
Abstract
Background:
Nursing Patient Classification Systems have been developed and utilized to classify patients based on their nursing needs in several countries. The literature suggests potential benefits of these systems in terms of outcomes.
Objective:
To map the literature that assesses outcomes in relation to the use of Nursing Patient Classification Systems in hospital settings and to describe them.
Methods:
A scoping review, based on the methodological framework developed by Arksey and O’Malley, was conducted in 2024. We searched electronic databases (CINAHL, Embase, PubMed, Scopus, and Web of Science), the OpenGrey database, and consulted stakeholders.
Results:
From a total of 964 abstracts initially identified, 4 studies were included in the review. Different Nursing Patient Classification Systems were used to classify only adult inpatients. Outcomes assessed were satisfaction, care areas identified, benefits to the patients, job attitude, and improvement in morale across different populations such as nurses, patients, and clinical partners. No studies assessed outcomes for caregivers, pediatric patients, or hospital organizations.
Conclusion:
The literature reports potential benefits related to the use of Nursing Patient Classification Systems and underlines the importance of exploring the relationship between their use and different types of outcomes. Despite this, the results highlight the limited research on this topic. To realize the potential of these systems, it is essential to understand their utility in advance. After implementation in daily practice, the evaluation of outcomes related to the use of these systems should become a standardized practice, contributing to both nursing science and quality improvement.
Keywords
Over the years, the healthcare system has undergone a significant transformation globally, shifting from a traditional disease-centered model to a patient-centered approach, together with the transition to hospitals for the intensity of care. 1 These kinds of hospitals aim to satisfy patients’ needs, by allocating them to the appropriate setting based on their intensity of care, as determined through a proper assessment.1,2
Patient Classification Systems and Outcomes
A common method to assess the patient is through Patient Classification Systems (PCSs). PCSs, whose creation started in the 1930s, 3 have been developed over time for multiple purposes and based on different concepts, acquiring right away a strategic role.4,5 PCSs were defined by Giovannetti as “the grouping of patients according to some observable or inferred properties or characteristics.” 4 (p4) Other authors also refer to these systems as “tools” or “instruments” without differentiating between the terms.6,7
In particular, in nursing, PCSs were defined as “the categorization of patients according to some assessment of their nursing care requirements over a specific period of time,” 4 (p4) and are generally called “Nursing Patient Classification Systems” (NPCSs), 4 although the 2 terms have often been used interchangeably. In this paper, we decided to use the term NPCS, even when the authors named it as “patient classification system,” “tool”, or “instrument.” NPCSs have been developed in response to the variable nature of nursing care demands. 4 NPCSs focus on patients and enable an accurate assessment of their care needs, resulting in proper categorization.3,8
In Brazil, the Federal Council of Nursing defined the utilization of NPCSs as critical for the success of any healthcare system, for patient safety, quality of care, and the optimization of human and material resources. 9 The Norwegian Parliament’s Coordination Reform of 2009, and a consequent project called “Better Resource Management,” gave the prompt for performing a broad evaluation of the patient through classification systems in healthcare.10,11 The utilization of data generated, 12 the assessment of the utility, and the performance of NPCSs have been considered fundamental in healthcare settings to demonstrate their effectiveness. 13 Some criticisms of NPCSs were underlined by Fasoli and Haddock, one of which is the need to identify nursing-sensitive performance indicators and outcomes. 14 In a healthcare setting, the assessment of outcomes becomes a central point in evaluating the impact of actions taken 15 on patients, healthcare providers, and the organizations. 16 This concept aligns with the continuous quality improvement approach, where the evaluation of outcomes related to implemented interventions is a mandatory and cyclical process to determine whether they have been effective in achieving the targeted objectives. 17
The literature suggests several potential benefits of using NPCSs in terms of the outcomes of care provided. 17 Fagerström and colleagues 18 suggested that using these systems in nursing could improve workforce planning, reduce staff costs, enhance the quality of care, increase nurse job satisfaction, decrease the amount of sick leave taken by nurses, and improve patient documentation.
Researchers have explored outcomes in relation to various aspects such as work environment, 19 care delivery models, 20 and nursing issues including skill mix,21,22 staffing level,23,24 costs, 25 education level, and quality of nursing care provided. 26 To our knowledge, however, the relationship between outcomes and the use of NPCSs has not been explored in the same way, despite what is suggested by the literature.17,18 In light of this, to bridge this gap, in 2024, we mapped the literature focusing on the outcomes assessed in relation to the use of NPCSs.
Purpose
This scoping review aimed to map the literature focusing on the outcomes assessed in relation to the use of NPCSs and to describe them.
Methods
Study Design
We decided to conduct a scoping review to answer our research questions because this type of review is useful for exploring emerging evidence, identifying knowledge gaps, and providing rigorous and transparent methods for mapping available evidence. 27 This scoping review followed the framework outlined by Arksey and O’Malley 27 and further refined by Levac et al, 28 which involves 6 steps: (1) identifying the research question; (2) identifying relevant studies; (3) study selection; (4) charting data; (5) collating, summarizing, and reporting the results; and a further optional sixth step concerning the consultation of stakeholders and the validation of the findings. Despite being indicated as the last step, Mak and Thomas 29 suggest that it can occur at different stages throughout the review.
