
Abstract
Aggressive end-of-life care in patients with advanced cancer is associated with poor experiences and outcomes. The purpose of the study was to examine the impact of aggressive end-of-life care on caregiver satisfaction for caregivers of bereaved advanced cancer patients. Data of 101 caregivers were gathered using a longitudinal, descriptive correlational design study. Postdeath interviews were conducted 2 months after the patient’s death. The most common end-of-life care indicators were patient not enrolled in hospice or enrolled within 3 days of death, >1 hospitalization, and intensive care unit admission. More than one-third of patients received at least one of the aggressive end-of-life care indicators in the last 30 days of life. From the multiple linear regression analyses, patient intensive care unit admission and having more than one hospitalization significantly affected caregiver satisfaction with care. Understanding caregiver satisfaction with care may improve the clinical practice of nurses who have crucial role in patients’ end-of-life care.
Aggressive end-of-life (EOL) care in patients with advanced cancer continues to remain common practice even though many studies have demonstrated that aggressive care before death is related to higher physical discomfort, psychological distress, and lower quality of dying.1,2 Aggressive EOL care is defined as care that focuses on intensive, life-sustaining treatments aimed at extending a patient’s lifespan. 3 Research has shown that the following indicators of aggressiveness in cancer care near the EOL are associated with poor patient experiences and outcomes: (1) administration of new chemotherapy during the last 30 days of life; (2) admission to intensive care unit (ICU) during the last 30 days of life; (3) more than 1 emergency department (ED) visit during the last 30 days of life; (4) more than 1 hospitalization during the last 30 days of life; (5) any intravenous chemotherapy during the last 14 days of life; and (6) no receipt of hospice care or hospice care started within 3 days of death. 4
End-of-Life Care and Caregiver Satisfaction
Caregivers of patients with cancer are often highly involved in patient care, not only in providing care but sharing decision-making responsibilities during the patient’s illness trajectory.5,6 Furthermore, caregivers’ experiences may vary during the patient’s EOL trajectory of care since patients and their families often experience changes in treatment plans, settings, and health care providers. 7 According to the study by Aoyama et al, 8 14% and 17% of caregivers suffered from complicated grief and major depressive disorder after patient death, respectively. Also, caregiver satisfaction with care had a significant impact on bereaved caregivers’ complicated grief, depression, and quality of life.8,9 Although factors related to improving EOL care satisfaction for patients with cancer has been widely investigated, few studies have focused upon caregivers’ satisfaction with EOL care. Since caregiver satisfaction is one of the crucial quality indicators of high-quality care and satisfaction can aid in the caregivers’ grief process after the patient has died,10,11 understanding caregiver satisfaction with EOL care is vital.
Purpose
The purpose of this study was to examine the relationships between aggressive EOL care and caregiver satisfaction with care for caregivers of patients with advanced cancer. The research question was as follows: Does aggressive EOL care in patients with advanced cancer have a significant relationship with caregivers’ satisfaction with care while controlling for caregiver’s age, gender, and evaluation of the effectiveness of the treatment plan at the patient’s death?
Methods
Design and Setting
Data for this study were gathered from a longitudinal, descriptive correlational design study that used convenience sampling to recruit 378 patient and their caregivers (R01NR014856). The parent study explored factors influencing treatment decisions, goals of care, and aggressiveness of care at EOL in patients with advanced cancer. Subjects were enrolled into the study from January 2015 to October 2018 at the Seidman Comprehensive Cancer Center outpatient oncology clinics at University Hospitals Cleveland Medical Center in Cleveland, Ohio.
Sample
There were 237 patient-caregiver dyads who participated in the parent study. In the parent study, all 237 caregivers provided study data at enrollment in the study as well as every 3 months until the end of the 15-month study prior or until patient death. Caregivers of patients who died were contacted by telephone 2 months postdeath and asked if they would be willing to answer questions related to their experience during the last weeks of the patient’s life. Of 137 caregivers who met the criteria and were contacted for interviews, 36 were omitted (32 did not respond to the calls or were lost to follow-up and 4 declined). The remaining sample was comprised of 101 (74%) caregivers who completed the interview. The major reason for declining the postdeath interviews was the emotional vulnerability of the caregiver (“not being ready to talk yet”).
