
Abstract
Chronic illnesses among Korean immigrants (KIs) in the United States have been rapidly increasing, yet the concept of chronic disease self-care in this group has not been delineated. The aim of this study was to review previous research on self-care among KIs with chronic diseases and describe the concept in cultural context. Using Rodgers’ Evolutionary Method, a total of 24 articles were analyzed. The definition and conceptual model of self-care in KIs with chronic diseases were proposed. The antecedents included knowledge and health literacy; social and family support; resources; patient-health care provider partnership; and elimination of cultural misbeliefs and disclosure of the disease. The attributes of the concept were aging well with diseases; treatment adherence; control and restriction; the acculturation process; care built on traditional Korean gender roles; and maintenance of mental health. The consequences involved positive physiological outcomes; self-efficacy; quality of life; and reducing worry about becoming a burden to the family. While the studied concept encompassed universal characteristics of chronic disease self-care, distinctive cultural features emerged. The findings contribute to a better understanding of chronic illness self-care in this population and the development of culturally sensitive and practical self-care interventions for KIs with chronic diseases.
With the aging of the population, advancements in medical technology, and increase in life expectancy, the prevalence of chronic diseases has continued to increase, placing considerable health care and economic burden on individuals and countries.1,2 Self-care has been recognized as the mainstay of successful chronic disease management and has drawn much attention from researchers and clinicians given its impact on health outcomes and quality of life. Ongoing research has shown that it is feasible to manage chronic disease symptoms and achieve the highest possible quality of life with appropriate treatment and self-care.3-5
Self-Care in Diverse Populations with Chronic Illnesses
According to Orem, self-care is goal-directed action gained by learning and behavioral feedback, which encompasses activities that help manage aspects affecting one’s life, health, and well-being by making changes in oneself or the environment. 6 Self-monitoring and self-management are frequently used interchangeably with self-care in the literature, as those terms also refer to activities taken by individuals to improve their health. 7 The use of these terms also varies among professional organizations with no clear definition of each.8,9 Overall, self-care for chronic diseases usually includes the acquisition of knowledge or skills, treatment adherence, symptom awareness, disease management, and using family support or community resources.10,11
Racial and ethnic differences are potential variables affecting chronic disease prevalence and mortality 12 and may influence chronic disease self-care. However, little is known about the concept of self-care in different racial and ethnic groups, despite its widespread use. Because chronic disease self-care encompasses a wide range of lifestyle behaviors that can be influenced by culture associated with race and ethnicity, the concept of self-care needs to be understood in the cultural context of a specific population group. With increasing diversity in the US population, this approach can assist in defining the scope and elements of self-care for various patients with chronic illness. It can also help develop self-care goals and practical strategies that all parties involved in health care (patients, health care providers, and researchers) understand. We hypothesized that a racial and ethnic group can exhibit particular self-care characteristics due to cultural differences, although some aspects of self-care are universal. Given that health care interventions should be based on an accurate understanding of the target population and prior theories, 13 establishing a conceptual model of self-care that considers a specific population and its cultural aspects would aid in developing and applying interventions to promote self-care and its effect on health.
Korean immigrants (KIs) represent the fifth-largest Asian minority group in the United States. 14 The population had increased by approximately 73% in 10 years, reaching around 1.9 million in 2020. 14 According to a study that analyzed data from the adult California Health Interview Survey, the prevalence of diabetes among KIs aged 50 and older with body mass index <30 kg/m2 was greater than that of non-Hispanic Caucasians (6.8% vs. 4.3%). 15 Moreover, although KIs rated their health as poorer than other Asian immigrant groups, their health care-seeking and health insurance rates were significantly lower. 16 Studies report that KIs are hesitant to seek health care due to a variety of reasons such as a lack of societal resources, financial restrictions, limited language proficiency, mistrust of the US health care system, or experience with Korea’s affordable medical insurance before immigration.17,18 These barriers to accessing medical care may result in unmet health care needs, diagnostic delays, or illness progression, all of which can lead to poor health outcomes, increased medical costs, and psychosocial isolation. 19
Culture is defined as the common norms, beliefs, and attitudes of an ethnic and racial group, which also influence an individual’s experience and outcome of diseases.20,21 Since Korean culture is strongly influenced by Confucianism, which values propriety, filial piety, and a sense of community, 22 it is vital to understand the chronic disease self-care performed by KIs living in a completely different Western culture in light of their original cultural background. Although research has been conducted intermittently but consistently to promote self-care in KIs with chronic diseases, self-care has been examined using various definitions and has not been fully explored in the Korean cultural context. It is also unclear how self-care in this population is conceptualized and understood. Therefore, this study aimed to investigate self-care in KIs with chronic illnesses while considering their cultural background.