This scoping review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 30
Stage 1: Identifying the Research Question
To ensure more comprehensive research and include all classification systems used in the nursing process meeting the inclusion criteria, we included both studies that defined NPCS and PCS, as these terms are often used interchangeably in the literature; in the same way, we also included them when defined as “tools” or “instruments.”
The research questions were as follows:
Is there literature assessing outcomes in relation to the use of NPCSs in hospital settings?
What outcomes are assessed in relation to the use of NPCSs in hospital settings?
The search strategy was structured according to the Population, Interventions and Outcome (PIO) framework, 31 where P = Inpatient, I = Nursing Patient Classification Systems, and O = Outcomes.
Stage 2: Identifying Relevant Studies
Based on our review questions, 5 databases were searched on June 13, 2024: CINAHL, Embase, PubMed, Scopus, and Web of Science. The search strategy was modified to fit each database with the support of a biomedical librarian (Table 1).
Search Strategies.
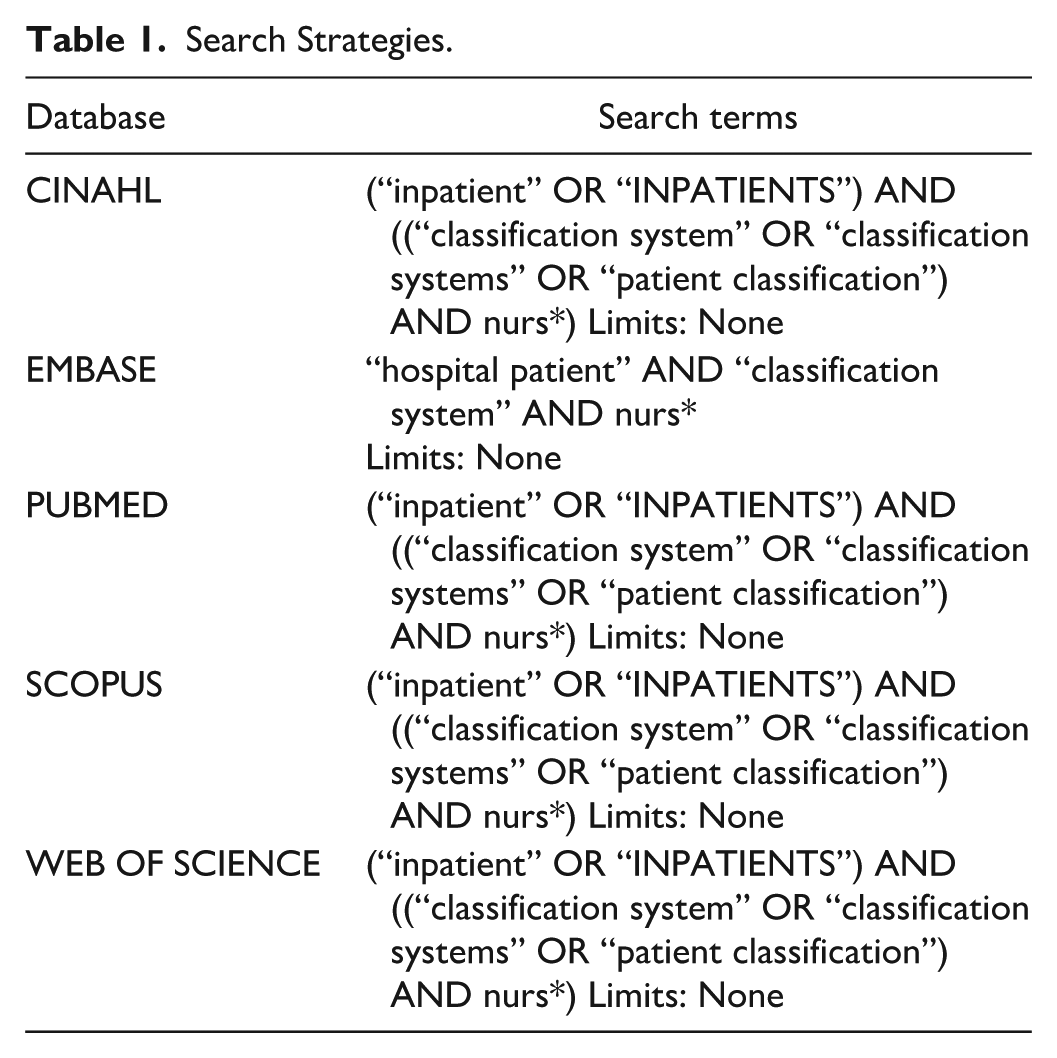
The initial search strategy was as comprehensive as possible to include the largest number of studies, which were then reduced on the basis of the inclusion and exclusion criteria. We also conducted a gray literature search using the OpenGrey database. To identify additional sources, the principal researcher (I.A.) contacted the authors known for important publications on NPCSs via email to gain further information pertinent to their studies and to obtain additional details on any potential studies, either published or ongoing, that were aligned with the research questions. All retrieved studies were managed using the reference management software Zotero, and duplicates were removed.
The study’s selection process included 2 phases:
An initial screening of titles and abstracts according to the inclusion and exclusion criteria was conducted. Two researchers (I.A. and R.D.R.D.M.) independently reviewed the studies. Studies were excluded if they did not meet all the inclusion criteria or if they met any of the exclusion criteria.
