
Abstract
Objective
To identify patient factors in older patients associated with making posttreatment visits in the first year after major head and neck oncologic surgery.
Study Design
Retrospective cohort study.
Setting
Academic institution.
Methods
Patients aged ≥60 years who underwent a neck dissection with or without a free flap reconstruction were retrospectively analyzed. Data collected included patient demographics, comorbidities, social variables, perioperative course, and clinical visits.
Results
Within a 1-year postoperative period, the 181 patients in our cohort had a mean ± SD 6.37 ± 3.6 postoperative clinic visits; 70% attended at least 4 visits. Multivariable regression analysis showed a significant association with distance closer to the hospital (P = .013): for every 10-mile increase in distance, the number of visits decreased by 0.15 (SE = 0.06). Additionally, receiving adjuvant radiation therapy (P = .0096) demonstrated significant associations: when compared with no adjuvant therapy, radiation therapy had on average 1.5 (SE = 0.56) more visits, and chemoradiation had 0.04 (SE = 0.73) more visits.
Conclusion
Older patients who undergo major head and neck oncology surgery are more likely to attend posttreatment visits in the 1 year following surgery if they are discharged home rather than to a skilled nursing facility, live closer to the hospital, and undergo adjuvant radiation therapy.
In 2021, it was estimated that >66,000 people in the United States will have developed head and neck cancer (HNC), with the percentage of older people who have or will be diagnosed with HNC rising due to the increasing average life span.1,2 Natural physiologic changes occur during the aging process, such as decreased muscle mass, diminished pulmonary function, and increased susceptibility to infection. Furthermore, the older patient population is at increased risk for complications, postoperative adverse events, and prolonged recovery.3,4
Specific characteristics found to be associated with worse outcomes in patients undergoing major HNC surgery include older age, moderate or severe comorbidities, body mass index <25, high frailty and worse geriatric assessment, duration of surgery, and additional operations.5,6 Medical complications (eg, thromboembolic, pulmonary, and cardiac) are seen at increasing rates in older patients as well.4,7 It becomes increasingly important to continue follow-up care to better survivorship especially when providers face a large percentage of HNC survivors discontinuing care with the treating institution. 8
Loss of follow-up or late diagnosis in HNC can lead to increased rates of metastatic disease, secondary malignancy, symptoms of mass effect in the head and neck area, localized and generalized symptoms of malignancy, and disease-specific death. 9 Furthermore, timely treatment initiation of HNC in older patients is essential in preventing hospitalization in the first year after treatment. In addition to health complications, older patients are faced with burdensome costs of treatment and postoperative care, with the burden of illness for HNC reported as $79,165 over 5 years per patient. 10 The projected cost of care for HNC in 2020 was estimated at $5.46 billion. 11
Optimizing postoperative care is vital for older patients as they recover from major head and neck surgery to avoid complications, minimize hospital readmissions, and decrease health care expenditure. In a study examining older patients undergoing head and neck ablation and reconstruction, out of the 376 patients who were followed, over half had a 30-day serious complication, 30 died within 90 days, and >30 declined to dependent status after surgery, proving that this demographic is particularly susceptible to poor outcomes. 5 To date, there has been limited study of older patient clinical follow-up and resource utilization in the first year after surgery for HNC. The aim of this study is to identify patient demographic, social, cancer, and treatment factors in older patients with HNC that may predict attending otolaryngology postoperative visits in the first year following major HNC surgery.
Methods
Patient Data Collection
This cohort study based on retrospective chart review was conducted within the Department of Otolaryngology at the UC Davis Medical Center (UCDMC) and received Institutional Review Board approval (No. 1529807). Clinical and surgical data were collected from the UCDMC electronic medical record for patients (N = 181) aged ≥60 years who were diagnosed with HNC (all patients with mucosal head and neck squamous cell carcinoma), initially presented to our institution, and ultimately underwent ablative head and neck surgery for HNC with at least a neck dissection with or without a free flap reconstruction between 2009 and 2019. The cutoff age of ≥60 years was utilized for “older patients,” as this age has been used in a number of studies exploring head and neck oncology.12-19
For each patient, the following variables were drawn from the electronic medical record: demographics, tumor characteristics, perioperative course, treatment regimen, complications per Clavien-Dindo classification with a dichotomous separation of grade <2 and ≥2 within 1 month postoperation,4,20 and postoperative disposition. These variables were than correlated with number of postoperative visits within the first year following surgery, given that total follow-up times varied greatly among patients. Postoperative visits were defined as in-person HNC clinic appointments with an HNC surgeon or nurse practitioner. Patients at our institution typically undergo close follow-up after surgery, then surveillance visits every 2 to 3 months from surgery for the first year, and subsequent follow-up per National Comprehensive Cancer Network guidelines, 21 with additional visits based on clinical judgment. Emergency department visits or inpatient admissions were excluded, as well as patients who did not undergo at least a neck dissection at our institution, traveled >200 miles to UCDMC, or had incomplete records. Distance traveled was measured as a straight line from the patient’s address to the hospital address.
