
Abstract
Older widows might experience poor health outcomes following their spousal dementia caregiving experience. Widows from rural areas with fewer resources may have worse health outcomes. Serial, qualitative interviews were conducted at baseline, 6-months and 12-months with 13 urban and nine rural older widows who cared for husbands with dementia. Perceptions of caregiving, widowhood, and resources were examined. Major themes were 24/7 Care, Watch the Man Go Down, Build a Network, Spiritual Support, No Regrets/Some Regrets, Time for Me Now, Loneliness, and Keep Reaching In. Compared to urban widows, rural widows had fewer emotional and tangible resources. All widows desired more support during spousal dementia caregiving and in their transition to widowhood. Nurses need to continue to support the transition from spousal dementia caregiving to widowhood and to test interventions unique to meeting the needs of urban and rural older women.
Approximately 5.7 million Americans are living with Alzheimer’s Dementia (AD) (Alzheimer’s Association [AA] 2019). AD is the sixth leading cause of death in the United States (Kochanek, Murphy, Xu, & Tejada-Vera, 2016). Beyond the numbers, dementia does not discriminate for gender, race, ethnicity, or geography (urban or rural), but it does afflict persons more so in the age range of 65 years and older. Also, more hospital, long-term care, and home care nursing days are accrued by persons with dementia every year than all other conditions in older persons (AA, 2019). Caring for someone with dementia is burdensome and stressful (National Alliance for Caregiving and the AARP Public Policy Institute, 2015). The dementia caregiving experience is well documented, but the post-caregiving phase has received little attention (Arruda & Paun, 2017). Nurses need to pay attention to the post-caregiving phase as the effects of dementia care on caregiver health can continue for years after the patient’s death (Corey & McCurry, 2018). Furthermore, to our knowledge, no study to date has examined rural widows’ post spousal dementia caregiving experience separate from spousal caregiving in general.
Spousal Dementia Caregiving to Widowhood
Evidence supports a relationship between the spousal dementia caregiving experience and outcomes in widowhood (Aneshensel, Botticello & Yamamoto-Mitani, 2004; Burton, Haley & Small, 2006; Corey & McCurry, 2018; Keene & Prokos, 2008; Schulz, Boerner, Shear, Zhang, & Gitlin, 2006). High caregiver burden, depression, anxiety, exhaustion (Schulz et al., 2006), social isolation (Burton et al., 2006; Schulz et al., 2006), sleep disturbances (Corey & McCurry, 2018), longer years as a dementia caregiver, and being an older women (Aneshensel et al., 2004) may contribute towards poor health outcomes post-caregiving. For example, as dementia progresses and social interaction declines, the social isolation that begins in caregiving carries over to widowhood (Burton et al., 2006). Moreover, sleep disturbances that occurred during caregiving are reported to continue for up to 10 years beyond the death of the patient (Corey & McCurry, 2018). Aneshensel et al., (2004) found that among 291 dementia caregivers, older women caregivers who had provided care the longest (M = 5.7 years) remained distraught into widowhood. Additionally, spousal caregivers in general tend to ignore their own health needs during the caregiving years (DiGiacomo, Lewis, Nolan, Phillips & Davidson, 2013). This lack of self-care during caregiving places widows at higher health risk into widowhood. Overall, dementia spousal caregiving may negatively alter women’s transition to widowhood (Chan, Livingston, Jones & Sampson, 2013).
In a recent integrative review on former dementia caregivers (survivors), the most prevalent health issues were depression, anxiety, guilt, longing, social isolation, and loneliness (Arruda & Paun, 2017). Additionally, limited information is available on resources used by survivors to help them with their loss. In a study of 224 survivors, every third survivor used some type of resource post-loss: support groups (n = 29), counseling (n = 30), or psychotropic medications (n = 37) (Bergman, Haley & Small, 2011). However, the use of psychotropic medications was fewer among those who were more engaged in religious practices (Bergman et al., 2011). Furthermore, religious practices have been associated with other survivor outcomes such as reduced feelings of loss, improved social support (Almberg, Grafström, & Winblad, 2000), and decreased complicated grief (Chan et al., 2013). Finally, the person’s death is a feature that cannot be ignored as survivors report feeling relieved, less stressed, and positive affect post-death (Arruda & Paun, 2017).
