
Abstract
Objective
To assess the effect of local anesthetic injection on subjective pain scores for pediatric tonsillectomies on postoperative days (PODs) 0 and 1.
Data Sources
A comprehensive literature search was conducted with the PubMed, Embase, Web of Science, and Scopus databases.
Review Methods
A 2-researcher team following the PRISMA guidelines performed a systematic review and meta-analysis. Studies with original data and a saline injection control arm were selected. Corresponding authors were contacted for missing data. The collated data were analyzed with RevMan version 5.4 (Review Manager; Cochrane Collaboration). Random effects modeling and standard mean difference were utilized to control for heterogeneity. Surgical technique subgroup analysis was performed.
Results
A total of 319 publications were identified, and 8 articles with 13 experimental arms (627 participants) were selected for meta-analysis. Local anesthetic injection was compared with placebo with saline injection. The standard mean difference for POD 0 pain was −0.81 (95% CI, −1.16 to −0.46; P < .00001) in favor of local anesthetic. The standard mean difference for POD 1 was −1.13 (95% CI, −1.48 to −0.78; P < .00001) in favor of local anesthetic. Subgroup analysis by surgical technique showed a less robust effect for cautery excision (−1.01 [95% CI, −1.37 to −0.66]) vs cold excisional technique (−1.19 [95% CI, −1.64 to −0.74]), with or without cautery-based hemostasis.
Conclusions
A local anesthetic injection during a pediatric tonsillectomy reduces postoperative pain on POD 0 and 1. Further analysis on total narcotic use and postoperative complications would benefit surgeon decision making.
Tonsillectomy is one of the most common ambulatory surgical procedures performed in the pediatric population, reaching an estimated 340,000 total ambulatory procedures in 2010 in the United States. 1 Due to its ubiquity, a range of techniques and adjuncts exist, with mixed results. 2 Despite grade A evidence revealing that a local bupivacaine injection reduces subjective pain, 3 local anesthetic is not discussed in guidelines from the American Academy of Otolaryngology–Head and Neck Surgery. 4 Additional studies have focused on the timing of injection—specifically, whether an injection prior to or immediately following tonsillectomy has a larger impact on postoperative pain. 5 However, reducing postoperative pain and subsequent narcotic use remains a hot-button topic.6,7
To better understand the effects of local anesthetic injection on pediatric tonsillectomy, a systematic review and meta-analysis was performed. The objective of this study was to assess the effect of local anesthetic injection as compared with saline injection on subjective pain scores for pediatric tonsillectomies on postoperative days (PODs) 0 and 1. Secondary analysis included assessment of tonsillectomy technique and injection timing on subjective pain scores.
Methods
Systematic Review
A 2-researcher team following the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses) performed a systematic review on August 1, 2020. A comprehensive literature search was conducted with the search terms “tonsillectomy,”“pediatric,”“injection,” and “local anesthetic” on the PubMed, Embase, Web of Science, and Scopus databases. Inclusion criteria included English-language manuscript, original data, randomized controlled trials, pediatric tonsillectomies with or without adenoidectomy, local anesthetic injection as compared with saline injection controls, and a patient population <18 years of age. Exclusion criteria were lack of reported subjective pain scale data on POD 0 or 1, use of the opposite tonsil in the same patient as the control, data consisting of adult patients that could not be separated, or patients ≥18 years old. Corresponding authors were contacted for missing data, which were used if possible. Risk of bias was assessed with the revised Cochrane risk of bias tool for randomized trials.
Meta-analysis
The data were analyzed with RevMan version 5.4 (Review Manager; Cochrane Collaboration). Meta-analysis utilized random effects statistical modeling, standard mean difference, and inverse variance weighting. If a study had >1 experimental arm meeting inclusion criteria, the arms were treated as separate groups and compared with the same saline control group. If additives were included with the local anesthetic in the injection, they were notated by a predesignated acronym and included in the forest plots to ease identification. Subgroup analysis was performed for surgical technique and timing of injection. Surgical technique subgroups were as follows: cold technique only (no electrocautery used), cold technique with electrocautery (electrocautery used only for hemostasis), and electrocautery (electrocautery used for excision and hemostasis). Subgroups by timing of injection were pretonsillectomy injection (injection of local anesthetic prior to excision of tonsils) and posttonsillectomy injection (injection of local anesthetic after excision of tonsils).
Statistical Analysis
If multiple data points were available, the highest pain score in the control arm and the correlating pain score in the experimental arm were selected for analysis. Each meta-analysis was assessed for significant heterogeneity (I2) and overall effect (Z) with an alpha of 0.05. Each subgroup analysis was also assessed for significant I2 and Z and subgroup differences, with an alpha of 0.05.
