
Abstract
Despite efforts to improve management and leadership behaviors among nurse managers, studies have shown the pervasive nature of abusive supervision in nursing practice, with strong evidence linking this type of behavior to reduced work productivity among nurses. This systematic review aimed to appraise and synthesize peer-reviewed studies that examine nurse-related and patient safety outcomes associated with abusive supervision. The review searched nursing literature from five databases (PubMed, CINAHL, Scopus, Web of Science, and PsycINFO) between August and November 2022. A total of 21 relevant studies were identified, with the Abusive Supervision Scale being the most frequently used measurement tool. Through content analysis, the review identified 29 outcomes which were categorized into six groups: (a) affective-based, (b) behavior/performance-based, (c) relationship-based, (d) cognitive-based, (e) health and well-being, and (f) nursing care. In addition, 10 mediators were identified and grouped into three categories: (a) affective-based, (b) motivation-based, and (c) health and well-being. The review findings provide compelling evidence regarding the detrimental effects of abusive supervision in the nursing workforce. Moreover, the review emphasizes the need for further research to explore how such behavior can impact patient safety outcomes. To address abusive supervision, it is crucial to promote positive behaviors among nurse managers through human resource mechanisms, relevant rules and policies, and theory-driven leadership development programs.
The shortage of nurses continues to present challenges to healthcare institutions worldwide, impacting the delivery of healthcare services and jeopardizing patient safety and the quality of nursing care. A global estimate has revealed a deficit of 13 million nurses, and the United States alone will require nearly 1.2 million nurses by 2030 to maintain an effective healthcare delivery system. 1 With the impending retirement of baby boomer nurses within the next 5 years 2 and the increasing rate of younger nurses leaving the profession, 3 the nursing shortage is expected to worsen. Given the detrimental consequences of a persistent nursing staff shortage, 4 it is not surprising that healthcare organizations have implemented various measures to address this issue, primarily focusing on different elements of the work environment that influence nurses’ decisions to leave. 5 Evidence has shown that the behaviors of nurse managers play a significant role in sustaining an adequate and committed nursing workforce and improving nursing staff retention. 6
Effective leadership and management behaviors (e.g. transformational and ethical) among managers and leaders have been consistently cited as strong precursors of employees’ work effectiveness and as strong factors influencing turnover decisions.6,7 Negative behaviors, including abusive supervision, have often been reported to be associated with a myriad of adverse effects on the labor workforce.8,9 Tepper 10 conceptualized abusive supervision as a subjective assessment rooted in subordinates’ perceptions of sustained hostile verbal and nonverbal actions by supervisors, excluding physical contact. A leader’s abusive behavior is believed to be affected by an individual’s disposition and the context. A negative workplace culture, the facility size, the span of management, the absence of policies and rules to govern employees’ behaviors in the workplace, and the lack or absence of check and balance systems are some of the contextual elements that may drive a leader to engage in abusive behaviors.11,12 Abusive behaviors of a leader may be dispositional in nature often as a response when there is a perceived threat to their status or position, when their goals are not met,10,13 or simply as a way to conceal their incompetence and unproductiveness. 14
In many healthcare settings, nurses are not only supervised by nurse managers but also interact with and receive supervision from their colleagues. 15 This dynamic is particularly evident in team-based healthcare environments where collaboration and interprofessional relationships are essential. 16 The involvement of colleagues in the supervision of nurses can have implications for the occurrence and impact of abusive supervision in nursing practice. Although nurse managers traditionally hold a formal supervisory role and have authority over the nursing staff, abusive behaviors can also be displayed by colleagues within the same hierarchical level or even from subordinate nurses. 17 Abusive supervision from both nurse managers and colleagues can contribute to a toxic work environment, negatively impacting the well-being, job satisfaction, and overall performance of nurses. 18
Although a specific theory explaining the emergence of abusive supervision has not been identified, previous studies have utilized various theoretical frameworks to examine this phenomenon. Some of the theories employed include the Conservation of Resources Theory (COR), 19 the Self-Determination Theory (SDT), 20 and the Social Learning Theory (SLT). 21 Among these theories, the COR has been widely used as a theoretical basis in abusive supervision studies across different disciplines. This theory suggests that individuals experience psychological strain when they perceive their resources to be threatened or lost.19,22 In response to perceived threats to their resources, individuals may choose to withdraw or disengage to protect their remaining resources and prevent further loss. 23 Applied to the nursing context, a nurse manager or leader who exhibits hostile behaviors or actions may threaten the resources (such as structural resources, work environment, and social support) that nursing staff need to effectively carry out their responsibilities.24-26 This, in turn, can have a negative impact on the work performance of the nursing staff and potentially affect the quality of care provided to patients.
