
Abstract
Objective
To perform a qualitative evaluation of the Thyroid Network, with a quantitative analysis of second opinion referrals for patients in the southwestern part of the Netherlands who have thyroid nodules and cancer.
Methods
This prospective observational study registered all patients with thyroid nodules and cancer who were referred to the academic hospital from 2 years before and 4 years after the foundation of the Thyroid Network. We implemented biweekly regional multidisciplinary tumor boards using video conference and a regional patient care pathway for patients with thyroid nodules and cancer. For qualitative evaluation, interviews were conducted with a broad selection of stakeholders via maximum variation sampling. The primary outcome was the change in second opinions after the foundation of the Thyroid Network.
Results
Second opinions from Thyroid Network hospitals to the academic hospital decreased from 10 (30%) to 2 (7%) two years after the start of the Thyroid Network (P = .001), while patient referrals remained stable (n = 108 to 106). Qualitative evaluation indicated that the uniform care pathway and the regional multidisciplinary tumor board were valued high.
Discussion
Establishing a regional network, including multidisciplinary tumor boards and a care pathway for patients with thyroid nodules and cancer, resulted in a decrease in second opinions of in-network hospitals and high satisfaction of participating specialists.
Implications for Practice
The concept of the Thyroid Network could spread to other regions as well as to other specialties in health care. Future steps would be to assess the effect of regional collaboration on quality of care and patient satisfaction.
Introduction
Problem Description
In the southwestern part of the Netherlands (2.1 million habitants), clinical care for patients with thyroid nodules and cancer is provided by several hospitals: 1 academic hospital (Erasmus University Medical Centre), 4 large medical teaching hospitals, 1 and 5 general hospitals (approximately 5500 hospital beds; Figure 1 ). Despite the close proximity of these 10 hospitals to one another, no formal regional collaboration existed for the treatment of patients with thyroid nodules and cancer. This resulted in a lack of uniform protocols, absence of formal centralization rules for rare thyroid cancers, and a need for second opinions. Second opinions have the potential to make beneficial changes in treatment recommendations and prognosis in some patients. 2 However, physical second opinions for advice that does not deviate from the initial advice are an example of inefficient care, which can cause extra burden for patients entailing inconvenient travel, delays in care, and higher costs. In addition, reducing unnecessary second opinions could be of benefit for the climate in general and for infection prevention in terms of COVID-19 due to fewer travel needs.

The Thyroid Network hospitals in the southwestern region of the Netherlands.
Available Knowledge
Thyroid cancer is a relatively rare disease (4.7 cases per 100,000 inhabitants in the Netherlands) requiring sufficient medical expertise. Guidelines recommend the use of a multidisciplinary approach and structured care pathways as the standard of care for patients with thyroid cancer.3,4 Through continuous improvement, care pathways aim to improve the quality of clinical care and increase patient satisfaction and efficiency in the treatment of thyroid cancer.5-7
Patients discussed at multidisciplinary tumor boards (MTBs) are more likely to receive more accurate and complete recommendations regarding diagnostics and treatments, especially in cancer care.8-11 Online MTBs attended by multiple regional hospitals are feasible to design and implement in a collaboration network with 1 academic medical hospital surrounded by multiple general hospitals.12-14 In the absence of regional MTB programs, hospitals are modifying variables affecting the chances of curative treatment and survival among patients with other malignancies.15-18 However, the impact of regional MTBs on patient referral patterns among regional hospitals concerning cancer care is unknown.
Rationale
We reasoned that implementation of a regional MTB and structured care pathway would reduce local practice variation and second opinions to the academic hospital. A uniform care pathway and biweekly MTBs have the potential to enhance the quality of care of patients with thyroid nodules and cancer as a whole at a regional level.
Specific Aims
The aim of this study was to perform a qualitative evaluation of the Thyroid Network by means of structured interviews with participants. In addition, a quantitative assessment was performed of the number of second opinions referred from Thyroid Network hospitals to the academic center regarding patients with thyroid nodules and/or cancer.
Methods
Context
Foundation of the Thyroid Network
To achieve standardized regional care for patients with thyroid nodules and cancer, the SchildklierNetwerk (Thyroid Network) was formed in January 2016. This collaboration among 10 hospitals is managed by a daily board of 5 specialists. A scientific council was founded within the Thyroid Network to jointly review research initiatives and grant applications. Every 2 years, a regional symposium is organized at which updates on thyroid cancer are reviewed and scientific data are presented. Detailed information about the foundation of the Thyroid Network can be found in Additional File 1 (available online).
Interventions
Intervention 1a
A regional care pathway for patients with thyroid nodules and cancer was developed, which was adopted by all Thyroid Network hospitals (Additional File 2, available online).
Intervention 1b
Simultaneous with the start of the Thyroid Network, MTBs were implemented via video conference. Every 2 weeks, groups of 2 to 5 regional hospitals first conduct a local MTB, followed by 1 collective regional MTB with all participating hospitals. The local MTB existed prior to the initiation of the Thyroid Network. There are clear agreements in the regional care pathway for determining which patients will be discussed in the regional MTB.