To be eligible for inclusion in the parent study, patients had to (1) be actively receiving treatment or regularly being seen by their oncologists; (2) be over the age of 18; (3) be cognitively intact; and (4) have a diagnosis of stage III or IV gastrointestinal, lung, or pancreatic cancers. Inclusion criteria for the caregivers included the following: (1) be identified by the patient as their primary caregiver (usually a family member); (2) be over the age of 18; and (3) be cognitively intact. Written informed consent was obtained for the patient and caregiver by trained research staff members. The study was approved by the University Hospital Institutional Review Board (approval code: 08-14-17C). G*power 3.1.9.7 was used for power analysis. Using a power of 0.80, alpha of .05, effect size of 0.15, and the number of predictors of 6, a minimum sample size of 98 was calculated as being needed for analyses.
Procedure
Patient and caregiver demographic data were obtained at study enrollment. After the patient death, a retrospective chart review was conducted to determine which of the 6 indicators of aggressive care at EOL were present. A phone call was made approximately 2 months after the patient’s death. The postdeath interview with the caregiver was conducted by a single research assistant with expertise in interviewing this caregiver population after patient death. Once the research assistant gave condolences and permission was established, the research assistant began the interview. The interview consisted of the administration of the Family Satisfaction with End-of-Life Care (FAMCARE) instrument by asking the caregivers a list of questions and 2 additional open-ended questions (see “Measures” section).
Measures
Patient and caregiver characteristics
Patient and caregiver demographics were collected at baseline. The demographic variables included age, gender, race, patient’s type of cancer, cancer stage, treatment status, caregiver relationship to patient, and whether the patient and caregiver were living together.
Aggressive end-of-life care
Aggressive end-of-life care was measured by conducting a chart review after death and documenting the receipt (or non-receipt) of 6 indicators commonly used to indicate aggressive care at EOL: The indicators were (within the last 30 days of life): (1) administration of new chemotherapy; (2) admission to ICU; (3) more than 1 ED visit; (4) more than 1 hospitalization; (5) any intravenous chemotherapy within the last 14 days of life; and (6) no receipt of hospice care or hospice care started within 3 days of death. 4 Each indicator was coded as 0 if the patient did not receive the specific aggressive care treatment or 1 if the patient did receive the specific aggressive care treatment. The total aggressive EOL care score was a sum of all 6 items with scores ranging from 0 to 6, with higher scores indicating greater amount of aggressive care received at EOL.
Family satisfaction with end-of-life care
The Family Satisfaction with End-of-Life Care (FAMCARE) questionnaire was used to measure family satisfaction with advanced cancer care, specifically at the end of life. 12 The FAMCARE consists of 13-items and is measured by a 5-point Likert scale (1 = very dissatisfied, 2 = dissatisfied, 3 = undecided, 4 = satisfied, and 5 = very satisfied). Mean imputations were made if ≤2 items were missing from the 13 FAMCARE items. The total score for the tool ranges from 13 to 65, with higher scores representing greater satisfaction with EOL care. The instrument has well-established reliability and validity with a Cronbach’s alpha of .95 identified in this study.13,14
Evaluation of the effectiveness of the treatment plan
Evaluation of the effectiveness of the treatment plan was measured using a single-item visual analog scale (VAS) question, “How well do you feel the treatment plan is working at death?” Subjects marked an “x” anywhere on the line that represented their response. Anchors for the VAS were 0 (not very well) to 100 (very well).
Open-ended questions
Two open-ended questions that related to caregivers’ experience of EOL care were asked at the postdeath interview. The 2 questions were as follows: (1) “Was there anything specific that made you think it was time to stop cancer therapy and focus on comfort care?” and (2) “Looking back, do you think the care and treatment your loved one received at EOL was consistent with his/her wishes?”
Data Analysis
Quantitative data were analyzed using IBM SPSS Version 27.0, the responses to the 2 open-ended questions were transcribed, and responses were grouped into common response categories. The categories of open-ended responses were reviewed by members of the research team and shared with researchers involved in EOL care research so as to ensure agreement in the classification of caregivers’ responses.
