
Abstract
Background:
Midlife Black women suffer disproportionately from cardiovascular disease and are 65% more likely to die following a cardiac event compared with White women. Recruitment and retention of midlife Black women in clinical trials has been historically low. The culturally tailored Midlife Black Women’s Stress Reduction and Wellness (B-SWELL) intervention was codeveloped with the community and designed to lower cardiovascular disease risk in midlife Black women.
Objectives:
We sought to assess participant satisfaction in the randomized feasibility trial of the B-SWELL intervention.
Methods:
A feasibility trial comparing the B-SWELL to a wellness intervention was conducted in the winter and spring of 2021 in compliance with pandemic research protocols. An adapted survey tool was used to rate satisfaction with the intervention and its technology using a Likert-type scale (1 [strongly disagree] to 5 [strongly agree]). Survey subscales assessed usefulness, ease, and acceptability of the intervention(s).
Results:
Randomization yielded no statistical demographic differences (N = 48). Satisfaction for the interventions was high in both the B-SWELL and Wellness intervention groups with mean scores of 4.57 and 4.56, respectively. Mean scores for technology were 4.49 for the B-SWELL and 4.47 for the Wellness group. Subscales were also rated highly. Narrative responses were positively aligned with satisfaction scores.
Conclusions:
Results support use of cultural adaptation and community participatory methods to develop and deliver interventions targeted to at-risk populations. Culturally adapted interventions designed in collaboration with the community have greater authenticity, increasing the potential for higher recruitment, retention, and participant satisfaction of underrepresented populations. The trial is registered in ClinicalTrials.gov (NCT 04404478).
Keywords
Cardiovascular disease (CVD) is the leading cause of death for all groups, yet Black women develop CVD at a younger age and midlife Black women ages 45 to 64 years are 65% more likely to die of CVD-related causes compared with White women of similar age. 1 Cardiovascular disease outcomes are compounded by upstream factors, individual characteristics, and comorbid conditions such as hypertension and obesity that drive the incidence and severity of heart disease in this high-risk population. 1 It is estimated that approximately 50% of Black women have heart disease, yet they are less likely to receive adequate preventive care and little more than 36% are aware that CVD is their greatest health risk.2,3
Tailored and targeted interventions are recommended to increase awareness of CVD risk and promote preventive behaviors in this at-risk subpopulation of women.4,5 Recruitment and retention of Black women in research studies have been historically inadequate.6,7 Thus, there has been a recent push to include midlife Black women in research studies to deepen our understanding of the factors affecting their health, preventive lifestyle behaviors, and overall wellbeing. For those studies that report success in the areas of recruitment and/or retention of midlife Black women, it is important to also publish measures of participant satisfaction.7,8 Such reports can provide insight for replication of interventions, inform intervention development, and aid future research intended to address health disparities impacting midlife Black women.
The purpose of this article is to describe satisfaction ratings for midlife Black women who participated virtually in the randomized feasibility pilot trial for the Midlife Black Women’s Stress Reduction and Wellness (B-SWELL) intervention. The B-SWELL is a theoretically based intervention designed to increase awareness and knowledge of CVD risk and promote adoption and adherence to healthy lifestyle behaviors.9,10 The intervention targets chronic stress, a known precursor for the inflammatory response that contributes to the development of heart disease and the adoption of unhealthy lifestyle behaviors. Following development, the B-SWELL materials and content were rated highly for content accuracy, topic relevance, stress relevance, cultural appropriateness, feasibility, usefulness, ease of use, and appeal by experts (details described elsewhere). 10 Satisfaction is particularly important to document when assessing feasibility of interventions tailored and targeted to at-risk groups. Satisfaction is often associated with quality, although it is more accurately a reflection of how well a program or intervention met the expectations of the participant, validating the design and providing insight into areas in need of improvement. 11 High satisfaction conveys confidence in the program structure, format, relevance, and content that may support continued use, development, or expansion. 12 As technology advances and we continue to explore novel ways to deliver interventions to underserved and at-risk communities, the inclusion of measures of satisfaction remains important.
