
Abstract
Our objective was to determine if past-year mental illness and substance use disorders (SUD) among pregnant smokers predicted the probability of receipt of counselling for cigarette smoking cessation. A secondary analysis of data from the National Survey on Drug Use and Health 2016–2019 was conducted. We found that approximately 83% of pregnant smokers (N = 373) received screening for cigarette smoking, and 65% received cessation counselling. Having mental illness predicted the probability of receipt of counselling for smoking cessation in pregnant smokers (adjusted odds ratio [AOR]: 3.75; 95% confidence interval [CI]: 1.25–11.27). However, having SUD (alcohol [AOR: 2.30; 95%CI: 0.57–9.26] or illicit drug use [AOR: 1.32; 95%CI: 0.26–6.82]) or comorbid mental illness and SUD (AOR: 0.23; 95%CI: 0.03–2.03) was not associated with receipt of counselling for smoking cessation. Practice guidelines and policy initiatives are needed to reduce cigarette use and its related adverse health outcomes in pregnant smokers with SUD.
Keywords
Prenatal cigarette use is a significant health issue due to the increased risk of perinatal complications, congenital malformations, miscarriages, and poorer neonatal/infant outcomes (U.S. Department of Health and Human Services, 2014). Based on national data, 9.6% of pregnant women reported past-month tobacco use in 2019 (Substance Abuse and Mental Health Services Administration [SAMHSA], 2020). Cigarette smoking is higher in pregnant women with mental illness (Salameh et al., 2021b; Tong et al., 2016) and substance use disorders (SUD) (Jarlenski et al., 2020) than in women without these disorders. Given their lower quit rates along with higher cigarette smoking rates (Salameh et al., 2021b; Tong et al., 2016) and the toll of cigarette smoking on the mother and her child, a better understanding of the receipt of counselling for cigarette smoking cessation in pregnant smokers with mental health and SUD is critical.
Counselling for Cigarette Smoking Cessation among Pregnant Smokers with Mental Illness and SUD
Trend studies show an increase in smoking rates among pregnant women with depression (Goodwin et al., 2017). This increase in smoking is in a reverse direction of the trend in smoking among the general population (Lawrence & Williams, 2015), reflecting the unmet needs of pregnant smokers with mental illness. Overall, there is less progress in meeting the needs of U.S. adult smokers with mental illness (Cook et al., 2014), particularly those with SUD (Shu & Cook, 2015). Over the past decade, there was an increase in SUD along with co-occurring cigarette use in pregnant women, especially in those with opioid use disorder (Jarlenski et al., 2020). Pregnant women with mental illness also are less likely to quit smoking than women without mental illness (Salameh et al., 2021b; Tong et al., 2016), indicating the urgency to meet their clinical needs.
The U.S Preventive Services Task Force (USPSTF, 2021) recommends that health care providers target smoking in pregnant women through screening for smoking and the provision of treatment for tobacco dependence. Recent medical recommendations for cigarette smoking cessation in pregnant women involve the provision of 5As (Ask, Advise, Assess, Assist, and Arrange) as an evidence-based intervention (American College of Obstetricians and Gynecologists [ACOG], 2020). A meta-analysis shows that compared to usual care, counselling interventions improved smoking cessation in late pregnancy when used as one component and in conjunction with other interventions such as health education (Chamberlain et al., 2017). Counselling involves interventions to support problem-solving skills and enhance motivation to quit smoking (Ortendahl et al., 2009). A cost-effectiveness analysis revealed that behavioral smoking cessation counselling targeting U.S. pregnant women is cost-effective and associated with fewer negative neonatal outcomes (e.g., stillbirth, preterm delivery, fetal growth restriction, and neonatal death) (Bacheller et al., 2021).
