
Abstract
Objective
To evaluate how the coronavirus disease 2019 (COVID-19) pandemic has affected tympanostomy tube placement and practice patterns.
Study Design
A retrospective review of billing data.
Setting
A large-volume practice with both community and tertiary care providers.
Methods
As part of a quality initiative, billing data were queried to identify children <18 years of age who underwent tympanostomy tube placement between January 2019 and December 2020. Patient age, practice location, and case numbers were gathered.
Results
The study included data from 2652 patients. Prior to state-mandated clinic and operating room restrictions, there were no significant differences in the number of tympanostomy tubes placed (P = .64), including month-to-month comparisons, the distribution of patients being cared for at community vs tertiary care sites (P = .63), or patient age at the time of surgery (P = .97) between 2019 and 2020. After resumption of outpatient clinical and elective surgical activities, the number of tympanostomy tubes placed decreased significantly between 2019 and 2020 (831 vs 303 cases, P = .003), with a persistent month-to-month difference. In addition, patients undergoing tube placement were older (4.5 vs 3.2 years, P < .001). The distribution of cases performed in the community setting decreased during this time period as well (P < .001).
Conclusion
During the COVID-19 pandemic, the rate of pediatric tympanostomy tube placement has significantly decreased. The age of patients undergoing surgery has increased, and more children are being cared for in a tertiary setting. These findings may reflect changes in the prevalence of acute and chronic otitis media as the result of the pandemic.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the novel coronavirus responsible for coronavirus disease 2019 (COVID-19), first emerged in late 2019 and spread around the globe quickly, with the World Health Organization (WHO) declaring a pandemic by March 11, 2020. 1 By mid-March, the Centers for Medicare & Medicaid Services had recommended deferring elective, preventative, and nonemergent medial services for patients of all ages, and the US Centers for Disease Control and Prevention also advised that elective surgical procedures and elective ambulatory visits be deferred to preserve health care resources and increase capacity. 2 In response to these recommendations, at our institution, nonemergent outpatient clinic activities were suspended after March 13, 2020, as were nonurgent, elective surgeries.
Myringotomy with tube placement (MT) is the most common ambulatory surgical procedure performed on children in the United States each year, with approximately 7% of children undergoing MT before the age of 3 years 3 and up to 20% of children with tubes requiring placement of a second set. 4 However, except in cases of suppurative complications, management of otitis media does not typically warrant urgent tympanostomy tube placement. Due to restrictions on performance of elective surgical procedures during the early months of the pandemic, an emphasis was placed on medical management and modification of behaviors and exposures to reduce the risk of otitis media 5 in cases that would typically be managed with elective tympanostomy tube placement.
After incrementally resuming nonurgent clinical operations June 1, 2020, based on statewide Health and Human Services guidelines, we observed a persistent decrease in the number of children presenting to the operating room for MT. This study was conducted as part of a quality improvement initiative using billing data to better understand and quantify this observation; our study does not evaluate underlying diagnoses or indication for surgery.
Methods
This study was completed as part of a quality initiative. Billing data from January 1, 2019, to December 13, 2020, for our department, which includes both tertiary care as well as community practices, were queried to identify children who underwent MT (Current Procedural Terminology code 69436). For each patient, the date of service, age at the time of service, and practice setting were recorded. We then examined the number of MT cases performed before pandemic-related restrictions on clinical operations (January 1 to March 13, 2020) and after reopening (June 1 to December 13, 2020) and compared this to the same time periods in 2019. Month-to-month comparisons were made to control for seasonal fluctuation in the number of MT cases performed. Practice setting and patient age were also compared during these periods. Comparisons were made using χ2 analysis for categorical variables and counts and 2-tailed t test for comparison of means of continuous variables. Statistical significance was considered when P≤ .05. Statistical analysis was performed using SAS University Edition software (SAS Institute). Data were analyzed between January 26 and January 27, 2021. The study was reviewed by and received an exemption from the Mass General Brigham Institutional Review Board.
Results
Between January 1 and December 13, a total of 1795 MT procedures were performed in 2019, compared to 838 in 2020 across 10 sites (2 tertiary, 8 community) by 29 providers. From January 1 to March 13, there was no significant difference in the number of procedures performed between 2019 and 2020 (482 and 514, respectively, P = .64). Prior to pandemic-related closures, month-by-month comparisons between 2019 and 2020 did not differ for January, February, or March (P = .92, .25, and .44, respectively). From June 1 to December 13, between 2019 and 2020, there was a significant decrease in the number of MT procedures performed (831 and 303, respectively, P = .003). This difference was significant for each month after resuming nonurgent care (P < .001 for each month evaluated) ( Figure 1 ).
