
Abstract
Background:
Unwanted workplace behaviors impact all organizations, but in the discipline of nursing, these behaviors impact both the welfare of nurses and the quality and safety of patient care. The terminology adopted to describe these behaviors varies widely, leading to confusion and inconsistency in research and practice.
Objectives:
This scoping review aims to explore the variability in the terminology used to describe unwanted workplace behaviors in nursing, identify the most commonly used terms, and analyze the implications of this variability for research, policy, and practice.
Methods:
The Population, Concept, and Context mnemonic was used to frame the review, as recommended by the Joanna Briggs Institute. A comprehensive literature search was conducted using relevant databases. Keywords used in the search included “moral harassment, nursing, definition, meaning, description,” “Shaming,” “Mobbing,” “Bullying,” “Vertical violence,” “Horizontal violence,” “Incivility,” “Microaggression,” “Lateral violence.” Boolean operators (AND, OR) were used to combine search terms appropriately.
Results:
The initial search yielded 299 references. Following full-text screening, 51 studies met the inclusion criteria and were included in the final review. The review revealed 13 different terms used to describe unwanted workplace behaviors.
Conclusion:
The review highlights a lack of consensus across the discipline. There is a call for a singular term to be applied across the field which would support policy implementation and practice.
The literature suggests that unwanted workplace behaviors in healthcare are common and directly impact recruitment, retention, and patient safety. 1 The shortages of healthcare personnel are felt globally, and in Australia, the baseline projections show an undersupply by the year 2035 of 70,707 FTE nurses. 2 Recent studies have demonstrated a significant correlation with unwanted workplace behaviors and turnover intention.3,4
Westbrook et al, 1 in their prevalence study of unwanted workplace behaviors, reported that 93.6% of nurses recounted experiencing at least 1 episode of unprofessional behavior in the past 12 months. Thirty-eight percent reported experiencing the behaviors from co-workers, weekly or more frequently. However, it is not only the paid workforce who are experiencing these behaviors. Student nurses, who participate in workplace learning, are particularly vulnerable to unwanted workplace behaviors, despite not being considered part of the permanent workforce. Although students are not officially in their “workplace,” the literature highlights that students frequently experience such behaviors. 5 Hallett et al 6 described that 81% of nursing students reported experiencing nonphysical aggression while on clinical placement.
When addressing this phenomenon, many authors in this field refer to the broader term of “workplace violence.” This term describes behaviors such as verbal and physical attacks and includes patients as perpetrators as well as victims.54-56 Violence against patients and violence between patients and healthcare providers was outside the scope of this review.
The main issue facing researchers in the field of unwanted workplace behavior is the variation in the terms used to describe it, complicating comparisons across disciplines and countries. 7 To address unwanted workplace behaviors and to support a sustainable nursing workforce, a consensus of terms is needed. The lack of consensus complicates efforts to clarify, measure, and address the phenomenon, 5 which exacerbates the situation, negatively affecting the psychological welfare of healthcare staff and students often leading to financial loss in terms of workers compensation, recruitment, and retention. 2
Terms such as bullying, abuse, vertical and horizontal violence, harassment, and incivility have been used interchangeably in scholarly literature.7,8 This inconsistency presents challenges for researchers striving to compare, contrast, and amalgamate findings in this field. Furthermore, this variability can impede the development of effective interventions and policies. Clear and consistent terminology is fundamental for policymaking and implementation, as variability can lead to gaps in protection and enforcement. In practice, nurses and healthcare managers may struggle to recognize and address unwanted behaviors without a shared understanding of terms.
Methods
As recommended by the Joanna Briggs Institute (JBI), the Population, Concept and Context (PCC) mnemonic was used to frame the review. 9 The population was defined as nurses and/or student nurses. Concept was defined as terminology used to describe unwanted workplace behaviors. The workplace, which included educational providers, was defined as the context. The PCC framework provided the foundation for the research question of “What terms are used to describe unwanted workplace behaviors in nursing?”
Search Strategy and Inclusion Criteria
A comprehensive literature search was conducted using 4 databases: OVID, CINAHL, Medline, and EBSCO Plus. As the phenomena first appeared in nursing literature in the 1980s with Meissner coining the phrase “nurses eat their young” in 1986, a date range of 1984-2024 was applied to the search. Search terms included “moral harassment,” “nursing,” definition, meaning, description, “shaming,” “mobbing,” “bullying,” “vertical violence,” “horizontal violence,” “incivility,” “microaggression,” and “lateral violence.” Boolean operators (AND, OR) were used to combine search terms appropriately. Articles were included in the search if they were published between January 1, 1984, and January 1, 2024, written in English, and they were original research articles. Studies were excluded if they did not relate to health, they were nonresearch papers, they did not include a definition, or they were published in a language other than English.