Methods
A mixed methods approach was used to assess participant satisfaction in the B-SWELL randomized feasibility trial. The culturally tailored intervention was piloted in the winter of 2021. Midlife Black women between the ages of 40 and 64 years were recruited from a large Midwestern metropolitan area. There were no exclusion criteria, except that which precluded women from full engagement in the study. A sample size of 50 was proposed for this study to assess outcome data trends (details reported elsewhere). 9 After written informed consent was obtained, eligible women were enrolled and randomized using a computer-generated algorithm to the B-SWELL intervention or the Wellness intervention. 9 Following randomization, participants received a study binder (B-SWELL or Wellness) and a Fire HD tablet loaded with the appropriate group content to aid participation in the virtual Zoom sessions. B-SWELL and Wellness participants attended 90-minute weekly virtual sessions for 8 weeks and partook in 3 data collection phone calls: at baseline (before the trial), 8 weeks (at completion of the intervention), and 12 weeks (4 weeks postintervention). Data collectors were blinded to participant groups and had no other contact with participants aside from the data collection calls. The trial was registered in ClinicalTrials.gov (NCT 04404478). Details of recruitment, retention, and primary outcome data trends have been published elsewhere.9,10 All activities were approved by the University of Cincinnati Institutional Review Board (2019-0426) prior to the start of the study.
Interventions
B-SWELL intervention
B-SWELL participants received a binder and Fire HD 8 tablet containing culturally tailored information about CVD, stress, stress reduction, healthy lifestyle behaviors as described by the American Heart Association’s Life’s Simple 7, online and community heart healthy resources (eg, exercise or nutrition apps, meal prep, local gyms, books), and goal setting guidelines. Links to online Life’s Simple 7 resources were also provided. The 90-minute B-SWELL sessions included guided meditation, group discussions, case studies, goal setting instruction, and interactive demonstrations for stress reduction.9,10
Wellness comparison group
Participants in the Wellness group received culturally tailored content (hard copy binder and Fire HD 8 tablet) highlighting the Life’s Simple 7 healthy lifestyle behaviors and online resources but did not receive formal information or instruction about stress, stress reduction, or goal setting. 9 Similar to the B-SWELL, relevant community resources were also included.
Outcome Measures
Intervention satisfaction