Statistical Analysis
To analyze the association between the number of postoperative visits and continuous variables, Spearman correlations were calculated; for categorical variables, the Kruskal-Wallis test was conducted. For the multivariable analysis, a model selection procedure was implemented where those variables with significant associations (at the 0.05 level) in the univariate analyses were included in a multivariable regression model, and the effect size and significance of each variable were assessed after controlling for the others. This elucidated which variables were independently associated with and were stronger indicators for increased postoperative care.
Results
Patient Demographics
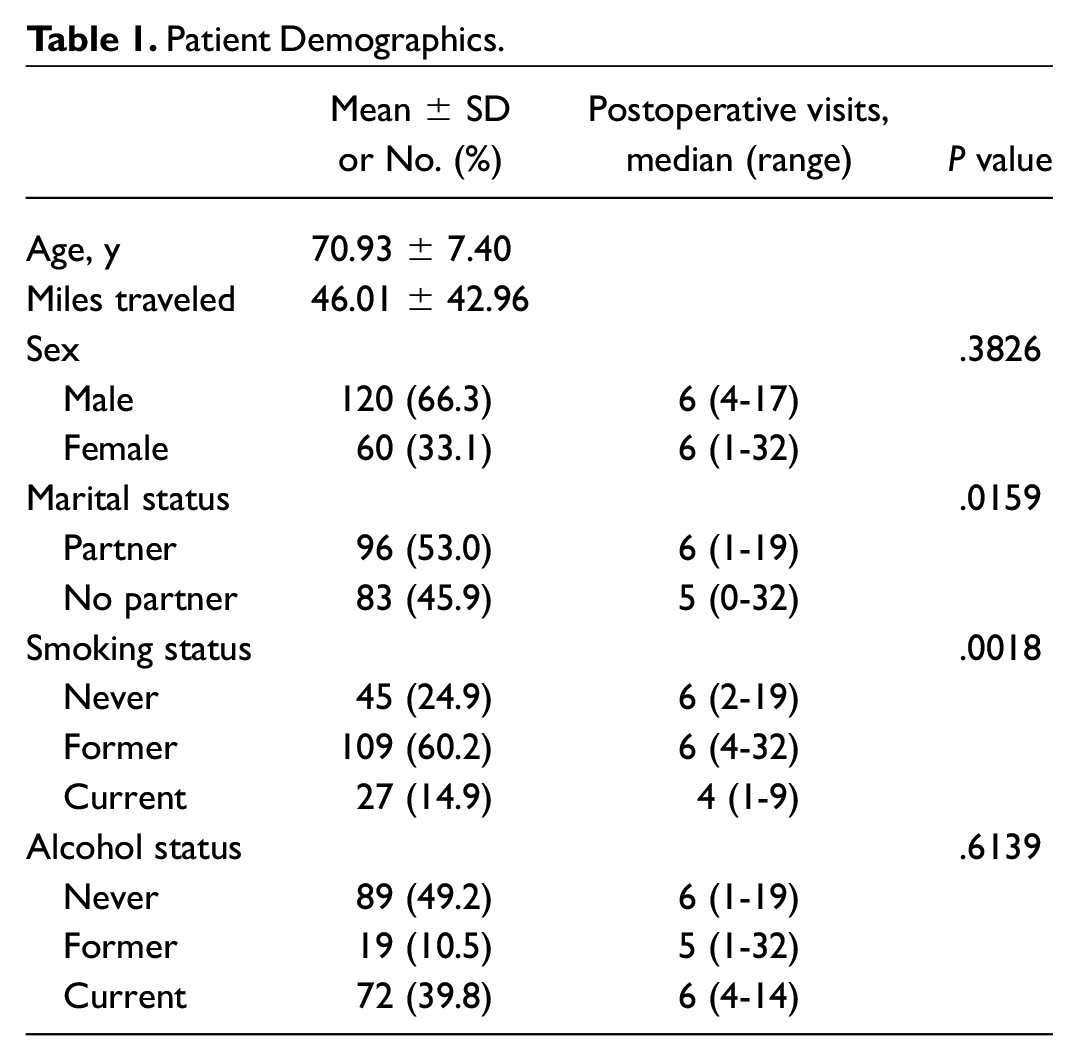
Table 1 summarizes the demographics of the 181 patients who underwent major head and neck surgery at UCDMC. Table 2 shows the patient presentation and workup. Most patients did not experience disease recurrence (81%) within the study timeline. The most common sites of HNC were the oral cavity (65%), oropharynx (15%), and larynx (16%). Forty-six percent of patients underwent free flap reconstruction, and 24% had a laryngectomy. Sixty-one percent of patients underwent postoperative adjuvant therapy.