Results
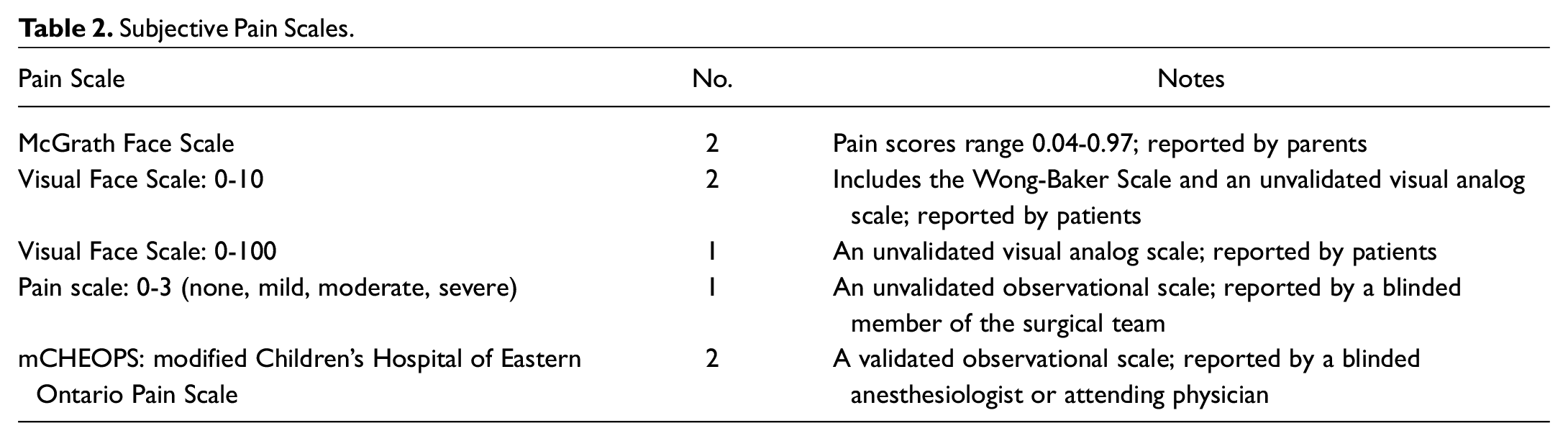
A total of 506 publications were queried, 187 duplicates were removed, and 319 abstracts were screened. After screening, 11 full-text articles met inclusion criteria and were reviewed, with 3 being excluded due to incomplete pain score reporting and inability to access the complete data. The remaining 8 articles were included in meta-analysis and accounted for 13 experimental arms ( Figure 1 ).8-15 Study and patient characteristics are outlined in Table 1 , and risk of bias for each study is described in Figure 2 . Only 1 study contained information on length of stay or time spent in the postanesthesia care unit. The local anesthetics and additives used are depicted in each forest plot legend. The subjective pain scales utilized were the McGrath Face Scale, Visual Face Scale, an unvalidated 0-3 pain scale, and the modified Children’s Hospital of Eastern Ontario Pain Scale ( Table 2 ). None of the studies utilized dexamethasone (Decadron) during anesthesia induction.