Full texts that were potentially eligible for inclusion were read and assessed independently by the same researchers (I.A. and R.D.R.D.M.). In case of disagreement, a third researcher was involved to reach an agreement. A member of the research team who is an expert in scoping reviews supervised the entire process (N.D.). The references of the included studies were checked to identify additional sources. The reasons for the exclusion of the full texts were recorded to track the decisions made. The methodological quality of the studies was not evaluated, as it was not essential for this kind of review, according to Arksey and O’Malley. 27
Stage 3: Study Selection
We decided to include studies meeting the following criteria: (1) having full-text paper available; (2) focusing on the use of NPCSs in hospital settings; (3) focusing on outcomes evaluation for inpatients, caregivers, healthcare providers, or organizations; (4) having at least one objective related to our research questions; and (5) written in English, French, Spanish, Portuguese, or Italian (languages known by the research team). We did not apply time limits for publication date. We also decided to include both primary and secondary studies, regardless of design or methodology, from commercial, academic, and gray literature. Gray literature was included if at least one author was declared.
We decided to exclude studies meeting the following criteria: (1) NPCSs used in settings other than hospitals, such as community dwelling, home care settings, or ambulatory care facilities; (2) focusing on the use of NPCSs to classify patients based on single health issue (such as pain), type of disease, or specific treatment; or (3) reporting only the development and validation of NPCSs. Since NPCSs do not focus on nursing staff but on patients, and aspects like nurse workload or staffing cannot be directly measured by such systems, as they are influenced by other variables unrelated to the patient, 3 we decided to exclude studies focusing exclusively on the use of NPCSs in relation to workload or staffing.
Stage 4: Charting the Data
A data charting form was developed according to the methodological framework followed. Before using the form, it was shared with the research team to discuss its potential effectiveness in relation to the review’s aims. Due to the limited number of studies retrieved, the form was not preliminarily tested by the researchers; however, any issues were addressed through an iterative process. Data charting was conducted independently by 2 researchers (I.A. and R.D.R.D.M.), who extracted and populated data from each study into the form: title, author/s and publication year, source (journal or other kind of source), country of origin, aim (only the relevant ones to address the research questions), research questions/hypotheses, study design/methodology, study procedures, year of data collection, setting, population/sample, sampling method and inclusion/exclusion criteria, population/sample characteristics, name of NPCS used to classify patients, strategies for bias management, data analysis, results, outcome assessed, declared limits, and conclusions.
Stage 5: Collating, Summarizing, and Reporting the Results
This stage was also conducted independently by the 2 researchers (I.A. and R.D.R.D.M.). This ensured a rigorous evaluation of the data, minimizing bias and enhancing the reliability of the conclusions drawn. A narrative synthesis of the data was conducted, which included descriptive characteristics; the studies retrieved were described with a special focus on the outcomes associated with the use of NPCSs and the subjects to whom their outcomes refer (e.g., inpatients, nurses).
Stage 6: Consulting Stakeholders
This stage was conducted at different moments during the scoping review process, as suggested by Mak and Thomas. 29 Since the aims of this scoping review were related to mapping the literature, we identified only authors as stakeholders. During the second stage, as stated, 7 authors were contacted by a researcher (I.A.) via email to determine whether further information pertinent to their studies was available or if studies addressing our research questions, and meeting the inclusion and exclusion criteria, to their knowledge, were ongoing or yet to be published. In particular, the authors were asked whether the impact of the NPCS they had published had been studied, especially in terms of health, care, clinical risk, quality, and organizational outcomes. None of the 5 authors who responded had studied this impact, but all acknowledged the importance of investigating this topic.
At the end of the scoping review, the research team sent an additional email to the same authors to share a synthesis of the preliminary results, to possibly obtain their feedback; determine if, in their opinion, the results can be representative; and foster a discussion on future research in this field. Two stakeholders responded to the email; one of them underlined the importance of this topic and the impact of using NPCSs. Another suggested that considering “indirect evidence” of outcomes could enrich the overview in this field.
Results
A total of 964 records were initially identified after searching the databases. No additional records were added following the search of gray literature and the contact with the authors in the second stage. Two hundred eighty-one records were removed as duplicates. After titles and abstracts were screened, 658 were eliminated. Two records did not lead to an available full text. Twenty-three papers underwent full-text review. Four papers were included after the 2 researchers (I.A. and R.D.R.D.M.) independently read the full texts. No additional records were added following the hand search of their references (Figure 1).
