
Abstract
Objective
Patients with palliative head and neck cancer experience many symptoms in a short period of time. Longitudinal data on patient-reported outcomes in this phase are lacking. The aim of this study is to use structurally obtained patient-reported outcome data combined with clinical patient data and obtain insight in patient-reported outcomes, survival, circumstances of death, and interventions and treatment during the palliative phase in order to improve the quality of end-of-life care and patient-centered counseling.
Study Design
Longitudinal observational cohort study.
Setting
Tertiary cancer center.
Method
Quality of life was prospectively collected using the European Organization for Research and Treatment of Cancer QLQ-C15-PAL. Tumor- and patient-specific data were retrospectively collected. Descriptive statistics, linear mixed models, and regression analyses were performed.
Results
A significant deterioration was found in global health status, physical functioning, fatigue, dyspnea, appetite loss, and constipation over time. However, emotional functioning improved. Median survival was 5.1 months, and only a low percentage of in-hospital death was observed (7.8%). Higher global health status at intake was associated with prolonged survival.
Conclusion
Structural measurement of patient-reported outcome together with clinical outcomes provides unique insight, which enables improvement of patient-centered counseling and care.
Keywords
Palliative care in general aims to improve quality of life (QoL) for patients and their families by providing relief from symptoms and stress of the disease. 1 Approximately 25% to 30% of the patients with head and neck cancer (HNC) will at a certain moment reach the palliative phase in which no curative treatment options are available. This phase is rather short, with a median survival of 5 months.2-4 During the palliative phase, patients often develop specific problems with swallowing, speech and airway, (fatal) bleeding, and dramatic appearance changes. The most frequently reported somatic symptoms during the palliative phase are pain, fatigue, and weight loss.5,6 These physical problems, combined with the knowledge of limited survival, can have a significant psychosocial impact on patients and their loved ones.2,7-10 Therefore, patients should be offered individualized palliative care focusing on early identification and treatment of symptoms.11-13 A multidisciplinary patient-centered approach has the potential to alleviate the burden of disease, preserve QoL as long as possible for both patients and their families, assist with decision-making, and reduce hospital admissions.14-22
Since 2005, an Expert Center of Palliative Care for patients with HNC is operational in the Erasmus Medical Center with dedicated head and neck surgeons and specialized oncology nurses as case managers. When patients become palliative due to exhaustion of curative treatment options or by refraining from curative treatment, we provide structural multidisciplinary patient care focused on symptom control and psychosocial support for patient and family. This setup led to improved psychosocial support, better doctor-patient relation, and fewer hospital admissions.23,24 Since 2016, this working method has been complemented with the structural implementation of electronic Patient-Reported Outcome Measurement data (ePRO), which we called the “Healthcare Monitor.” 25 This monitor is used during every patient encounter and works as a “guide” during individual patient contacts, and it helps to early detect issues in the palliative phase. This can lead to more individualized symptom management and end-of-life counseling and care. 25
Literature and learnings on palliative HNC care stay scarce due to a relatively short palliative phase and often vulnerable patients not being able to participate in research. Our working method guides optimal care and at the same time provides us with useful insights on the development of patients’ functioning and burden during the entire palliative phase. The aim of this study is to evaluate structurally obtained outcome data from our palliative care program in order to obtain insight in (1) longitudinal patient-reported outcomes, (2) survival and associated factors, (3) circumstances of death, and (4) interventions and treatment during the palliative phase.
Methods
Institutional Routine and ePROs
Following the palliative diagnosis, the patient is referred to a specialized oncology nurse. They are the patients’ case manager and keep contact with the patients’ general practitioner (GP), who has a central role during the palliative phase. However, due to the rarity of HNC, our Expert Center of Palliative Care provides accessible information for all GPs. 3 The patient can contact the team of specialized oncology nurses whenever needed via remote care or during a physical appointment. On the other hand, the nurses proactively contact the patient every 6 to 8 weeks. The patient fills in the ePRO (EORTC QLQ-C15-PAL) prior to these encounters. When patients are vulnerable or lack digital skills, they will be supported by the specialized oncology nurse. Results act as a guideline for individual patient contacts.
Research Ethics and Patient Consent
This study was approved by the institutional review board and ethics committee from the Erasmus University (MEC-2020-0314). All participating patients provided electronic written informed consent.