Patient Demographics.
Patient Presentation and Workup.
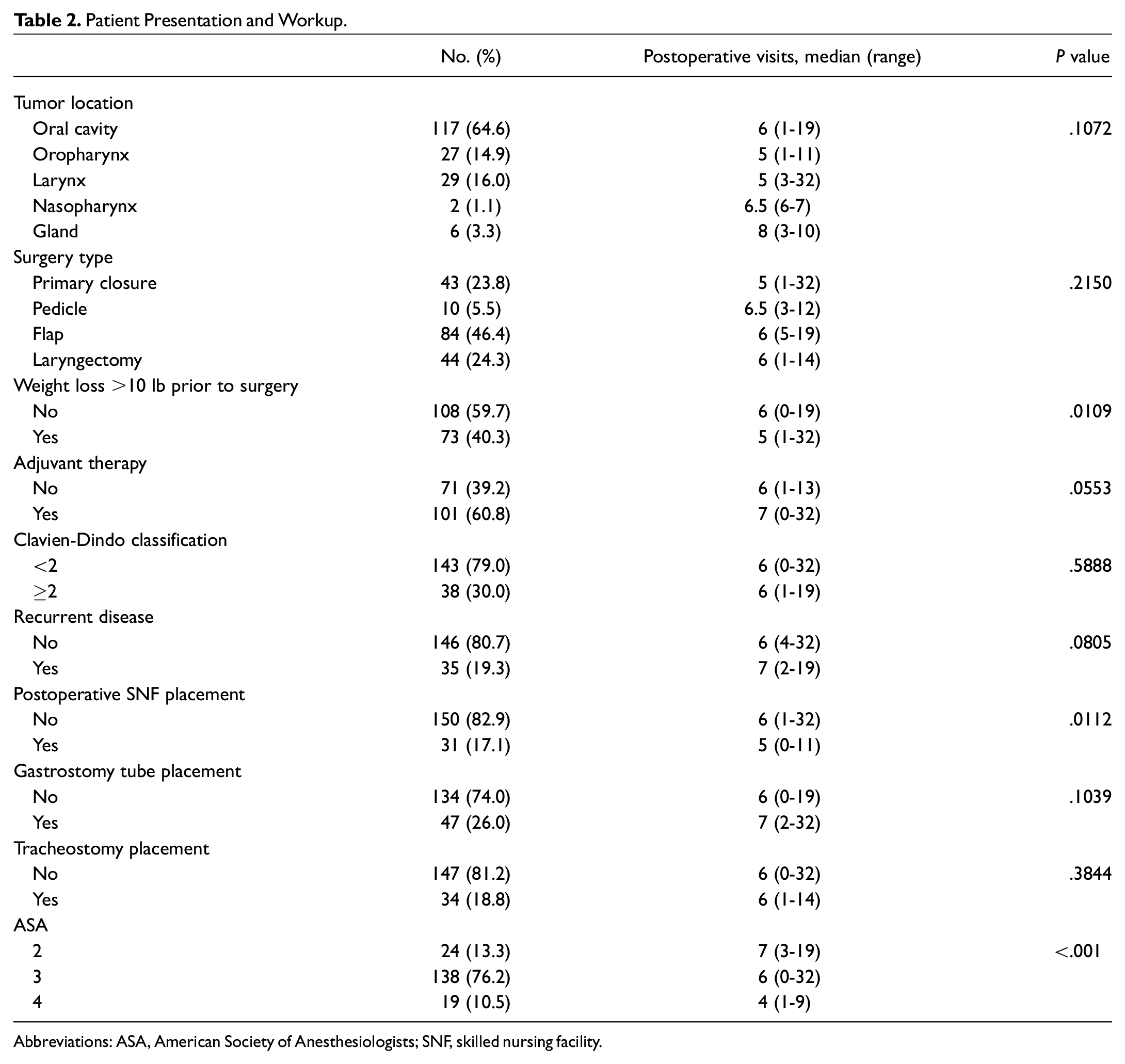
Abbreviations: ASA, American Society of Anesthesiologists; SNF, skilled nursing facility.