Existing literature has provided evidence that nurse managers’ abusive supervision can have negative effects on nurses’ work productivity 27 and their health and well-being. 28 In addition, a limited body of evidence has linked abusive supervision to suboptimal nursing care. 29 However, it is important to consider a broader perspective when designing and implementing leadership interventions and formulating measures to enhance work productivity in nurses and maintain an effective nursing workforce. To fill this lacuna, this systematic review was conducted to examine the current state of the science related to abusive leadership in the nursing workforce. Specifically, this review aimed to identify (a) the association between abusive supervision and nurse-related and patient safety outcomes and (b) mediators that serve as pathways between abusive supervision and a broad range of outcomes in nursing.
Methods
Design
This systematic review of literature examined the association between abusive supervision and outcomes in nurses and patients using guidelines from the Center for Reviews and Dissemination. 30 The results of the systematic review are presented following the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 31 The PRISMA statement provides a structured framework for reporting systematic reviews and meta-analyses, ensuring transparency and consistency in reporting methods, results, and conclusions.
Search Methods
Articles relevant to this review were gathered from five sources, namely, PubMed, CINAHL, Scopus, Web of Science, and PsycINFO. The following Medical Subject Headings (MeSH) and key terms were used individually or in combination, with the utilization of Boolean operators (AND, OR, and NOT): abusive supervision, nursing, nurse manager, nurse leader, nurse administrator, patient safety, care quality, job performance, turnover intention, burnout, job satisfaction, and work engagement. In addition, we manually searched the references of the included articles.
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria were applied to identify relevant articles for this systematic review. The criteria for inclusion were as follows: (a) the study focused on abusive supervision in the nursing context, (b) the study examined outcomes related to abusive supervision (including nurse-related, patient, and organizational outcomes), (c) the study investigated mediators of abusive supervision, and (d) and the articles were peer-reviewed. Owing to the substantial number of abstracts and the sole English language proficiency within our research team, our focus was exclusively on nursing studies that had been published in English. To ensure consistency and comparability among the included studies, qualitative studies, gray literature, and studies where nurses were not the primary population were excluded. No restrictions were set on the publication year to capture all relevant research on abusive supervision in nursing.
Quality Appraisal
The Joanna Briggs Institute (JBI) Critical Appraisal Tool 32 was the quality appraisal tool used to evaluate the methodological rigor of the studies reviewed. The JBI checklist evaluates eight elements in a study, including the criteria for selecting samples, research settings and samples, exposure measures, the use of objective and standard criteria for measurement conditions, confounders, management of confounders, measurement, and data analysis.
Data Screening
A total of 375 citations were retrieved and exported to EndNote to facilitate data management and screening. After eliminating duplicate entries, the titles and abstracts of all retrieved documents were reviewed, applying the predefined inclusion/exclusion criteria. For abstracts that remained after this initial screening, full articles were procured and meticulously examined to ascertain their alignment with the inclusion/exclusion criteria. To ensure the rigor of the screening process, two reviewers (LJL/CK) independently evaluated the eligibility of the selected studies, conducting two rounds of assessment. In cases where differences of opinion arose, consensus meetings were convened between the reviewing pair, and any discrepancies were resolved through comprehensive deliberation. Should a unanimous decision prove elusive, a third reviewer was consulted to determine the final inclusion status of the respective article. This systematic and collaborative approach was employed to ensure the thoroughness and reliability of the study selection process.
Data Abstraction and Synthesis
All included articles were assessed by two independent reviewers (LJL and CK), and the following information was extracted and entered into a matrix table: author name, sample size, country, research approach, scales used, and the reliability and validity of the scales (Table 1). Due to the heterogeneity of the study results, statistical pooling was not conducted. Therefore, the mediators and outcomes of abusive supervision were identified through conventional content analysis. Conventional content analysis refers to a process of analyzing and categorizing textual data extracted from included studies in a systematic and structured manner. 33 The two independent reviewers sorted all outcomes and mediators based on their characteristics and commonalities, and clustered them into meaningful categories. Discussion was conducted to reach a consensus and identify the final categories. Tables 2 and 3 present the outcomes and mediators of abusive supervision.
Summary of Articles Reviewed.