Descriptive statistics were used to describe the sample of patients and caregivers. Continuous variables were examined using mean, median, standard deviation, and range, and categorical variables were examined using frequencies and percentages. To examine the relationships between caregiver satisfaction with care and aggressive care received at EOL, point-biserial correlations and multiple linear regression were conducted. The predictor variables were the 6 indicators of aggressive EOL care, and the dependent variable was caregiver satisfaction with care (total score). In addition, the following covariates were included in the analysis: caregiver’s age, gender, and evaluation of the effectiveness of the treatment plan at the patient’s death, because significant relationships between these variables and caregiver satisfaction with care were found in other studies.13,15
Results
Demographic and clinical characteristics of the 101 patients and their caregivers are seen in Table 1. Caregivers were predominantly female, white, spouse of the patient, and lived with the patient. On average, caregivers were 66.0 (SD = 9.3) years old. The mean score of caregivers’ evaluation of the effectiveness of treatment plan at the patient’s death was 61.6 (Mdn = 55.5, SD = 27.1). On average, patients were 60.0 (SD = 12.7) years old, were equally split between male and female, and were predominantly white. The majority of patients had a diagnosis of gastrointestinal cancer (39.6%), followed by lung cancer (38.6%) and pancreatic cancer (21.8%). The majority of patients in the study had a stage IV diagnosis and received chemotherapy at the time of enrollment.
Patient and Caregiver Characteristics at Baseline (N = 101).
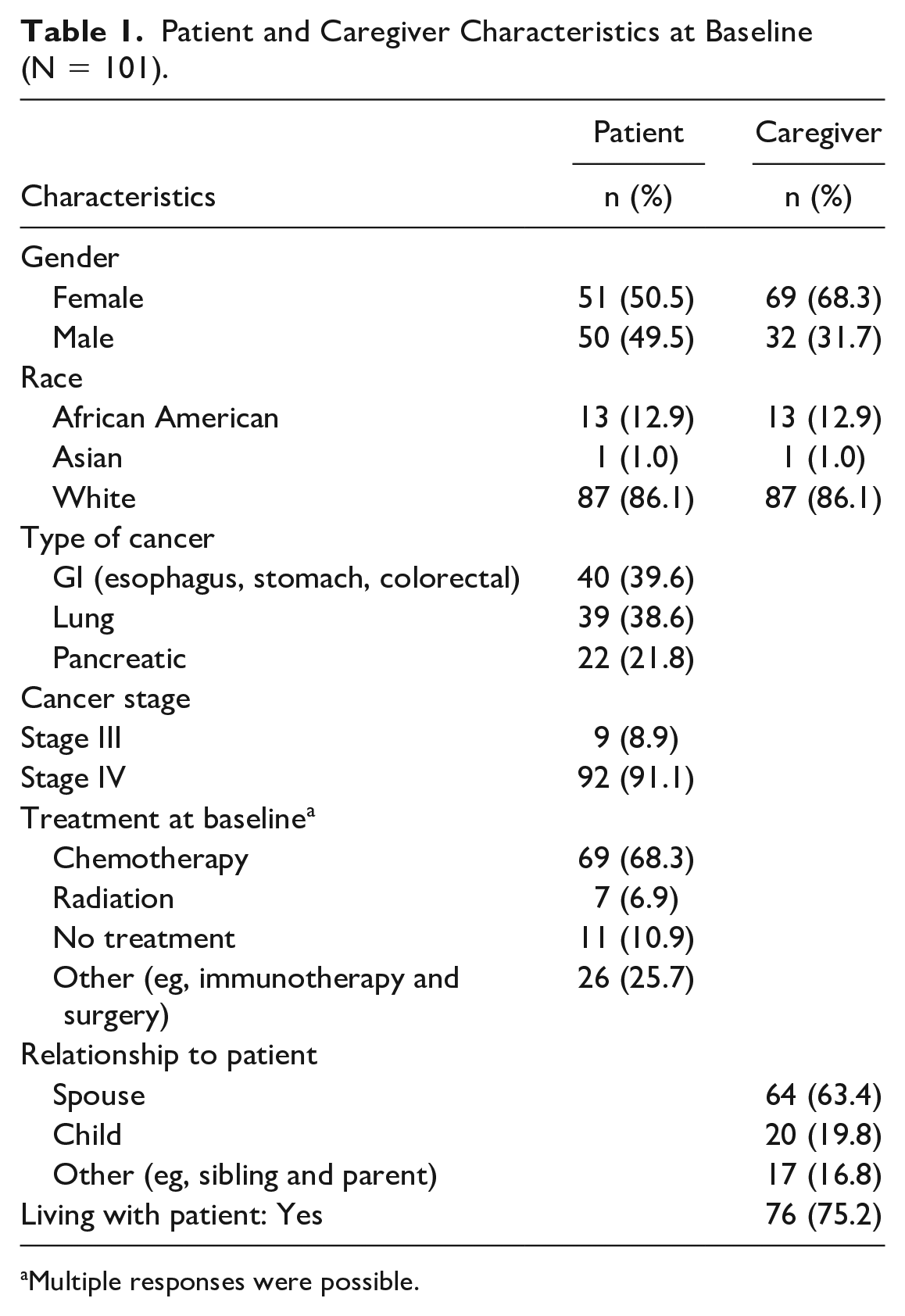
Multiple responses were possible.