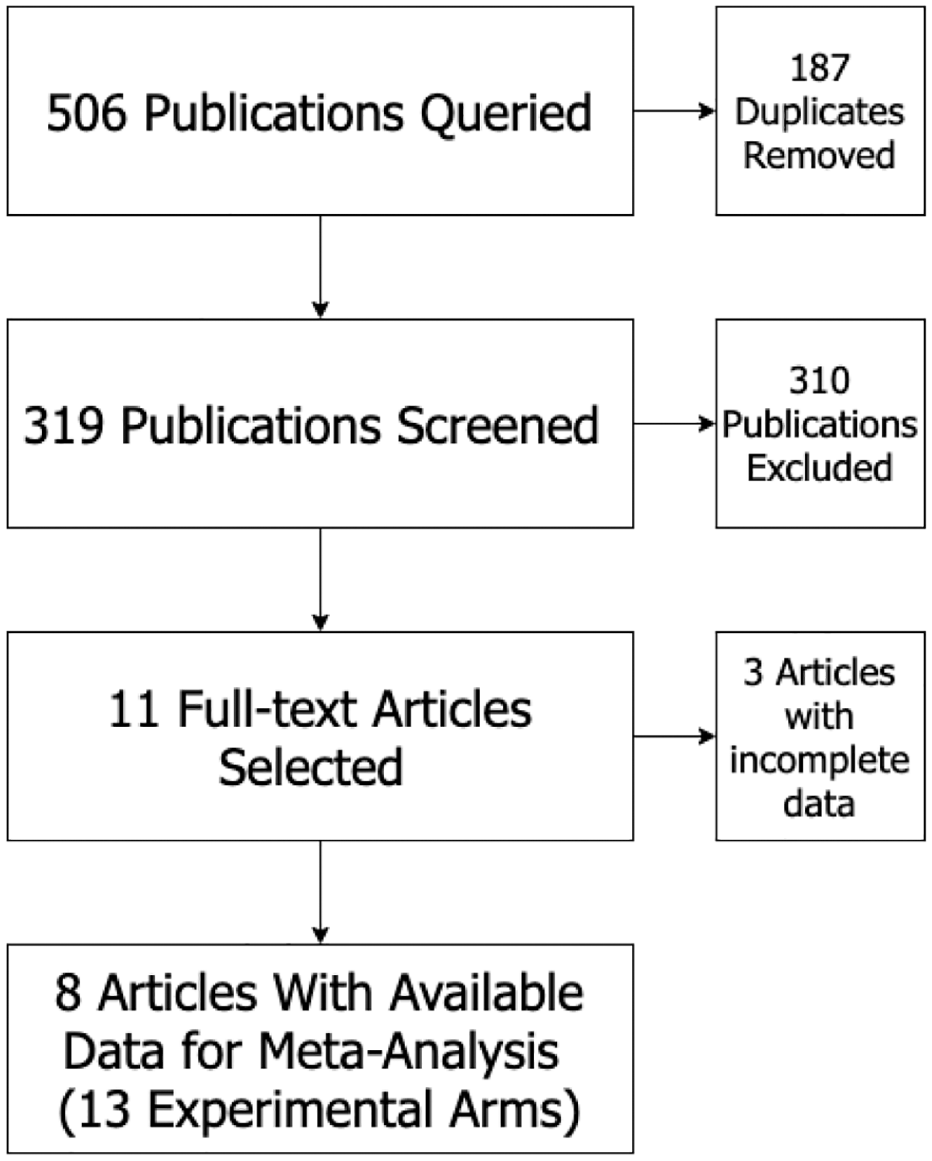
Flow diagram of the literature search based on the PRISMA recommendations (Preferred Reporting Items for Systematic Reviews and Meta-analyses).
Study Characteristics.
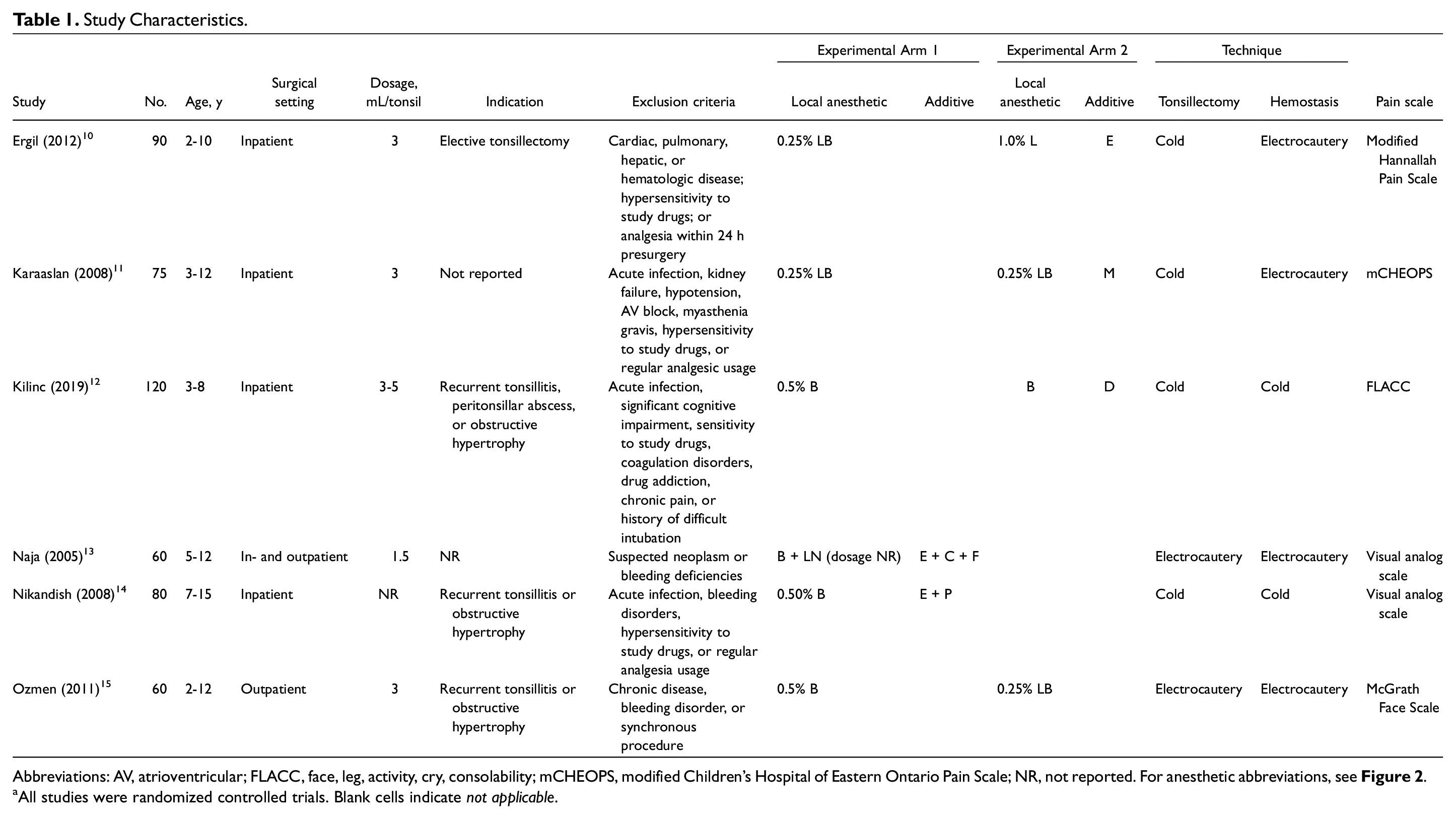
Abbreviations: AV, atrioventricular; FLACC, face, leg, activity, cry, consolability; mCHEOPS, modified Children’s Hospital of Eastern Ontario Pain Scale; NR, not reported. For anesthetic abbreviations, see Figure 2 .
All studies were randomized controlled trials. Blank cells indicate not applicable.
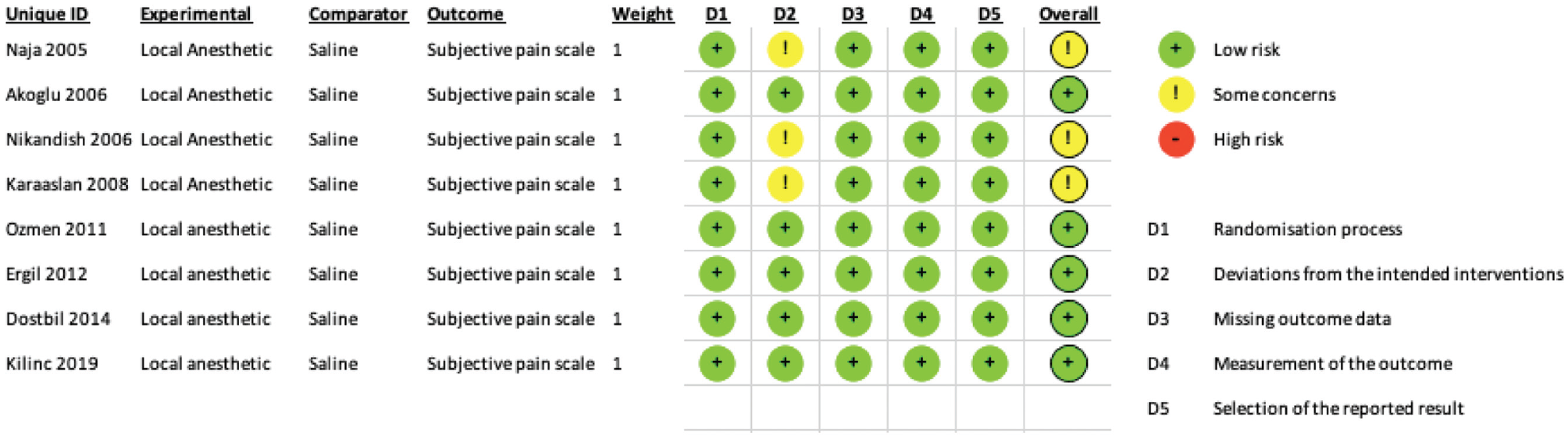
Bias assessment results per RevMan version 5.4 (Review Manager; Cochrane Collaboration).
Subjective Pain Scales.
The first meta-analysis compared subjective pain scores at 1 hour postoperatively ( Figure 3 ) and included 6 studies with 10 experimental arms. The standard mean difference, Z = 3.17 (P = .002), was in favor of local anesthetic, with significant heterogeneity, I2 = 88% (P < .00001). Subgroup analysis of the tonsillectomy technique identified overall effects for electrocautery, the cold technique with electrocautery, and the cold technique only: Z = 0 (P > .99), Z = 2.39 (P = .02), and Z = 2.25 (P = .02), respectively. The test for subgroup differences was significant (P = .02). Statistically significant heterogeneity was found within 2 groups: cold technique with electrocautery and cold technique only. Subgroup analysis of pre- and posttonsillectomy injection identified overall effects of Z = 2.43 (P = .02) and Z = 2.57 (P = .01), both in favor of local anesthetic. The test for subgroup differences was insignificant (P = .06), and significant heterogeneity was found within both groups.