Study of Interventions
Data Collection and Patients for Referral Analysis
The analyzed cohort comprised all patients registered in the academic hospital from 2 years before to 4 years after the Thyroid Network foundation and all patients discussed at the regional MTB in the 4 years after the foundation. All newly referred patients with thyroid nodules (including multinodular goiter) and cancer to the academic hospital were prospectively registered. Referrals for Graves’ disease, adjuvant radioactive iodine treatment, and other thyroid diseases were registered separately and therefore not included in this study. Baseline characteristics, diagnosis at presentation, way of entry in the academic hospital (second opinion, patient referral, or intercollegial consultation from another specialty in the academic hospital), treatment, and vital status were collected. A patient referral was defined as a definite transfer of patient care (eg, treatment or follow-up) from a general hospital to the academic hospital, while a second opinion was defined as a visit to a clinician in the academic hospital without transfer of care. Data were derived from the patient electronic health records and referral letters. The regional MTB data from individual patients were registered following a structured protocol. The form contained the local electronic health record number of the patient, the date of registration, and clinical characteristics such as TNM stage and the proposed treatment. TNM stages were described with the eighth edition of the AJCC Cancer Staging Manual. 19
Interviews
The BeterKeten Foundation conducted a qualitative interview study with a broad selection of stakeholders. Interviewees were selected by purposive sampling, as well as maximum heterogeneity sampling. 20 Purposive sampling involves the selection of interviewees with direct involvement to the research topic and aims to select information-rich cases for studying a topic in depth. Maximum heterogeneity sampling attempts to collect data from the most extensive range of perspectives possible about the topic of interest. In the current study, interviewees varied in age, medical specialty, hospital of employment, and duration of involvement with BeterKeten.
The interviews were conducted by applying a realistic evaluation approach to identify context factors and underlying mechanisms that influence collaboration. 21 In advance, 2 authors (E.V.B. and M.S.) developed an interview guide with a list of open-ended questions to explore context factors, mechanisms, and outcome patterns. A detailed description of these identified themes can be found in Additional File 3 (available online).
Measures
The primary outcome was the change in second opinions of in–Thyroid Network hospitals after the foundation of the Thyroid Network. Secondary outcomes were changes in second opinions from outside-network sources, patient referrals of in– and out–Thyroid Network sources, number of patients registered in the academic center, and findings from the interviews.
For the quantitative analysis of referral patterns within the academic hospital, 3 cohorts were defined. The first cohort comprised patients who were referred to the academic hospital in the 2 years before the referring hospital joined the Thyroid Network and thus had no regional MTB meeting available (pre-rMTB cohort). The second cohort consisted of all patients who were referred to the academic hospital or discussed in the regional MTB in the first 2 years after the referring hospital joined the Thyroid Network (early-rMTB cohort). Patients who were registered 2 to 4 years after the referring hospital joined the Thyroid Network were embedded in the continued cohort (cont-rMTB). A timeline regarding the foundation of the Thyroid Network and the cohorts is displayed in Figure 2 .
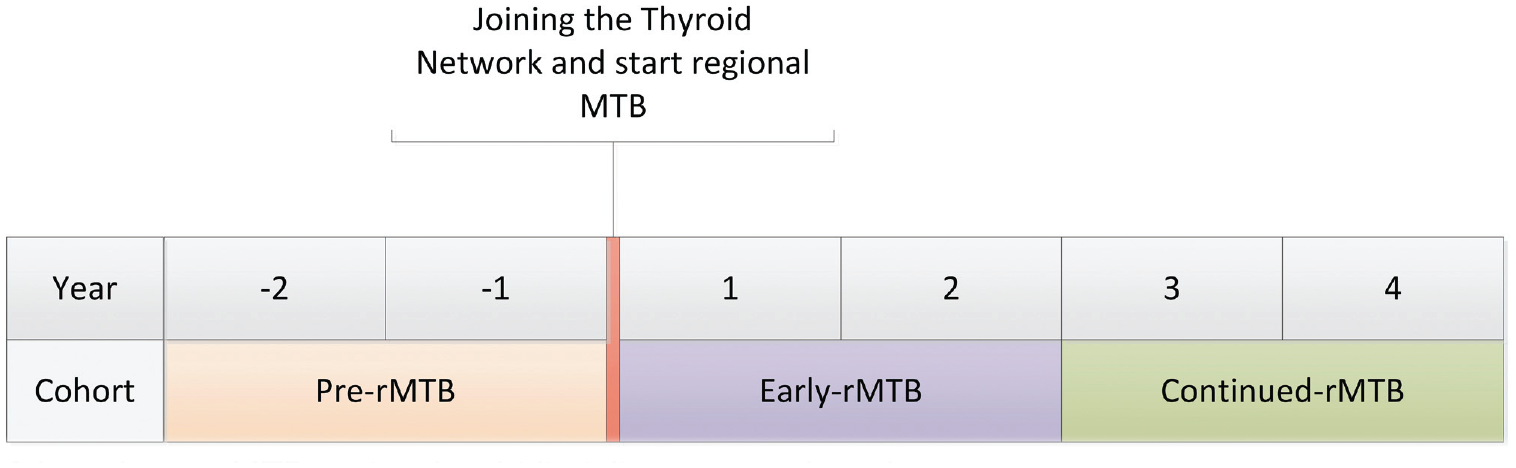
Timeline of the cohorts. rMTB, regional multidisciplinary tumor board.