The number and percentage of the patients who received aggressive EOL care within 30 days of death are presented in Table 2. The 3 most common EOL care indicators were patient not enrolled in hospice or enrolled within 3 days of death (n = 18, 19.8%), >1 hospitalization (n = 15, 15.2%), and any ICU admission (n = 11, 11.1%). More than one-third (n = 36, 35.6%) of patients with cancer received at least one of the aggressive EOL care indicators during the last 30 days of life. Almost one-fifth (18.8%) received only 1 indicator of aggressive EOL care, 10.9% received 2, 5.0% received 3, and 1.0% received 4 indicators of aggressive EOL care before death.
Number of the Patients who Received Aggressive End-of-Life Care Within 30 Days of Death (N = 101).
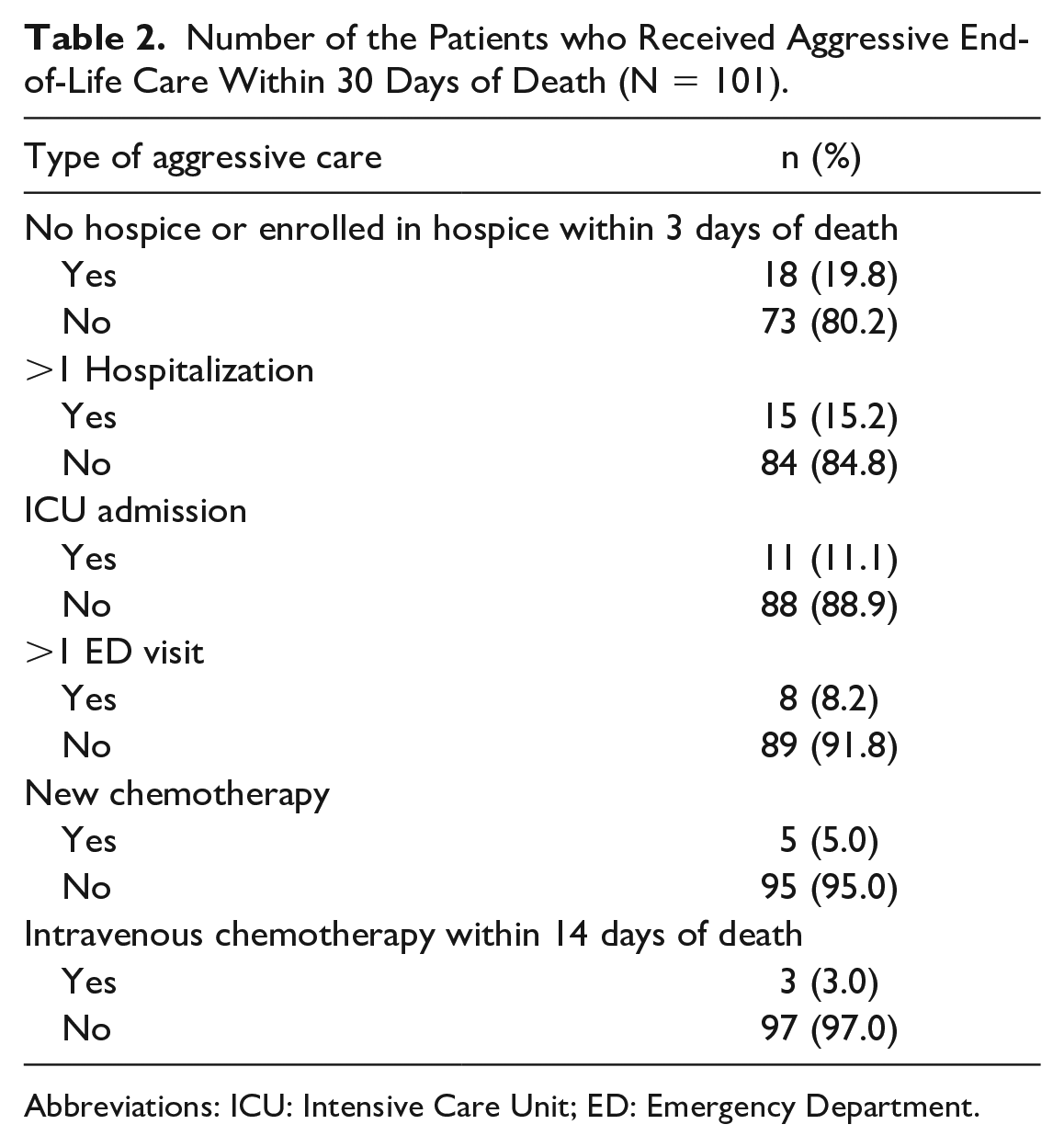
Abbreviations: ICU: Intensive Care Unit; ED: Emergency Department.
The average total FAMCARE score was 54.40 (Mdn = 55, SD = 10.17), ranging from 18 to 65. As seen in Table 3, the means varied by item, with the highest mean score reported for the item “the way the family was included in treatment and care decisions” and the lowest mean score reported for the item “information provided about when patient’s death was likely to occur.”
Responses to FAMCARE Items and Total Score (N = 101).
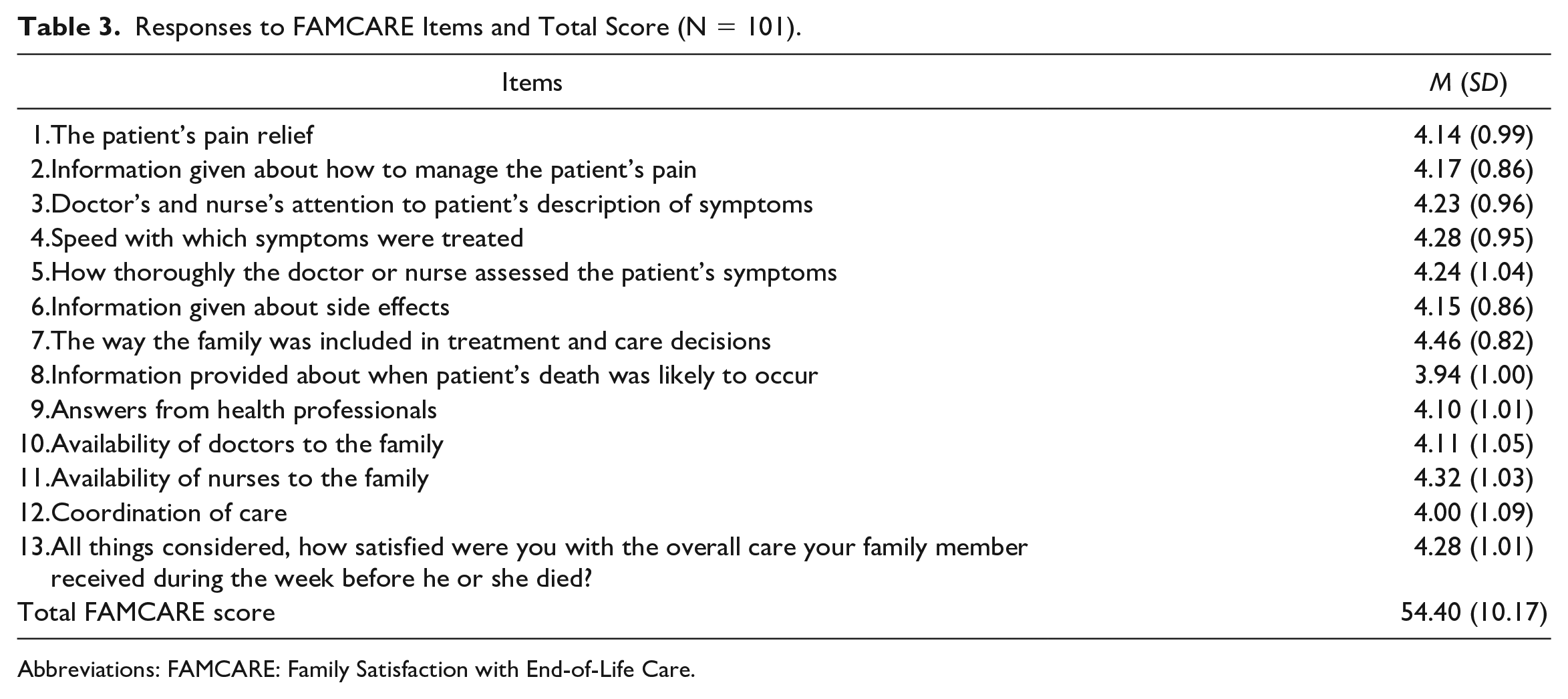
Abbreviations: FAMCARE: Family Satisfaction with End-of-Life Care.