Screening Process
The literature selection process was managed using Covidence (Veritas Health Innovation, Melbourne, Australia), an online software platform designed to streamline the production of systematic reviews. There were 3 steps involved in the study selection process. The first step was to import all references identified from the database searches into Covidence, where duplicates were automatically removed. The next step was to screen titles and abstracts of the imported studies. Applying the inclusion and exclusion criteria, 2 independent reviewers screened the titles and abstracts of all imported references. Any discrepancies between reviewers were resolved through consultation with a third reviewer. The final step was to undertake a full-text review. Studies that met the inclusion criteria during the title and abstract screening were retrieved for full-text review. Full-text articles were independently assessed by the same reviewers to determine their eligibility. A third reviewer resolved any disagreements. The interrater reliability analysis produced a Cohen’s kappa value of 0.46, indicating a moderate agreement between raters.
Data Extraction and Analysis
A standardized data extraction form was developed and pilot-tested on a sample of included studies to ensure consistency and comprehensiveness. Data extracted from each study included the study characteristics (author, year, country), aim of the study, study design, type of participant, characteristics of terms used, and definitions. A textual narrative synthesis was used. The goal of a textual narrative synthesis is to provide a coherent summary of the findings while highlighting patterns, relationships, and variations across studies. 10
Results
The initial search produced 299 references which were imported into Covidence. After the removal of 95 duplicates, 204 references were screened based on titles and abstracts. Of these, 102 articles were retrieved for full-text review. Following the full-text screening, 51 studies met the inclusion criteria and were included in the final review (see Figure 1).
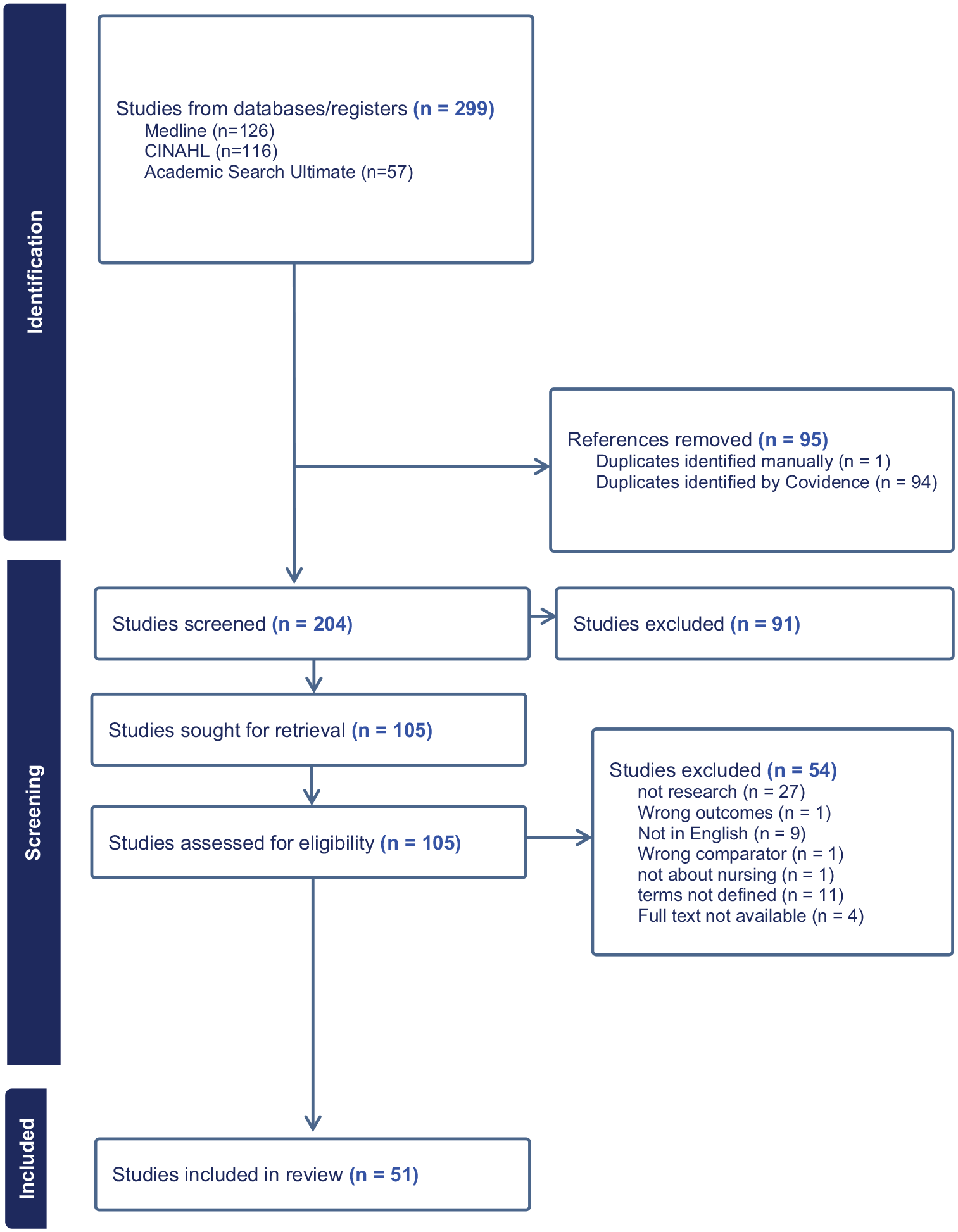
Study Screening Process.