The satisfaction survey used in this study was adapted from the Telephone Assessment and Skill-Building Kit (TASK) satisfaction rating scale created by Dr. T. Bakas to assess satisfaction of stroke caregivers participating in the novel TASK program. 13 The TASK satisfaction scale is comprised of 9 items and 3 subscales that assess usefulness, ease of use, and acceptability. The survey tool was adapted to measure the intervention and technology satisfaction for the B-SWELL feasibility trial in week 8, after completing the intervention. The B-SWELL satisfaction survey consisted of 9 statements (Table 1) and 3 short answer questions. Statements were rated on a Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree) with a total maximum satisfaction score of 45. Maximum score for individual items was 5. Items rated the materials, virtual sessions, and presentations on usefulness (4 items), ease of use (3 items), and acceptability (2 items). The short answer questions included (1) What did you like most about the program? (2) What can we do to make the program better?, and (3) Would you recommend the program to others?
Program Satisfaction.
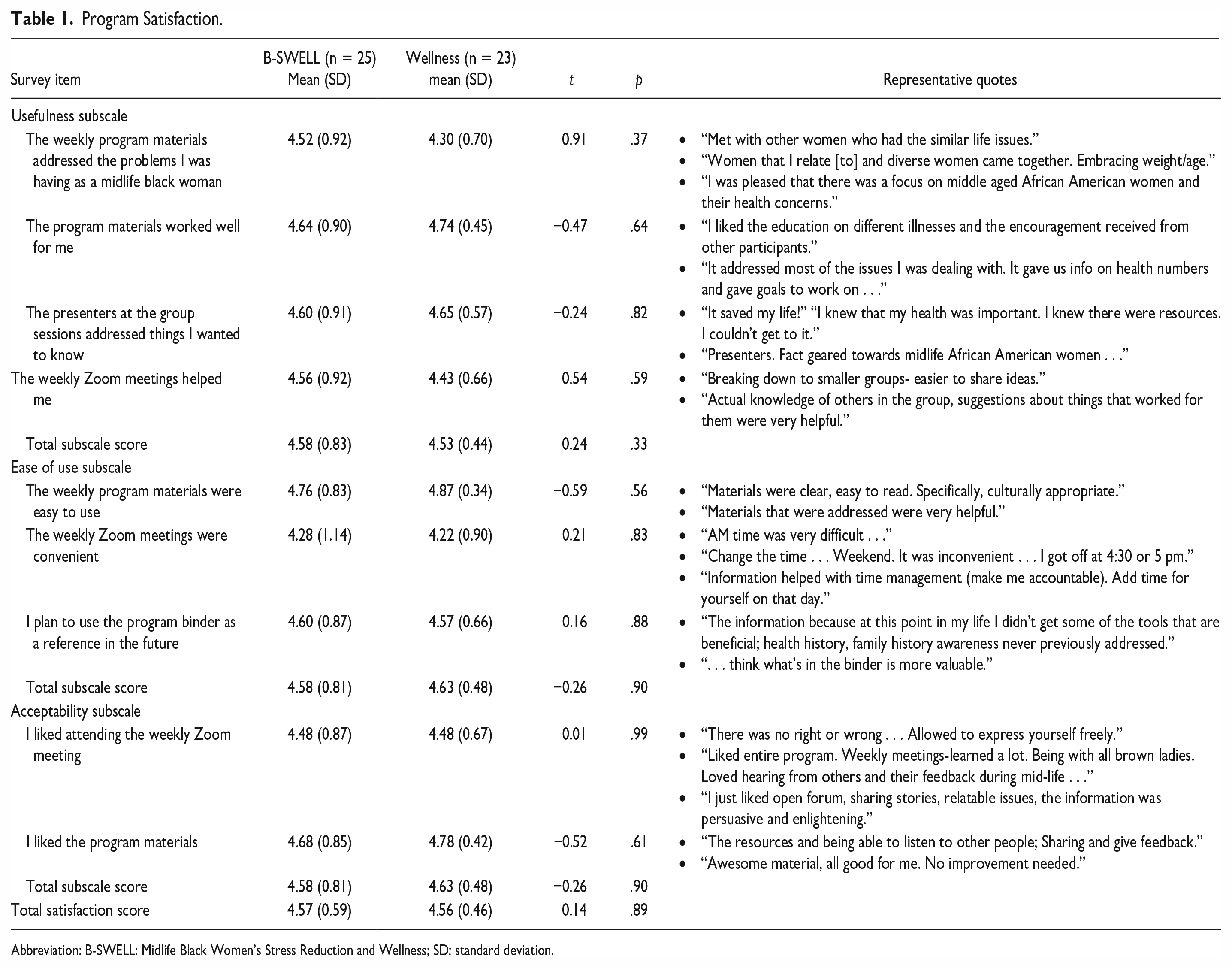
Abbreviation: B-SWELL: Midlife Black Women’s Stress Reduction and Wellness; SD: standard deviation.
Technology satisfaction
The B-SWELL technology survey (Table 2) consisted of 7 statements and 3 open-ended questions. Like the intervention satisfaction survey, statements were rated on a Likert-type scale ranging 1 (strongly disagree) to 5 (strongly agree) and categorized according to usefulness (3 items), ease of use (2 items), and acceptability (2 items). The short answer questions included (1) What suggestions do you have to make the tablet and Zoom experience better? (2) What do you like most about the tablet? and (3) What did you like most about Zoom?
Technology Satisfaction.
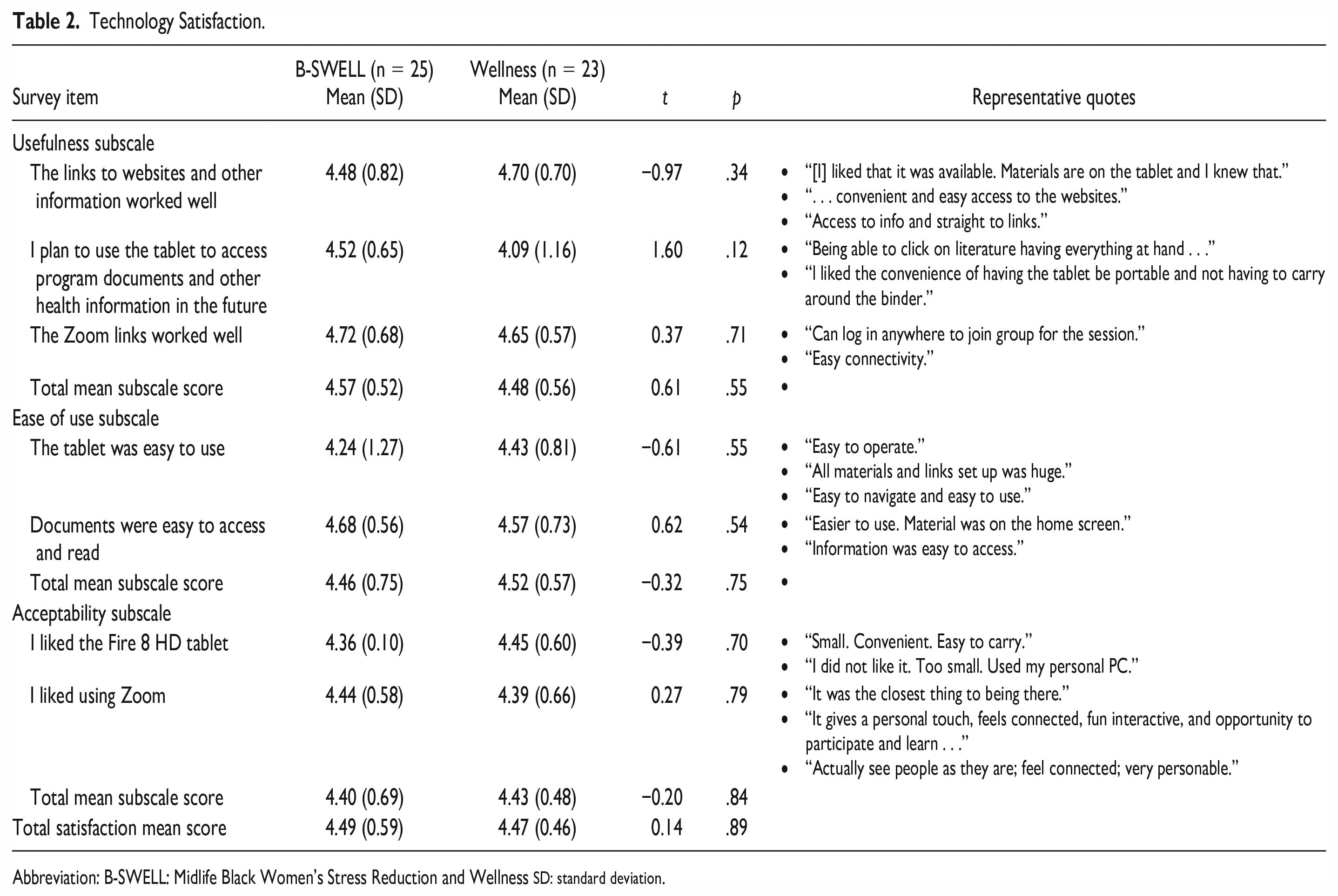
Abbreviation: B-SWELL: Midlife Black Women’s Stress Reduction and Wellness SD: standard deviation.
Data Analysis
Collected satisfaction survey data were checked and double checked for accuracy and errors. Data were then checked for normality, multicollinearity, and outliers. Group mean comparisons for satisfaction were assessed with independent t-tests. All statistical analyses were conducted using SPSS Version 28 (SPSS Inc, Chicago, Illinois). Qualitative responses from participants were coded and analyzed by 2 researchers using a simple thematic process, as described by Saldaña, 14 where responses are reviewed and categorized.
Results