The interviews were conducted face-to-face in the hospital or through video conferencing during the COVID-19 pandemic. All semistructured in-depth interviews were digitally audio recorded, anonymized, and transcribed ad verbum. All respondents (n = 24) gave permission to use the anonymous interview report for analysis.
Analysis
For the quantitative analysis, descriptive statistics were used to express continuous variables with normal distribution as mean with standard deviation or abnormal distribution as median with interquartile range. Distribution was assessed with the Shapiro-Wilk normality test. Categorical variables are described as count and percentage. Differences among the groups were analyzed with the Mood median test for continuous variables and the Pearson chi-square test for nominal variables. SPSS Statistics version 25 (IBM Corp) was used to perform all statistical analyses. P values <.05 were considered significant.
For the qualitative data analysis of the interviews, ATLAS.ti version 8 software (ATLAS.ti Scientific Software Development GmbH) was used. At first, codes were assigned to the verbatim transcription of the recordings (open coding of raw data). Next, coded text fragments were sorted and grouped into themes of context factors, mechanisms, and outcomes/values. These fragments and themes were compared by means of axial and selective coding, which allowed for detecting patterns in responses. The most relevant and illustrative quotes were selected to invigorate the results of the qualitative data analysis. A concept version of these results was returned to participants to check for accuracy and resonance with their experiences. This is also known as member checking or participant validation, a technique for exploring the credibility of results. 22
Ethical Considerations
This study was approved by the Medical-Ethics Committee of Erasmus Medical Centre (MEC-2018-1195). The SQUIRE 2.0 guideline was used (Revised Standards for Quality Improvement Reporting Excellence). 23
Results
Referral Patterns
Trends in New Patients With Thyroid Nodules or Cancer Referred to the Academic Hospital Without Being Discussed in a Regional MTB