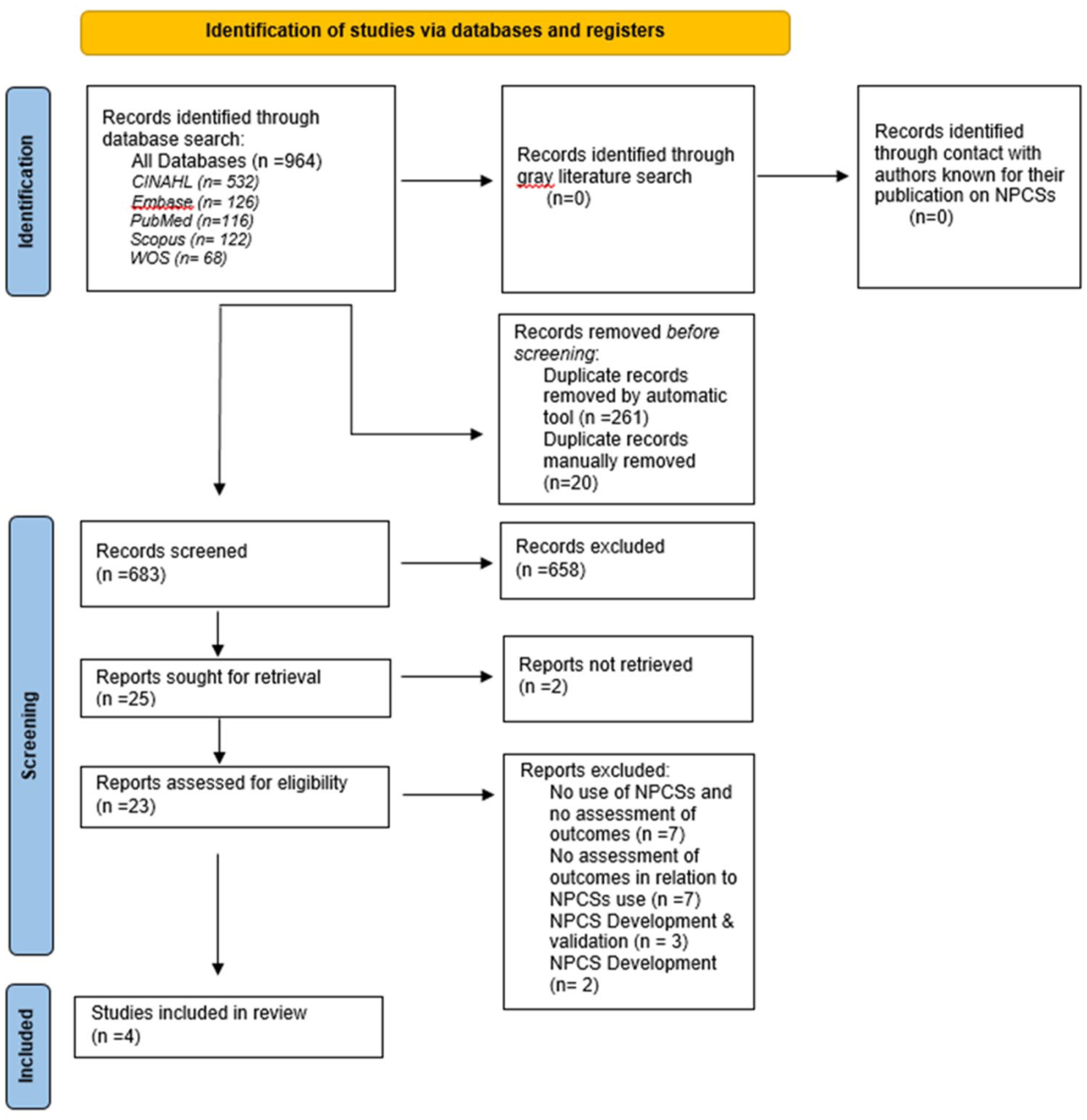
PRISMA flow diagram.
Characteristics of the Studies Included in the Review
The studies were conducted in Brazil (n = 2),6,32 Finland (n = 1), 33 and the United States (n = 1). 34 They involved different hospital units and were published between 1998 and 2015.6,32 -34 None were experimental studies. One was conducted as part of a quality improvement project. 34 No study focused on assessing outcomes for caregivers, the pediatric population, or at an organizational level. The population and outcomes assessed in the included studies are shown in Figure 2. The studies were based on the use of different NPCSs (Table 2). In only one hospital, the NPCS was already systematically used in daily practice, 33 while in another hospital, NPCSs use became standard practice for organizational reasons, followed by a research project. 34 In the other 2 articles, this issue was not clearly stated.6,32 In 3 out of 4 studies, the use of NPCSs was implemented after nursing and staff education,33,34 or nurses were already aware of it. 32 In all the included studies, NPCSs were used to classify only adult patients during their hospital stay. No homogeneity was found regarding the timing of the patient classification. In the study conducted by Fagerström and colleagues, 33 the patient’s classification occurred during the afternoon shift, concerning the previous 24 hours. In the study conducted by Perroca, 6 it was not clearly stated when the patient classification was performed during the nurses’ shift. Pagliarini and Perroca 32 utilized the NPCSs at the time of hospital discharge planning, while in the study conducted by Thomasos and colleagues, 34 the patients were assessed upon admission to the ward and whenever there was a significant change in their condition. The main characteristics of the included studies are synthesized in Table 3.