While pregnant women have greater contact with health care providers (Hollis et al., 2020) and thus more chances for smoking screening and counselling cessation, a majority of pregnant women with mental illness and SUDs are not receiving mental health and substance use treatment despite their needs (Salameh & Hall, 2020; Salameh et al., 2020, 2021a). Health care providers themselves have misconceptions about pregnant smokers with mental health and SUD such as cigarette smoking cessation that can affect the outcomes of mental health (Howard et al., 2013) and substance use treatment (Fallin et al., 2016), thus not prioritizing smoking cessation treatment (Howard et al., 2013).
Purpose
Evidence on the efficacy of counselling on cigarette smoking cessation is derived mainly from clinical samples of pregnant women (Chamberlain et al., 2017); there is sparse evidence about counselling among pregnant smokers with mental illness and SUDs. Therefore, the purpose of this study was to determine if past-year mental illness and SUD (i.e., illicit drug or alcohol use disorder) among pregnant smokers predict the probability of receipt of counselling for cigarette smoking cessation, controlling for potential confounders (i.e., age, race/ethnicity, marital status, education level, employment status, income, health insurance, self-rated health status, past-year receipt of mental health and substance use treatment, and smoking frequency).
Methods
Data Source
We used data from the 2016–2019 National Survey on Drug Use and Health (NSDUH), a nationally representative cross-sectional survey of household respondents in the United States (Center for Behavioral Health Statistics and Quality [CBHSQ], 2020). The NSDUH uses a multistage probability stratified sampling approach to collect data via computer-assisted interviews to address mental health and substance use issues. From 2016 to 2019, a total of 63,885 women aged 18–44 years responded to the NSDUH; 2,776 (4.3%) reported that they were pregnant at the survey time. Of pregnant women, there were 373 women who reported past-month cigarette smoking who comprised the sample of this study. Because we used publicly available de-identified data from the NSDUH, the study was exempt from Institutional Review Board approval.
Measures
Women respondents to the NSDUH reported their pregnancy status (yes vs. no); those who were pregnant indicated their trimester of pregnancy (first, second, or third trimester). Smoking status was measured via self-report of past-month cigarette use. The frequency of smoking was determined by a survey item addressing the number of days the respondents used cigarettes in the past month (1–5 days, 6–19 days, 20–29 days, 30 days). Screening of cigarette smoking use was measured with the survey item: “During the past 12 months, did any doctor or other health care professional ask, either in person or on a form, if you smoke cigarettes or use any other tobacco products?” (CBHSQ, 2020). Counselling of cigarette smoking cessation was measured via the following item: “During the past 12 months, did any doctor or other health care professional advise you to quit smoking cigarettes or quit using any other tobacco products?” (CBHSQ, 2020).
Mental illness in the NSDUH was measured as having any mental illness in the past year based on a statistical predictive model of responses to the Kessler Psychological Distress Scale (Kessler et al., 2003), World Health Organization Disability Assessment Schedule (Novak et al., 2010), past-year major depressive episode (MDE), and suicidal ideation. The questions in the NSDUH measuring MDE were originally derived from the Diagnostic and Statistical Manual of Mental Disorders (DSM) IV criteria (American Psychiatric Association [APA], 1994). Consistent with the definition of the DSM V criteria (APA, 2013), the NSDUH classifies individuals as having MDE in the past year if (a) they had a lifetime MDE, (b) felt depressed or lost pleasure or interest in daily activities for 2 weeks or longer in the past 12 months, and (c) reported having “some of other problems” during this period of 2 weeks or longer.
The NSDUH uses self-report questions derived from the DSM IV criteria (APA, 1994) to measure past-year SUD: alcohol or illicit drug dependence or abuse (CBHSQ, 2020). Past-year mental health treatment was defined as the receipt of inpatient or outpatient treatment or taking any medication for mental health issues. Past-year substance use treatment receipt was defined as the receipt of alcohol or drug use treatment at a special facility (CBHSQ, 2020). Appendix A in the online supplemental materials includes a detailed description of the measures of the main variables included in our study.