Study Characteristics
The included studies varied in their design, target populations, and terminology used. The majority of the studies were conducted in the United States (n = 24), Canada (n = 4), Iran (n = 3), Korea (n = 3), Australia (n = 3), Turkey (n = 2), Brazil (n = 2), with one study each in South Africa, New Zealand, India, Italy, the United Kingdom, China, Lithuania, Norway, Sweden, and Switzerland. The types of studies were mainly qualitative in design such as descriptive and concept analysis. Quantitative designs were mainly cross-sectional studies. Of the articles that disclosed the target population, 30 studies recruited clinicians as participants and 6 focused on student nurses.
Terminology and Definitions
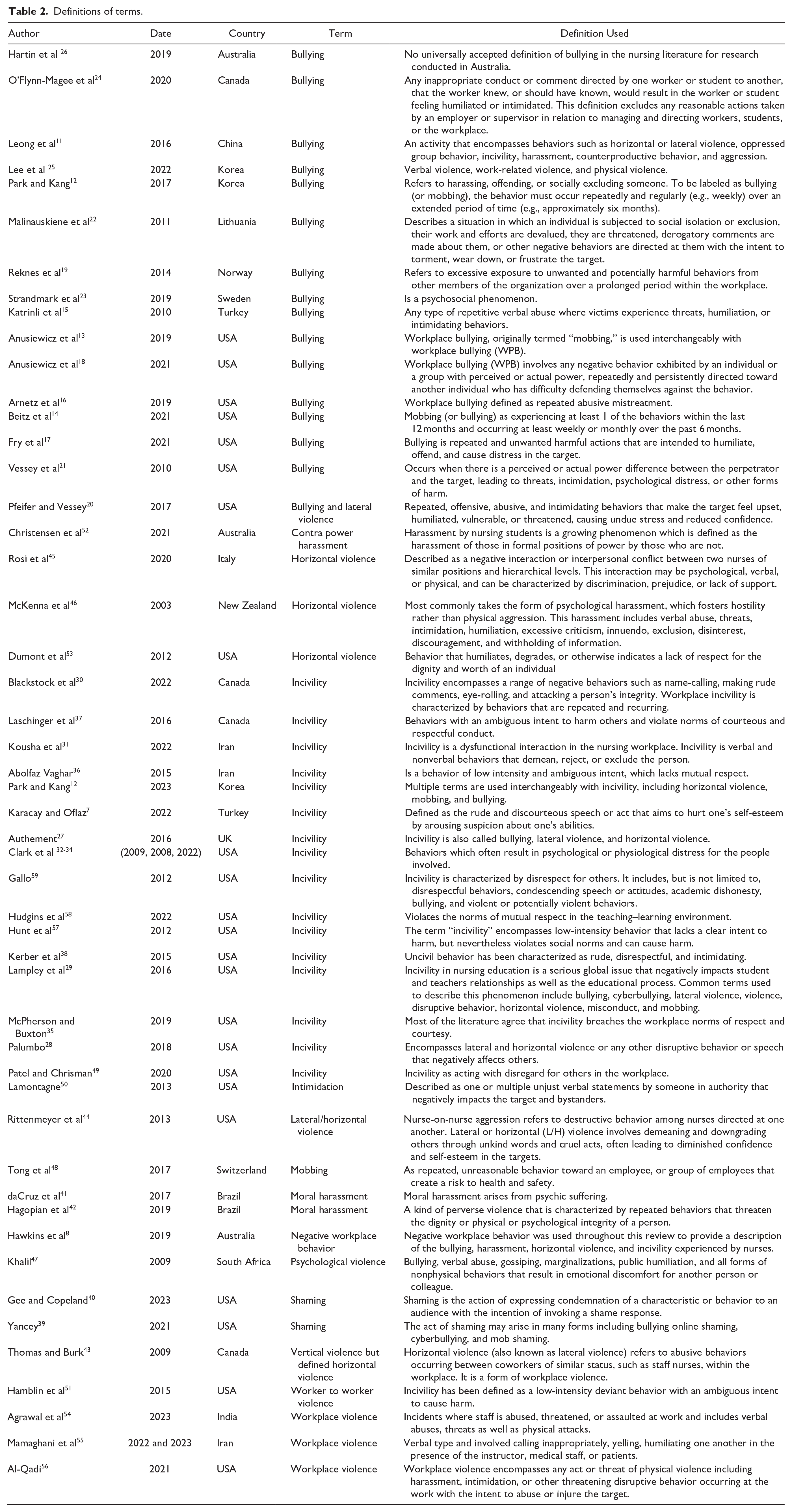
Thirteen different terms used to describe unwanted workplace behaviors were identified. The most frequently encountered terms in the literature were bullying and incivility (Table 1). The definitions of these terms overlapped and were used interchangeably (Table 2). Many of the definitions of bullying included the term “incivility” 11 in the description of behaviors, while the definition of incivility also included the descriptors of bullying. 12 Many of the articles included more than one definition of terms.
Frequency of terms.

Definitions of terms.
Bullying
The concept of bullying in the workplace is a complex and multifaceted issue, often defined inconsistently across studies. Anusiewicz et al 13 and Beitz et al 14 include mobbing within their definitions of bullying, a perspective also supported by Park and Kang. 12 Leong et al 11 describes a subset of bullying behaviors that encompass horizontal or lateral violence, oppressed group