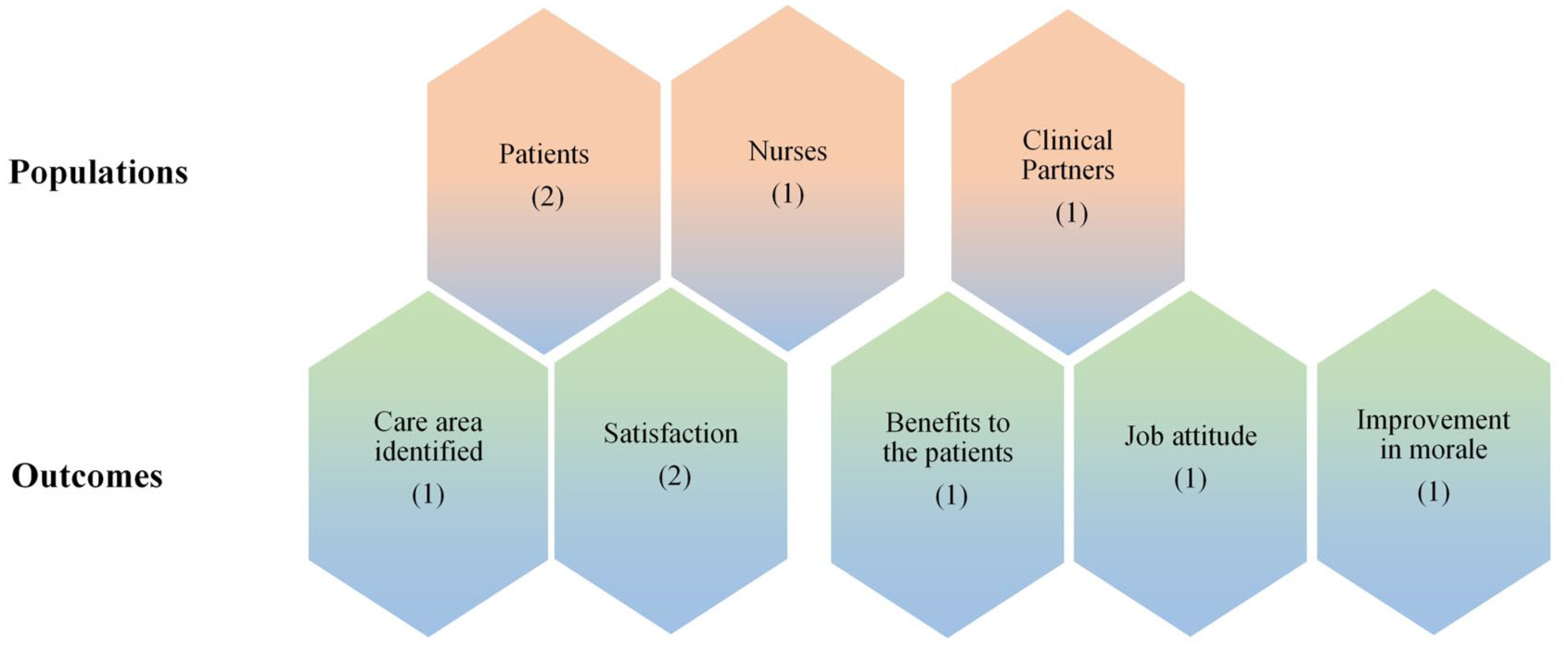
Populations and outcomes in the included studies.
Description of NPCS Used.
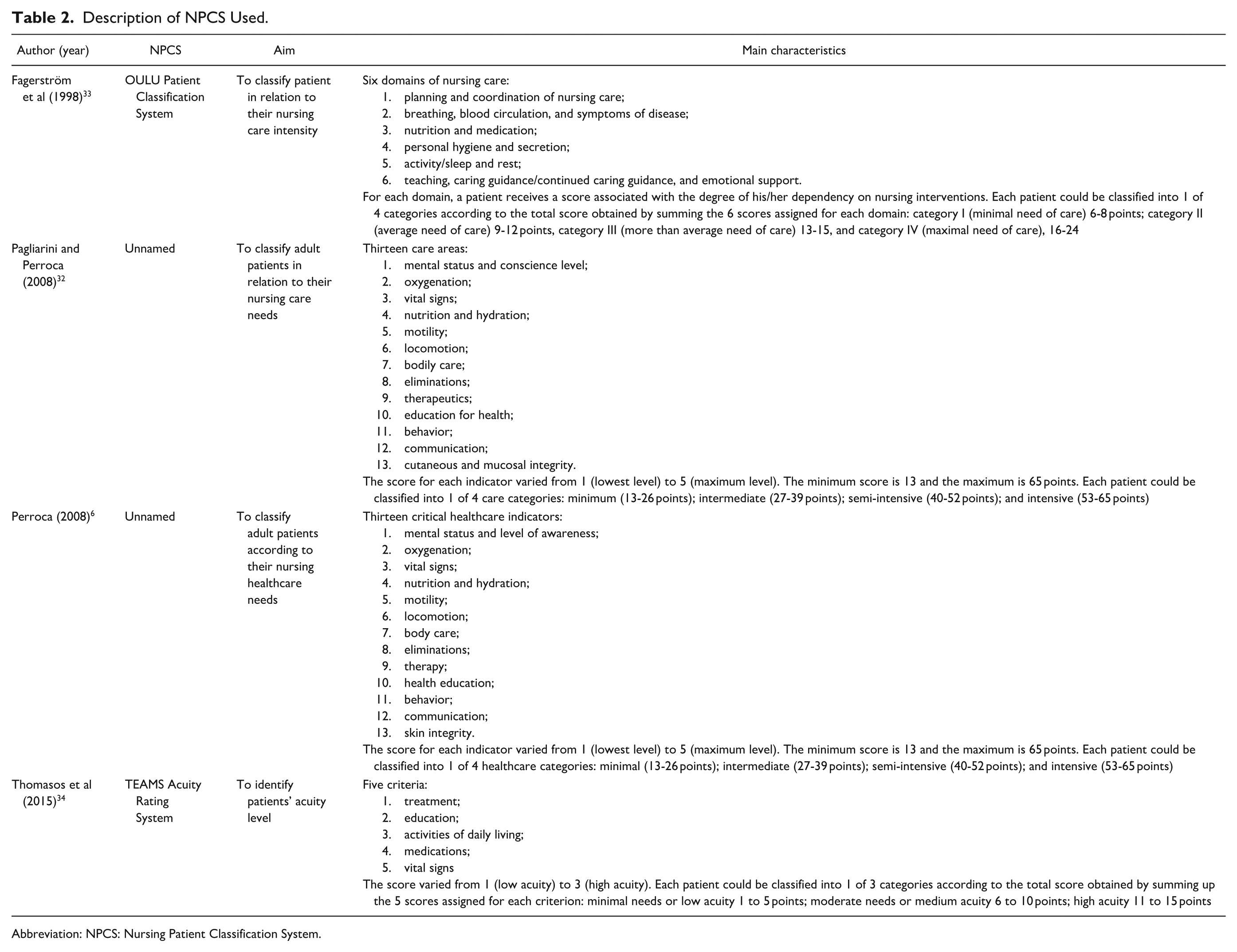
Abbreviation: NPCS: Nursing Patient Classification System.