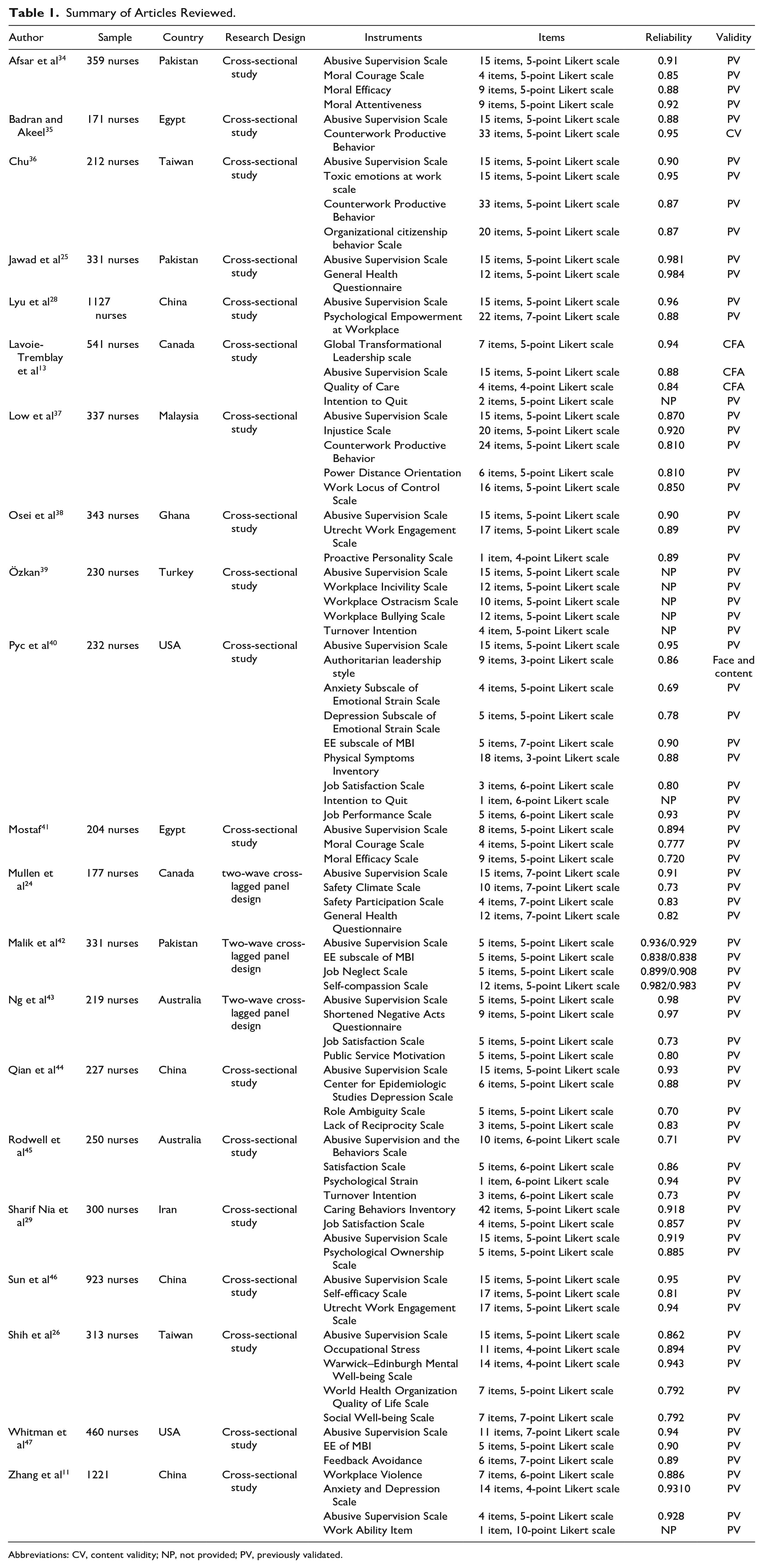
Abbreviations: CV, content validity; NP, not provided; PV, previously validated.
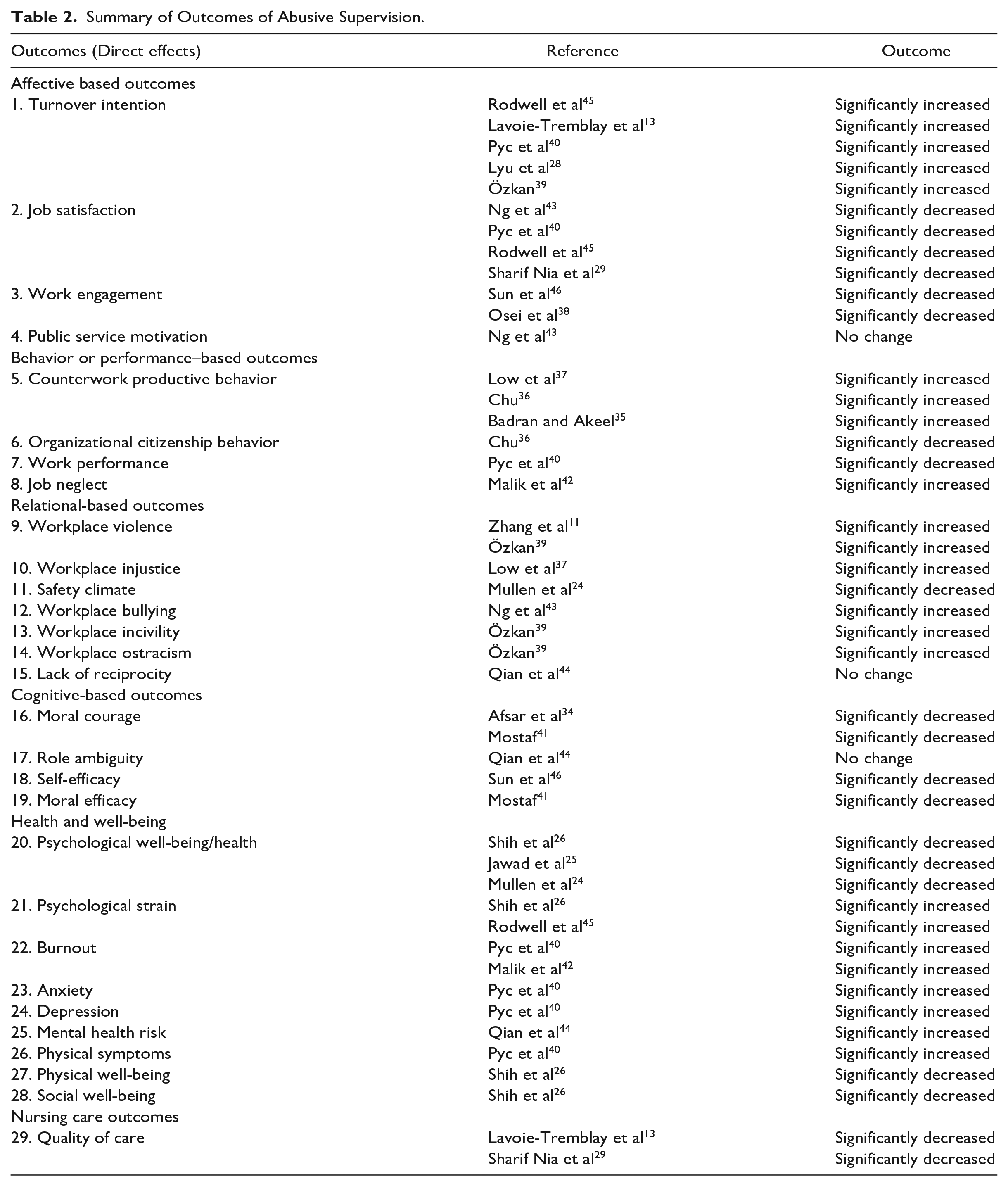
Summary of Outcomes of Abusive Supervision.
Summary of Mediators of Abusive Supervision.

Results
Search Outcomes
During the initial search, a total of 375 articles were identified. After removing duplicates, 213 articles remained for further screening. Based on the screening of titles and abstracts, 167 