Sociodemographic variables included maternal age, marital status, race/ethnicity, level of education, household income, employment status, county urbanicity, and perceived health status (Table 1). Time was defined as the survey year and considered a covariate.
Characteristics of Pregnant Women Aged 18–44 Years by Current Cigarette Smoking Status and Receipt of Counselling for Smoking Cessation, NSDUH 2016–2019.
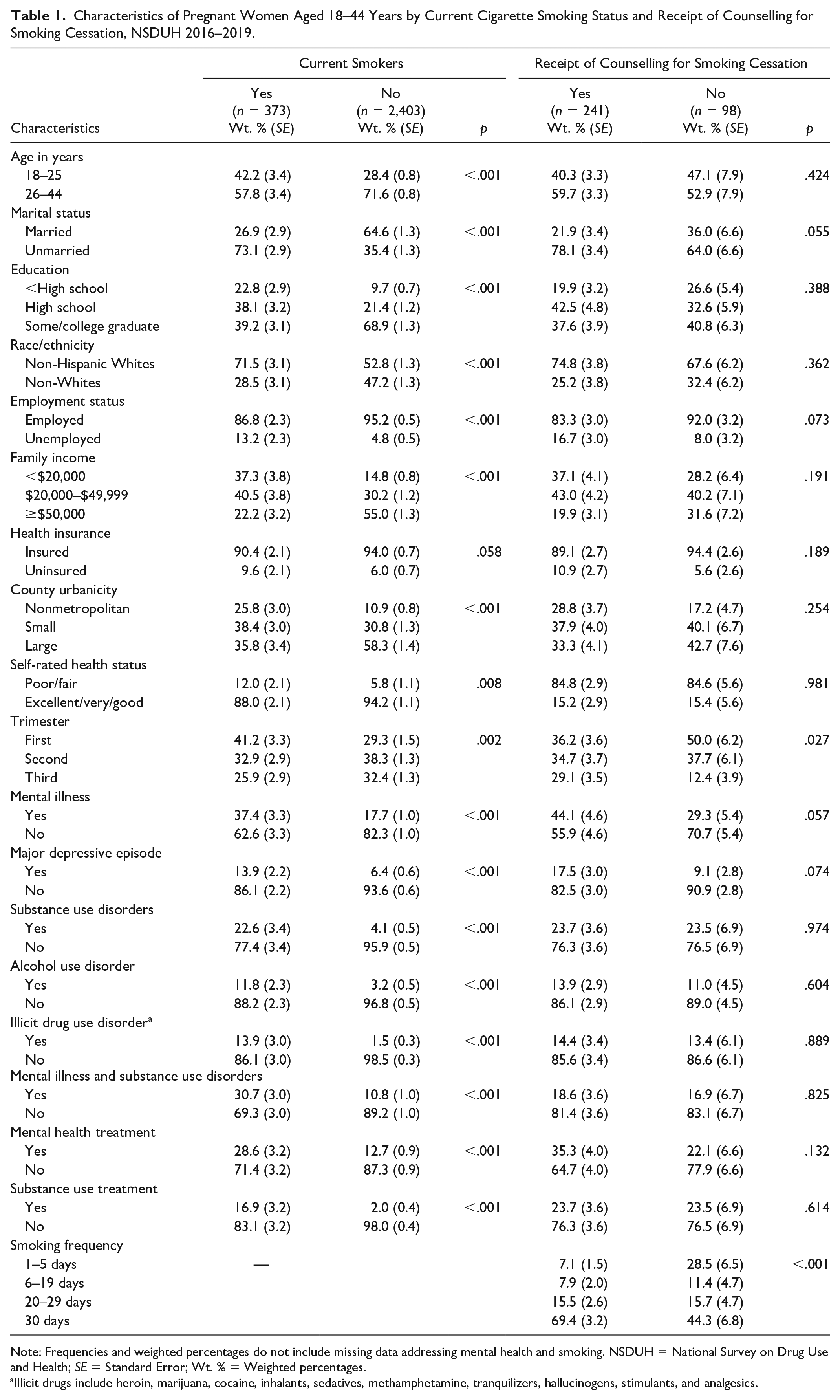
Note: Frequencies and weighted percentages do not include missing data addressing mental health and smoking. NSDUH = National Survey on Drug Use and Health; SE = Standard Error; Wt. % = Weighted percentages.