To our knowledge, no study to date has documented rural-urban contrasts for the post-spousal dementia caregiving experience. Research is needed for several reasons. First, rural caregiving is underreported (Sanford & Townsend-Rocchiccioli, 2004) and comprises 28% of all caregiving (National Alliance for Caregiving and AARP Public Policy Institute, 2015). Second, rural caregivers use fewer respite services than urban caregivers (Kosloski, Schaefer, Alwardt, Montgomery & Karner, 2002). Third, older, rural women might have higher health risks due to social isolation, geographically imposed with fewer health and community resources, and overall lower socioeconomic status (Gerrior, Crocoll, Hayhoe & Wysocki, 2008). Fourth, persons living in rural areas have higher unemployment rates, are less likely to have high speed internet to access health information, have greater issues with travelling to and from a health care provider, fewer health care providers in general, and access to more or better health care facilities than persons living in urban areas (National Rural Health Association, 2017). Most importantly, nurses need to know how rural and urban spousal dementia caregivers differ and implement care that best meets their needs.
Conceptual Framework
The conceptual framework for this study is based on Meleis’s (2010) transitions theory. This theory is particularly relevant to this study since it addresses both developmental and role transitions: spousal dementia caregivers of their husbands are facing a developmental transition (widowhood) as well as a role transition (wife, caregiver). When a role is central to one’s identity (e.g., wife or caregiver), involuntary role exit (husband’s death → widow) may be a stressful disruption. Meleis (2010) proposes that the experience of life transitions and developmental trajectories is contingent on the specific circumstances under which the transitions occur. Individual attributes might include: health status, coping efforts, current and past roles, family, and social context (Meleis, 2010). Thus, the experience of spousal dementia caregiving and the transition to widowhood for the women in this study will be influenced by their specific circumstances. See Figure 1 for a schematic model of concepts used to guide this serial, qualitative study.
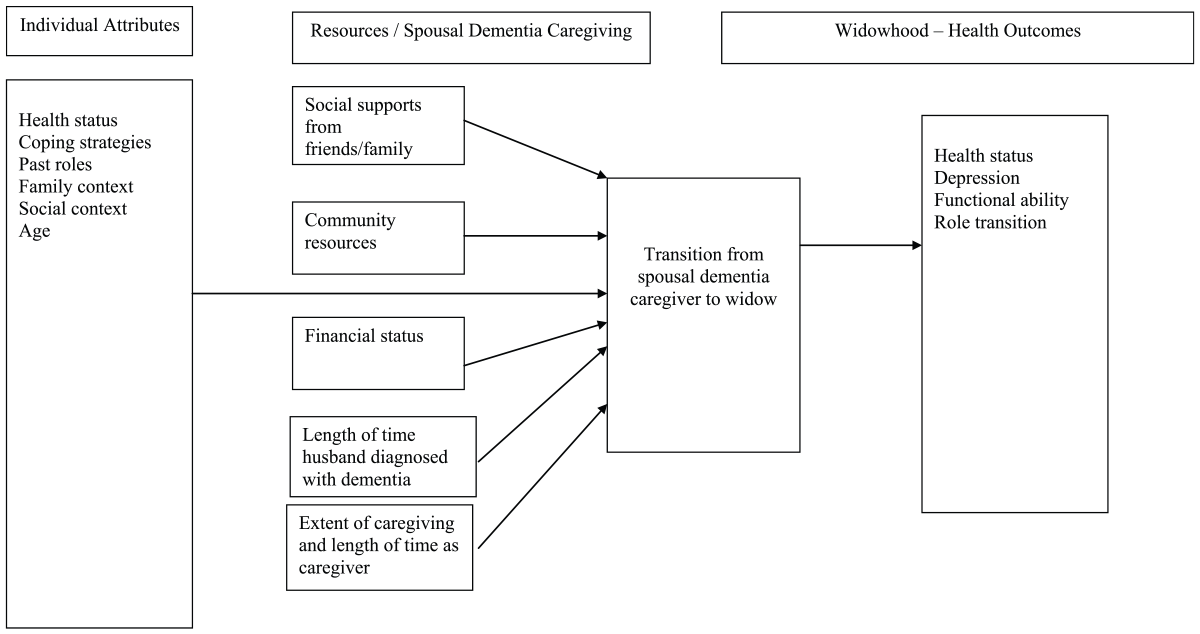
Schematic model of concepts used to guide the design of this serial, qualitative study.