From the point-biserial correlation analysis, lower caregiver satisfaction with care was significantly related to patient ICU admission (r = −0.25, p = .013) and having at least 1 hospitalization (r = −0.24, p = .021) within the last 30 days of life. A multiple linear regression was conducted to examine the predictors of caregiver satisfaction with care. Assumptions for multiple linear regression were tested and 3 predictor variables failed to meet the assumption of adequate variance which had more than 90% of cases in 1 category. These variables were removed from the multiple linear regression analysis because of concern regarding the potential for them to weaken correlations with other variables. 16 Therefore, the 3 predictor variables included in the regression analysis were ICU admission, >1 hospitalization, and no hospice or was enrolled hospice within 3 days of death. Covariates (caregiver’s age, caregiver’s gender, evaluation of the effectiveness of the treatment plan at the patient’s death) were included, and the outcome variable was caregiver satisfaction with care (total score). The following variables made a statistically significant contribution toward predicting caregiver satisfaction with care: patient ICU admission and >1 hospitalization within 30 days of death (R2 = 0.17, R2adj = 0.10, p = .040). As seen in Table 4, having >1 hospitalization made a slightly larger unique contribution than ICU admission to caregiver satisfaction with care. Caregivers of patients with 0 or 1 hospitalizations demonstrated a higher satisfaction with care compared with those who had >1 hospital admission (M = 55.87, SD = 9.44 vs M = 48.34, SD = 10.90; p = .009). Caregivers of patients with no ICU admissions reported significantly higher satisfaction with care than caregivers of patients who did have an ICU admission experience (M = 55.39, SD = 9.24 vs M = 47.26, SD = 14.47; p = .028).
Effects of Aggressive End-of-Life Care on Family Satisfaction (N = 101).
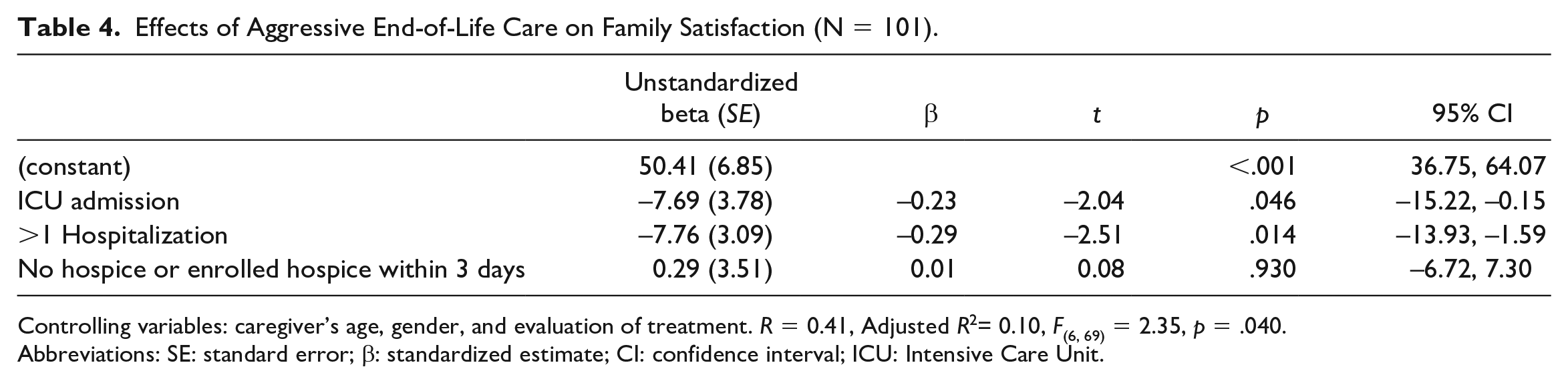
Controlling variables: caregiver’s age, gender, and evaluation of treatment. R = 0.41, Adjusted R2= 0.10, F(6, 69) = 2.35, p = .040.