Case Selection and Data Collection
All palliative patients diagnosed between January 1, 2016, and January 5, 2020, with a head and neck carcinoma were retrospectively included in this study. This included squamous cell carcinoma, melanoma, sarcoma, and salivary gland tumors. Head and neck metastases from other tumors were not included. Patients could be declared palliative due to exhaustion of curative treatment options or by refraining from curative treatment. Patients were excluded when ePROs were incomplete, lost to follow-up, or if the palliative status was revoked when there was no evidence of disease after palliative (experimental) treatment.
Instruments Used
Patient-reported QoL was assessed from intake up to 6 months with the European Organization for Research and Treatment of Cancer (EORTC) QLQ-C15-PAL. 26 This questionnaire is a shortened version of the EORTC QLQ-C3030 and recommended for use in patients with advanced, incurable, and symptomatic cancer with a median life expectancy of a few months. It consists of 15 questions, assessing 10 domains. A score for physical functioning is a combination of 3 separate items. Emotional functioning, fatigue, and pain are 2-item scales. Dyspnea, insomnia, appetite loss, constipation, nausea/vomiting, and global health status are single-item scales. All questions are scored on a 4-point scale, ranging from 1 (not at all) to 4 (very much). A higher score indicates a better QoL for the domains of emotional functioning, physical functioning, and global health status. In contrast, for the remaining domains, lower scores indicate better QoL.
At baseline, the following clinical variables were scored: patient physical capability of functioning in daily life by means of the WHO Performance Status, 27 Adult Comorbidity Evaluation–27 (ACE-27), 28 age, sex, weight loss (yes/no), marital status, tumor location and TNM stage, tumor chronology (primary or recurrent disease), and social network. Clinical outcome information assessed during follow-up period includes place and cause of death, gastric tube placement within the first 2 months, involvement of the dietitian and pain team, and starting and ending palliative treatment.
Statistical Analysis
Statistical analyses were performed using R. 29 Descriptive statistics were used to calculate the frequencies and proportions for baseline characteristics. The evolution over time and effect of clinical variables was assessed for each domain of the EORTC-QLQ-C15-PAL with linear mixed-model analysis. Mixed-model analyses are most appropriate for these multilevel data as they account for the correlations between repeated measurements within each individual and take missing data into account. 31 For every model, comprising 1 domain, a fitting procedure was performed, and an optimal covariance matrix was chosen based on the –2 restricted log likelihood. Within every model, the effect and estimated mean of the random intercepts of the following variables were investigated: age, sex, performance status, ACE-27, treatment, tumor chronology, metastatic disease, weight loss, marital status, and tumor stage. Predicted means with 95% confidence intervals were derived from the best-fitted models. Changes over time were analyzed for significance, and clinical relevance was considered using minimally important differences (MCIDs) proposed by the EORTC.32,33 Disease-specific survival (DSS) was defined as the time from palliative diagnosis until death or last day of follow-up. The Cox proportional hazard regression model was used to calculate the multivariable hazard ratios for clinical variables and 1 patient-reported outcome measure (global health status). Two-tailed significance levels of ≤5% were used for all analyses. Correction for multiple testing was performed.
Results
Between January 1, 2016, and January 5, 2020, 337 patients with HNC in the palliative phase were retrospectively identified. Four patients were excluded due to revocation of the palliative status, 1 patient was excluded due to incomplete ePROs, and 1 patient was excluded due to loss to follow-up. In total, 331 patients were included in this study for further analysis. The number of patients lost to attrition were 86 (26.0%) at 2 months, 151 (54.4%) at 4 months, and 194 (58.6%) at 6 months.
Baseline Characteristics
The mean age at the time of palliative diagnosis was 70 years, with 65.9% of the patients being male. In total, 145 patients (43.8%) lived alone, and 60 patients (18.1%) had an inadequate social network. Comorbidity was present in almost all patients; only 7.3% of the patients had no comorbidities. Most patients (88.3%) had squamous cell carcinoma. Distant metastasis was present in 40.5% of all patients. At the time of inclusion, 74 patients (22.4%) were still alive. For all baseline characteristics, see Table 1 .