Summary and Main Characteristics of Included Studies.
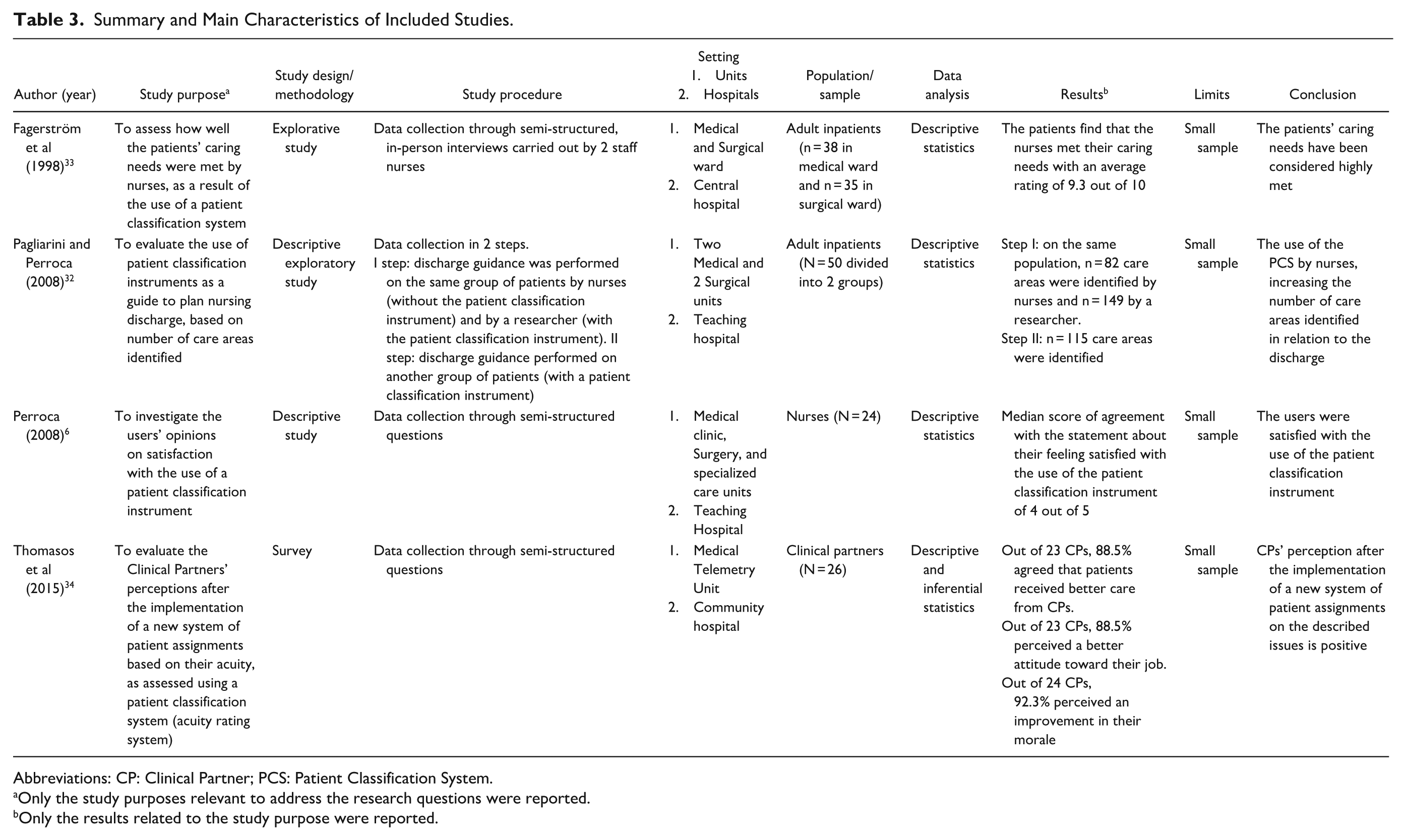
Abbreviations: CP: Clinical Partner; PCS: Patient Classification System.