Illicit drugs include heroin, marijuana, cocaine, inhalants, sedatives, methamphetamine, tranquilizers, hallucinogens, stimulants, and analgesics.
Statistical Analysis
All statistical analyses were conducted using complex sample analysis with SPSS software, version 28.0 (IBM Corp., 2013). As data were pooled for four years, a weighting variable was created by dividing the final person-level analysis weights by four. Weighted percentages and standard errors (SE) were calculated to describe sociodemographic and clinical characteristics including mental illness, SUDs, and treatment receipt among pregnant women. The chi-square test for independence was conducted to compare the sociodemographic and clinical characteristics by smoking status in pregnant women and by receipt of smoking cessation counselling in pregnant smokers. In addition, the weighted percentages of the receipt of smoking cessation counselling were calculated and compared by trimester of pregnancy as stratified by type of disorder (i.e., mental illness and/or SUD). Multiple logistic regression was used to determine the probability of receipt of cigarette smoking cessation counselling among pregnant smokers conditional on past-year mental illness and/or SUD, controlling for time and confounding variables (i.e., age, race/ethnicity, marital status, education level, employment status, income, health insurance, self-rated health status, past-year receipt of mental health and substance use treatment, and smoking frequency). p-Values <.05 were considered statistically significant for all analyses.
Results
Participant Characteristics (Smokers vs. Nonsmokers)
From 2016 to 2019, 11.3% of pregnant women reported past-month cigarette use. Pregnant smokers compared to nonsmokers were more likely to be aged 18–25 years, unmarried, non-Hispanic Whites, unemployed, have a high school or less than high school education, have an income level of less than $50,000, and live in a small metro or nonmetro area (p < .001 for all; Table 1).
Compared to nonsmokers, pregnant smokers were more likely to report past-year mental illness (37.4% vs. 17.7%, p < .001), major depressive episode (13.9% vs. 6.4%, p < .001), alcohol use disorder (11.8% vs. 3.2%, p < .001), illicit drug use disorder (13.9% vs. 1.5%, p < .001), and comorbid mental illness and SUDs (30.7% vs. 10.8%, p < .001). They also reported higher rates of treatment for mental health (28.6% vs. 12.7%, p < .001) and SUD (16.9% vs. 2.0%, p < .001) than nonsmokers.
Factors Associated with Smoking Cessation Counselling Receipt
Among pregnant smokers, 71% reported the receipt of counselling for smoking cessation. Neither sociodemographic characteristics nor having past year mental illness and/or SUD differentiated the receipt of smoking cessation counselling (Table 1). However, pregnant women who received smoking cessation counselling were more likely to be in the third trimester of pregnancy (29.1% vs. 12.4%, p = .027) and have higher smoking frequency, that is, every day in the past 30 days (69.4% vs. 44.3%, p < .001) compared to nonrecipients of smoking cessation counselling. Stratified analysis by the type of disorder revealed higher rates of counselling receipt for cigarette smoking in the third trimester compared to the first trimester (Figure 1). Pregnant smokers in the first trimester with only mental illness (73.9% vs. 92.4%, p < .05) or only SUD (50.9% vs. 72.9 %, p < .05) had significantly lower rates of cessation counselling than those in the third trimester, respectively.