Patient Characteristics (N = 331). a
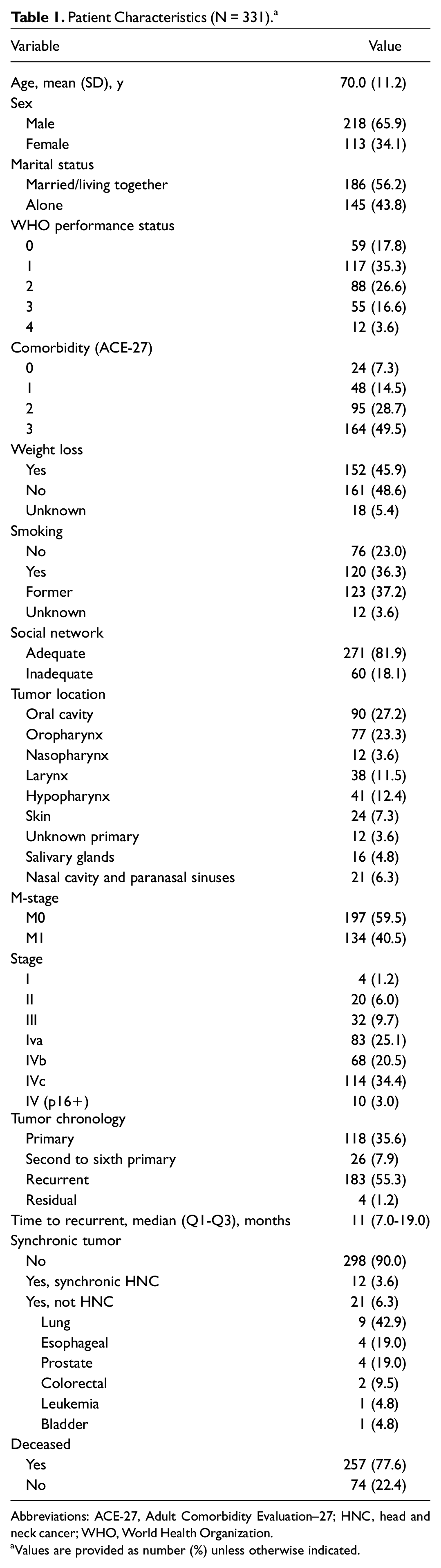
Abbreviations: ACE-27, Adult Comorbidity Evaluation–27; HNC, head and neck cancer; WHO, World Health Organization.
Values are provided as number (%) unless otherwise indicated.
Palliative Characteristics
Palliative characteristics can be found in Table 2 . In 269 patients (81.3%), the palliative phase started because no curative options were available. The other 62 patients (18.7%) refrained from curative treatment or even necessary diagnostic tests. In the group that refrained from curative treatment, a significant higher proportion were females (47.6% vs 31.2%, P = .014), had synchronous tumors (20.6% vs 7.4%, P = .002), or eventually chose euthanasia (26.5% vs 9.6%, P = .001).
Palliative Characteristics (N = 331).
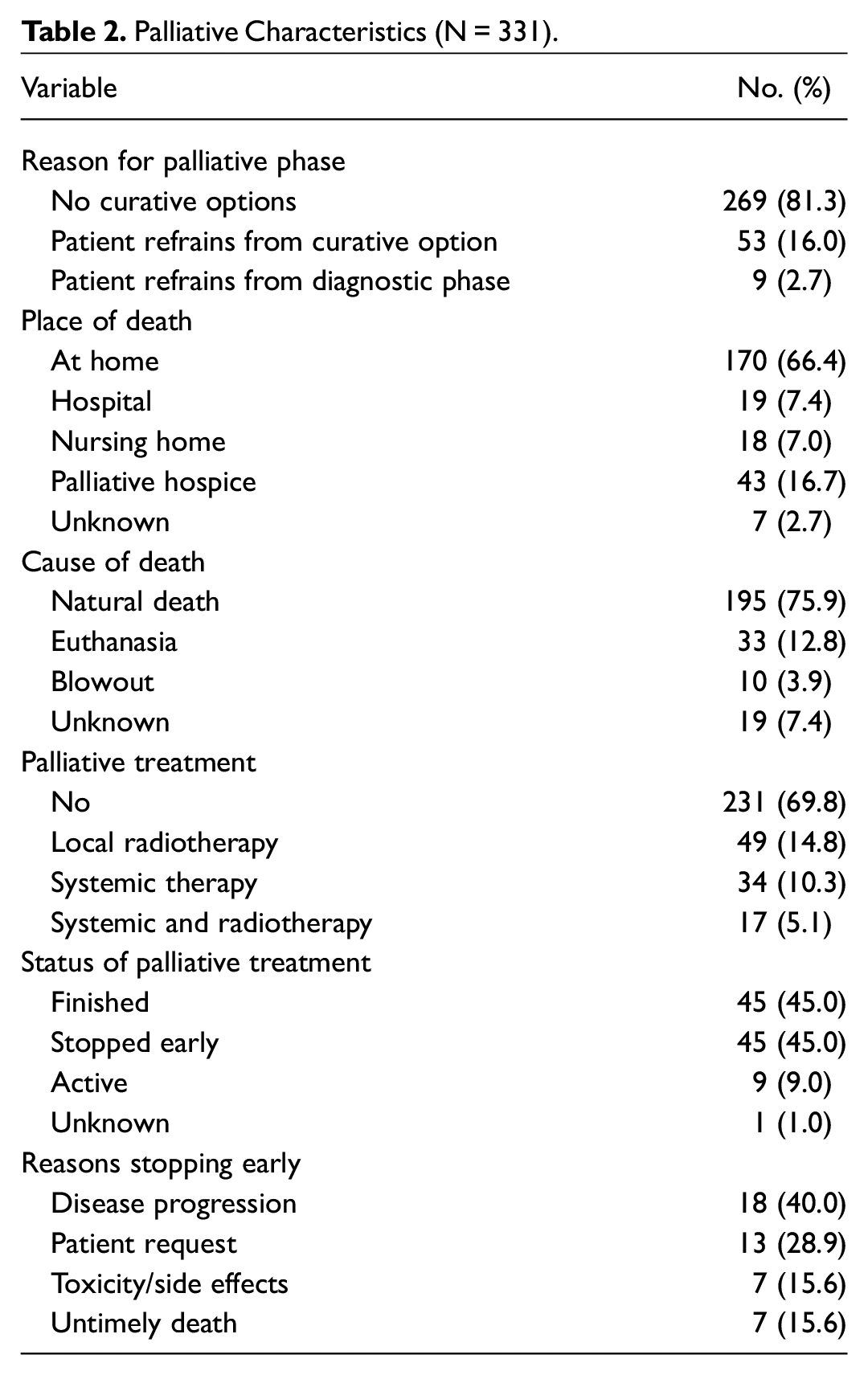
In-hospital death occurred in only 19 patients (7.8%). Reasons for hospital admissions in this final phase of life were mainly acute deterioration (eg, imminent bleeding or acute dyspnea). Living together with a partner was significantly associated with dying at home. In contrast, patients living alone or without adequate social network were associated with dying in a nursing home or palliative hospice.
