effective methods for integrating key mental health–related topics into JJ PD plans.
Of the 85 respondents, more reported that the choice of training topics was based on state/federal requirements (n = 68) than any other possible reason. It remains unclear which topics are actually required and which clinical directors believe are required. Furthermore, if some topics are viewed as required, it is interesting that so few professionals receive training in any given category. Future research is needed to provide clarity to this issue of required PD, as well as the degree to which there is overlap between required topics, facility needs, and staff suggestions for topics. Given the limited time and resources available for mental health PD, there is a need to understand more specifically how topics are prioritized and which topics are identified in light of facility and youth characteristics. Future research is also needed to understand the potential impact of topic choices in terms of the length of time needed for developing and implementing training.
Staff participation in PD
In addition to concerns that certain PD topics are not addressed via PD in many facilities, the generally low percentages of any professional participating in PD are unsettling. Only clinical directors and counselors participated in any given topic in more than 80% of facilities and, even for these professionals, it was only for suicide risk/prevention. As reported, PD participation rates for professionals other than clinical directors and counselors were commonly in the 30% and 40% ranges. When excluding physical/sexual abuse and self-care and burnout, professionals that typically have the most direct contact hours with youth (i.e., COs, teachers, teacher assistants) almost never exceeded 50% PD participation. Moreover, alarmingly low rates of participation in PD existed for professionals that focused on helping youth with anger management and life skills development, which are both important considerations for youth when attempting to reintegrate into society upon release. For nurses, social workers, administrators, COs, teachers, and teacher assistants, participation rates in these topics hovered around 30%. Specifically, youth that are incarcerated during their formative teenage years do not have adequate opportunities to develop the general life skills that are necessary for employment and independence (VanderPyl, 2015). Given the high percentage of youth that have experienced trauma and the links between trauma and anger and aggression, the lack of training related to youth aggression is also concerning (VanderPyl, 2015).
In light of the trends concerning which professionals are commonly excluded from PD, there is a need to conduct research that will provide clarity around who makes decisions about participation in PD, how decisions are made, the rationale for decision, and the potential influence of logistical issues. Additional lines of inquiry may also include (a) the extent to which the previous training of professionals in certain positions is or could be considered when deciding on participation; (b) if and how the professional duties for a given position are taken into account when deciding who receives PD on a given topic; and (c) the potential for coordinating interdisciplinary PD participation in a way that professionals who work on the same shifts and/or with the same youth can participate together in PD.
Characteristics of PD provided
In terms of training format and frequency of PD, facilities overwhelmingly relied on a face-to-face approach, with only about 30% of facilities using blended learning for any given topic. About 85% of facilities provide PD on any given topic once or once per year, with most providing a given topic once per year. Future research should investigate the extent to which face-to-face, blended, and completely online learning result in learning and actual implementation of skills and information by JJ professionals. Future research should also examine the length of trainings, depth of content, and participant activities related to each PD topic.
This study provides a first look at which recommended attributes of PD are implemented when providing mental health PD in JJ. Only about two-thirds of facilities used any of the approaches most of the time. Future research is needed to identify ways in which recommended attributes of PD (e.g., trainings are focused on evidence-based/best practices in working with adolescents in JJ, are multidisciplinary, provide sufficient PD to generalize interventions to various situations, and there is a plan to assist personnel in implementing new knowledge and skills following training) can be more fully integrated. Although this study provides information on the use of these methods, information is still needed to establish who is providing the PD and in what ways they are using these methods. In addition, methods need to be identified for overcoming barriers to providing PD that fully integrates recommended attributes of PD.
Although most facilities (n = 70) rely on written evaluations of PD, follow-up research is needed to better understand the content of the evaluation. Guskey (2002) identified a need to evaluate participants’ reactions, learning, and use of new knowledge and skills. Currently, the extent to which written evaluations address these issues remains unknown. Also, a small number of facilities evaluate actual implementation. Future research should explore the implementation of interventions based on PD topics, as well as the short-term (e.g., youth behavior change) and long-term (e.g., recidivism, engagement in society post-exit) effects on youth.
There are serious concerns with the quality of PD related to mental health in JJ settings. With the exception of two topics (e.g., physical/sexual abuse, suicide risk/prevention), only about half of respondents rated the PD on any given topic as adequate. This study sets the stage for a much-needed evaluation of JJ PD. Information is needed on the reasons that the PD for each topic is rated as inadequate. Future research should also explore potential links between the approach to PD, professional dissatisfaction with the PD, and the degree to which information and skills are used and integrated into the JJ setting.