Only the study purposes relevant to address the research questions were reported.
Only the results related to the study purpose were reported.
Outcomes Assessed in Relation to Use NPCSs
Inpatient outcomes
Care areas identified
The descriptive, exploratory study conducted by Pagliarini and Perroca 32 evaluated the impact of the application, either by a researcher or by a nurse, of an NPCS during the discharge process on the number of care areas identified in relation to discharge. The use of an NPCS increased the number of care areas identified on the same 25 patients during the first step of the study, from 82 identified by nurses (mean of 3.28 ± 1.2 per patient) to 149 identified by a researcher (mean of 5.96 ± 3 per patient). In a second step, on a different sample of 25 patients, the care areas identified by the nurse using the NPCS were 115 (mean of 4.6 ± 2.6 per patient). The use of the NPCS by nurses, increasing the number of care areas identified in relation to discharge, leads to more detailed discharge guidance, which could be seen as a strategy to improve quality.
Satisfaction
Fagerström and colleagues, 33 in their explorative study on a sample of patients (n = 73), assessed, among others, their experience of how well nurses met their caring needs, help, and support as a result of the use of an NPCS. The way patients perceive how well the nursing staff has addressed their caring needs should be considered a crucial aspect and component of care quality. Based on the study’s results, they found that the patients were highly satisfied with how the nurses addressed their caring needs (average rating of 9.3 on a scale ranging from 4 to 10).
Nurse Outcomes
Satisfaction
Only one study assessed outcomes related to nurses. 6 As 1 of the 2 aims of this descriptive study, the author evaluated the satisfaction of 22 nurses regarding the use of a new version of a validated system for patient classification, as a part of its acceptance. 6 The results, obtained from responses to a single question in a 14-statement questionnaire, showed a high level of agreement, with a median score of 4 out of 5 (IQR: 3-4) with the statement about their feeling satisfied with its use.
Clinical partners’ outcomes
One survey assessed outcomes related to Clinical Partners (CPs). 34 Thomasos and colleagues 34 described CPs as “unlicensed individuals who work with doctors, nurses, and other health care professionals to provide direct patient care in a variety of environments.”(p39) The outcomes assessed included CPs’ perceptions of benefits to the patients, and CPs’ job attitudes and morale, as part of an improvement project following complaints and dissatisfaction among CPs with the traditional system of assigning patients. The authors asked 26 CPs what their preference was between the traditional assignment system (by adjacent room numbers) versus a new one (by acuity on the basis of results of an NPCS). The authors assessed the CPs’ perception of the new assignment system by measuring their agreement on a 4-point Likert scale in relation to a list of 12 statements. The results showed a high level of agreement with the proposed statements in different areas.
Benefits to the patient
Most of the CPs (n = 23, 88.5%) agreed that since their assignments have been patient acuity-based, the patients have received better care from them.
Job attitude
The same percentage of CPs (88.5%) agreed that being assigned patients on the basis of their acuity had given them a better attitude about their job. In addition, the CPs’ rating of their preference for the new system of assigning patients was significantly correlated with a better job attitude.
Improvement in morale
Similarly, almost all CPs (n = 24, 92.3%) agreed that having patient assignment by acuity has improved the CPs’ morale in the unit, as it was perceived as a fair system compared to the patient allocation system previously used. The CPs’ rating on the statement about patients receiving better care with the new system of assigning patients was also significantly correlated with CPs’ morale improvement.
Discussion
To the best of our knowledge, this is the first scoping review aiming to map the literature focusing on outcomes assessed in relation to the use of NPCSs.
This scoping review arises from the need to introduce an NPCS into clinical care practice in a pediatric hospital, and to assess its impact on outcomes for inpatients, caregivers, healthcare providers, and hospital organizations, as suggested by the literature.12,13,17,18 Our aim was therefore to identify studies that provided results on the outcomes assessed in relation to the use of NPCSs, potentially to be used as a starting point for quality improvement strategies and as a guide for future research agendas.
Due to the scarcity of available literature, despite our extensive review, we could identify only a few outcomes assessed in relation to the use of NPCSs. This finding was unexpected, since the literature has evidenced the potential benefits of using these systems, which can provide a scientific basis (rational, systematic, objective, and evidence-based) for the quality of healthcare services and patient outcomes improvement.11,35
Nursing literature has discussed how to integrate nurses’ research study data into clinical practice 36 to ensure high-quality and safe care, demonstrate their fundamental role, and contribute to healthcare science and outcomes. The results of this review prompt further inquiry into why, despite the widespread adoption of NPCSs, so few studies evaluating outcomes related to their use have emerged from the literature, and why no recent studies have been published on this issue. The lack of studies meeting the inclusion criteria could be due to possible gaps in indexing, a lack of standardized outcome measures, or a lack of uniformity in terminology and the use of NPCSs. This result also prompts us to think over several points, such as how data obtained from the use of NPCSs are put into action, or whether their use is intended for purposes whose outcomes cannot be assessed considering the nature of NPCSs.