Natural death occurred in 195 patients (75.9%), 10 patients died of a carotic blowout (3.9%), and 33 chose for euthanasia (12.8%). Euthanasia was performed mainly at home (81.8%) and in patients who did not receive any palliative treatment (78.8%). Patients who chose for euthanasia were predominantly diagnosed with stage IV disease (81.6%). Carotic blowout occurred most in oropharyngeal (40.0%), laryngeal (20.0%), and oral cavity (20.0%) tumors. Of the patients dying from a carotic blowout, 9 patients (90.0%) had recurrent disease.
Patient-Reported Outcome Measures
Longitudinal patient-reported QoL up to 6 months is presented in Table 3 . In total, 704 measurements were completed. Significant deterioration during the 6-month follow-up was seen in the domains of global health status (–6.6), physical functioning (–8.4), fatigue (+10.4), dyspnea (+5.6), appetite loss (+9.1), and constipation (+4.9). A significant improvement was seen for the domain of emotional functioning (+6.0). Longitudinal mean differences for patients with high performance status compared to low performance status were observed for global health status (–11.8), physical functioning (–29.9), fatigue (17.3), pain (15.4), dyspnea (11.4), and appetite loss (11.3). Patients with higher comorbidity scores were associated with worse scores for physical functioning (ACE 2: –16.4; ACE 3: –12.0), as were patients with recurrent disease (–9.6) and absence of treatment (–10.3). Mean estimates for other significant clinical and demographic factors can be found in Table 4 .
Longitudinal Mean Estimates for Patient-Reported Quality of Life From Intake to 6 Months.