Purpose
The purpose of this concept analysis was to review the existing research on self-care among KIs with chronic diseases and to identify and clarify the conceptual model considering their cultural aspects. A detailed understanding of the self-care concept in KIs with chronic diseases is necessary to enhance awareness and efforts to promote self-care in this population. Moreover, it would help determine the need to construct a culturally sensitive and effective self-care intervention for KIs with chronic diseases.
Methods
Rodgers’ Evolutionary Method 23 was used to analyze the concept of self-care in KIs with chronic diseases. Rodgers defines a concept as a cluster of attributes with its antecedents and consequences. 23 Concept analysis is a dynamic and objective process for identifying the current consensus on a concept and providing a basis for further development. 23 This study method can help discover and clarify the meaning of words within a disciplinary context, thereby forming the basis for generating theory, education, and practice. 24
The method of concept analysis entails the following steps: (1) identification of the concept including its historical context and conceptual evolution; (2) collection of an appropriate realm setting and data sources; (3) selection of relevant data from contextual backgrounds and related concepts; (4) the analysis and summary of the concept’s characteristics to identify the concept’s attributes, antecedents, and consequences; (5) identification of a concept example; and (6) identification of implications for further research. 23 This method shows how the concept has evolved and developed over time and helps to improve and sustain the discipline’s clarity and utility. 23 Given the maturity of the selected concept in this study, Rodgers’ evolutionary method was the best-suited methodology. 23
Data Selection
The literature sampling was initiated using the PubMed, CINAHL, and PsycINFO databases. To specify the direction and scope of the study, the researchers conducted a preliminary search using terms such as “Korean immigrant*,” or “Korean American*,” and reviewed the literature. The search query was completed for relevant articles by combining the MeSH terms “self-care” and “chronic disease” with the terms “Korean immigrant*,” “Korean American*,” “self-monitoring,” “self-management,” and “chronic illness*” within the title and abstract. Chronic diseases were not limited to any specific diseases. However, search results revealed that the majority of articles that satisfied the selection criteria focused on type 2 diabetes (T2DM) and hypertension (HTN). Therefore, an additional search was performed by combining the query with the terms “diabete*” and “hypertensi*” to verify the exhaustiveness of the initial search. After carrying out several searches, duplications were eliminated. Cancers were excluded since they differ from other chronic diseases in terms of disease progression and the nature of self-care and its scope.
Full-text articles published in the English language were screened. Additionally, purposive sampling was conducted to review grey literature and references in the selected articles. There were no limitations on the published year or method of the study. To support the selection process, the authors determined inclusion criteria questions as follows: (1) Does the article aim to address and/or clarify the concept of self-care in KIs with chronic diseases? (2) Does the article have the potential to describe the concept’s attributes, antecedents, and/or consequences? (3) Does the article describe related terms of the concept?
Initially, 109 articles were obtained from the databases, and 6 articles were purposively searched. A total of 98 titles and abstracts were reviewed after duplicate items were removed. All articles were available in full text, but those that did not meet the inclusion criteria were excluded. Finally, a total of 24 key articles were included in this concept analysis (Figure 1).