Within the 6-year time frame ( Figure 2 ), 908 new patients with thyroid nodules or cancer were registered at the thyroid center in the academic hospital, without previous discussion in the regional MTBs. Diagnoses at presentation included a suspicious thyroid nodule (n = 460, 50.7%), thyroid cancer (n = 243, 26.8%), and multinodular goiter (n = 171, 18.8%). In total, 655 patients were referred from other hospitals (72.1%), 161 were referrals from other specialties within the academic hospital (17.7%), and 92 were referred for a second opinion (10.1%).
Analysis over the 3 cohorts (pre-, early-, and cont-rMTB) shows that second opinions from general hospitals within the Thyroid Network significantly decreased from 30.3% (n = 10) in the pre-rMTB cohort to 6.7% (n = 2) in the cont-rMTB cohort (P = .001). Second opinions from general practitioners decreased from 30.3% (n = 10) to 3.3% (n = 1), and second opinions from hospitals outside the region doubled. After the initiation of the Thyroid Network, more referrals from hospitals outside the region were received ( Table 1 ).
Clinical Characteristics of Newly Registered Patients in the Academic Hospital. a
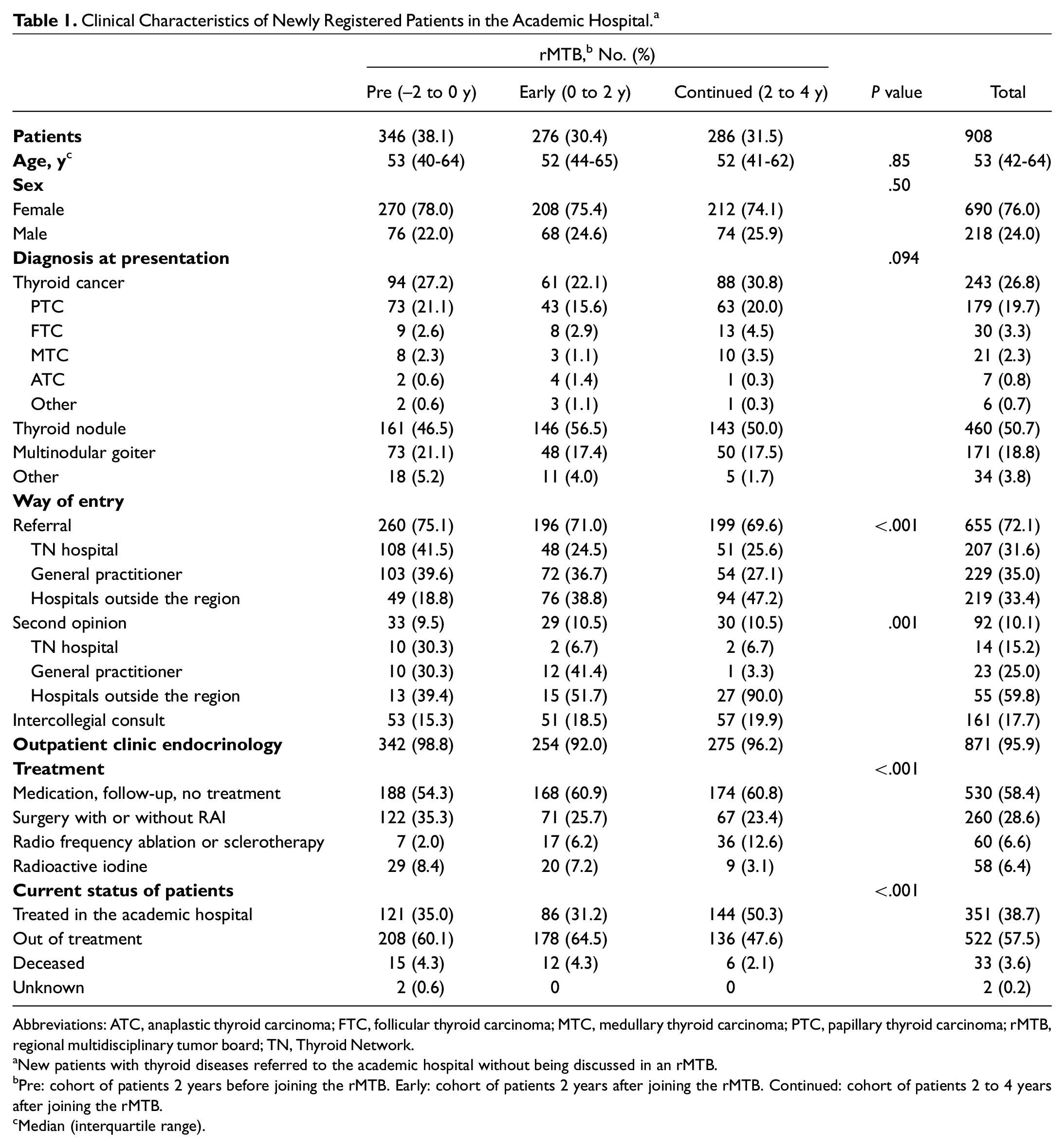
Abbreviations: ATC, anaplastic thyroid carcinoma; FTC, follicular thyroid carcinoma; MTC, medullary thyroid carcinoma; PTC, papillary thyroid carcinoma; rMTB, regional multidisciplinary tumor board; TN, Thyroid Network.
New patients with thyroid diseases referred to the academic hospital without being discussed in an rMTB.
Pre: cohort of patients 2 years before joining the rMTB. Early: cohort of patients 2 years after joining the rMTB. Continued: cohort of patients 2 to 4 years after joining the rMTB.
Median (interquartile range).
Patients Discussed in the Regional MTBs
In total, 309 patients were discussed in the regional MTBs in a time range of 4 years. Thirty-nine patients were discussed for other thyroid diseases (eg, parathyroid disease, autoimmune thyroiditis). These patients were excluded from the analysis, which resulted in 270 discussed patients with thyroid nodules and/or cancer. In the early-rMTB cohort, 41.6% (n = 62) of the patients discussed in the regional MTB were referred to the academic hospital, whereas this percentage was 47.9% (n = 57) in the cont-rMTB cohort ( Table 2 ).
Clinical Characteristics of Patients Discussed in the rMTBs.
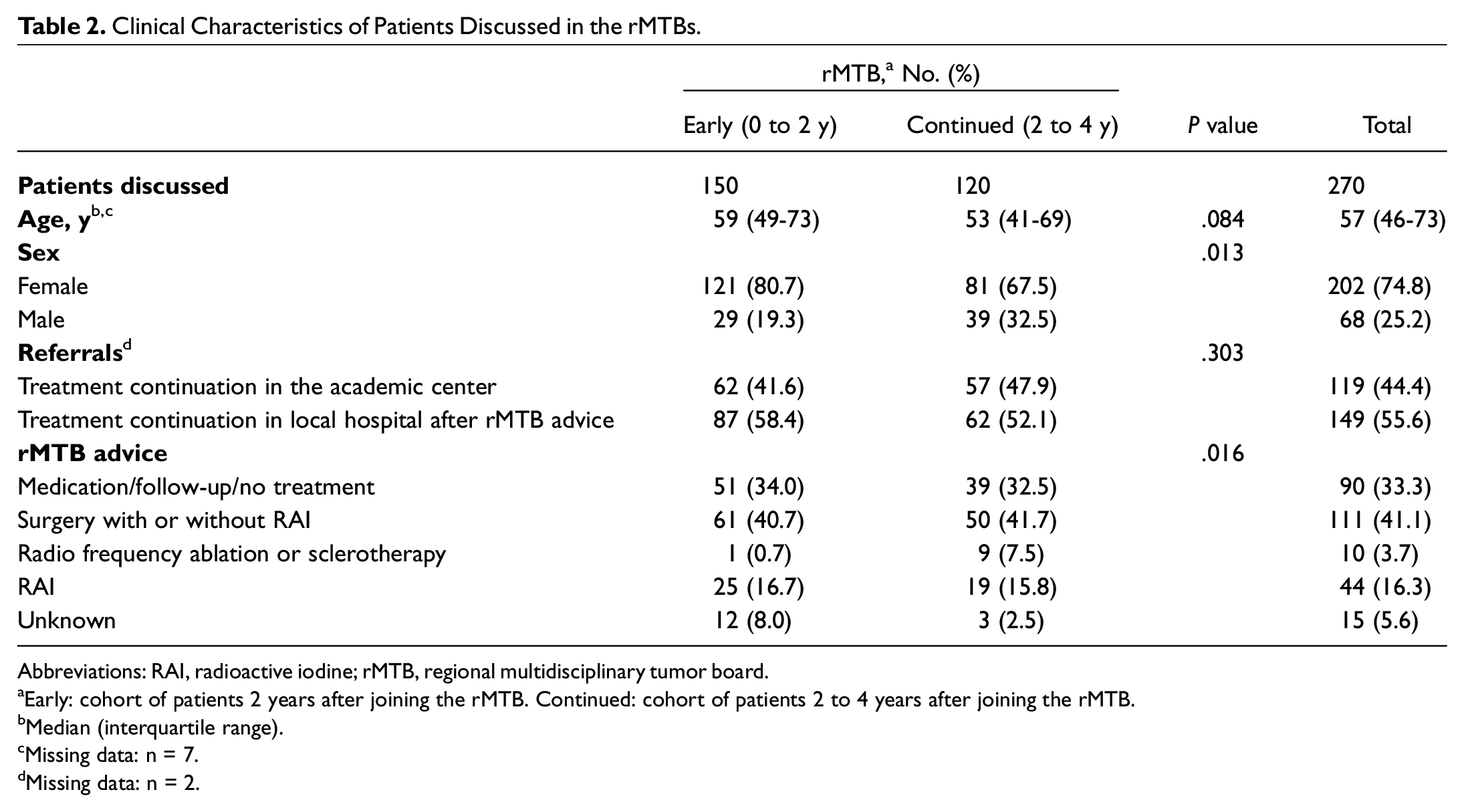
Abbreviations: RAI, radioactive iodine; rMTB, regional multidisciplinary tumor board.