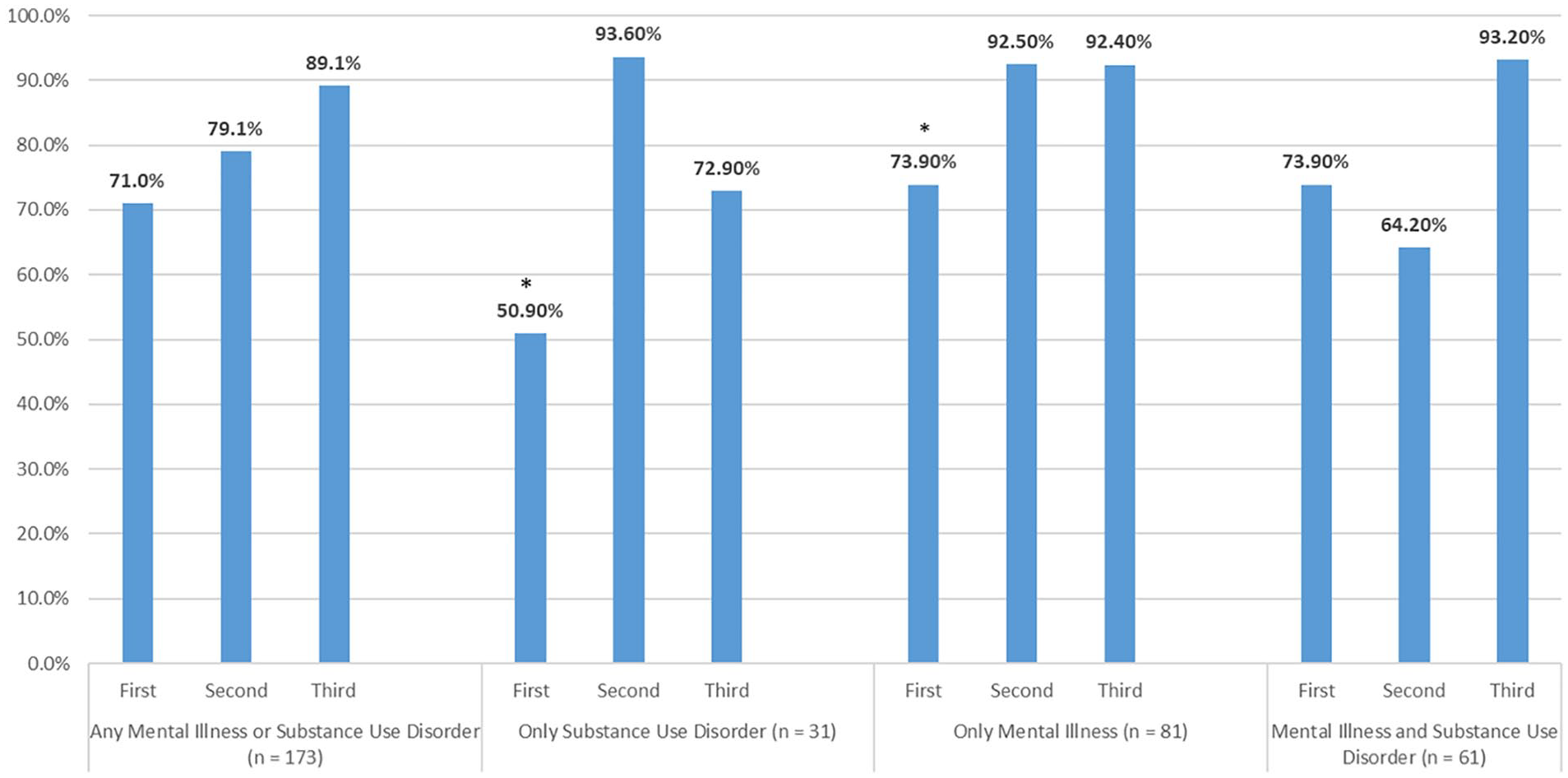
Rates of Counselling Receipt for Cigarette Smoking Cessation by Trimester of Pregnancy Stratified by Type of Disorders in Pregnant Smokers Aged 18–44 Years, NSDUH 2016–2019.