articles were excluded, leaving 46 articles for full-text screening. After assessing the full-text articles, an additional 25 articles were excluded, resulting in a final selection of 21 articles for inclusion in the systematic review. The search and selection processes are visually presented in Figure 1, illustrating the flow of articles throughout the review.
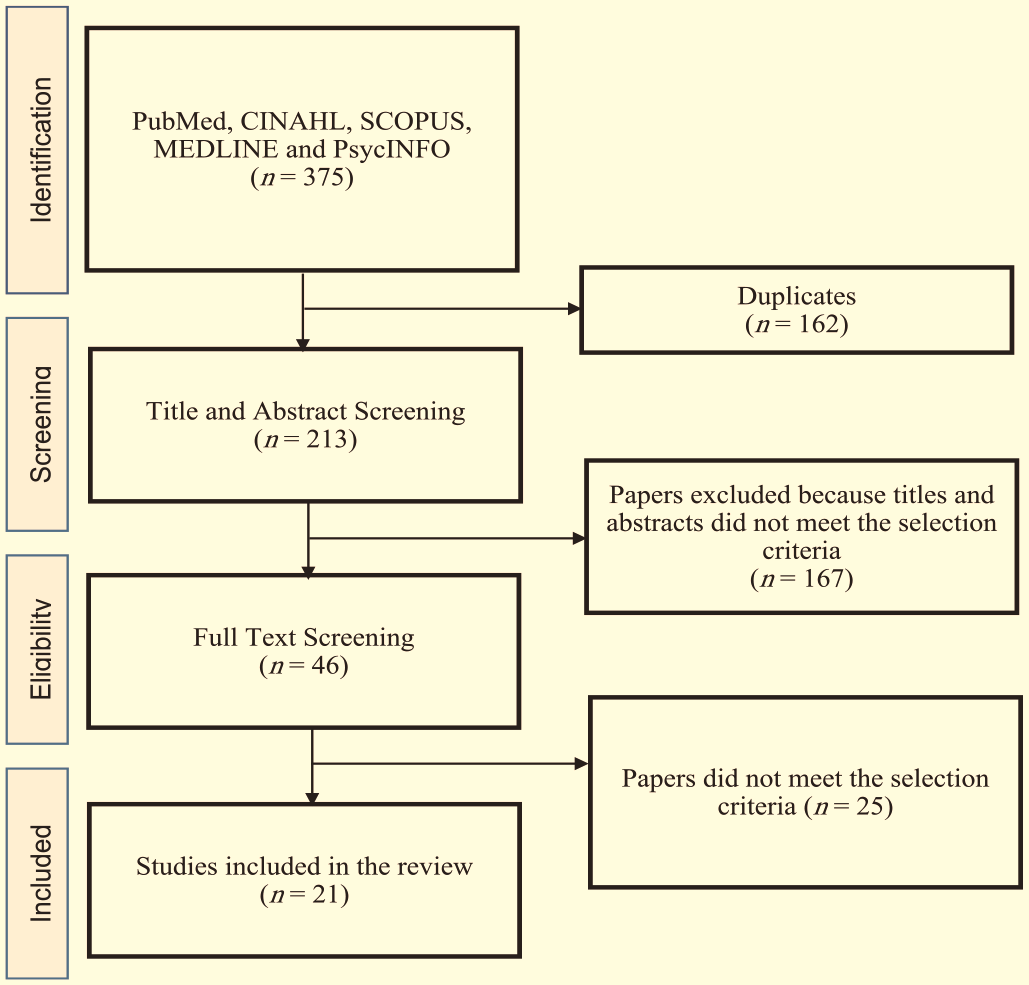
Diagram of the process used to identify references for the review.