Early: cohort of patients 2 years after joining the rMTB. Continued: cohort of patients 2 to 4 years after joining the rMTB.
Median (interquartile range).
Missing data: n = 7.
Missing data: n = 2.
Patients who were referred to the academic hospital after regional MTB discussion were more likely to have thyroid cancer (n = 90 [75.6%] vs n = 55 [36.9%], P < .001) and have a higher T stage than patients who were recommended to stay at the local hospital (P = .028). Also, 48% of patients with thyroid cancer referred to the academic hospital had lymph node metastases, as opposed to 7% who were recommended to stay at the local hospital (P < .001). Patients did not differ in M stage and overall TNM stage ( Table 3 ).
Differences in Clinical Characteristics of Patients Discussed in the rMTBs. a
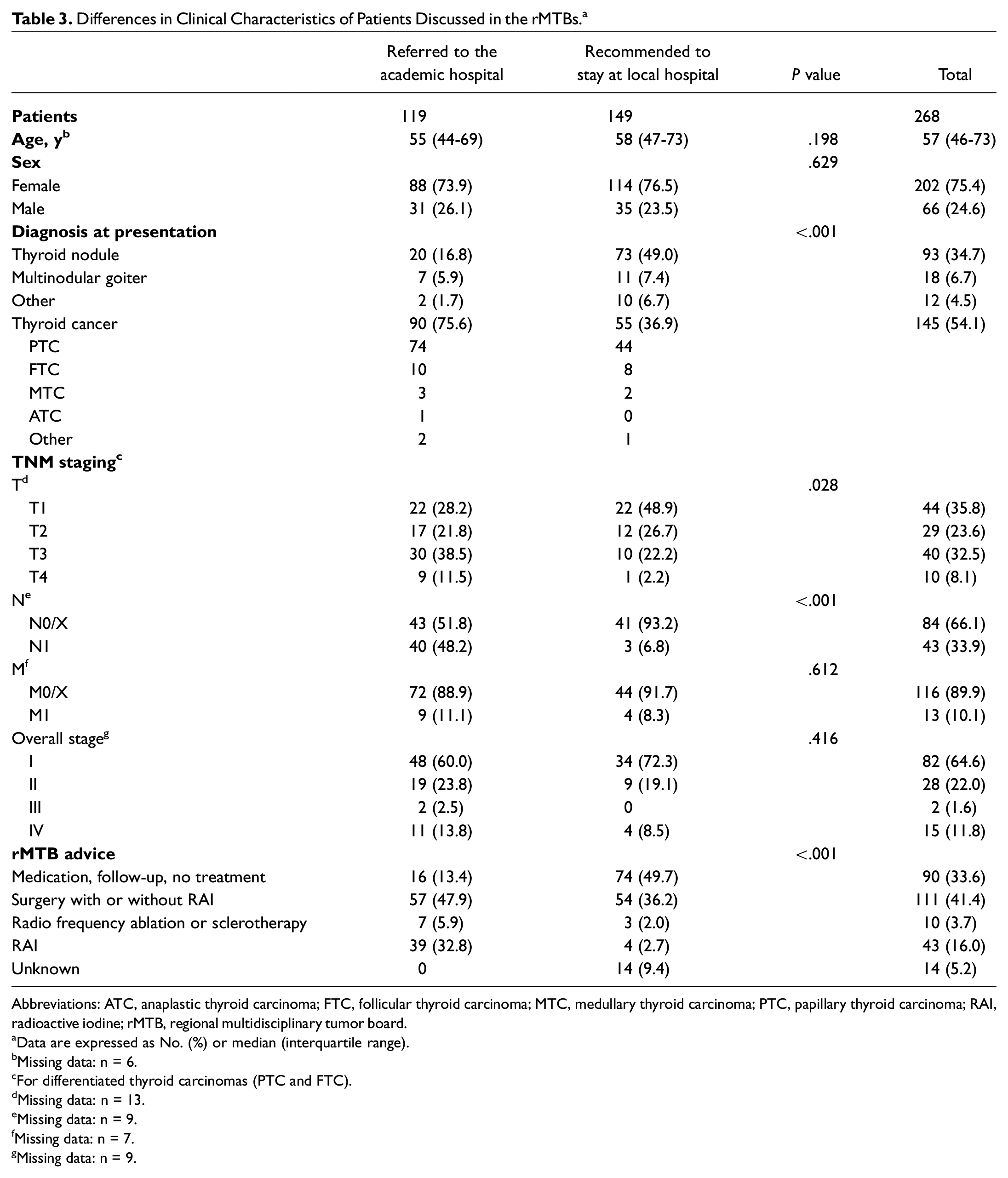
Abbreviations: ATC, anaplastic thyroid carcinoma; FTC, follicular thyroid carcinoma; MTC, medullary thyroid carcinoma; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; rMTB, regional multidisciplinary tumor board.