Respondents most frequently noted more training as the greatest need to improve training. Still, less than half of the respondents noted this issue for any topic. A need exists for research that looks into other potential issues that may also impact the adequacy of PD and effective approaches to addressing these issues. Although a need for resources was also a prevalent need to improve PD, future research should provide additional information concerning which materials are needed and the intended purpose of these materials.
Limitations
Study findings should be considered in the context of some important limitations. First, the response rate of 45% is slightly lower than the accepted and common 50% rate (Baruch & Holtom, 2008); however, it should be noted that the sample exceeds the number needed to achieve a 95% confidence level and 10% margin of error. Also, given the length of the survey and focus on a number of PD attributes and topics, a decision was made to limit general background information to the facilities and youth at the facilities. As such, the lack of in-depth respondent demographics is a limitation. In terms of the focus of the survey, there are two limitations: (a) A specific time frame for participation in PD was not identified and (b) PD provided outside of the facility context was not specifically addressed. Although mitigated by assurances of confidentiality of responses, another limitation inherent in survey research is that respondents could have misrepresented the actual situation with regard to PD in their facility.
Finally, to maintain an appropriate survey length, it was necessary to maintain a relatively broad focus on the current state of PD in JJ. For example, this manifested in the use of a three-point scale for questions in the survey section focused on recommended attributes of PD, as well as the question asking about the adequacy of PD for each topic. It is acknowledged that the length of the survey necessitated these rather broad choices. Moreover, the survey did not address other critical issues, including the actual content, depth, length, or specific instructional strategies used for each topic or the variations that exist across topics. Nevertheless, this national study provides the most comprehensive picture of mental health–related PD in JJ in the United States currently available.
Implications for Practice
Several important implications for practice are evident regarding the overall frequency of PD on mental health topics, which professionals participate in PD, the quality of PD, and the inclusion of recommended PD attributes. Perhaps, the most urgent implication is the need to ensure that all JJ staff have the necessary mental health–related PD to promote the safety, well-being, rehabilitation, and education of youth. The links between youth mental health and recidivism are clear (Schubert & Mulvey, 2014; Wibbelink et al., 2017). Given the importance of providing incarcerated youth with ongoing mental health support in their day-to-day interactions (VanderPyl, 2015), it is disturbing that, for any PD topic, participation rates for case managers, nurses, social workers, administrators, COs, teachers, and teaching assistants are commonly about 50% or below. Eventual and successful youth transition out of the facility requires coordination and collaboration of professionals from multiple areas and systems within a JJ facility and a common knowledge base regarding youth mental health needs and approaches to intervening (Griller-Clark et al., 2016). It is recommended that JJ facilities prioritize mental health–related PD topics based on the common characteristics of incarcerated youth and provide interdisciplinary training experiences that include all of these crucial staff (Gagnon et al., 2012; Krisberg, 2014).
Respondents identified major concerns with the quality of PD, and particularly, the need for more training and resources. Although facilities are limited by time and money, prioritizing topics and ensuring complete coverage of prioritized topics may be one approach to address this issue. It is important for facilities to move away from the notion that PD can be provided as a “one-shot” workshop (Gagnon et al., 2013). Also, the use of blended and solely online PD is relatively rare. Online or blended PD may provide needed flexibility to maximize PD and the time JJ professionals have for face-to-face PD (Nelson et al., 2010). Granted, the quality of such PD would need to be evaluated, but these approaches have the potential to assist in several ways, including (a) providing for greater flexibility with timing; (b) reducing costs; (c) affording time for participants to reflect on information and engage in online discussions; and (d) allowing for professionals in different fields within a facility, as well as professionals across multiple facilities, to engage in discourse on ways to apply knowledge and skills (Dede et al., 2009).
The scarcity with which recommended attributes of PD are used in JJ is concerning. Perhaps, there is a link between the frequency of training on a given topic and the potential to include a number of approaches. For example, use of a plan to assist personnel in implementing new knowledge and skills following training was quite rare and this may be a function of the amount of time that it would take participants to develop and monitor such a plan. Nevertheless, it is recommended that facilities rely on evidence-based treatment models and interventions, and do so in multiple multidisciplinary sessions that promote and hold staff accountable for follow-up action (Swank & Gagnon, 2016). It is also crucial that facilities accurately and completely evaluate PD. Evaluation methods should measure participants’ reactions, learning, and use of new knowledge and skills (Guskey, 2002). Facilities should also consider conducting further analysis on the extent to which there is organizational support for change and professional application of new knowledge and skills, as well as the effects of changes on youth short-term outcomes and long-term success with reintegration.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by an internal grant from the College of Education, University of Florida.