Study Characteristics
The systematic review included a total of 21 studies, with varying geographic distribution. Four studies were conducted in China, while three studies each were conducted in Pakistan, Egypt, the United States, Australia, Taiwan, and Canada. In addition, one study each was conducted in Malaysia, Ghana, Turkey, and Iran. Eighteen studies employed a cross-sectional research design, providing a snapshot of the relationship between abusive supervision and its outcomes. In three studies, a two-wave cross-lagged panel design was utilized, allowing for the examination of causal relationships over time. The sample sizes across the studies ranged from 171 to 1221 nurses, representing a diverse range of participants. In terms of measurement, all studies utilized the Abusive Supervision Scale, originally developed by Tepper, 10 to assess nonphysical abusive behaviors exhibited by managers. Among the studies, 18 used the original 15-item scale, while two studies used a five-item version and one study used an eight-item version of the scale.
Quality Rating
Quality appraisal identified 13 studies with moderate quality scores, and eight with high quality scores. Quality appraisal was conducted by the two researchers independently; however, when disagreement arose, both researchers discussed the evaluation. Quality ratings were not used as a basis to exclude articles from the review. The focus was to capture as much relevant information and evidence as possible, given the existing literature landscape on the topic (Supplementary File 1).
Theoretical/Conceptual Framework
Of the 21 articles reviewed, only five used a theoretical basis to guide the research, while the remaining studies used varied conceptual frameworks to illustrate the interaction between the key study variables. Three studies utilized the conservation of resources (COR) theory as the theoretical underpinning,25,26,47 one study used the SDT, 43 and one study used the SLT. 39
Abusive Supervision Outcomes
Content analysis revealed 29 outcomes, which were categorized into six clusters: (a) affective-based, (b) behavior/performance-based, (c) relationship-based, (d) cognitive-based, (e) health and well-being, and (d) nursing care.
Affective-based outcomes
Affective-based outcomes of abusive leadership refer to the emotional or affective responses experienced by individuals who are subjected to abusive supervision. In this review, 11 studies reported four affective-based outcomes, including turnover intention, job satisfaction, work engagement, and public service motivation. Turnover intention was the most frequently tested outcome and was reported in five studies.13,28,39,40,45 In these studies, abusive supervision was associated with a higher turnover intention among nurses. Four studies attributed increased job dissatisfaction to a higher perception of abusive supervision.29,40,43,45 Other studies associated abusive supervision with decreased work engagement,38,46 but not with public service motivation. 43
Behavior/performance-based outcomes
Performance-based outcomes of abusive leadership refer to the effects of abusive supervision on employees’ job performance and work-related behaviors. In this review, five studies reported four behavior/performance-based outcomes of abusive supervision. In three studies,35-37 abusive supervision was significantly but positively associated with counterproductive work behavior in nurses. In addition, abusive supervision was attributed to increased job neglect, 42 poor work performance, 40 and decreased organizational citizenship behavior. 36
Relationship-based outcomes
Relationship-based outcomes of abusive leadership refer to the effects and consequences of abusive supervision on the relationships between leaders and their subordinates. Across six studies, four relationship-based outcomes of abusive supervision were identified. Workplace violence was highlighted as a significant outcome in two studies.11,39 The findings of a Turkish study indicated that abusive behaviors exhibited by nurse managers were associated with increased workplace incivility and ostracism. 39 Moreover, abusive supervision was linked to workplace injustice, 37 workplace bullying, 43 and an unsafe work climate. 24
Cognitive-based outcomes
Cognitive-based outcomes of abusive leadership pertain to the effects of abusive supervision on the cognitive processes, perceptions, and beliefs of individuals within a work environment. Four studies identified four cognitive-based outcomes of abusive supervision. Among them, two studies reported a significant decrease in moral courage among nurses who worked with abusive nurse managers.34,41 Sun et al 46 demonstrated a significant negative influence of abusive supervision on nurses’ self-efficacy, while Mostaf 41 reported a negative effect of abusive supervision on nurses’ moral efficacy. However, one study found no effect of abusive supervision on role ambiguity. 44
Health and well-being outcomes
Health and well-being outcomes of abusive leadership refer to the effects that abusive supervision has on the physical, psychological, and social well-being of employees, specifically in the context of their health-related outcomes. Seven studies examined the outcomes of abusive supervision related to health and well-being, identifying nine key outcomes. Specifically, three studies highlighted the significant impact of abusive supervision on the psychological health and well-being of nurses.24-26 Two studies each reported a correlation between abusive behaviors of nurse managers and increased emotional exhaustion42,45 as well as psychological strain.26,45 In addition, several studies found associations between abusive supervision and increased anxiety, 40 depression, 40 and mental health risks. 44 Poorer physical well-being26,40 and social well-being 26 were also identified as significant outcomes of abusive supervision.