Data are expressed as No. (%) or median (interquartile range).
Missing data: n = 6.
For differentiated thyroid carcinomas (PTC and FTC).
Missing data: n = 13.
Missing data: n = 9.
Missing data: n = 7.
Missing data: n = 9.
Patient Flow in the 3 Periods
The academic hospital was involved in 20% more patient treatment decisions after the implementation of the regional MTBs (n = 346, pre-rMTB; n = 426, early-rMTB; n = 406, cont-rMTB). Meanwhile, the number of patients seen in the outpatient clinic remained stable (n = 342, pre-rMTB; n = 316, early-rMTB; n = 332, cont-rMTB). The total number of referrals from the hospitals within the Thyroid Network also remained stable after the initiation of the regional MTB (n = 108, pre-rMTB; n = 108, early-rMTB; n = 106, cont-rMTB; Figure 3 ).
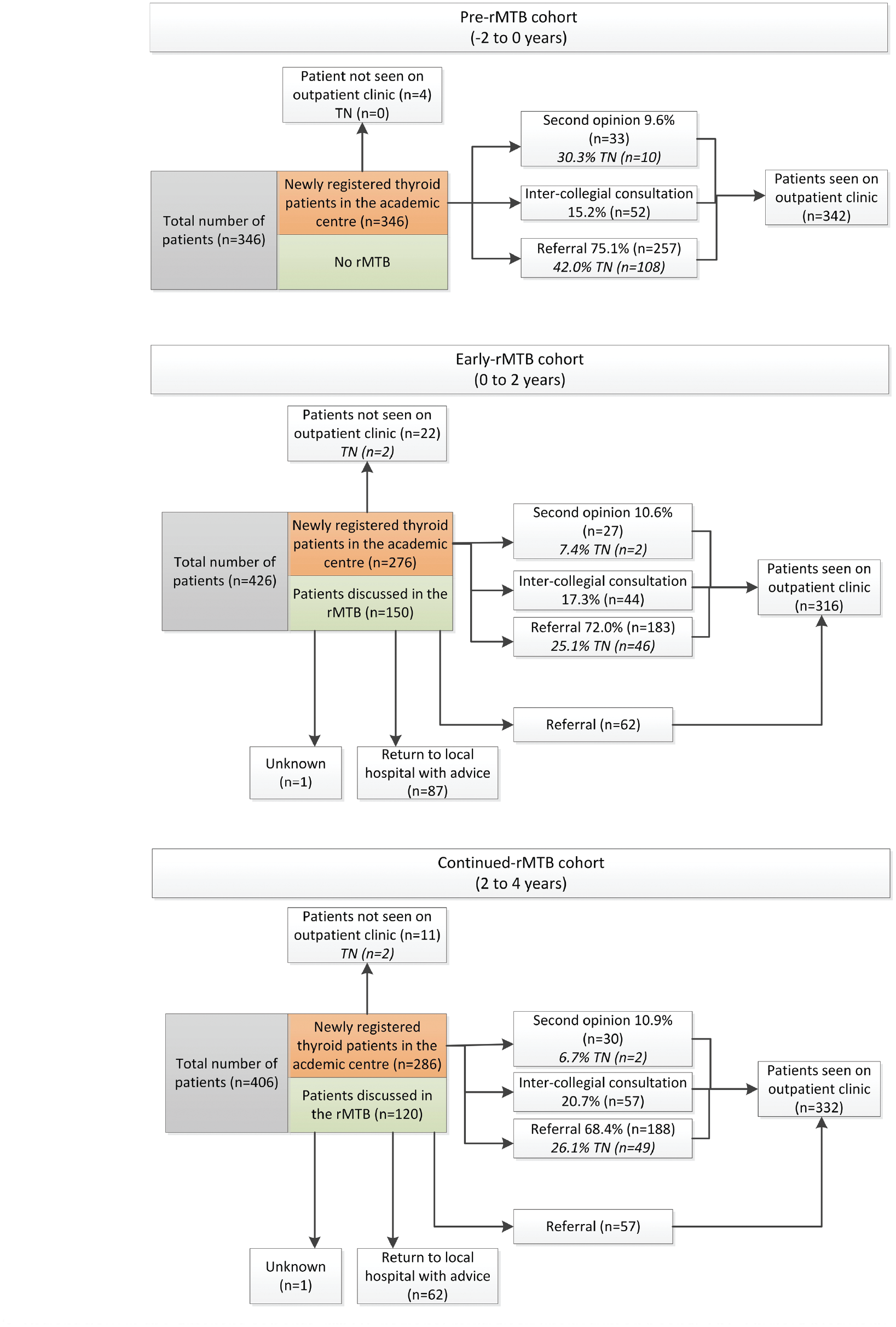
Patient flow in the different cohorts. rMTB, regional multidisciplinary tumor board; TN, Thyroid Network.