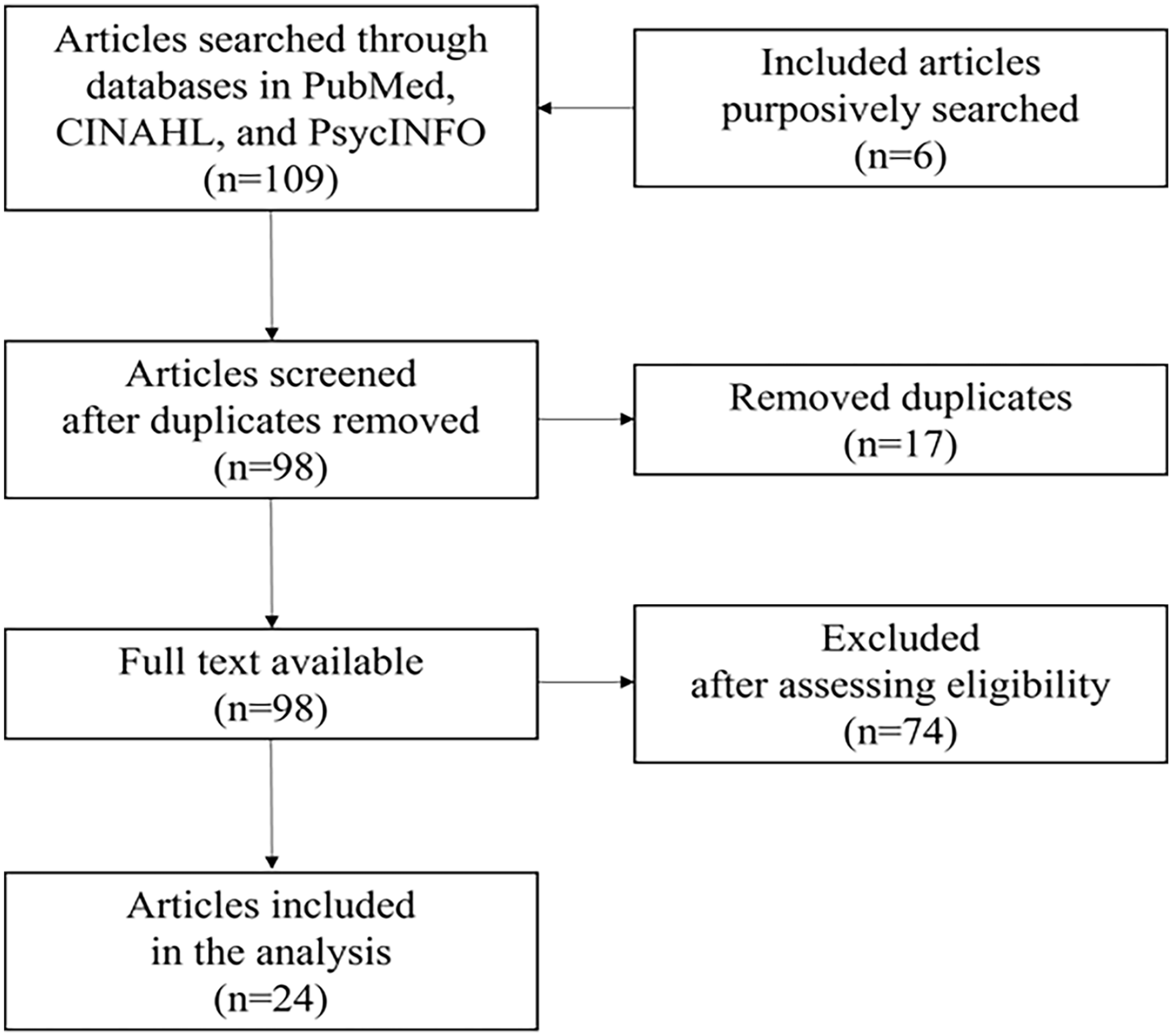
Flow Diagram of Literature Search.
Results
Summary of the Literature
The earliest article on self-care by KIs with chronic diseases was published in 2006 and the latest was in 2021. Of the 24 articles, 15 were on self-care for T2DM, and 6 were for HTN. There was one study dealing with both T2DM and HTN, one on chronic obstructive pulmonary disease and asthma, and one on chronic hepatitis B. Although all of the selected literature was for first-generation immigrants from Korea to the United States, the terms used for each study were slightly different: 8 articles used the term “Korean immigrants,” two used “Korean American immigrants,” and 14 articles used “Korean Americans.”
Definition of the Concept
The studied concept was defined based on the preceding analysis. Self-care among KIs with chronic disease is an ongoing process throughout one’s life involving multidimensional properties after a disease diagnosis. Specifically, as KIs age with chronic diseases in the United States, they strive to adhere to treatment, control their lifestyles, and maintain mental health, reconciling acculturation in the new culture while taking on a traditional Korean gender role.
Attributes
In total, 6 major attributes emerged from the 24 studies: (1) aging well with disease, (2) treatment adherence, (3) control and restriction, (4) the acculturation process, (5) care built on Korean traditional gender roles, and (6) maintaining mental health. Each of these attributes is discussed in detail below.