Since 2000, several authors have emphasized the importance of utilizing data obtained from these systems 13 and linking it to outcomes.12,37 In this regard, less than one-third of nurses, administrative staff, and personal staff in a 500-bed university teaching hospital stated that they do not use the information generated by NPCSs. 12 In literature, the importance of not reducing the use of NPCS to a mere bureaucratic activity was emphasized, highlighting the broader potential of such systems. 38 It was suggested that data obtained from the use of NPCSs should be utilized in nursing management, as, without this integration, the implementation of the system within the organization cannot be justified. 37 In addition, the importance of exploring the relationship between the information generated by using NPCSs and costs, quality, and care outcomes was suggested. 12 This exploration could be crucial to provide valid information for nurse administrators and to understand how different health professionals, in relation to their organizational roles, use the information generated by NPCSs. Such understanding could serve as a basis for defining strategies to increase the implementation of NPCSs and establish a predefined set of desired outcomes to be achieved. 12 An outcome database could be used to plan clinical research, staff training programs, and initiatives for quality improvement. 39 Furthermore, through the use of NPCSs, the nurse’s contribution to patient’s health can be made visible. Data could allow for a better understanding of nurses’ influence on patient outcomes and healthcare costs 11 and to assess the efficacy of new nursing care and staffing models. 39
Nevertheless, despite the widespread development and use of NPCSs by nurses, there is limited evidence linking their implementation to improvements, for example, in nursing outcomes. 14 As highlighted by our results, only a few outcomes were assessed and only for some populations. In particular, the outcomes assessed focused on adult patients and healthcare providers (satisfaction and perception of benefits), with none addressing outcomes on caregivers, pediatric population, and not even at the organizational level, although the literature reported the potential benefits of using NPCSs in terms of cost and resource optimization.11,18
Outcomes that have instead been particularly studied in relation to the use of NPCSs are workload and staffing.38,40 -42 This scoping review did not include these outcomes since this issue is questioned. Several authors, in fact, report that they cannot be directly assessed in relation to the NPCSs’ use, as they are influenced by other variables not related solely to the patient’s condition.3,39
Given the current gaps in evidence, future research should focus on multisite, longitudinal studies that include different populations and healthcare settings, taking into account health outcomes for patients, caregivers, and healthcare providers, as well as organizational and economic outcomes, such as cost-effectiveness, to fully capture the impact of NPCSs. Furthermore, applying an implementation science framework could provide valuable insights into how NPCSs are adopted and sustained within healthcare systems, helping to identify and overcome barriers to their effective use and enhancing the generalizability of findings.
The development of standardized outcome sets that can be related to NPCSs would foster consistency across studies; the establishment of comprehensive databases containing NPCS-related outcomes would further guide clinical research. These efforts would contribute to making the nursing role in patient care more visible, measurable, and actionable, informing staff training programs, facilitating evidence-based management decisions, and consequently supporting ongoing quality improvement.
Limitations
Several limitations of this review must be acknowledged. The small number of included studies limits the robustness of conclusions, and the heterogeneity of studies, outcomes assessed, and NPCSs usage patterns makes it difficult to synthesize the findings meaningfully. Certain groups (e.g., the pediatric population, caregivers, and organizations) were not represented in the findings, which undermines the validity of the results. Other limitations are that this review presents data that is not recent, and comes from studies with small sample sizes, along with the potential exclusion of studies published in languages not spoken by the authors, and lacks an evaluation of the quality of the evidence. For these reasons, these limitations should be considered when interpreting the results of this study. Continued research and development in this field are essential to optimize the use of NPCSs in order to achieve the benefits described in the literature. Robust long-term studies on the same population or populations not yet investigated could complete this mapping.
Conclusion
The map of literature provided by this scoping review suggests that outcomes have been scarcely assessed in relation to the use of NPCSs. If the impact that the use of NPCSs could have on the outcomes, for example, on patients, caregivers, healthcare providers, and organizations, is not demonstrated with objective data, it could be difficult to change practices or justify the implementation of such systems. To fully realize the potential of NPCSs, it is essential to understand their utility in advance; after their implementation in daily practice, the evaluation of outcomes related to NPCSs should become a standardized practice. The use of NPCSs and their derived data can play a strategic role not only in providing nursing care based on patient characteristics and their nursing care needs, but also in achieving the desired outcomes.
Footnotes
Author Contributions
All listed authors meet the authorship criteria, and all authors are in agreement with the content of the manuscript. I.A., R.D.R.D.M., N.D., C.R., G.O., S.C., G.M.N., S.R., and S.S. made a substantial contribution to the work submitted. I.A., R.D.R.D.M., N.D., and S.R. conceived the article. I.A. and R.D.R.D.M. drafted the article. I.A., R.D.R.D.M., N.D., C.R., G.O., S.C., G.M.N., S.R., and S.S. critically revised the article for important intellectual content. I.A., R.D.R.D.M., N.D., C.R., G.O., S.C., G.M.N., S.R., and S.S. reviewed and approved the article before submission. I.A., R.D.R.D.M., N.D., C.R., G.O., S.C., G.M.N., S.R., and S.S. are accountable for the work and its published form.
Data Availability Statement
The complete data extraction sheet is available upon request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Italian Ministry of Health (5x1000 project 2017 5M-2017-23684151).
Ethical Approval and Informed Consent
This was a review study. No primary data were collected from human participants for this work. Institutional review board/ethics committee review and informed consent were not required.