Predicting the Probability of Smoking Cessation Counselling Receipt
In the adjusted analysis, pregnant smokers with mental illness had higher odds of receipt of counselling for cigarette smoking cessation compared to those without mental illness (adjusted odds ratio [AOR] 3.87; 95% confidence interval [CI]: 1.28–11.69; Table 2). Neither having SUD and mental illness (AOR: 0.23; 95% CI: 0.03–2.03) nor having alcohol (AOR: 2.30; 95% CI: 0.57–9.26) or illicit drug use disorder (AOR: 1.32; 95% CI: 0.26–6.82) predicted the probability of receipt of cigarette smoking cessation counselling.
Logistic Regression Modeling the Probability of Counselling Receipt for Cigarette Smoking Cessation among Pregnant Smokers Aged 18–44 Years, Conditional on the Presence of Mental Illness and/or Substance Use Disorders, Controlling for Sociodemographic Characteristics, Smoking Frequency, and Time, NSDUH 2016–2019 (N = 373).
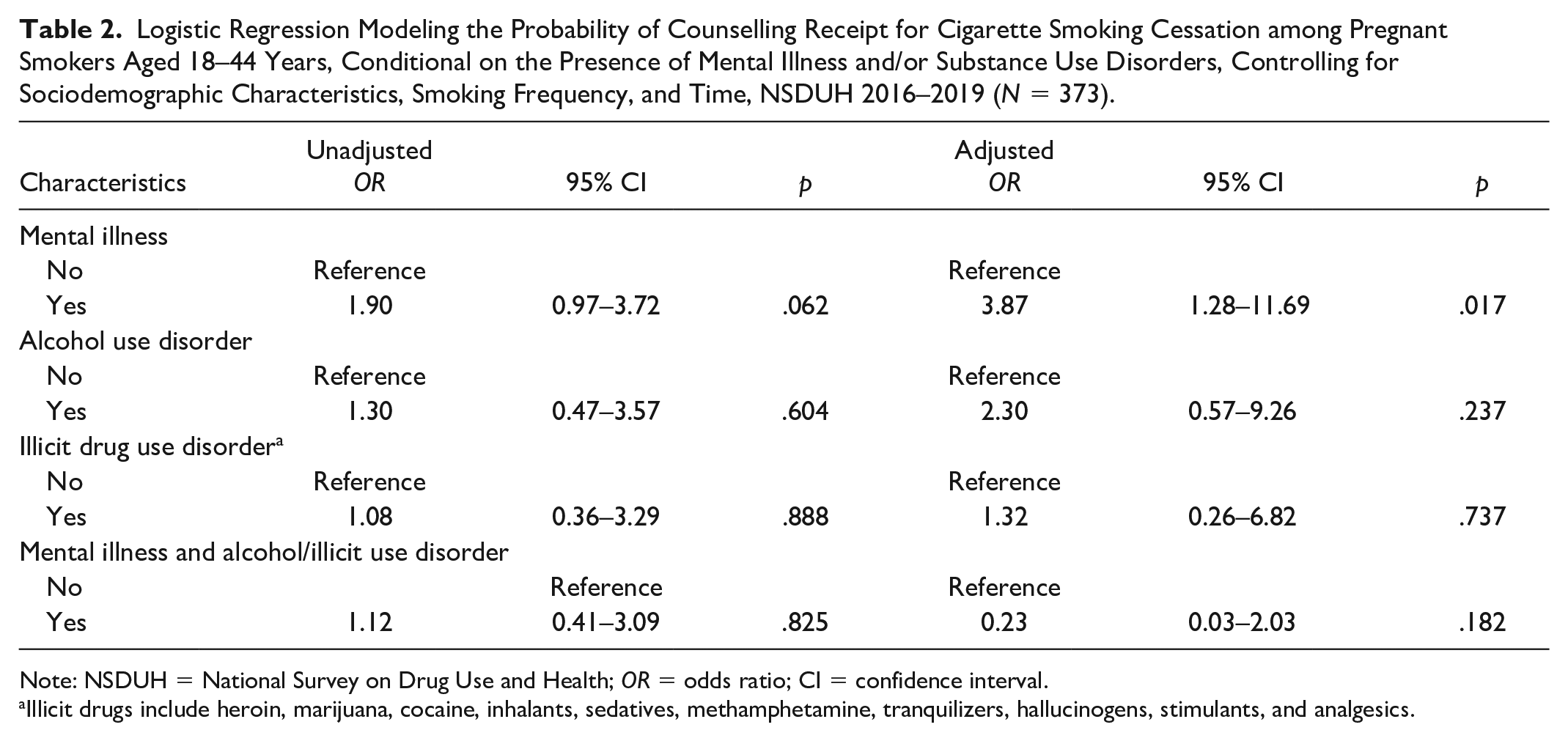
Note: NSDUH = National Survey on Drug Use and Health; OR = odds ratio; CI = confidence interval.