Purpose
The purpose of the study was to clarify perceptions of widows on their transition from spousal dementia caregiving to widowhood.
Specifically, the research questions are:
What are widows’ perceptions of their spousal dementia caregiving experience?
What are widows’ perceptions of their transition to widowhood?
What are widows’ perceptions of resources that helped their transition to widowhood and what resources might have helped more?
Are there rural–urban contrasts in widows’ perceptions of spousal dementia caregiving to widowhood?
Methods
This study used a serial, qualitative design as described by Murray et al. (2009). The serial interview method supports a trusting relationship between participant and researcher that encourages participants to express themselves more freely over time (Murray et al., 2009).
Sample
Following approval by the institution’s internal review board, the following recruitment strategies were initiated: telephone and email communications with caregiver and grief support group leaders, clergy, health care providers, social workers, and faculty/staff at the researchers’ academic institution; advertisements in church bulletins, flyers posted in libraries, community centers, and medical clinics; and face-to-face meetings and telephone communications with leaders of the state’s Greater Chapter Alzheimer’s Association. Equal numbers of widows were desired from urban and rural settings. The urban environment consisted of county 1 (pop. 1,753,893) and the rural environment consisted of county 1 (pop. 15,041), county 2 (pop. 25,337), country 3 (pop. 40,599), county 4 (pop. 290,494) and county 5 (pop. 41,182) (U.S. Census Bureau, 2019).
The participant inclusion criteria were the following: (a) Widows, > 65 years of age and former caregivers of husbands with AD or another form of dementia, (b) Husband died in the last 6 months, (c) English speaking, and (d) Mini Mental State Exam score > 24. Recruitment efforts lasted 6 months. To achieve an adequate sample size, the death of the husband was extended to < 3 years based on the widows recruited for the study. For this reason, the inclusion criterion was changed to “Husband died in the last 3 years.” Thirteen urban and nine rural women met criteria for the study. Participation rate for the length of the study was 100%.
Data Collection and Analyses
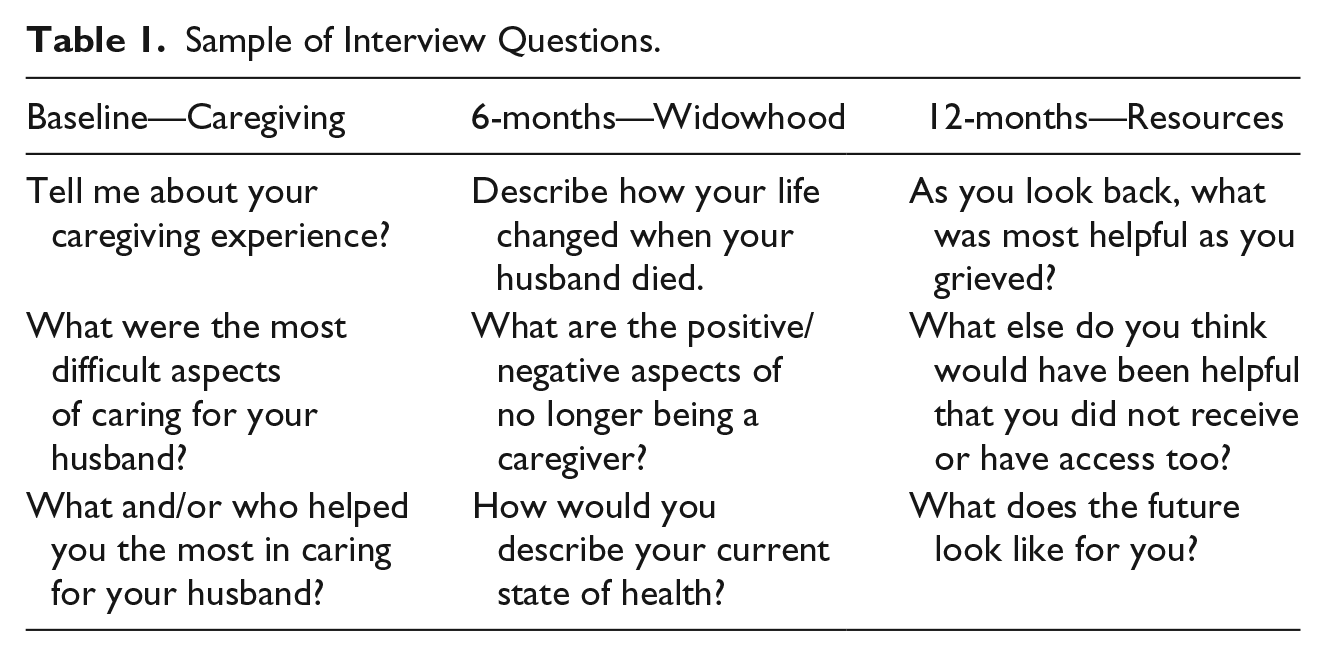
Semi-structured interviews were conducted at the following times: baseline, 6-months and 12-months. Six month intervals were chosen to allow sufficient time for the complex process of caregiving to widowhood to unfold. Table 1 shows a sample of questions that were asked at each interview. The questions were developed by the researchers and were derived from the literature review and transitions theory (Meleis, 2010). Questions were open-ended and non-judgmental to allow for a range of responses. The baseline interview assessed perceptions of their spousal dementia caregiving experience. The 6-month interview assessed perceptions of their transition to widowhood. The 12-month interview assessed perceptions of resources that helped their transition to widowhood and what resources might have helped more.