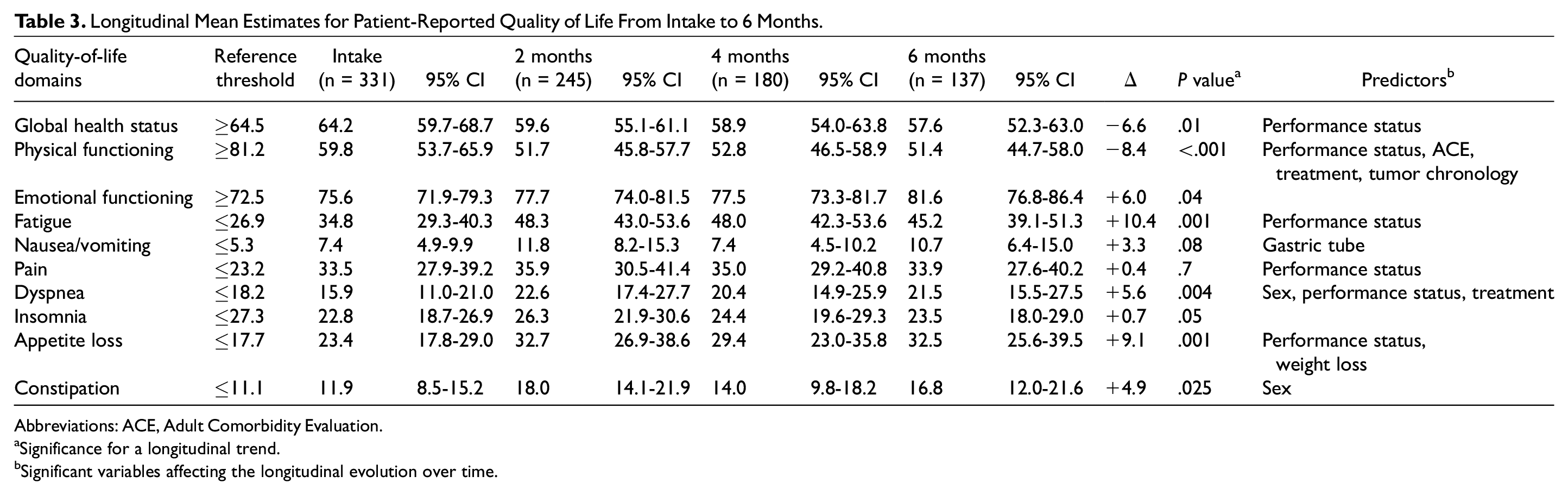
Abbreviations: ACE, Adult Comorbidity Evaluation.
Significance for a longitudinal trend.
Significant variables affecting the longitudinal evolution over time.
Estimates of significant Random Intercepts.
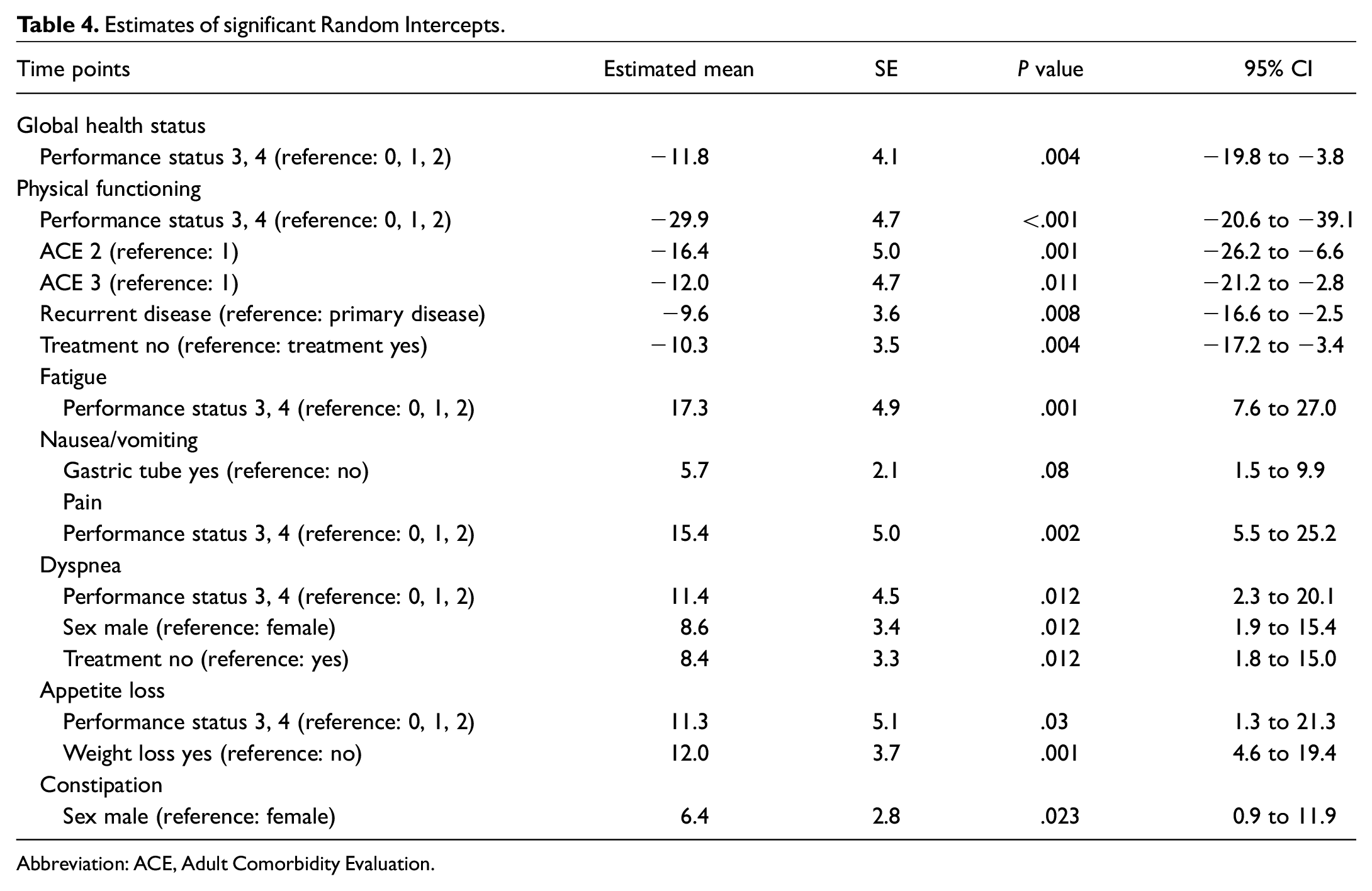
Abbreviation: ACE, Adult Comorbidity Evaluation.
Survival Analysis
The median DSS of all patients was 5.1 months (range, 0.1-40.5 months). Higher age at entry in the palliative phase, higher performance status, severe comorbidity, higher tumor stage, and receiving no palliative treatment were significantly associated with a lower DSS. Moreover, a higher reported global health status at intake was associated with prolonged survival (hazard ratio [HR], 0.988; P = .000). The multivariable Cox regression analysis can be found in Table 5 .
Multivariate Cox Regression Analysis: Impact on DSS.
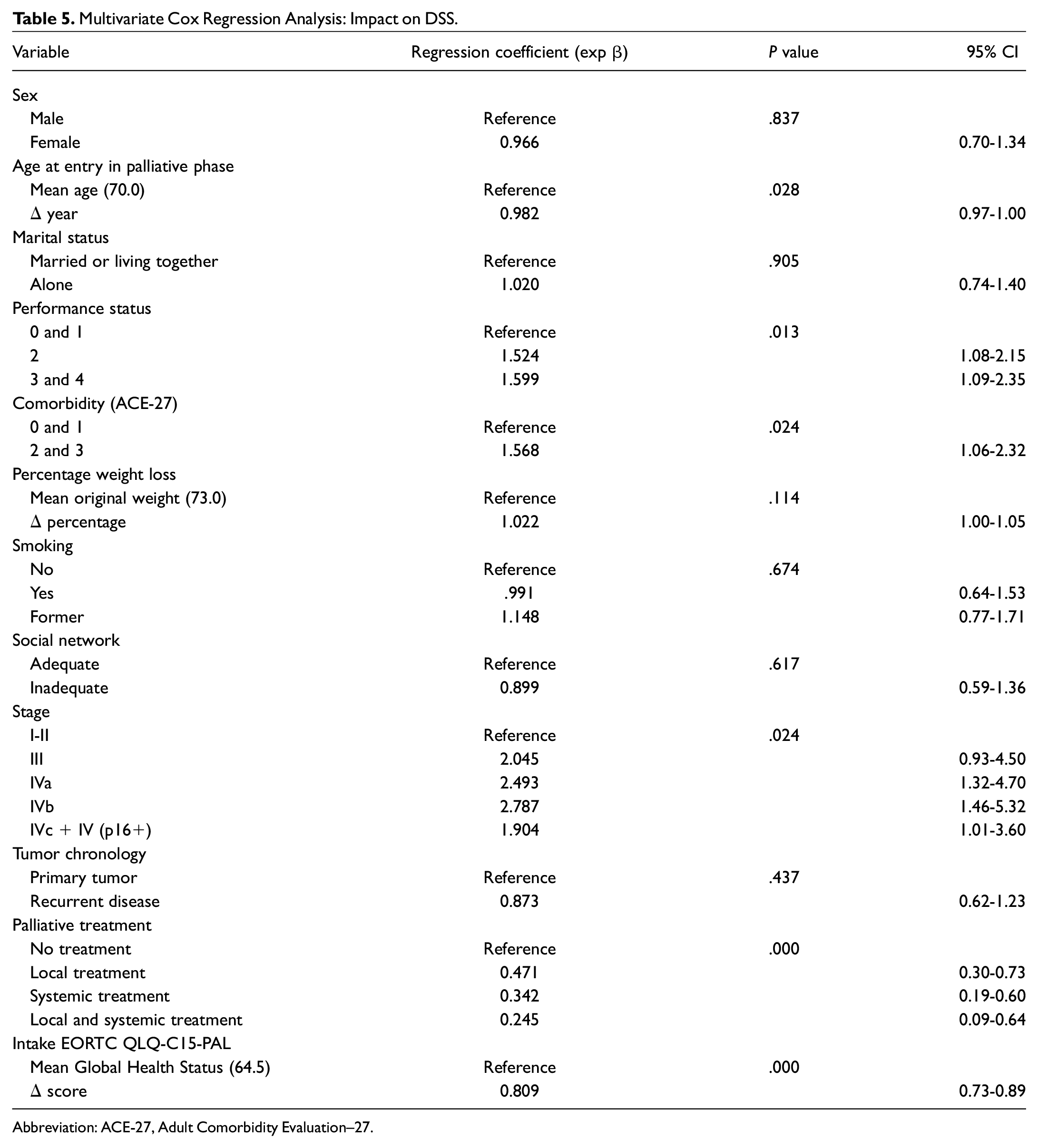
Abbreviation: ACE-27, Adult Comorbidity Evaluation–27.
Palliative Interventions and Treatment
Palliative treatment was given to 100 patients (31.2%). At the time of inclusion, 9 patients (9.0%) were still in the palliative treatment process, 45 finished (45.0%), and 45 (45.0%) had stopped prematurely. Reasons for stopping treatment were mainly disease progression (40.0%) and patient request (28.9%). The pain team was consulted in 41 patients (12.4%). The dietitian was consulted in 196 