Illicit drugs include heroin, marijuana, cocaine, inhalants, sedatives, methamphetamine, tranquilizers, hallucinogens, stimulants, and analgesics.
Discussion
The findings revealed that 83% of pregnant smokers were screened for their smoking behavior, and 65% who were smokers received cessation counselling. These are encouraging findings and reflect current practice recommendations. Pregnant women with mental illness, but not those with SUD or comorbid mental illness and SUD, had significantly increased odds of receiving cessation counselling. The higher proportions of smoking cessation counselling in pregnant smokers with mental illness may indicate frequent contact with health care providers (Hollis et al., 2020) and therefore more chances for receipt of counselling to quit smoking. Although this finding is encouraging, the question about the receipt of cessation counselling in the NSDUH is general and does not specify the type of health care provider, such as obstetrician, maternity nurse, or mental health professional. Regardless, the USPSTF (2021) recommends all health care providers screen for cigarette smoking and provide treatment interventions for pregnant women. ACOG (2020) also recommends clinicians conduct brief counselling and provide pregnancy-specific materials and individualized care for pregnant smokers by the provision of behavioral, psychosocial, and pharmacotherapy interventions.
Little is known about mental health professionals’ practices regarding smoking cessation counselling for pregnant smokers. In a prior study based on the 2008–2014 NSDUH, pregnant women who received mental health treatment had higher odds of cigarette smoking cessation (Salameh et al., 2021b), though this relationship was not significant; this indicated a potential effect of mental health treatment on smoking cessation. In a study among the general population, those who received mental health treatment had a significantly higher odds of cigarette smoking cessation (Cook et al., 2014). A global systematic review revealed that health care providers acknowledge that they need to consider women’s stressors and psychological state while advising them to quit smoking (Kumar et al., 2021). Given the higher prevalence of cigarette smoking in pregnant women with mental health disorders (Salameh et al., 2021b; Tong et al., 2016), further research is needed to examine cessation counselling in clinical settings among pregnant women with mental illness.
Our findings show that neither having SUD nor having comorbid mental illness and SUD in pregnant women is associated with the receipt of counselling for smoking cessation. Thus, pregnant smokers with these disorders continue to face multilevel barriers to smoking cessation assistance. There is a misbelief among health care providers about smoking cessation’s effect on substance use treatment outcomes (Fallin et al., 2016), as qualitative studies of pregnant women with SUD revealed that treatment providers discourage smoking cessation during treatment (Fallin et al., 2016). Although smoking cessation is not considered a priority (Knudsen, 2017), health care providers may not have the skills and resources to treat the dual dependence on nicotine and other substances (Fallin et al., 2016; Knudsen, 2017). Overall, health professionals may feel less prepared to care for patients with SUD compared to mental illness (van Boekel et al., 2013), which may explain our finding that having mental illness but not SUD increased the probability of the receipt of cessation counselling. These findings also are consistent with the general population in the United States (Samples et al., 2018).