Aging well with disease
This is an important overarching component that can encompass the remaining attributes. Chronic diseases typically deteriorate as people age. However, the literature indicated that KIs with chronic diseases implemented better self-care as they got older.25,26 This may suggest that as the disease progresses, although additional self-care is required for KIs to maintain the desired level of physical and psychological condition, they accept that their disease is hardly treatable, and develop their own self-care routine based on what they had learned over the years about the disease. Moreover, as they get older and retire from work, KIs may have more time to take care of themselves. This characteristic demonstrates that self-care in KIs with chronic illness is a continuous process of adaptation and the individual’s health journey with the disease.
Treatment adherence
This attribute has observable and quantifiable features, such as regular medication intake, adherence to a prescribed diet or exercise program, and periodic blood pressure or blood sugar monitoring. As a result, the majority of the literature has defined this attribute as self-care.27-29 These characteristics also enable self-care to be identified as a behavior or activity. Based on this attribute, health care professionals can set achievable goals, develop educational interventions, measure outcomes, and encourage patients to improve this attribute. Additionally, treatment adherence showed a high potential to have a direct and positive impact on the consequences of self-care.
Control and restriction
Self-care for chronic illnesses inevitably entails this corresponding attribute. KIs make various life decisions to properly manage the symptoms of chronic diseases rather than their own preferences. 30 This may include not only ingredient selection and physical activity levels but also the scope of social activities. In particular, the literature has emphasized the patient’s self-doubt and the emotional burden associated with this attribute.31,32 Psychological distress occurs as a result of excessive restrictions, incorrect information, misbelief, or a lack of support. This essential attribute, which is also closely linked to antecedents and consequences of the concept, suggests that self-care in KIs with chronic diseases is a path to achieving balance.
The acculturation process
The fourth attribute of the studied concept is acculturation. The term acculturation is defined as “the dual process of cultural and psychological change that takes place as a result of contact between two or more cultural groups and their members.” 33 At the individual level, it involves modifications of a person’s behavioral routine and psychological changes occurring over time. 33 In this regard, self-care in KIs with chronic disease is embedded in the acculturation process. According to the literature, KIs remain in the active acculturation stage despite decades of living in the United States.31,34 For example, KIs stated that they needed to adapt by converting the units of measurement from Korean to American or taking an active role in their own treatment, trying to move away from the brief and passive communication patterns they used with Korean health care providers. This attribute shows that self-care in KIs is a process that produces changes in cultural and social behaviors. A self-care intervention that considered the patient’s degree of acculturation was effective in promoting self-care in KIs with chronic diseases.35,36
Care built on traditional Korean gender roles
This is a distinct attribute of self-care in KIs with chronic illnesses. As shown in the literature, KIs maintain traditional Korean gender roles influenced by Confucianism despite living in the United States. As a result, the sources of support for self-care that each gender required varied, as did the degree of support needed.37,38 For instance, KI men consider themselves responsible for the financial management of the household and defer most of their diabetes care to their spouses. 39 Meanwhile, most Korean wives stated that they were responsible for planning and preparing meals for the family, and they chose family preferences over their prescribed diabetes diet. This indicates the profound impact of traditional gender roles on self-care in KIs for chronic diseases. Comprehending the traditional gender roles in the Korean cultural context may help to uncover gender-specific factors that constitute and facilitate chronic disease self-care in KIs.
Maintenance of mental health
Self-care encompasses both the physical and mental aspects of health. Mental health was one of the major concerns for KIs with chronic illnesses. In the literature, psychological factors have been measured along with self-care in KIs with chronic diseases. In particular, levels of depression in KIs with T2DM were significantly higher than those found in other racial and ethical groups. 40 However, studies applying an intervention promoting self-care for chronic diseases revealed that the degree of depression among the participants lowered significantly.27,41 In addition, the KIs used emotion-focused strategies along with problem-focused strategies to cope with their chronic disease symptoms. 42 As the participants quoted the phrase “sound mind, sound body,” self-care in KIs incorporates multidimensional interactions between physical and mental health domains.