Interviews
The BeterKeten Foundation conducted a qualitative interview study with 24 stakeholders, 24 including 4 board members of the Thyroid Network and 18 specialists from other regional networks of BeterKeten. The other regional networks each had their own regional MTB. The 4 board members of the Thyroid Network were from different hospitals and 2 specialties, surgery and endocrinology. A description of the selected participants is shown in Additional File 4 (available online).
Context Factors and Mechanisms
All respondents (24/24) acknowledged that by participating in a regional MTB, they learn from peers and enhance their knowledge and expertise. Written regional MTB evaluation shows that the majority of the respondents (22/24) found it desirable and/or interesting to join the regional MTB, even without presenting a case study of their own. One board member stated that the fact that the consulting academic hospital does not receive any compensation for patients who are discussed in the regional MTBs could be a restraining factor in the continuation of a regional network collaboration such as the Thyroid Network.
Outcomes and Values
The interview data showed that all 4 board members concordantly acknowledge and appreciate the added value in the cooperation within the Thyroid Network. The uniform care pathway for referral and treatment of patients and the associated biweekly structured joint regional MTB were indicated by all board members as being most important for a successful collaboration.
The most important aspect of BeterKeten is that I am learning from others; I am expanding my knowledge as well as my professional network. (respondent 8)
Another respondent emphasized the benefit of the regional MTB when it comes to saving travel time and providing a full professional opinion.
When a patient living outside the region of Rotterdam says to me, “Doctor, I would like to be referred to the Erasmus MC,” I can answer, “I will provide even more: the university hospital and 9 other hospitals.” The patient does not have to travel to Rotterdam, because his case is discussed in the regional MTB and the patient is provided with a professional opinion supported by 10 different hospitals. Thus, care is provided close to home and it saves the patient a ride to Rotterdam and back. (respondent 9)
Discussion
Summary
This prospective study evaluates the impact of a multicenter network on referral patterns within 10 hospitals in the southwestern region of the Netherlands. There were fewer second opinions from the hospitals within the Thyroid Network after the start of the regional MTBs while maintaining a stable amount of referrals for tertiary care. In addition, the academic hospital was involved in 20% more patient cases than before the start of the collaboration. The Thyroid Network can be indicated as a “professional learning network” in which the learning capacity is large and effective due to the continuity of the biweekly regional MTB.
Interpretation
Collaborating networks such as the Thyroid Network often grow organically, 25 leaving no opportunity to observe and analyze improvements in, for example, quality of care, hospitalization costs, referral patterns, or quality of life. By prospectively registering all newly referred patients with thyroid nodules and cancer, we were able to analyze and evaluate how the interventions influenced referral patterns in 1 of the largest academic hospitals in the Netherlands concerning thyroid care.
The implementation of the structured regional care pathway was intended to decrease regional practice variation and standardize referral patterns, thereby reducing second opinions. This is in line with the 2014 British Thyroid Association guideline on thyroid cancer, 4 which recommends that hospitals providing secondary care for thyroid cancer should develop well-defined and streamlined pathways of referral and care for general practitioners. Several cancer guidelines for malignancies other than thyroid cancer recommend the initiation of regional MTBs to ensure that all relevant disciplines are involved, provide relevant educational opportunities for medical specialists, and reduce practice variation and individual physician biases.26,27 In addition, the initiation of a structured care pathway and regional MTB is in line with the Dutch government promoting care close to the patient, where different health care providers cooperate and digital channels are increasingly used.
By conducting an online regional MTB, all patients with thyroid nodules/cancer in the southwestern region of the Netherlands, regardless of the hospital in which the diagnosis is made, are offered the same optimal treatment. The regional MTB made it possible for general hospitals to instantly discuss and review patients, instead of referring them for second opinions. This leads to a more efficient and structured way of decision making and selective referral of patients necessitating academic expertise. This is reflected by the relatively lower number of patients needing to attend the outpatient clinic of the academic hospital. Patients do not have to travel for a second opinion, and due to the high number of participating hospitals in the regional MTB, patients are provided with a widely supported professional opinion. This is in accordance with a study from the United States on the implementation of online regional MTBs and the reduced burden of travel needs for patients with hepatocellular carcinoma. 28
Second opinions and referrals from hospitals outside the region doubled after the implementation of the Thyroid Network and the 2 interventions. Presumably, the structured collaborative approach implemented by the Thyroid Network is considered best practice by these hospitals, which could be a reason for the increase in second opinions and referrals. Literature shows that interhospital collaboration facilitates the accessibility of hospitals with higher quality of care, resulting in improved outcomes for individual patients as well as for regional health care systems.29,30 In addition, organizational centrality in a collaborating referral network is associated with fewer readmissions and lower hospitalization cost.31-33 This substantiates the assumption that an interhospital collaboration such as the Thyroid Network is the preferred approach in patients with thyroid nodules and cancer.