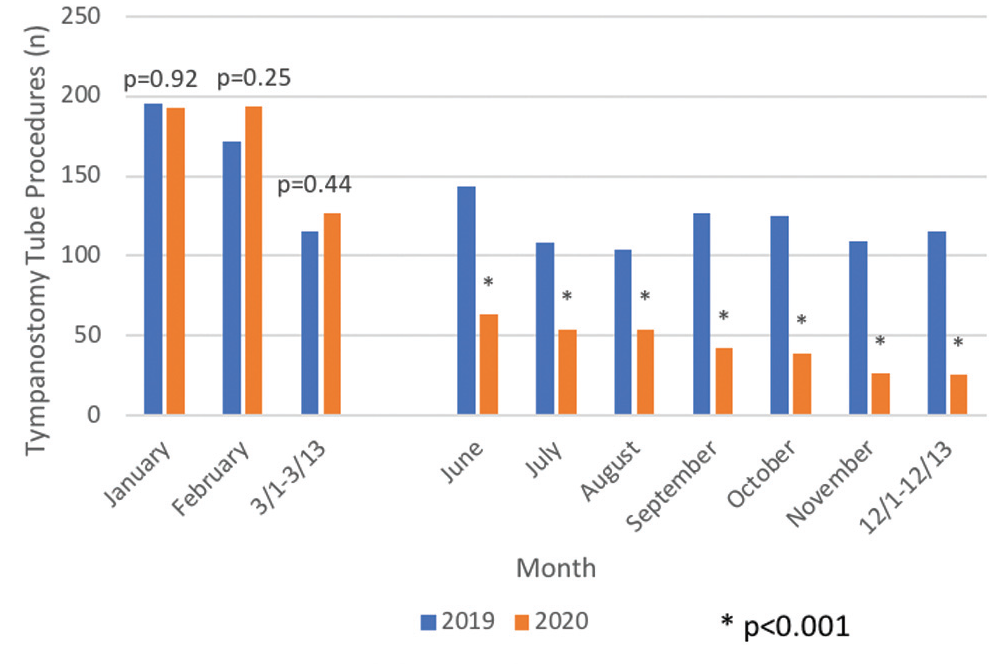
Pre- and post-COVID-19 pandemic surgical procedures.
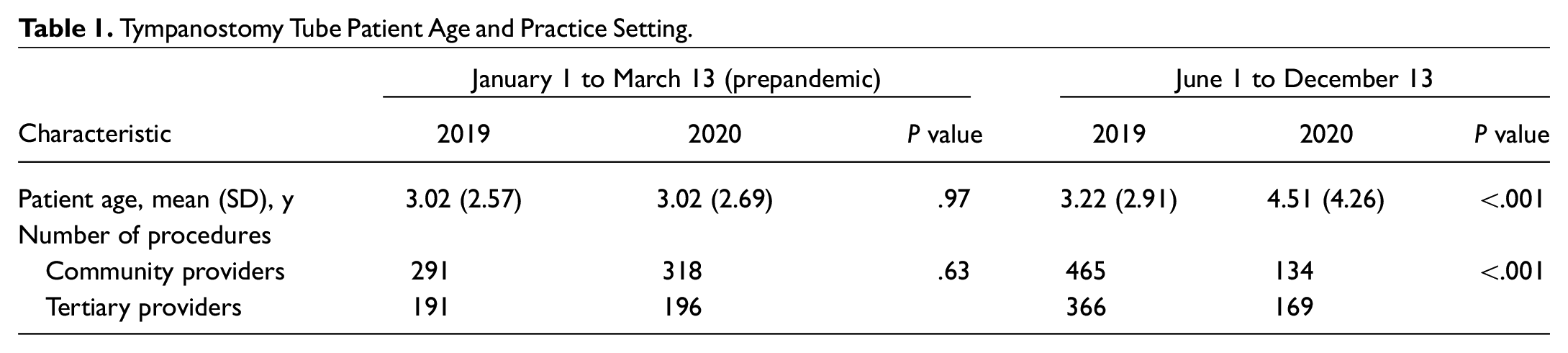
Prior to COVID-19, the proportion of MT cases being performed by surgeons practicing in the community did not differ between 2019 and 2020 (60.4% and 61.9%, respectively, P = .63). However, after reopening, the proportion of cases being performed by surgeons practicing in a tertiary setting increased (55.8% from 44.0%) and in a community setting decreased (44.2% from 56%) between 2019 and 2020; this difference was significant (P < .001) (see Table 1 ). Evaluating data from both 2019 and 2020, community providers performed procedures in significantly younger children than tertiary providers (mean [SD], 2.8 [2.6] vs 3.7 [3.5] years, P<.001). After reopening, across practice settings, an increase in mean (SD) age at MT emerged (4.51 [4.26] vs 3.2 [2.91] years, P < .001) ( Table 1 ). This age increase was observed at both community and tertiary care locations (mean [SD], 2.9 [2.59] to 3.49 [3.06] years, P = .03, at community locations and 3.7 [3.22] to 5.3 [4.87] years, P < .001, at tertiary locations, respectively).