Model Case
Mrs Han, a 51-year-old woman, lives in Houston with her husband and two children. She immigrated to the United States, 17 years ago, and runs a laundry shop. She was diagnosed with T2DM 3 years ago, but on busy mornings she often forgets to check her blood sugar and take her medications. Finally, she realized she needed a different approach and put the glucometer and medication next to the refrigerator. This makes it possible to check her blood sugar and take her medications every morning as soon as she comes into the kitchen to prepare breakfast for her family. She also faces some challenges in maintaining her diet plan because the food recommended for her diabetic diet is unsatisfactory to the family. First, her husband insists on having white rice every meal, whereas multigrain or brown rice is recommended for patients with diabetes. Since she runs the shop with her husband and shares all their meals, she abandons her diabetic diet plan and prepares the meals with white rice to prevent conflict with her husband and save the trouble of cooking her own meals separately. In addition, her children’s favorite snacks are rice cakes and cupcakes. She always purchases them from the store, but it is frustrating not to be able to share them with the family due to her medical condition. To prepare homemade healthy snacks for the family to enjoy together, she decided to enroll in healthy baking classes. As she gained baking experience, she became acquainted with the ounce and Fahrenheit units, which she had never considered using previously. She learned how to make her own healthy bread by changing the sugar level and substituting whole wheat flour. The family enjoyed the healthy bread she made. She also convinced her husband to change to half and half white/brown rice for his health. Her glucose level improved and her emotional stress decreased. She plans to ask her physician on her next clinic visit to refer her to a nutritionist and diabetes educator for more education and information regarding her weight management.
This example case includes defining attributes. To solve the problem of forgetting her medications in her busy lifestyle, she creates new habits to manage her disease. This allows her to regularly take the prescribed medications and follow treatment regimens. Additionally, she can manage her blood sugar levels and mental wellness by learning to cook in a healthy way that follows the diabetes diet guidelines. While playing the Korean traditional mother and wife role, she is also assimilating into American culture by using American measuring units in cooking that she has not used before and proactively discussing her self-care plan with her health care provider rather than simply walking out of the clinic with prescriptions.
Antecedents
Five antecedents were identified from the selected literature. Antecedents are the preceding conditions of self-care.
Knowledge and health literacy were not only measured most frequently in the literature but also showed a high correlation with self-care. Educational interventions to enhance disease-specific knowledge lead to improvement in self-care. Health literacy is the ability of an individual to obtain, process, and understand basic health information and services necessary to make appropriate health decisions. 43 The effect of health literacy on self-care in KIs with chronic diseases has been considered in recent studies.29,44
Social and family support has been extensively studied along with self-care among KIs, who are considered a family and community-oriented group. Family and social support have been shown to improve self-care and health outcomes in KIs with T2DM. 37 Particularly, for this group with such strong collectivist values to promote self-care by using the more individualistic US health care system, a specific understanding of both is needed. 45
Resources include time, transportation, and financial circumstances that precede the ability to perform self-care for patients. Depending on the extent of available resources, the range of self-care that an individual can perform may vary. A striking feature related to KIs’ self-care resources in the literature was the low rate of health insurance. 44 Additionally, they looked for health care resources at the Korean community level in the United States. 34
Patient-health care provider partnership increases the quality and level of self-care among KIs with chronic illnesses. Moreover, the physical and emotional changes of self-care can be sustained through continuous and positive feedback and rewards from health care professionals. 41
Elimination of cultural misbeliefs and disclosure of the disease entails unique cultural aspects for KIs in dealing with the disease and preserving their social image (e.g., losing face, embarrassment). Some KIs also often concealed their illness, as they felt self-conscious about their family members’ reputations as well as their own. 46 Moreover, some of their traditional cultural views on “good” or “bad” food are inconsistent with dietary recommendations for particular chronic diseases. 30
Consequences
Consequences are the outcomes of self-care. Four consequences of self-care were identified from the selected literature as follows.
Positive physiological outcomes included improvement of blood pressure, HbA1c, total cholesterol, and/or body weight. These findings were observed along with the enhancement of self-care despite the application of the relatively short period of intervention.35,47
Self-efficacy is defined “as people’s beliefs about their capabilities to produce designated levels of performance.” 48 These psychological effects are usually accompanied by increased self-care activities in the literature.26,49 This can indicate that self-efficacy is not a prerequisite or requirement for self-care in KIs with chronic diseases but rather a characteristic after the experience of self-care or confirmation gained by performing it.
Quality of life in the reviewed studies was measured by concerns about the future or satisfaction with treatment. Improvement in quality of life was reported with better self-care in KIs with chronic illnesses. 50
Reducing worry about becoming a burden to the family is related to what patients want to achieve from adequate self-care for their chronic disease, 32 which could be a manifestation of distinct strong Korean cultural values.