Abbreviations: SE: standard error; β: standardized estimate; CI: confidence interval; ICU: Intensive Care Unit.
Of the 51 caregivers who participated in the interview portion of the study, 62.75% had negative comments with a focus upon (1) inconsistency of care, (2) negative EOL care experience due to aggressive treatments, (3) the need to introduce discussions of hospice care earlier in the illness trajectory, (4) the lack of information given (or discussed) by health care providers that focused on the patient’s EOL care goals, and (5) the lack of symptom management at EOL—especially pain control. Several caregivers noted that for patients with a terminal illness, “getting hospice sooner rather than later was important.” Concerns regarding transitioning to hospice were noted with ~25% of caregivers noting that the transition to EOL care made them feel “abandoned by oncology” or “out of the picture.” Also, caregivers focused on an impression that while in hospice care, the patient was over-medicated, and there was a lack of consistency in nursing care with different nurses caring for their loved one every day. Finally, there were noted concerns regarding aggressive EOL care that their loved one received. These comments included that they were “tired of [their loved one] ending up in the hospital or ICU” and in thinking that “the patient would have passed away more peacefully” had EOL care not been so aggressive.
Discussion
Based upon findings from this study, there were 2 major findings. First, we identified 2 key factors that significantly contributed to lower caregiver satisfaction with care: ICU admission and >1 hospitalizaton within the last 30 days of life. The finding that lower satisfaction with care in caregivers related to their loved ones being admitted to the ICU close to death is supported by other studies.17,18 It is possible that the high-technology environment of the ICU interfered with caregivers’ ability to be in a close and a supportive environment with their loved one.19,20 Research has shown that caregivers of patients who were admitted to the ICU often experience negative emotions (eg, fear and helplessness) due to the patient’s condition and the ICU environment. 19 As a result of their negative experience, caregivers’ satisfaction with care can be negatively affected. 20
Our findings regarding the significant relationship between patient hospitalization (>1) and caregiver satisfaction with care has mixed support from prior studies. Some studies report similar relationships between hospitalization and low caregiver satisfaction,17,21 while others have found no significant relationships. 18 The potential reasons for inconsistent support of this finding may be due to the sample characteristics of the studies. Studies examining the relationship between EOL care and caregiver satisfaction with care have varied in patient characteristics (patient age and cancer stage),17,18 and caregiver demographic characteristics (eg, age and gender).22,23 It is important to note that while our study found no significant association between caregiver satisfaction and any of these demographic or clinical factors, it is possible that our sample was different in key characteristics (eg, stage of cancer) from other studies.
From the multiple linear regression analysis, 10% of caregiver satisfaction with care was explained by the independent variables included in the analysis (small effect size), limiting the clinical significance of this finding. There may be several reasons for the low coefficient of determination. First, 16 incidences of aggressive EOL care from the 3 indicators were not included in the analysis due to the insufficient variability (administration of intravenous chemotherapy within 14 days of death, administration of new chemotherapy, and >1 ED visits within 30 days of death). Given the relatively low rates of aggressive EOL care use, removal of the 3 indicators of aggressive EOL care may have influenced the overall regression R2.
The other possible reason for the low R2 could be that the independent variables included in the analysis may not have thoroughly captured the factors related to caregiver satisfaction with care. For example, location of patient death is often included as one of the indicators of aggressive EOL care in other studies,15,18,21 which reported a significant relationship between the location of patient death and caregiver satisfaction with care.15,21 Caregivers reported higher satisfaction with care if the patient died in their preferred location 15 or if the patient died in a hospice/palliative care unit rather than died in an inpatient care unit. 21 Therefore, the inclusion of this variable will be needed for future research to fully understand the factors related to caregiver satisfaction with care.