Regardless of the presence of mental illness and SUD in pregnant women, systematic reviews showed that health care providers require training to assist pregnant women to quit smoking in maternity care settings (Diamanti et al., 2019; Nims et al., 2019). For instance, most U.S. obstetric/gynecology programs provide minimal training and education on smoking cessation counselling (Nims et al., 2019). Furthermore, a qualitative study of 45 health care providers (i.e., perinatal/neonatal nurses, midwives, and physicians) and 21 pregnant smokers indicated that health care providers conveyed inconsistent information and guidance related to smoking cessation during pregnancy (Britton et al., 2017). This suggests the importance of continuing education to support pregnant smokers quit smoking while placing more emphasis on those with mental illness and SUD.
Pregnant women with mental illness or SUD had lower proportions of cessation counselling receipt in the first trimester of pregnancy than in the second and third trimesters. ACOG (2020) recommends that the best benefit of smoking cessation is by 15 weeks gestational age. This indicates the importance of early screening and counselling for pregnant smokers, especially since research shows women with mental illness and SUD are motivated to quit (Fallin et al., 2016), and most pregnant women may quit early in the second trimester of pregnancy regardless of the presence of mental illness (Salameh et al., 2021b). Hence, pregnancy provides a unique opportunity to support those with mental illness and SUD to quit smoking and sustain abstinence, thereby decreasing smoking rates in this population.
There are some limitations to this study. Although the NSDUH measures screening of smoking and counselling for smoking cessation, the survey does not identify the type of health care providers who provided the screening, which is an important clinical aspect for pregnant women. In addition, this survey does not specify when pregnant women entered prenatal care, which might confound when these women received counselling for smoking cessation. There is also a potential misclassification as the survey asked about the receipt of counselling for smoking cessation in the past year, whereas pregnancy status was measured at the time of the interview. However, most pregnant women were in the second and third trimesters of pregnancy, which might minimize this bias. The NSDUH relies on self-report measures for pregnancy status, smoking, mental illness, and SUD, all of which are subject to recall bias. Mental illness and SUD are sensitive topics, and pregnant women may feel reluctant to disclose; however, the NSDUH ensured privacy and confidentiality through the use of computer-assisted interviews. Although we found that having any mental illness increased the likelihood of smoking cessation counselling, it is not clear whether particular mental health disorders are associated with greater receipt of cessation counselling. Hence, future clinical and population-based studies need to stratify by counselling practices for smoking cessation across different mental problems in pregnant women (e.g., depression and anxiety). Likewise, it is essential to examine such practices with a larger sample of pregnant smokers with SUD while addressing the needs of women with particular prevalent disorders such as opioid use.
Conclusion
Smoking in pregnant women with SUD and comorbid mental illness and SUD does not increase the probability of receiving cessation counselling. This indicates the sensitive and complex needs of pregnant women with SUD (Center for Substance Abuse Treatment, 2009; Fallin et al., 2016), and therefore the necessity for improving smoking cessation counselling among this population. Although pregnant smokers with mental illness had an increased likelihood of smoking cessation counselling receipt, further studies are required to examine health care providers’ practices to support smoking cessation in pregnant women and to examine whether counselling is associated with smoking cessation among the general population of pregnant women with mental illness.
Supplemental Material
sj-pdf-1-wjn-10.1177_01939459221127803 – Supplemental material for Cigarette Smoking Cessation Counselling in Pregnant Smokers with Mental Illness/Substance Use Disorders
Supplemental material, sj-pdf-1-wjn-10.1177_01939459221127803 for Cigarette Smoking Cessation Counselling in Pregnant Smokers with Mental Illness/Substance Use Disorders by Taghreed N. Salameh, Lynne A. Hall and Martin T. Hall in Western Journal of Nursing Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.