patients (59.2%) and most often in the care for oropharyngeal and laryngeal patients. In 68 patients (20.5%), a gastric tube was in situ, consisting of 45 (66.2%) nasal tubes, 21 (30.9%) gastrostomies, and 2 (2.9%) jejunostomies.
Discussion
The aim of this study is to evaluate structurally obtained outcome data from our palliative care program in order to obtain insight in (1) longitudinal patient-reported outcomes, (2) survival and associated factors, (3) circumstances of death, and (4) interventions and treatment during the palliative phase.
With this study, we fill in the paucity of longitudinal studies in patients with palliative HNC.
Our study reports a median survival of 5.1 months in which patients with palliative HNC experience significant deterioration in global health status and physical functioning, fatigue, dyspnea, appetite loss, and constipation. It is important to see these longitudinal patient-reported outcomes within the light of clinical significance and relevance.32,33 Changes are clinically small (5-10) for global health status, physical functioning, dyspnea, and appetite loss and clinically moderate (10-20) for fatigue. 33 According to the EORTC Head and Neck and Quality of Life Groups, all longitudinal changes in these domains, except for constipation, exceed the threshold for a minimally important difference. 32 The fact that the increase in scores for fatigue is the only clinical relevant change does not surprise as fatigue is seen as the most common symptom experienced in overall palliative care. 6
There is little research available, longitudinal in particular, on patient-reported outcome measures in palliative HNC care. Compared to previous but cross-sectional research using the EORTC-QLQ-C15-PAL in HNC, our results show similar median scores at baseline for physical functioning, fatigue, pain, nausea and vomiting, dyspnea, and constipation.5,34 This is also in accordance to a recent review in which the domains of physical functioning, fatigue, and pain were mentioned as most prevalent. 6
Despite the overall deterioration over time for most domains, emotional functioning appeared to improve during follow-up. This is an interesting outcome considering previously reported major depressive disorders and high incidence of suicide in HNC populations.35-38 To our knowledge, the longitudinal evolution of emotional functioning has not been investigated before in HNC. A study from van Roij et al 39 found that quality of care elements (eg, more satisfaction with care provided, continuity of care and information) were associated with higher emotional functioning. We would argue that our expert clinic approach with psychosocial support during individual follow-up counseling, and close contact with the general practitioner can be an explanation for this improvement.