Mean age was 56.2 years in the B-SWELL group (n = 25) and 53.3 years in the Wellness group (n = 23). There were no statistically significant demographic group differences at baseline for the final sample (N = 48). Demographic characteristics were previously reported. 9
Satisfaction
Satisfaction ratings were high for both the B-SWELL and Wellness participants. Total mean satisfaction scores for B-SWELL (4.57) and Wellness (4.56) participants were similar, t(46) = 0.14, p = .89. Individual items in the satisfaction survey also rated highly for both groups with a range of 4.22 to 4.87 (Table 1). The statement that received the lowest ratings from participants (mean scores = 4.28 [SD = 1.14] and 4.22 [SD = 0.90]) was “The weekly Zoom meetings were convenient” (Table 1). The question “What did you like most about the program?” elicited a wide array of responses including the following:
“[I liked] the guest speakers.”
“The sisterhood.”
“The comradery, support system, and having accountability.”
“. . . uplifting and [I] liked the women in the group.”
“Meeting women and establish friendship. Motivation for me to look at health and improve it.”
“. . . connection, feeling supported added to quality of life.”
Ideas related to sisterhood, comradery, and support were noted several times. Other favorable responses that frequently occurred referred to the culturally adapted materials and having a program specifically for midlife Black women.
The technology survey ratings were also high. Total satisfaction scores for technology used in the B-SWELL trial were similar for the B-SWELL (4.49) and Wellness (4.47) groups (t(46) = 0.14, p = .89; Table 2). Although ratings were high for both groups across all items, there were some notable group differences. For the B-SWELL group, the lowest ratings (4.24 [SD = 1.27]) were in response to the statement “The tablet was easy to use.” Comments related to weblinks, Zoom meetings, and the tablet were mixed but most referred to convenience, ease, and a sense of “feeling connected” (Table 2). Other responses about the Fire HD tablet and Zoom included “It was the closest thing to being there,” “I did not like it . . .,” and “It gives a personal touch . . . and opportunity to participate . . .”
Overwhelmingly, the participants were positive when asked if they would refer the program to others. Responses to the question “What suggestions do you have to make the program experience better?” were varied and constructive. Multiple women expressed a desire for time changes or specific days of the week, whereas others suggested longer sessions, in-person groups, and additional weeks in the program. Responses included the following:
“Add extra 30 mins to [breakout groups] to address concerns voiced by the group.”