behavior, incivility, harassment, counterproductive behavior, and aggression. Katrinli et al, 15 Arnetz et al, 16 Fry et al, 17 Beitz et al, 14 Anusiewicz et al, 18 Park and Kang, 12 Reknes et al, 19 and Pfeifer and Vessey 20 all emphasize the repetitive nature of bullying. Furthermore, Vessey et al 21 and Anusiewicz et al 18 highlight the importance of a power differential that must exist between the perpetrator and the target in defining bullying. While Malinauskiene, 22 Strandmark et al, 23 and O’Flynn-Magee et al 24 all refer to psychosocial impacts including isolation and exclusion.
Characteristics of bullying behaviors often include verbal abuse, threats, humiliation, or intimidation, with the perpetrator’s actions interfering with the target’s job performance. 15 O’Flynn-Magee et al 24 describe bullying as inappropriate conduct or comments that a person knew or reasonably ought to know would cause humiliation or intimidation to a worker or a student. Arnetz et al 16 refer to bullying as abusive mistreatment, while Fry et al 17 identify it as harmful actions intended to humiliate, offend, or cause distress. Lee et al 25 includes both verbal and physical violence in their definition of bullying. Park and Kang 12 describe bullying behaviors as harassing, offending, or socially excluding someone, or negatively affecting their work. Similarly, Malinauskiene et al 22 and Pfeifer and Vessey 20 include social isolation or exclusion, devaluation of work efforts, threats, derogatory comments, or other behaviors aimed at tormenting, wearing down, or frustrating the target as bullying actions. However, as Hartin et al 26 noted in their review, there is no universally accepted definition of bullying in the literature.