Univariate Factors Associated With Increased Postoperative Office Visits
Within a 1-year postoperative period, patients in our cohort had a mean ± SD 6.37 ± 3.6 postoperative clinic visits. Factors that were associated with increased posttreatment visits were having a partner (P = .0159), living a closer distance to the hospital (P = .0046), not being an active smoker (P = .0018), being discharged home rather than to a skilled nursing facility (SNF; P = .0112), ASA score (American Society of Anesthesiologists; P < .001), and weight loss >10 lb prior to surgery (P = .0109; Table 2 ). Receiving adjuvant therapy (P = .0553) was associated with an increased number of postoperative visits, though it did not reach statistical significance. Age, location of primary cancer, and extent of surgery were not statistically significant factors in the number of postoperative visits.
Factors Associated With Increased Postoperative Office Visits on Multivariable Analysis
In the multivariable model ( Table 3 ), distance traveled from home to hospital (P = .013) and postoperative radiation therapy (P = .0096) were significantly related to increased attendance of postoperative visits. The variables that were no longer significant included not being a current smoker (P = .097), having a partner (P = .656), having had weight loss >10 lb prior to surgery (P = .398), having an ASA status of 3 and 4 (P = .761 and .156, respectively), and receiving adjuvant chemotherapy (P = .959). While receiving adjuvant chemoradiation therapy did not reach significance, receiving radiation therapy alone was associated with an average 1.46 more postoperative appointments (P = .0096) against no adjuvant therapy at all. The average numbers of postoperative appointments for patients who received no adjuvant, radiation, and chemoradiation therapy were 5.27, 6.55, and 5.17, respectively. For every 10-mile increase in distance traveled, an average 0.15 fewer appointments were attended (P = .013; Figure 1 ).
Multivariate Analysis.
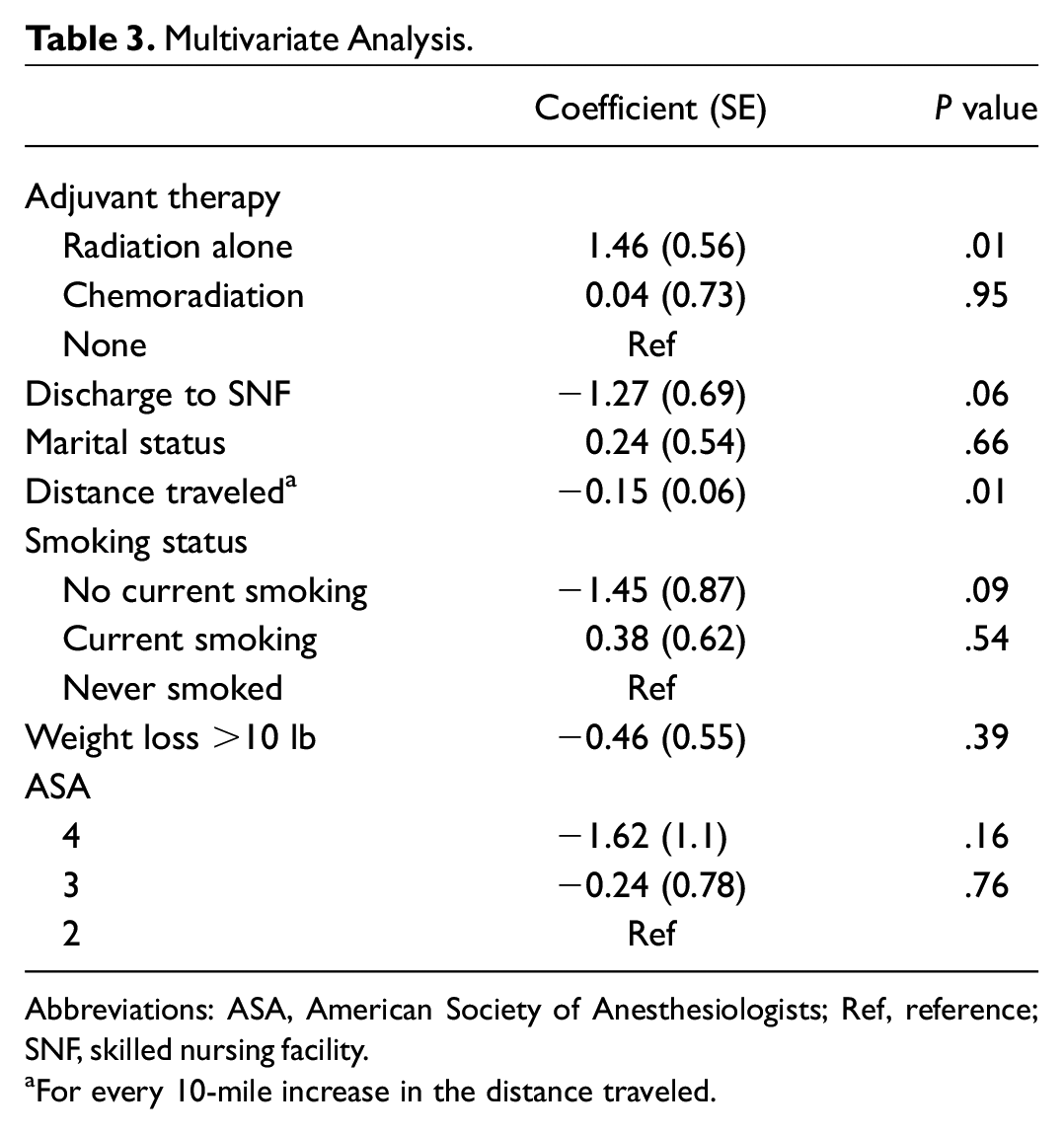
Abbreviations: ASA, American Society of Anesthesiologists; Ref, reference; SNF, skilled nursing facility.
For every 10-mile increase in the distance traveled.
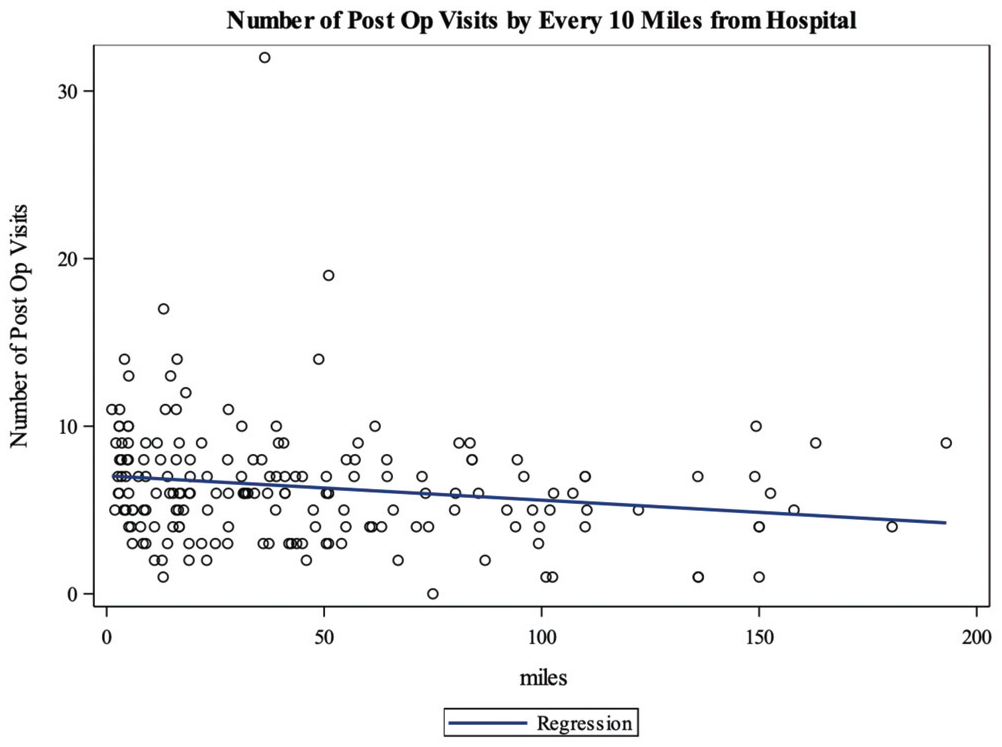
Number of postoperative visits by every 10 miles from hospital. The scatterplot indicates that there are fewer postoperative visits with an increase in distance from the hospital.