Nursing care outcomes
The outcomes of abusive supervision related to patient care were reported in two studies. Lavoie-Tremblay et al 13 and Sharif Nia et al 29 found a significant and negative association between abusive supervision and nurse-assessed quality of nursing care. These findings suggest that exposure to an abusive nurse manager may have an impact on the delivery of quality, safe, and effective nursing care to patients.
Abusive supervision mediators
Ten mediators were identified in this review, which were categorized into three clusters: (a) affective-based, (b) motivation-based, and (c) health and well-being.
Affective-based mediators
Job satisfaction was the most frequently tested affective-based mediator between abusive supervision and the four nurse-related outcomes. Job satisfaction had a partial mediating influence on the association between abusive supervision and turnover intention 45 and public service motivation. 43 In other words, nurses who experienced abusive supervision were more likely to have lower job satisfaction, which, in turn, increased their intention to leave their job and negatively affected their motivation to serve the public. However, job satisfaction did not mediate the relationship between abusive supervision and work engagement, as indicated by Osei et al. 38 Although abusive supervision may negatively impact work engagement among nurses, job satisfaction may not be the mechanism through which this relationship operates. Sharif Nia et al 29 found that job satisfaction acted as a pathway between abusive supervision and nursing care quality, suggesting that nurses who experienced abusive supervision may have lower job satisfaction, which subsequently affected the quality of care they provided.
Motivation-based mediators
Three studies in this review reported motivation-based mediators that linked abusive supervision to three outcomes: turnover intention, work engagement, and counterproductive work behavior. Low et al 37 found that workplace injustice partially mediated the association between abusive supervision and counterproductive work behavior. This implied that nurses who experienced abusive supervision were more likely to perceive workplace injustice, which, in turn, increased their engagement in counterproductive work behaviors. Similarly, Özkan 39 found that workplace incivility, ostracism, and bullying acted as mediators between abusive leadership and turnover intention. Nurses who experienced abusive leadership may also have encountered workplace mistreatment, such as incivility, ostracism, and bullying, which then contributed to their intention to leave the organization. However, Osei et al 38 found that silence behavior did not mediate the relationship between abusive supervision and work engagement. Although nurses may have chosen to remain silent in response to abusive supervision, it may not have directly affected their level of work engagement.
Health and well-being mediators
Six studies in this review reported mediators related to health and well-being, including anxiety, psychological distress, and emotional exhaustion. Anxiety was found to be a mediator between abusive supervision and job satisfaction, 45 work performance, 45 and workplace ability. 11 Nurses who experienced abusive supervision were more likely to experience higher levels of anxiety, which in turn negatively impacted their job satisfaction, work performance, and overall ability to function effectively in the workplace. Pyc et al 40 also found that anxiety partially mediated the relationship between abusive supervision and emotional exhaustion, physical symptoms, and turnover intention. This indicates that abusive supervision may contribute to increased anxiety levels, which then lead to higher levels of emotional exhaustion, physical symptoms, and a greater likelihood of considering leaving the organization. In other studies, occupational stress was identified as a mediator between abusive supervision and physical, social, and psychological well-being 26 and turnover intention. 45 Nurses who experienced abusive supervision may also experience higher levels of occupational stress, which can negatively impact their overall well-being and increase their intention to leave the organization. Emotional exhaustion was found to mediate the association between abusive supervision and feedback avoidance 47 and job neglect. 42 Nurses who experienced abusive supervision were more likely to experience emotional exhaustion, which then led to avoidance of feedback and neglect of job responsibilities.
Discussion
Numerous reviews in nursing have been conducted to illustrate the association between effective leadership (e.g. ethical, authentic, and transformational) and nurse-related and patient safety outcomes.6,7 However, to the best of our knowledge this systematic review represents the first comprehensive synthesis of literature on abusive supervision specifically in the nursing field. The findings of this review offer valuable insights that can greatly assist hospital and nursing administrators in formulating effective strategies aimed at enhancing the leadership competence of nurse managers. Furthermore, these findings can inform the development of targeted programs aimed at improving work productivity, enhancing the health and well-being of nursing staff, and promoting higher levels of staff retention. In general, the findings of this review suggest that abusive supervision could result in multiple dysfunctional consequences for nurses. These findings provide additional support to research conducted in nursing28,39 and nonnursing sectors,9,48 showing that a leader’s abusive behavior may have motivational, relational, cognitive/social-cognitive, and affective impacts on subordinates.