Place of death is a critical outcome in palliative care.40,41 In our study, two-thirds died at home, and only a minority of 20 patients (7.8%) died in the hospital. These results reveal an improvement within our department since 2008, when 38% died in the hospital and 18% in 2013. 24 This is noteworthy as previous international research in palliative HNC stated that 47% to 70% of the patients died in the hospital.9,42 However, we are aware that this comparison should be made cautiously as the place of death can be culturally determined. In our study, euthanasia was performed 33 times (12.8%). In contrast to other countries, this is a legal option for patients with unbearable suffering with no prospect of improvement. It is no absolute right, and strict guidelines should be followed. 43
Strengthen Patient-Centered Counseling and Care
From our results, implications for clinical practice can be derived to strengthen patient-centered care. Overall, patients and health care professionals should be aware of the limited survival, which leaves a short period for optimizing palliative care. It is important to inform patients on what to expect.
Patients with high performance status are prone to lower outcomes on the domains of patient-reported physical functioning, fatigue, pain, and appetite loss. Patients who did not receive palliative treatment had lower overall survival and scored significantly worse on the domains of physical functioning and dyspnea. These insights can be used by health care professionals for screening and providing adequate counseling and support. Furthermore, monitoring patients without an adequate social network more closely is also advised. Our results concerning place of death show that it is feasible to achieve a very low rate of in-hospital death. We would argue that advanced care planning and discussing the circumstances of death should be done early in the palliative phase. In addition, we would advise that a dietitian and pain team are part of the multidisciplinary palliative team for all patients.
Strengths and Limitations
A significant strength of our research is the availability of rich data concerning clinical and patient-reported outcomes. A strength is also the use of linear mixed models, which enables the use of all available information without excluding patients due to missing data. Another strength of our study is the comparison we were able to make with previous research from our department.5,23,24
A limitation of our study is the heterogeneity of the studied population. Outcomes can differ between tumor locations and morphologic types. Also, we are aware of the exploratory analysis and the need for caution in interpreting and drawing conclusions. Another limitation can be found in the absence of an item on patient-reported dysphagia, trismus, xerostomia, and loss of speech in the EORTC QLQ-C15-PAL.26,44 These domains should be incorporated into future measures of patient-reported outcomes. Other important factors that have not been included in our study are loss of sensation, body image, sense of dignity, and fears of mortality. In addition, we did not have the data available on race, ethnicity, socioeconomic status, and education levels. It should also be noted that the generalizability is affected by a different health care system compared to the Netherlands.
Future Perspectives
As improvement in health care is a continuous process of implementation and evaluation, our team developed an easy-to-use professional improvement dashboard. This dashboard provides health care professionals real-time feedback on clinical and patient-reported outcomes on an aggregated level and is used periodically.
Following previous evaluation research with our Expert Center, 24 we will evaluate our current value-based approach from the patients’ point of view. This research will comprise patients’ experiences and wishes concerning remote palliative care with our ePRO structure, the Healthcare Monitor. A next step would be to include familial or caregiver insights into the end-of-life experience and quality of death in our approach.45-47 Currently, we are working on our ideas of an app for remote care that enables continuous symptom control and easy facilitation of contact with experts from our hospital. Our hypothesis is that this will lead to less hospital visits, enhance patients’ empowerment, and improve end-of-life care.
Our team is currently developing a prognostic model for survival for patients in the palliative phase. The use of this model will provide patients and their caregivers with adequate information on expected survival, which consequently enables patient-centered end-of-life decision-making.
Corresponding to previous research,48-51 our results showed that global health status at baseline is a significant predictor for survival. Therefore, we believe that our data provide opportunities for further prognostic research, modeling longitudinal QoL, and incorporating QoL in prediction models for survival.
Conclusion
This study provides a unique insight into the palliative phase of a large cohort of patients with HNC. A short median survival was observed with a low rate of in-hospital death. Patient-reported global health status, physical functioning, fatigue, dyspnea, appetite loss, and constipation deteriorated over time, and higher global health status at intake was associated with improved survival. Emotional functioning improved over time. By analyzing structural obtained outcome information, we are able to learn from and improve our patient-centered end-of-life counseling and care.
Footnotes
Acknowledgements
We thank Aaron Boon for his linguistic corrections.
Author Contributions
Disclosures
Data Management and Sharing
Data can be obtained on request. Requests should be directed toward the data management team of the Head and Neck Department of the Erasmus MC Cancer Institute (