Discussion
In this study, we identified that for older patients, increased distance to the hospital and postoperative discharge to an SNF were associated with decreased postoperative visits for the ensuing year after surgery. With the increased life expectancy and subsequent increase in HNC diagnoses in the older population, it has become more important to determine patient factors associated with adequate surveillance and appropriate postoperative follow-up.
Overall, patients in our study had a median follow-up of 6.4 visits within a 1-year period, with 70% attending at least 4 visits, which is the National Comprehensive Cancer Network’s recommended minimum number of visits for surveillance in the first year following treatment. In a 2022 cross-sectional study by Hoyle et al, 10.6% of patients with HNC were lost to follow-up within 2 years, 22 and in a retrospective cohort study, Gill et al showed that 50% of patients with cancer were lost to follow-up at 5 years. 23 In a cohort study examining the importance of the time between surgery and postoperative radiation therapy in the combined management of HNC, a delayed start of postoperative care adversely affected the results of combined surgical and radiotherapeutic management of HNC. 24 These included primary and secondary site recurrence, metastases to distant sites, and death due to metastases. 24
Studies have demonstrated that age is a significant risk factor for predicting postoperative morbidity after head and neck surgery; therefore, thorough pretreatment evaluation and care for older patients are required. 25 Medical conditions such as diabetes, cardiovascular disease, and pulmonary disease are reported risk factors of surgery in older patients. 24 The presence of comorbidities in older patients is a key indicator against surgery because comorbidities increase the risk of postoperative complications. 26 This may also be attributed to the frailty of older patients with an impaired ability of the immune system to generate an efficient response against tumors and an even poorer tolerance to the applied therapies. The therapies are consequently less aggressive and less effective. 27 This seemingly necessary monitoring occurs with attendance of postoperative visits that can guide patients in the months following their surgery alongside potential adjuvant therapy. Patients discharged to an SNF may not be monitored as closely as those at home with a friend or family member.
Ambroggi et al noted that the burden of travel from patient to provider influences access and care of patients with cancer, with greater distances creating delays in diagnosis and care. 28 In particular, distance traveled to the hospital can influence stage of presentation, appropriate treatment and follow-up, oncologic outcomes, and quality of life. Treating institutions are set in large urban settings, and the patients in the farther, small urban, and rural areas are faced with barriers to food, safety while outside the home, and higher poverty rates. 28 Farther distances from treating hospitals also show a decrease in radiotherapy follow-up and treatment completion. 29 Studies have shown a predictable pattern of the effect of distance on frequency of contact and that patients who traveled longer distances to see their providers were more affected in utilizing medical services. 30 Later-stage diagnosis for cancer in Medicaid patients was significantly associated with greater travel distances to providers: for every 100-mile increase in driving distance to a primary care physician, the odds of a patient being diagnosed at a later stage of breast cancer increased by 49%. 31
Patients with adjuvant therapy, which included radiation or chemoradiation, had an increased number of attended postoperative visits (P = .034). This is understandable, as patients who participated in adjuvant therapy were required to come back to the hospital for chemotherapy and/or radiation administration. Adjuvant therapy can also require more scheduled visits with radiation oncology and medical oncology for specialized follow-up outside the surgical teams that can monitor postoperative care. Additionally, toxicities of adjuvant therapy for HNC can require a patient to return for more follow-up visits to manage these iatrogenic symptoms. Radiation therapy is associated with toxicities, short-term (within 3 months after completion) and long-term (after 3 months), and can include cell damage leading to mucosal membrane damage, lung tissue injury, gastrointestinal damage, and vascular damage. 32
There are several limitations inherent to a retrospective design. The postoperative appointments recorded were not differentiated between a routine surveillance visit and a nonroutine visit. It would be difficult then to see whether the increased number of postoperative visits was not confounded by additional visits. A bias associated with distance traveled from home to hospital is that patients who do live far away may visit other hospitals closer to their homes. Due to patients traveling far distances, it is also likely that all emergency department and inpatient admissions may not be at the home institution and were not included as an outcome measure of the study. Patients in this study had varying degrees of ablation and reconstruction with more complex surgery potentially being prone to higher morbidity and therefore higher postoperative needs. This is a single-institutional experience, which may not be generalizable to other centers.
Conclusion
This study elucidated factors that may predict the likelihood that a patient attends a scheduled posttreatment visit, which can help clinicians identify patients at risk for poor follow-up. Patients who live closer to the hospital and are discharged home are more likely to follow up in the first year after major head and neck surgery.
Footnotes
This article was presented at the Virtual AHNS 10th International Conference on Head and Neck Cancer; July 22-25, 2021.