The concept of supervision in leadership involves the behaviors exhibited by leaders, which have an impact on outcomes that are not directly connected to those behaviors. Instead, these outcomes are influenced by intermediate variables known as mediators. In other words, the actions and behaviors of leaders have an indirect effect on distal outcomes through the involvement of proximate variables or mediators. 11 Prior studies in other disciplines have identified a myriad of mediators (e.g. affective, motivational, and behavioral) that could explain how a leader’s abusive behavior leads to dysfunctional outcomes in workers. 48 This review found that the most frequently assessed mediators were affective (e.g. job satisfaction), motivational (e.g. workplace incivility), and health-related (e.g. psychological strain) in nature, consistent with earlier reports.49,50 Based on our findings, we developed a model (Figure 2) illustrating the interaction between the mediators and outcomes of abusive supervision, which could be applied in nursing and healthcare.
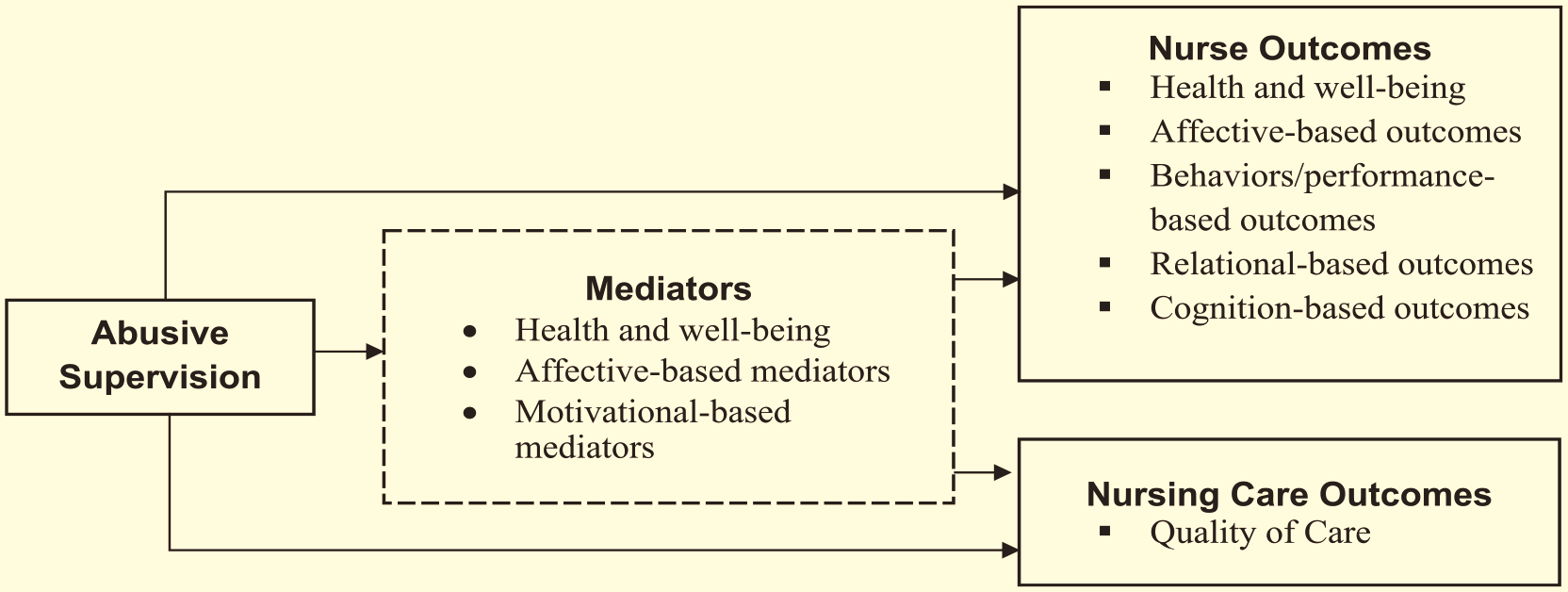
Synthesis of the review findings.