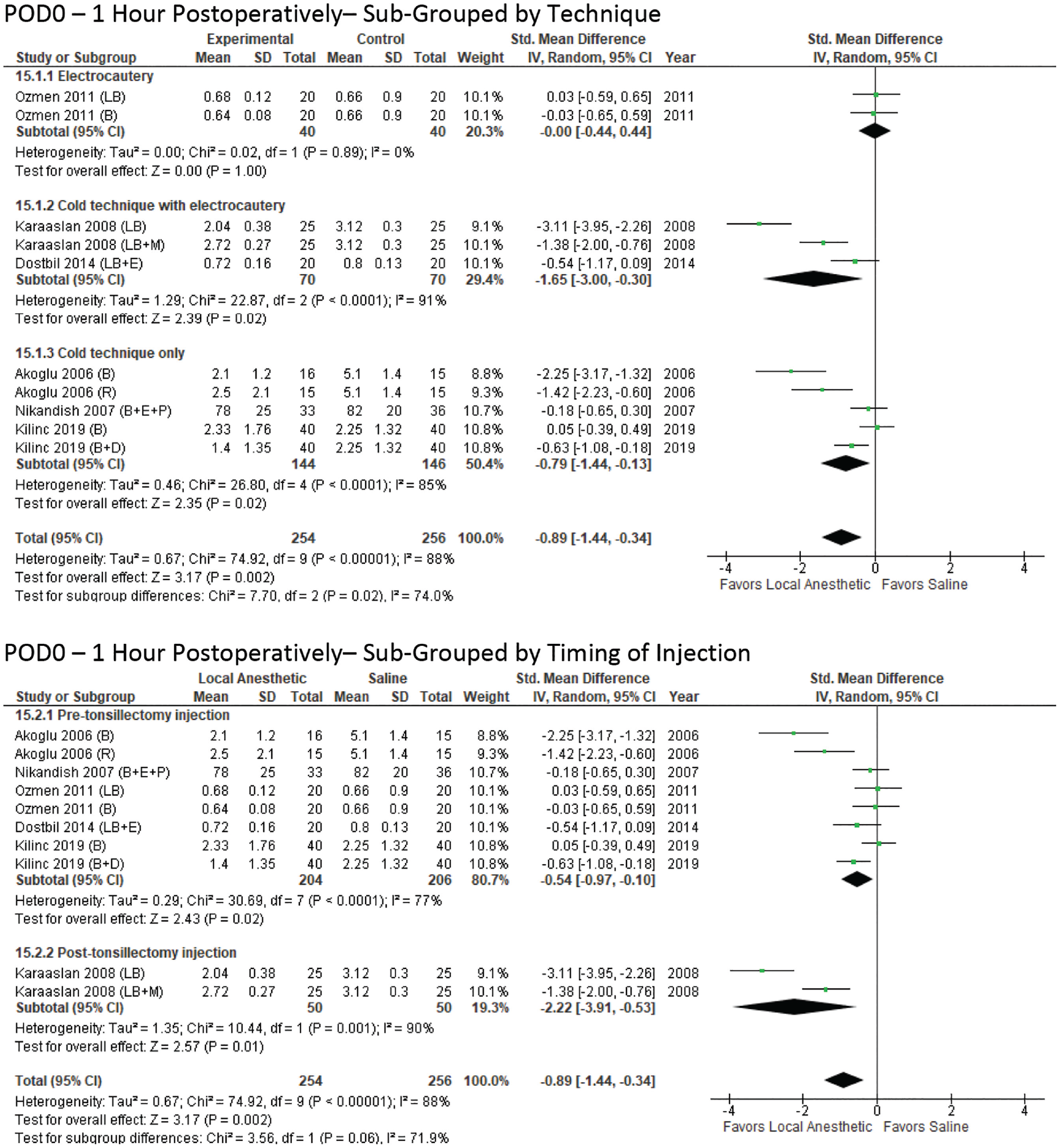
Postoperative day 0 (at 1 hour postoperatively) by technique. Subgroup analysis of pre- and posttonsillectomy injection identified overall effects in favor of local anesthetic.