Tympanostomy Tube Patient Age and Practice Setting.
Discussion
This study demonstrates that despite the resumption of clinical activities and operating room access for nonurgent care, the number of children undergoing MT procedures remains dramatically decreased both overall and in month-to-month comparison to the previous year. We also observed a significant change in the setting where these children are being cared for, with a shift to tertiary care over community practice settings. Finally, we observed a significant increase in the age of children undergoing tympanostomy tube insertion. While certainly patient hesitation to seek evaluation and treatment during a pandemic may contribute to the decrease in frequency of tube placement, a change in the rates of acute otitis media (AOM) and symptoms associated with chronic otitis are likely to be major factors contributing to these differences as well.
As a result of the pandemic and rising case numbers, by March 18, 2020, national school closures were implemented in over 107 countries affecting over 862 million children around the world, 6 including many in the United States. The school and daycare closures and restrictions imposed to reduce the spread of SARS-CoV-2 may have had an impact on the spread of other infectious diseases in the community as well. The bacterial pathogens most commonly responsible for AOM (Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis) are more likely to be present in children with symptomatic and asymptomatic viral infections. 7 Heikkinen et al 8 identified a specific viral cause of AOM in 41% of cases among 456 children, demonstrating that viral upper respiratory infections represent an important pathophysiologic precursor to AOM as well. Decreased peer contact at school and social gathering, along with increased hygiene practices to reduce the spread of respiratory viruses, likely has affected the incidence of AOM among pediatric patients.
Data about rates of acute and chronic otitis media requiring tympanostomy tube placement are lacking during the COVID-19 era, but recent studies have suggested that during the pandemic, otitis-related complaints and diagnoses of AOM have decreased. In 2020, Torretta et al 9 published a study of 102 Italian children with frequent otitis and found that during lockdown, 82.3% of them demonstrated improvement, with statistically significant decreases in the incidence of AOM, otorrhea, and antibiotic use compared to the same time period in 2019. Of the children with chronic otitis who were examined during the study period, 89.3% demonstrated normal middle ear findings.
In June 2020, McBride et al 10 published a study evaluating AOM diagnoses in Dane County, Wisconsin, in the COVID-19 era. The incidence of AOM was calculated during months of school closure in 2020 and compared to the same time annually since 2015; researchers found a significant reduction in AOM in 2020 (relative risk, 0.6; P < .001). While eustachian tube immaturity is often cited as the dominant factor in AOM in infants, the current findings and existing literature support the concept that antecedent upper respiratory infections may represent the principal risk factor.
In our geographic area, rates of return to in-person learning during the pandemic have varied greatly depending on the school district, a child’s age, local case positivity rate, and whether education is publicly or privately funded. Some schools resumed in-person learning in September 2020, even if through a hybrid model alternating in-person and remote learning, while others have remained entirely remote during the 2020 to 2021 school year. Despite some area schools reopening, we observed a persistent decrease in MT during the fall months. Further research is needed to better understand how the pandemic and associated mitigation strategies have affected rates of acute and chronic otitis media. Several factors, including decreased prevalence of otitis media, increased reliance on medical rather than surgical management for recurrent AOM and chronic otitis media with effusion, and reluctance on the part of patients and families to seek care for otitis media during the pandemic, either due to financial or health reasons, may all be contributing to the observed drop in rate of MT.
For our study, which was based on billing data, diagnosis codes were not examined. However, the observed increase in mean age of children undergoing tube insertion suggests a shift in indication for surgery from AOM, which is most prevalent in infants, toward otitis media with effusion, which tends to affect a broader age range. Further work is needed to assess the root cause of the observed age difference as well as shift in practice setting where patients are seeking care.
Conclusion
The rate of pediatric tympanostomy tube placement has significantly decreased during the COVID-19 pandemic. The age of patients undergoing surgery has increased, and more children are being cared for in a tertiary setting. These findings may reflect changes in the prevalence of acute and chronic otitis media as the result of the pandemic and associated changes in health care delivery, infection mitigation strategies, education, and social gathering.