Sample of Interview Questions.
Urban widows were interviewed by the same researcher and rural widows by the other researcher in the study. Most widows were interviewed in their home (n = 21). One urban widow preferred her church. The home setting provided details of where caregiving took place, for example, witnessing the presence of a hospital bed once occupied by a spouse or seeing packages of incontinent pads stacked in a hallway. Widows shared photographs of their husbands, family pictures, obituaries, and other personal items to explain who their husbands were. All interviews were private and audio-recorded, and they lasted 1–3 hours each. Researchers allowed widows as much time as needed to express themselves and answer questions. Additional questions were asked to clarify statements when needed. Non-verbal cues of listening, undivided attention, and silence were implemented to allow time for widows to gather their thoughts and formulate responses. Expressions of grief (crying) were common during the baseline and 6-month interviews, and offers were made by the researchers to stop the interviews when this happened. None of the widows stopped the interviews. At the end of each interview, the widow was thanked and given a gift card for her participation ($35 after baseline, $35 after 6-months, and $40 after 12-months). The researchers wrote reflective notes after each interview. Overall, the sample size was adequate to achieve data saturation.
Every interview was transcribed verbatim and checked again with each recording. When discrepancies were found, transcripts were corrected. Data were uploaded in Atlas.ti.8 software, organized into six separate sets of data for each timeframe (baseline, 6-month, and 12-month) and categorized as urban or rural. Data were analyzed using qualitative methods (Miles, Huberman & Saldaña, 2014). Specifically, the researchers reviewed the data for similarities and irregularities to develop codes when large chunks of data fit together. Sub-codes were developed when enough data supported finer details of a larger code. Full paragraphs and sentences were stored under codes and sub-codes as supportive testimony. Pattern codes were developed from the first cycle of codes considering the amount and types of testimonial support. From the codes, major themes were formulated. The reflective notes were useful in the final stages of theme development as additional evidence. Additionally, for validation and confirmation purposes, the themes derived from the baseline and 6-month analyses were shared with the widows at the 12-month interview, and they agreed with the findings.
To address the research question, “Are there rural-urban contrasts in widows’ perceptions of spousal dementia caregiving to widowhood?” researchers reviewed the data for conceptual contrasts. The transcripts revealed a redundancy regarding the concept of resources. Next, a table was built of exemplars that demonstrated contrasts on resources used by rural and urban widows.