The second meta-analysis compared subjective pain scores between postoperative hours 4 and 8 on POD 0 ( Figure 4 ). All 8 studies and 13 experimental arms were included. The standard mean difference, Z = 3.94 (P < .0001), was in favor of local anesthetic, with significant heterogeneity, I2 = 93% (P < .00001). Subgroup analysis of tonsillectomy technique identified overall effects for electrocautery, the cold technique with electrocautery, and the cold technique only: Z = 1.78 (P = .07), Z = 2.29 (P = .02), and Z = 2.86 (P = .004), respectively. All subgroups had significantly high heterogeneity. Subgroup analysis of pre- and posttonsillectomy injection identified overall effects of Z = 3.16 (P = .002) and Z = 4.64 (P < .00001), both in favor of local anesthetic. The test for subgroup differences was significant (P < .0001), and significant heterogeneity existed within both groups.
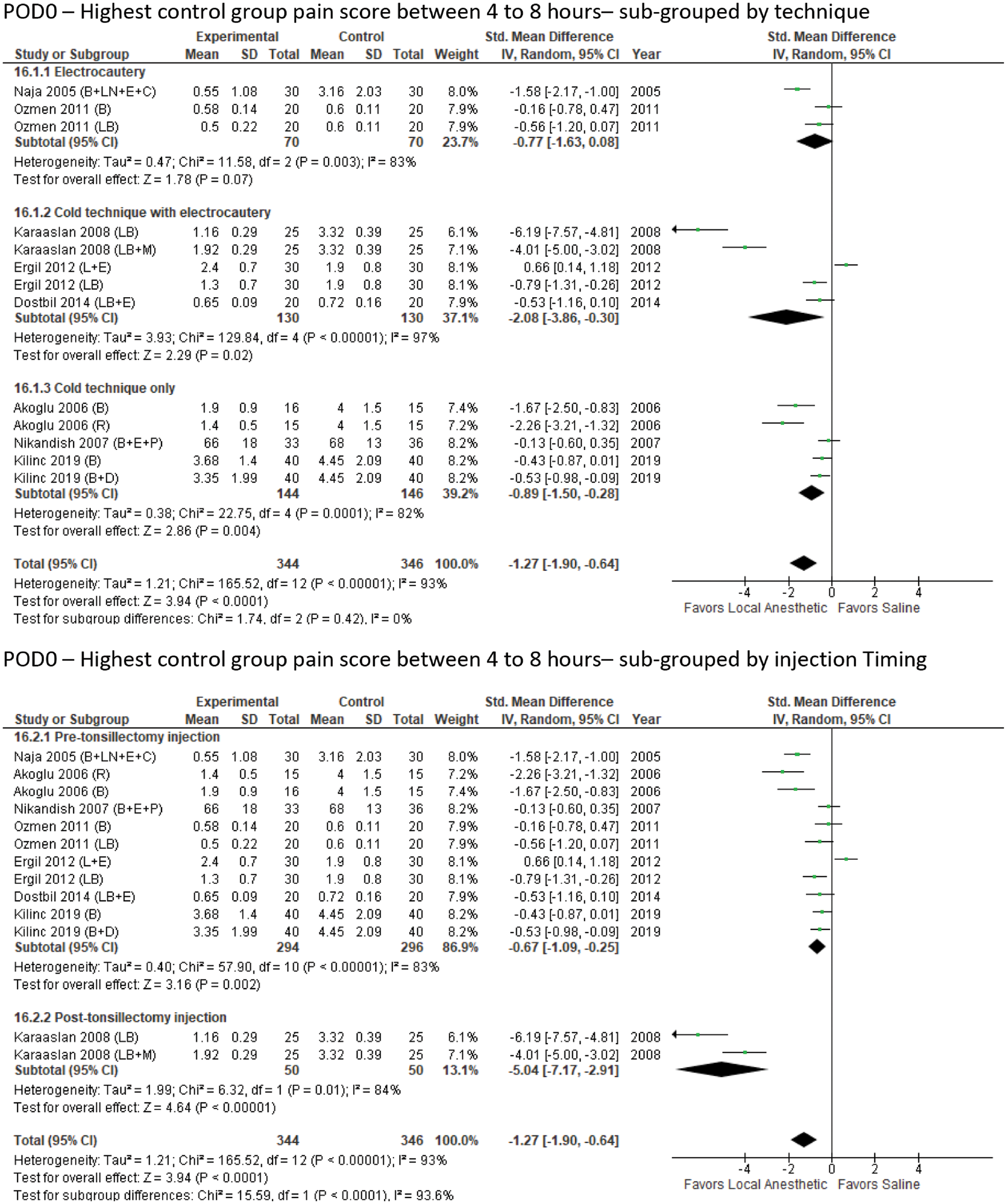
Postoperative day 0: highest control group pain score between 4 and 8 hours by technique. The mean difference was in favor of local anesthetic.