All board members of the Thyroid Network emphasized that the uniformly structured care pathway among general practitioners, general hospitals, and the academic hospital is a key ingredient for a successful interhospital collaboration of physicians concerning thyroid care. The close cooperation within the Thyroid Network ensures mutual trust to learn from one another and to share knowledge in formal as well as informal settings. Therefore, the Thyroid Network can be indicated as a “professional learning network.”
There is one major negative consequence following the establishment of the Thyroid Network. In the Netherlands, costs concerning local MTBs can be charged by all hospitals. However, hospitals attending regional MTBs can claim their expenses only if they are the primary care provider for the discussed patient. Currently, the consulting academic hospital does not receive any compensation for patients who are discussed in the regional MTBs. All costs concerning regional MTB patients (eg, pathologic specimen revisions) are covered from the academic hospitals’ own resources. To create a sustainable, structured implementation of regional MTBs in the Netherlands, a regional MTB should come with financial compensation.
Limitations
We were unable to assess changes in quality of care since we did not implement quality assessment tools yet. To assess the effect on quality of care after initiation of the Thyroid Network, qualitative analysis should be performed regarding treatment strategies, quality of life, and treatment complications before and after the initiation of the Thyroid Network. The interview study did not include any patients. This study was conducted within the Netherland’s health care system; therefore, the results and implementation barriers may not extrapolate to other systems. Occasionally, there was insufficient documentation of patients who were discussed in the regional MTB. Although the number of unregistered patients is estimated to be low, the exact incidence is unknown and could not retrospectively be determined.
Conclusions
The interhospital collaboration of 10 hospitals in the southwestern region of the Netherlands and the initiation of the regional MTB have resulted in a decrease in second opinions from the Thyroid Network hospitals to the academic hospital while maintaining referrals for tertiary care. The regional MTB led to a 20% increase in patient cases wherein the academic hospital was involved. The concept of the Thyroid Network could spread to other regions as well as to other specialties in health care. The next step would be to integrate primary health care within the Thyroid Network and to assess the effect of the Thyroid Network on quality of care and patient satisfaction.
Supplemental Material
sj-docx-1-oto-10.1177_01945998221086203 – Supplemental material for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns
Supplemental material, sj-docx-1-oto-10.1177_01945998221086203 for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns by Sam P.J. van Dijk, Ivona Lončar, Elizabeth van Veen-Berkx, W. Edward Visser, Robin P. Peeters, Charlotte van Noord, Elske T. Massolt, Manuel Castro Cabezas, Marlise Schouten, Erik M. von Meyenfeldt and Tessa M. van Ginhoven in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-2-oto-10.1177_01945998221086203 – Supplemental material for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns
Supplemental material, sj-docx-2-oto-10.1177_01945998221086203 for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns by Sam P.J. van Dijk, Ivona Lončar, Elizabeth van Veen-Berkx, W. Edward Visser, Robin P. Peeters, Charlotte van Noord, Elske T. Massolt, Manuel Castro Cabezas, Marlise Schouten, Erik M. von Meyenfeldt and Tessa M. van Ginhoven in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-3-oto-10.1177_01945998221086203 – Supplemental material for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns
Supplemental material, sj-docx-3-oto-10.1177_01945998221086203 for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns by Sam P.J. van Dijk, Ivona Lončar, Elizabeth van Veen-Berkx, W. Edward Visser, Robin P. Peeters, Charlotte van Noord, Elske T. Massolt, Manuel Castro Cabezas, Marlise Schouten, Erik M. von Meyenfeldt and Tessa M. van Ginhoven in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-4-oto-10.1177_01945998221086203 – Supplemental material for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns
Supplemental material, sj-docx-4-oto-10.1177_01945998221086203 for Establishing a Multicenter Network for Patients With Thyroid Nodules and Cancer: Effects on Referral Patterns by Sam P.J. van Dijk, Ivona Lončar, Elizabeth van Veen-Berkx, W. Edward Visser, Robin P. Peeters, Charlotte van Noord, Elske T. Massolt, Manuel Castro Cabezas, Marlise Schouten, Erik M. von Meyenfeldt and Tessa M. van Ginhoven in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
We thank Dr Ir S.G. Elkhuizen for her assistance in the statistical analyses. The Thyroid Network consists of the following hospitals (as of January 2021): Admiraal de Ruyter Hospital, Albert Schweitzer Hospital, Erasmus Medical Center, Franciscus Gasthuis & Vlietland Hospital, Het Van Weel-Bethesda Hospital, Ikazia Hospital, Ijsselland Hospital, Maasstad Hospital, Oogziekenhuis Rotterdam, Reinier de Graaf Groep, Spijkenisse Medical Centre, and ZorgSaam Hospital.
This article was presented at the Research and Science Symposium of the Thyroid Network; November 4, 2021.
Author Contributions
Disclosures
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.