Incivility
The concept of incivility is often conflated with bullying, lateral violence, and horizontal violence. Authement 27 and Palumbo 28 suggest that incivility is frequently referred to using these terms, a view echoed by Lampley et al, 29 who list bullying, cyberbullying, lateral violence, disruptive behavior, and mobbing as common descriptors of incivility. Park et al 12 also notes that terms such as horizontal violence, mobbing, and bullying are used interchangeably with incivility. Blackstock et al 30 identify uncivil behaviors as including name-calling, rude comments, eye-rolling, and attacks on a person’s integrity. Kousha et al 31 expand on this by including verbal and nonverbal behaviors that demean, reject, or exclude individuals. Clark et al 32-34 refer to the psychological and physiological distress caused by the behaviors, while the notion of respect, or the lack thereof, is frequently associated with incivility, as noted by McPherson and Buxton, 35 Vagharseyyedin, 36 Laschinger et al, 37 and Kerber et al. 38 Common descriptors of the behaviors associated with incivility are “disrespect” 59 and “discourteous” 7 ; however, authors also denote a range of behaviors including potentially violent behaviors.39-61
Discussion
Despite bullying and incivility being the most common terms used to describe unwanted workplace behaviors, new terms such as shaming, cyber bullying, moral harassment, and contrapower have been more recently introduced. Shaming as defined by Yancey 39 and Gee and Copeland 40 includes reference to online modalities such as cyber bullying, but both authors suggest shaming requires an audience in order to evoke the shame response, be that virtual or actual. The two authors that refer to moral harassment, daCruz et al 41 and Hogopian et al 42 are both from Brazil and draw similarities with incivility whereby the definition includes reference to the target’s dignity and integrity. Contrapower harassment is another term more recently presented in the literature. 52 This term can be likened to vertical, 43 lateral,20,44 or horizontal violence45-47,53 through which positions of power differentiate the target and perpetrator, as described in the definitions of bullying. Contrapower harassment was specifically used to describe student harassment of faculty. 52
The review noted that the severe emotional and psychological impact on targets and witnesses can lead to significant distress.21, 32-34,42,45,46 Feelings of humiliation, intimidation, and social exclusion have been highlighted as an intent and consequence of unwanted workplace behaviors.15,46,48 The review also noted unwanted workplace behaviors negatively impact the work environment, which leads to decreased job satisfaction and increased stress and desire to leave employment.32-34,17,20
It is unclear when or how nurses learn, accept, and model acts of unwanted workplace behaviors, but we know student nurses are also vulnerable to unwanted workplace behaviors despite not being considered part of the recognized workforce.24,29 There is evidence to suggest that student nurses are exposed to these behaviors during workplace learning5,60 and exhibit similar acts themselves participating in simulation learning and teaching activitites. 61
Based on this review, it is clear there is a need for a universal term and definition of unwanted workplace behaviors. Authors such as Boyle and Wallis 62 made a call in 2016, identifying the lack of consensus as a barrier to nursing researchers’ ability to compare and contrast perceptions and incidences of unwanted behaviors across disciplines and countries. Standardized terminology would improve recognition, reporting, and management of these behaviors, which in turn would facilitate better research, policy, and practical workplace interventions. 26
Unwanted workplace behaviors involve a form of aggression, whether overt or subtle, and contribute to a hostile work environment. However, each behavior differs in their specific dynamics and manifestations. While these terms have been used to describe destructive behaviors that disrupt the workplace, it seems that the nuances in their definitions are what separates the application of terms.49-61
Each term addresses different forms and levels of severity of unwanted workplace behaviors. However, each behavior shares intent. The intent of the behaviors is to intimidate, humiliate, disrespect, and isolate.15,46,47 More attention is needed to understand the motivation of the behaviors rather than labeling of the unwanted workplace behaviors that remain undesirable and unsafe in nursing practice regardless of the terminology used to describe them.
Limitations
Several potential limitations in the review methods may have influenced the findings. First, many of the studies relied on self-reported data, and this may result in under- or over-reporting of behaviors. While the review identified a wide range of terms, it did not assess the impact of these behaviors in specific cultural or organizational contexts, which may vary significantly across different healthcare settings. Despite including international studies, the heterogeneity of the studies in terms of settings, populations, and definitions of unwanted behaviors may limit the comparability of results. The review also predominantly included studies from high-income countries, which may not be generalizable to low- and middle-income settings where healthcare dynamics and workplace cultures differ significantly. The review included only original research studies which excluded possible relevant discussion and opinion pieces and unpublished or gray literature that could provide additional insights into the terminology used to describe unwanted workplace behaviors in nursing. The search included the term “workplace” which seemed to remove studies that focused on unwanted behaviors experienced from patients and family members, leaving the focus on nursing workforce.
Conclusion
This scoping review highlights significant variability in the terminology used to describe unwanted workplace behaviors in nursing. Addressing this variability is essential for advancing research, policy, and practice. Clear, consistent definitions and a singular graded term will improve the recognition, reporting, and management of these behaviors, ultimately enhancing the work environment for nurses and the care they provide to patients. By establishing a standardized language, researchers can more accurately measure the prevalence and impact of these behaviors, leading to more robust and comparable data across studies. Policymakers can develop more targeted interventions and regulations to mitigate these behaviors, while healthcare organizations can implement more effective training and support systems for their staff. Ultimately, a unified approach to defining and addressing unwanted workplace behaviors will contribute to a more sustainable, safer and more productive healthcare environment, benefiting both healthcare workers and patients alike.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval was not required for this review, as it involved the analysis of publicly available data.