Overall, there were eight major themes with one theme (spiritual support) counted twice for both the spousal dementia caregiving experience and widowhood. There was one major contrast and one sub-contrast identified in the rural-urban analysis. The researchers counted each theme, contrast and sub-contrast as one. One disagreement arose which prompted further review of the transcripts and reflective notes to assess for researcher bias and clarification of the data. The researchers agreed on the results with > 90% agreement.
Results
Of the 22 widows, the mean age of the nine rural widows was 77 years (SD = 7.2) and of the 13 urban widows was 80 years (SD = 4.6). Ninety-one percent of widows were Caucasian and unemployed. Urban widows were married longer to their husbands than rural widows to their husbands (M = 49, SD = 15 vs. M = 39, SD = 21). Of those sampled, 41% were high school graduates, 27% had some college education, and 32% were college graduates. Urban widows reported higher annual incomes than rural widows of > $40,000/year (62% vs. 22%). Eighteen widows (82%) lived alone. When providing care to husbands, urban widows reported having attended caregiver support groups at a slightly higher rate than rural widows (46% vs. 44%). Reported hours of care for husbands each day were similar, with rural widows slightly higher with more reported hours (M = 23, SD = 2.5 vs. M = 21, SD = 5.3). The majority of husbands were in hospice at the time of death (77%). More husbands died in a hospital, memory care unit, or long-term care facility (55%) than at home (41%). The mean number of months since death of husbands at the first baseline interview was less for rural widows than urban widows (M = 26, SD = 11 vs. M = 40, SD = 21).
Widows’ Perceptions of Spousal Dementia Caregiving
The major themes were the following: 24/7 Care, Watch the Man go Down, Build a Network, Spiritual Support and No Regrets/Some Regrets. All widows expressed care as “24/7” to describe the constancy of this level of care: “Sometimes, if we came home too soon in the afternoon, he’d say, “What are we going to do now?” It was constant keeping him occupied.” Even when husbands transitioned from home to long term care, widows still perceived themselves as the caregiver: “I was there with him mostly. Early in the morning till late.” Moreover, during times of respite, their thoughts were still preoccupied with concerns for their husband: “I constantly worried about him.” Overall, “24/7 Care” included time with and time away from their husband.
All the widows gave examples of what it was like to “Watch the Man Go Down”: “A complete change in behavior of the man he was. He was educated, college degree, good job, retirement was good.” For example, one widow described the need to cover all mirrors in their home: “He would talk and nod at the guy in the mirror and then later on that person in the mirror became a threat.” For another widow, her husband’s new obsession with sex overwhelmed her: “He would just stand at the shower and watch me. It was awful.” Having sexual relations was also problematic: “He would try but he didn’t know what to do, it was hard.” However, to “Watch the Man Go Down” facilitated widows’ transition towards feeling relief when husbands died: “It was awful to see this man the way he was and know he would never have wanted to be that way.”
“Build a Network” was very important for widows in handling the demands of caregiving to get respite and help in making care decisions: “Mom, you can’t keep doing this. He is going to hurt you.” They readily accepted help from family, friends or neighbors and listened to their advice: “You need rest. You need respite.” Caregiver support groups were an important part of the network when used: “The support groups were what got me through to the next month.” When support groups were not available, widows felt they would have helped: “If somebody would’ve told me what was going to happen in AD, I would’ve been in a better place.” Paid caregivers were also part of the network of support beyond family and friends:” Sometimes my daughter would come over and then other times if she wasn’t available, then I would have one of the caregivers.” Overall, widows regarded a network of others as very important during the caregiver years.
For the theme “Spiritual Support”, all widows felt that their beliefs in a higher being (God) helped them the most: “When you see somebody going down like that. Spiritually, you become closer to God.” Most of the widows used some form of religious practice (prayer, church attendance, and church volunteer). Spiritual beliefs helped them to cope:” I will see him again or he is going to a better place or God only gives you what you can handle.” Not one widow in the study waivered on the importance of what they gained spiritually or through religious practices: “I was as close to God as I ever have been during that time.” One widow did feel she could have used more spiritual support when the AD diagnosis was made: “That’s when you really need the spiritual support.” Overall, they leaned on God to get them through each day: “Lord, help me get through this day, another day. Because sometimes you’d just feel like oh, I can’t do this another day.”