Surrogate Terms and Related Concepts
Surrogate terms refer to the expressions or words used by researchers to explain the same concept. 23 In the reviewed literature, the terms “self-care” and “self-management” were used interchangeably. Another term, “self-help,” named after Braden’s self-help model, 51 was repeatedly used as the title of an intervention by one research team across several studies.28,50,52
While related concepts have common ideas with the concept, they do not share all of the associated attributes. 53 In this study, the concept of self-care was explored within specific patients in limited circumstances; that is, KIs with chronic illness living in the United States. Without these limitations, self-care generally has related concepts, such as self-monitoring, symptom management, disease management, and self-maintenance. 54 However, none of the reviewed literature made use of those phrases.
Discussion
This study comprised a comprehensive review of the literature on self-care in KIs with chronic diseases to ascertain the concept’s definition and characteristics. Based on this, a conceptual model of self-care in KIs with chronic diseases was proposed (Figure 2). Self-care is a concept with a long history that has been studied extensively. The authors postulated, however, that this concept might have distinct attributes when applied to a particular demographic or a set of health concerns. Thus, we believed that even if the concept of this study is limited to specific patients and situations, a conceptual model needed to be identified. As a result of this study, the concept was defined while taking cultural aspects into account. While Orem’s definition of self-care covers the studied concept broadly, 6 distinctive cultural characteristics were added to attributes, antecedents, and consequences, and these were incorporated into the definition.
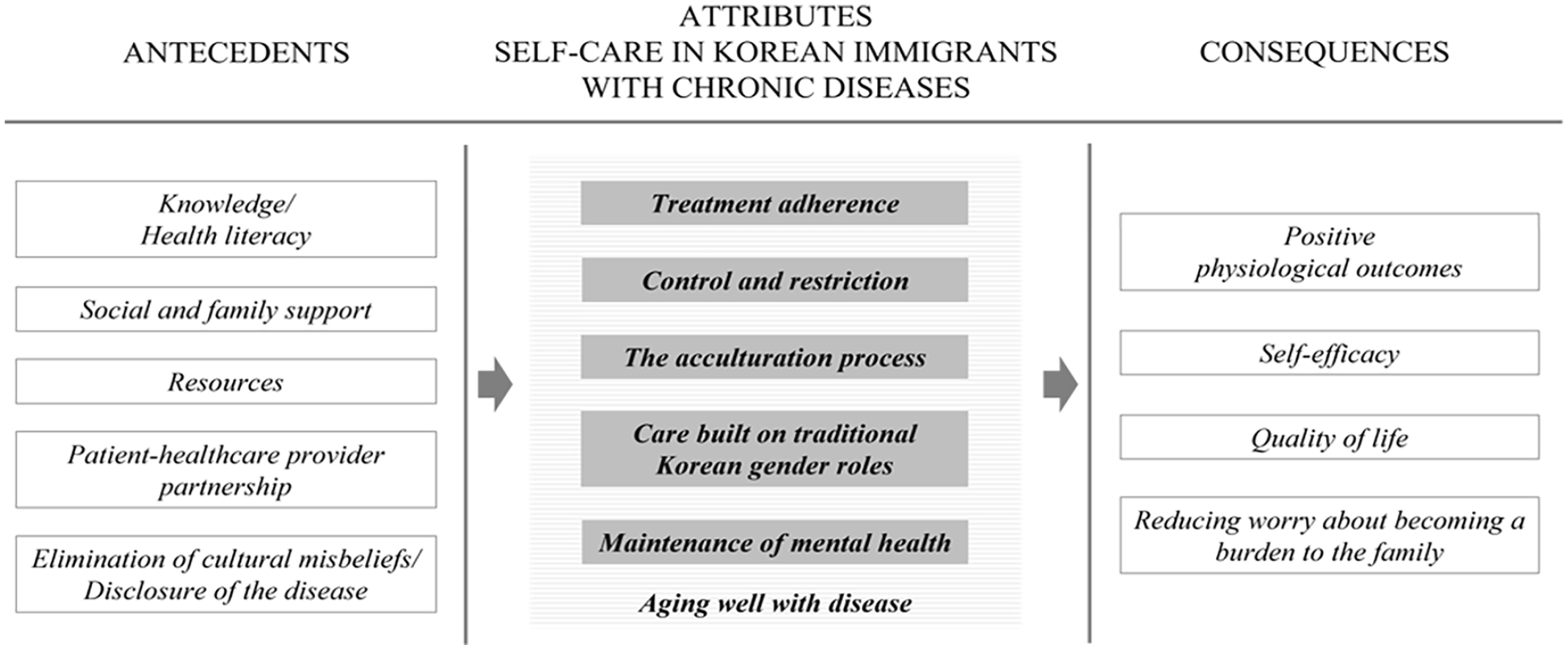
Conceptual Model of Self-Care in Korean Immigrants with Chronic Diseases.