The most common type of aggressive EOL care received by patients found in this study (no hospice or enrolled hospice within 3 days of death) was consistent with what is reported in other studies (38.2%-47.7%).17,18 However, the overall percentage of patients who received any episode of aggressive EOL care (35.6%) was lower than what was found in another study (72.3%) by Ersek et al. 21 Furthermore, the number of patients who received each aggressive EOL care indicator was relatively lower in this study when compared with other studies.17,18,21 For example, 11.1% of patients were admitted to the ICU in this study while others reported ranges from 13.1% to 25.4%.17,18,21 The differences in the number of patients receiving aggressive EOL care can be explained by the patients’ cancer stage, since patients’ treatment options can be different based on their stage and survival estimates. 24 In this study, most of the sample was comprised of patients with stage IV cancer and their caregivers (91.1%), while other studies have reported samples consisting of 66% to 72.3% of patients with stage IV cancer.18,21
A second finding was that the overall caregiver satisfaction with care reported in this study was high. In addition, on average, caregivers were satisfied or very satisfied with care. This result is consistent with other studies that showed cancer caregivers’ satisfaction with care tended to be high.22,23,25 As seen in Table 3, the FAMCARE item “Information provided about when patient’s death was likely to occur” had the lowest mean score among the 13 items. This finding is similar to the findings from Naoki et al, 23 who reported that information given to caregivers about the patient’s prognosis was the most dissatisfying factor of EOL care in family caregivers of patients with advanced cancer. This is also supported by the responses from the 2 open-ended questions in that caregivers expressed negative experiences related to the lack of discussion or information provided on EOL care.
There are some limitations of this study that need to be noted. First, convenience sampling was used in the parent study, which has the potential to reduce the generalizability of results. Second, among the 6 indices of aggressive EOL care, administration of new chemotherapy, >1 ED visit, and any intravenous chemotherapy were omitted from the regression analysis due to violation of key assumptions. It is not possible to know what, if any, role these factors would have played in our analyses had there been sufficient data to include these variables. In addition, small variability in both independent and dependent variables limits the generalizability of study results. Third, more than 90% of patients were in stage IV; therefore, the generalizability of study results to all patients with cancer and their caregivers is limited. Finally, a single individual conducted all of the FAMCARE interviews, which has the potential to introduce research bias. 26
Despite these limitations, the findings from this study provide additional evidence regarding factors that influence caregivers’ sense of satisfaction with care. Our ability to reproduce findings across studies and populations is important if we are to provide meaningful EOL care—care that impacts not only the patient but their caregiver as well. While it is noted that caregivers showed the lowest satisfaction on information given related to patient death, active EOL conversations between health care providers and caregivers are needed in clinical settings. In the literature, health care providers often report uncomfortable or distressed feelings in bringing up bad news or starting EOL discussions. 27 To enhance the effectiveness of EOL discussion, guidelines for health care providers will be needed and barriers to delivering the EOL discussion should be identified. Also, avoidance of ICU admission or hospitalization at EOL may enhance the overall caregiver satisfaction with care. As found in the interviews, in-depth conversations about treatment plans, including aggressive EOL care, between health care providers, patients, and their caregivers are needed. For future research, inclusion of the 6 indicators of aggressive EOL care as well as other variables, such as location of patient death, should be performed to fully understand the phenomena.
Along the cancer care continuum, nurses play important and diverse roles. 28 Nurses often identify their role when caring for patients with cancer at EOL as a supporter, advocate, and middle person who provide information to physicians, patients, and caregivers. 29 Nurses play a crucial role in coordinating patients’ EOL care and facilitating communication between patients, caregivers, and health care providers throughout the care trajectory. 28 While the focus of care and support at EOL is correctly upon the patient, the importance of providing support to the caregiver is vital as well. When nurses have information about how EOL care impacts them, months after death, there is potential to draw attention to this need. Results from this study may expand nurses’ understanding of caregiver satisfaction with EOL care and may inform their clinical practice so that they can be more aware of the impact of EOL care upon not only the patient, but the caregiver as well.
Footnotes
Acknowledgements
The authors thank all of the patients and caregivers who gave of their time to participate in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Health/National Institute of Nursing Research (R01NR014856).