“A follow up . . . getting everyone back together to see how we are doing.”
“Continue meeting once/month like a Facebook group.”
“I think the group should be held in person after [pandemic] situation is over.”
“Coaching to do physical activity.”
“Program was very helpful. No contact with anyone since then. Assigning a partner or peer person . . . Check on each other- possible build another connection.”
“Add topic: Dealing with children/elderly parents and grand kids. Caretaking in general.”
Discussion
The B-SWELL intervention was created to address the existing cardiovascular disparities experienced by midlife Black women and the paucity of interventions tailored to their needs. Results from the trial demonstrate high satisfaction for both the intervention and comparison groups. Despite the differences in content and materials received in the B-SWELL and Wellness group, both groups reported high satisfaction for the respective interventions and the technology used during the pandemic. Findings from this study demonstrate the importance of cultural adaptation and community participatory methods for recruitment and retention of midlife Black women and for subsequent satisfaction. In addition, the findings demonstrate acceptability of a virtual online group setting to deliver interventions targeted to midlife Black women.
These findings are significant given that Black women are historically under-represented in research and the literature suggests difficulty in recruitment and retention of this at-risk subgroup.15,16 Often research reports targeted to Black women do not report participant satisfaction but focus on recruitment and retention. Retention data may provide broad insight into general satisfaction but cannot replace investigation into specific areas of satisfaction. Satisfaction in our study was associated with feeling connected to women like themselves, receiving relevant culturally specific health information and receiving permission to perform self-care. The virtual format enabled participants to feel connected despite the limitations associated with the pandemic. In line with our findings, a prior study by Sheppard et al 17 noted that communication and familial support were important aspects of satisfaction for Black women.
Recent studies reported high participant satisfaction in programs designed to improve health-related outcomes in Black women.17,18 The theoretical basis 18 and use of community participatory methods 17 were credited with the success of the interventions and the participants’ satisfaction. Others reported high self-rated health satisfaction in Black women following program participation. 19 The B-SWELL is both theoretically and community-based. Short answer responses to the satisfaction survey in this study were generally positive and aligned with the satisfaction ratings.
Implications for Future Research
It was important to assess satisfaction of a virtual, community-based intervention conducted during the coronavirus pandemic as the use of technology and remote platforms have gained popularity. Representative members of a targeted population should be included when planning disease prevention interventions. We recommend that researchers determine how best to measure satisfaction for new interventions prior to a trial, taking into consideration mode(s) of delivery and the use of technology. The information gained may be crucial for successful delivery, receipt, and refinement of the intervention.
Limitations
The strengths associated with this study include the sound theoretical foundation and use of community participatory methods. Despite the strengths of the design and delivery, there were limitations. First, the small sample prohibited the ability to make inferences. Second, the coronavirus pandemic may have indirectly influenced satisfaction ratings as many participants were longing for social interaction. 20 For example, reports of depressive symptoms, concerns of isolation, and sadness in our sample of midlife Black women were similar to other reports in the general population during the pandemic. 9 Finally, findings from this study may not be generalizable to midlife Black women across the United States, although the preliminary research that supported development of the B-SWELL included midlife Black women from the San Francisco Bay Area in addition to those from the Midwest.21,22
Conclusions
Despite the existing disparities experienced by midlife Black women and recommendations for culturally tailored interventions, there remains a paucity of interventions intended to prevent chronic disease and promote healthier lifestyle behaviors for this vulnerable group. The successful trial of the B-SWELL intervention demonstrates the ability to recruit, retain, and engage midlife Black women in research and community-based programs. Methods used in this study resulted in high satisfaction for the program and its delivery methods. The use of mixed method techniques to conceptualize and develop appropriate interventions is encouraged to provide objective data while simultaneously giving voice to the population of interest. The rigorous approach used to create the B-SWELL intervention can serve as an exemplar to create appealing and culturally appropriate programs for at-risk groups.23,24 Furthermore, the high satisfaction ratings observed in this study support continued development of the B-SWELL as an intervention to lower CVD risk and CVD-related disparities among midlife Black women.
Footnotes
Acknowledgements
Members of the West End Community Research Advisory Board were instrumental in conducting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH) (K01HL141676); the University of Cincinnati College of Nursing’s Dean’s Research Award; NHLBI grant R25 HL105400 to Victor G. Davila-Roman and DC Rao; and the NIH Clinical and Translational Science Award program, Ohio (grant 2UL1TR001425).