In a previous concept analysis of chronic disease self-care, which did not target a specific ethnic and racial population, self-care was defined as continuous efforts to promote, control, and manage health at the individual, family, and community level with or without the advice of health care professionals. 5 In light of this definition, self-care in KIs with chronic diseases is much more focused on family. Moreover, self-care in KIs seems to be initiated and managed by health care providers. Therefore, readiness, an essential attribute of self-care 5 meaning that the patient is interested in their self-care activities and has the sufficient inner power to carry them out, does not correspond to any attributes of self-care in this study. This result is also distinct from other recent self-care studies that concentrate on patient-oriented attributes such as self-reliance and awareness.55,56
The familial traits observed in chronic illness self-care among KIs were also considered crucial in the diabetes self-management model of Chinese immigrants. 57 However, no gender-based differences in Chinese immigrants’ self-management were found, 57 contrary to the findings of this study. In addition, the study reported that Chinese culture stigmatized mental illness, viewing it as humiliating for themselves as well as their families and making them ashamed to seek therapy. 57 This result is comparable to that of this study; KIs conceal their chronic diseases to protect their and their family’s reputations. According to a study of self-care among African immigrants with noncommunicable diseases, respondents indicated that gym activities were not culturally acceptable, and being “fat” was viewed as a symbol of health. 58 KIs were reluctant to visit medical clinics or take medicines as they believed overcoming the condition without medication was preferable. 19 Thus, it is vital to recognize that some aspects of self-care in different groups encompass their cultural misbeliefs.
In addition to presenting a clear conceptual model, we identified several areas for future research on self-care in KIs with chronic disease. First, the literature on self-care in KIs with chronic diseases has concentrated primarily on T2DM and HTN. It is assumed that chronic diseases with a higher prevalence were studied to avoid small sample sizes. However, in light of the growing number of KIs, self-care research on a variety of chronic diseases is needed to identify any commonalities and differences between diseases. Second, some of the reviewed literature recruited the subjects from a specific religious community. This approach could have facilitated access to a large number of certain participants but may have also introduced a selection bias. As a result, it is necessary to establish a recruiting strategy that will enhance the generalizability of the research by including a varied sample of KIs.
While defining self-care in KIs, we realized that the term “Korean American” also needed to be defined explicitly in the health care field. In the literature, the terms “KIs,” “Korean American immigrants,” and “Korean Americans” have been used interchangeably to refer to the group of immigrants from Korea to the United States without a separate definition or explanation. However, as the number of people of Korean descent born in the United States continues to grow, the term “Korean American” becomes complicated when considered in the contexts and the interests it represents. 59 It may not be realistic or appropriate to group together individuals who have personally immigrated from Korea and those who have lived their entire lives in the United States. Moreover, Korean Americans of different generations may share different experiences and values. 60 Therefore, it is important to demarcate and separate the term based on the purpose and expected results of studies.
This study had some limitations. First, while a systematic search was conducted, it is possible that pertinent research might have been missed. To address this issue, researchers carried out repetitive and purposive searching. Although the amount of primary literature searched in the databases was less than the number of papers reviewed by other concept analyses, it was sufficient to support meaningful discussion because the scope of the concept to be studied was specific. Second, the patients in the reviewed literature were first-generation KIs from across the United States. Their self-care for chronic diseases may vary according to where they live in the United States, but the number of studies available to confirm geographic differences in self-care in this study was insufficient. Third, we were unable to include second-generation KIs due to no available literature on this group. Therefore, the findings of this study may be difficult to apply to the next generation of Korean Americans.
In this study, we analyzed the concept of self-care in KIs with chronic illness and identified the attributes, antecedents, and consequences in consideration of cultural values. These findings contribute to a better understanding of self-care of KIs with chronic diseases, providing information for research and practice that can lead to further studies and interventions for this underserved ethnic minority population. Based on the self-care conceptual model presented in this study, nurses and other health care professionals working with KIs with chronic illness may adopt a different perspective and apply appropriate motivating strategies for them. This model may help researchers conceptualize self-care of KIs with chronic disease and compare it to that of another racial and ethnical group or disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.