The final meta-analysis compared subjective pain scales for POD 1, reported as either the 24th hour or a single recording for POD 1, and comprised all 8 studies and 13 experimental arms ( Figure 5 ). The standard mean difference, Z = 6.34 (P < .00001), was in favor of local anesthetic, with significant heterogeneity, I2 = 77% (P < .00001). Subgroup analysis of tonsillectomy technique identified overall effects for electrocautery, the cold technique with electrocautery, and the cold technique only: Z = 5.61 (P < .00001), Z = 3.3 (P = .001), and Z = 3.85 (P = .0001), respectively. There was no significant difference among subgroups (P = .8). Significant heterogeneity was found within 2 groups: cold technique with electrocautery and cold technique only. Subgroup analysis of pre- and posttonsillectomy injection identified overall effects of Z = 6.03 (P < .00001) and Z = 5.03 (P < .00001), both in favor of local anesthetic. Test for subgroup differences was significant (P = .01). Heterogeneity was moderately high and statistically significant for the pretonsillectomy injection group only.
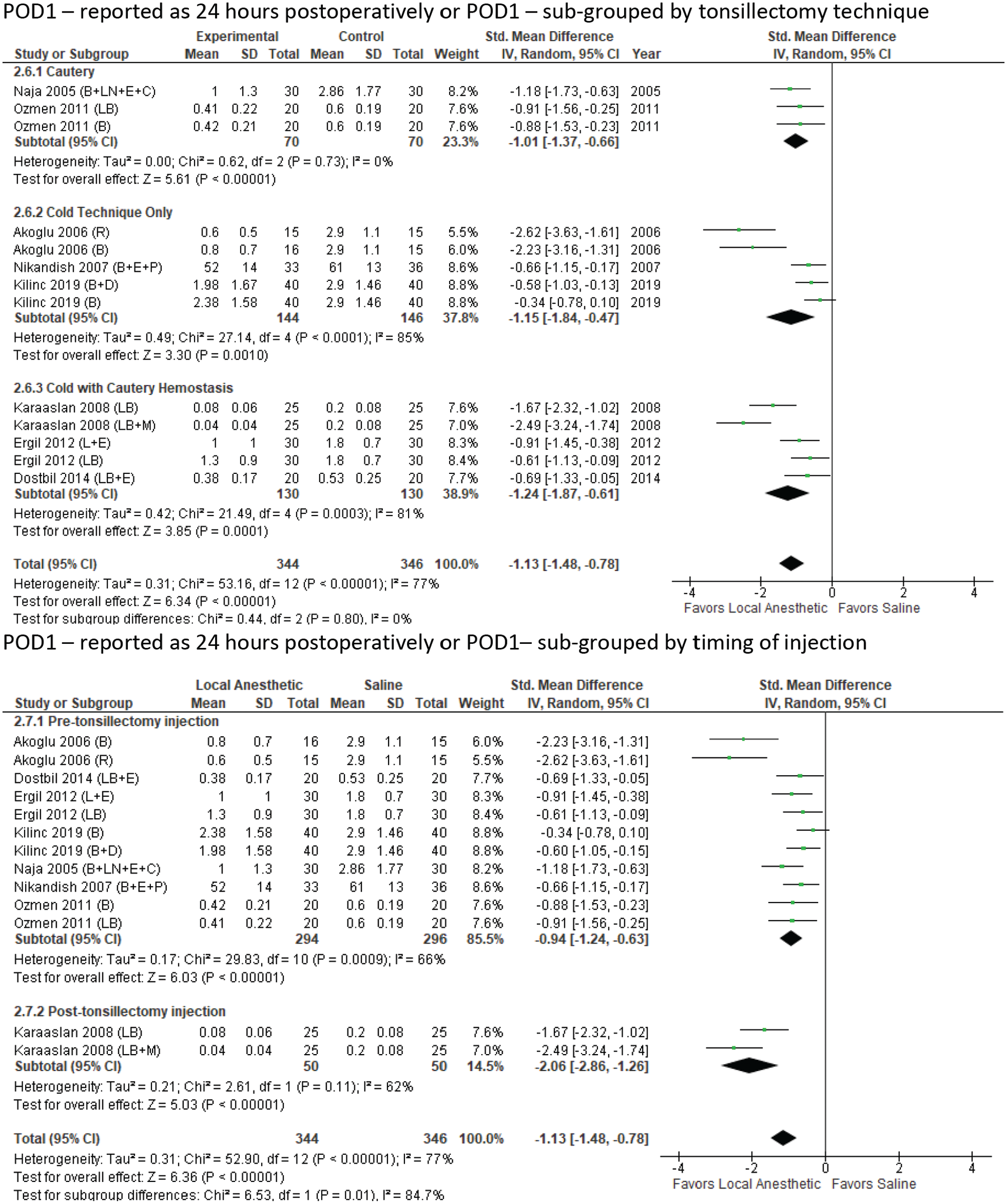
Postoperative day 1 (or reported as 24 hours postoperatively) by tonsillectomy technique. The standard mean difference was in favor of local anesthetic.