This review has identified several limitations that could have implications for future research on abusive supervision. First, a limited number of studies have provided well-grounded theoretical frameworks to help explain the association between abusive supervision and a broad range of nurse-related outcomes and mediators. Interestingly, only four studies25,26,39,47 provided a theoretical basis, which is partly attributed to the lack of a specific theory explaining how abusive supervision occurs. Having a well-grounded theoretical basis is useful as it can guide researchers in interpreting and analyzing results effectively. Meanwhile, given the dynamic nature of abusive leadership and its associated constructs, using a more rigorous research design, such as a longitudinal design, could provide clearer and more meaningful results. Most of the studies reviewed used nonprobability sampling, and future studies should employ probability sampling methods, which could yield more valid and generalizable findings. Although Tepper’s 10 scale has been widely tested across professions and found to be highly valid and reliable in assessing abusive supervision, developing a scale specific to nursing may generate results that best reflect the unique nature and behaviors of nurse managers/leaders. Finally, it is worth noting that the majority of studies included in this review originated from non-Western countries. This is significant because cultural and contextual factors can influence the expectations and perceptions of nursing practice and what constitutes an abusive work setting. Different countries may have distinct cultural norms, power dynamics, and organizational structures that shape their understanding of workplace abuse. Therefore, the concept of abusive supervision may be interpreted differently in non-Western contexts, reflecting the unique cultural and societal values prevalent in those countries. This highlights the importance of considering cultural variations when studying and addressing abusive supervision in nursing practice, as interventions and strategies may need to be tailored to specific cultural contexts to effectively mitigate its negative impacts.
Limitations of the Review
The interpretation of this review’s findings should take into account several potential limitations. The exclusive reliance on studies published in English could introduce publication bias, possibly excluding pertinent research in other languages and thereby affecting the overall comprehensiveness of the synthesized literature. While the deliberate focus on abusive supervision in the nursing field serves a clear purpose, it could inadvertently limit the examination of abusive leadership dynamics within broader healthcare contexts, potentially constraining the generalizability of the findings. In addition, the limited number of studies investigating the correlation between abusive supervision and patient safety outcomes might curtail a comprehensive understanding of the potential ramifications of abusive leadership on patient care. Notably, the absence of longitudinal studies in the review might impede the establishment of causal relationships between abusive supervision and outcomes pertinent to nurses. The existence of variations in how workplace abuse is defined across diverse cultural contexts could potentially restrict the applicability of the findings on a universal scale. Although the review hints at possible implications for strategies aimed at mitigating the adverse effects of abusive supervision, it lacks specific insights into the formulation of such strategies. Finally, the review’s emphasis on affective, motivational, and health-related mediators could inadvertently overshadow other potential mediators, emphasizing the necessity for a more comprehensive exploration of this aspect.
Relevance to Nursing Practice
The overall findings of this systematic review suggest that promoting positive leadership and behaviors among nurse managers can be an effective strategy for enhancing nurses’ work satisfaction, productivity, and retention, ultimately leading to improved nursing care quality. Addressing abusive supervision in the workplace requires a multifaceted approach that can be categorized into three levels of prevention. 8 At the first level of prevention, it is important to implement rigorous screening processes for potential abusive behaviors in nurse or nurse manager candidates, conduct thorough background checks to identify any history of hostile behaviors, and regularly assess the leadership and behaviors of nurse managers. In addition, establishing clear organizational policies that outline expected behaviors of nursing staff is crucial. 51 The second level of prevention involves providing relevant training programs to enhance the behaviors of nurse managers, including anger management, sensitivity training, and emotional intelligence programs. It is also important to offer counseling sessions, stress management programs, and strategies for coping and building resilience for nurses who have been exposed to abusive behaviors.13,29 The third level of prevention focuses on changing the behaviors of nurse managers and providing leadership competency training programs based on theoretical frameworks. Extensive research has highlighted the significance of leadership and management development programs in promoting positive leadership and behaviors among nurse managers, as well as their potential in reducing abusive behaviors or management styles.7,52 Other strategies that have shown significant improvements in leader behaviors and management styles include simulation-based activities for management and leadership, leadership mentoring, and leadership certifications.12,53,54
Conclusions
With the current shortage of qualified nurses and the challenges in retaining skilled and experienced nursing staff, the promotion of positive leadership and behaviors among nurse managers has become increasingly crucial in organizations. The results of this systematic review provided compelling evidence of the detrimental consequences associated with abusive supervision in the nursing workforce. Furthermore, the review highlighted the pathways through which abusive supervision impacts various nurse-related and patient safety outcomes. The findings emphasized the significance of developing a cohort of nurse leaders and managers who possess the skills to effectively lead and manage a nursing workforce dedicated to delivering safe and high-quality nursing care. However, despite the growing body of evidence linking abusive behaviors of nurse managers to a wide range of outcomes in nurses, there remains a scarcity of studies examining how such behaviors may affect patient safety outcomes. To address this research gap, future studies should focus on exploring the impact of abusive supervision on patient safety outcomes.
Supplemental Material
sj-docx-1-wjn-10.1177_01939459231212402 – Supplemental material for Abusive Supervision and Its Relationship With Nursing Workforce and Patient Safety Outcomes: A Systematic Review
Supplemental material, sj-docx-1-wjn-10.1177_01939459231212402 for Abusive Supervision and Its Relationship With Nursing Workforce and Patient Safety Outcomes: A Systematic Review by Leodoro J. Labrague in Western Journal of Nursing Research
Footnotes
Acknowledgements
The expertise of Dr. Claire Kirmas is acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Clearance
This review study does not require ethical approval since human samples were included.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.