Discussion
Meta-analyses confirm that a local anesthetic injection reduces postoperative pain for pediatric tonsillectomies on PODs 0 and 1, consistent with a prior meta-analysis with 7 studies utilizing topical or locally injected anesthetics. 3 Bupivacaine (with or without epinephrine), levobupivacaine (with or without epinephrine), lidocaine with epinephrine, and ropivacaine all have a duration of action of 3 to 6 hours, making them easier to compare than other anesthetics.16-18 Interestingly, subgroup analysis on pain scores reported in the 4- to 8-hour time frame identified a significant difference favoring local anesthetic in 2 groups: cold technique only and cold technique with electrocautery. This pattern was true for the first meta-analysis as well, which tested subjective pain scales at 1 hour postoperatively. The third meta-analysis, analyzing pain on POD 1, showed statistical significance in favor of local anesthetic in all 3 tonsillectomy technique groups.
How local anesthetic injections reduce pain 4 to 6 hours postoperatively and, even more surprising, that their effects continue into POD 1 is unclear. However, long-lasting effects of anesthetic injections have been seen across other surgical domains. 19 The palatine tonsil has a dense arterial supply receiving branches from the facial artery, greater palatine artery, ascending pharyngeal artery, and dorsal lingual artery, and electrocautery is often used to control bleeding. 20 Their effect could be related to the role of epinephrine in reducing bleeding and subsequently lessening the role of electrocautery. Additionally, local anesthetics are known to be less effective in acidic environments, such as an inflammatory state. 21 These mechanisms help to explain why the electrocautery-only group did not show a significant difference in subjective pain scales on POD 0. Nevertheless, just 4 experimental arms used epinephrine, and the first experimental arm by Ergil et al included lidocaine and epinephrine with electrocautery for hemostasis only, although subjective pain scales favored the control group. 10
Another explanation may be the desensitization of pain fibers by the local anesthetic. The palatine tonsils are innervated by the lesser palatine nerve (cranial nerve V2) and tonsillar branches of the glossopharyngeal nerve (cranial nerve IX). 20 In the pretonsillectomy injection studies, placement of injections was described as submucosal infiltration of the tonsillar pillars,8-10,12-15 while the posttonsillectomy injection study focused on the tonsillar fossa. 11 Subgroup analysis for injection timing identified posttonsillectomy injection to have a more robust overall effect (Z) than pretonsillectomy injection. However, it is important to note that posttonsillectomy injection consisted of just 1 study by Karaaslan et al, who used levobupivacaine without epinephrine in 2 experimental arms. 11 Given the significant heterogeneity identified among studies, concluding that subjective pain scores are more robust when injection is performed after tonsillectomy may be a type I error.
Further subgroup analysis was performed for experimental arms with or without epinephrine, dexamethasone, or clonidine, and no meaningful conclusions were made. Meta-analyses were also performed for PODs 2 to 6, but there were significantly limited data for each time point, skewing the results due to selection bias.
As expected, there were significant limitations in our study related to the significant heterogeneity among the studies, such as the subjective pain scales as well as the local anesthetics and associated additives. To account for this, we utilized random effects statistical modeling, standard mean difference, and inverse variance weighting in the meta-analyses, as well as strict inclusion/exclusion criteria that required each study to have a control arm of separate patients who received a saline injection. However, it is encouraging that the risk of bias was low for all studies ( Figure 2 ). It should also be noted that just 2 studies (2 experimental arms) utilized a local anesthetic other than bupivacaine or levobupivacaine. White the overall results favor the injection of local anesthetic, this list is not representative of all local anesthetics, and there may be a difference in effectiveness based on the duration of action.
Conclusions
Injection of moderate-acting local anesthetics (duration of action, 3-6 hours) leads to lower subjective pain scores in pediatric tonsillectomies on PODs 0 and 1. This effect is more robust when a cold tonsillectomy technique is utilized with or without electrocautery and when the injection is done posttonsillectomy on POD 0 but is similar for all techniques on POD 1. Further analysis of narcotic usage, bleeding risk, and other complications would be help guide surgeon practice. Future studies would be helpful that investigated the effects of liposomal (long-acting) local anesthetics on pain control and complications for tonsillectomy.
Footnotes
This article was presented virtually at SENTAC; December 4, 2020.