Finally, the theme “No Regrets/Some Regrets” represents responses when answering about the most rewarding aspects of caring for their husbands. All widows felt “No Regrets” having been their husband’s primary caregiver and felt they did their best: “Knowing that I cared for him the best way I could.” Yet, all widows shared “Some Regrets” in decisions made such as placement in long term care (“It was terrible to leave him in that nursing home. There were times I felt like I was deserting him or Maybe he could have stayed home”), thoughts of wishing it would all end (“I had thoughts like oh, I wish this was over–then I would have to bop myself”), how they could have done things differently (“more patience, more understanding of the progression of AD, just put him in a wheelchair and still take him to church”), or more willing in letting to allow their husbands do what they felt they needed to do without a fuss (“check doors all the time”). However, “No Regrets” was predominant and in the words of one widow that summarized all others thoughts on the matter: “If I had to do it over, I would.”
Widows’ Perceptions of Widowhood
The major themes were “Time for Me Now” and “Loneliness”. Time for Me Now meant shifting their focus from their husbands in their former caregiver role to their own needs: “I’m my main concern now.” Widows ignored their health during the caregiver years: “I didn’t take care of myself very well.” One extreme example was the widow who described the symptoms of colon cancer which she ignored during caregiving and underwent surgery to remove the tumor from her colon months following her husband’s death. This occurred between the baseline and the 6-month interview. Thus, they desired to regain their health:” I’m better now than I was before, because you are exhausted (during caregiving).” They exercised more and in a variety of ways: yoga, biking, bowling, golfing, long walks, and even meditation: “I am meditating every night before I go to bed.” They slept better, and had less stress and worry: “I don’t have to worry about him falling or doing something he shouldn’t be doing.” “Time for Me Now” also meant time with family and friends (“I want to connect with people again on an on-going basis”) and enjoying activities like book club or playing cards (“I have something planned every day”). Moreover, many of the widows were now offering support to other caregivers of family members with dementia: “I can give of myself and be there.” Some continued to attend their caregiver support groups: “The strongest thing I have is sympathy for women going through it.” Overall, “Time for Me Now” meant the freedom to focus on their health, being with others again, enjoying activities and supporting others in caregiver roles.
All widows expressed “Loneliness”: “I’m lonely.” They missed their husbands: “I miss him.” They missed being a caregiver: “Not having someone to care for or pamper, that’s a negative aspect.” They had difficulty transitioning out of being a caregiver: “I had a purpose when he was here.” All the widows affirmed feeling lonely despite the variability in months since their husband’s death: “This is my second year; it is a downhill situation all the way.” Some were bothered seeing other women with their husbands: “It’s just not fair.” One widow missed having sex: “Sex is very important.” Several widows talked about dating again during the 12-month interview, but none of the widows were in new relationships during the study. Overall, all the widows expressed “Loneliness” stemming from a lack of intimacy, adjusting to being alone, or no longer being a caregiver.
Widows’ Perceptions of Resources
The major themes were “Spiritual Support” and “Keep Reaching In”. “Spiritual support” was as important in widowhood as it was during caregiving: “It (my faith) got stronger after he died.” Widows reflected on the importance of faith in God in their lives: “My faith keeps me from taking my own life.” Whether it was attending church services, singing in the choir, prayer, journaling, reading the bible, or practicing gratitude, widows continued to express their spirituality: “I write a daily thank you note, something that God brings into my mind. I am up to 506.” Widows remained thankful for their years as caregivers: “I thank God every day for allowing me to have taken care of him.” Overall, spiritual support was an ingredient used by widows to cope and function.
Widows expressed the need for others to “Keep Reaching In” to encourage them as they gradually move forward in life: “Keep knocking on the door and inviting because, sooner or later, I’ll venture out again.” The social isolation began during the caregiver years: “Others (friends and family) quit coming around.” For widows, whose family did reach in, this was viewed positively: “Someone calls or comes by every day to check on me.” Some widows wished clergy, in particular, would have done more: “They (clergy) knew about my husband but never reached out to help.” Widows who had built a network during caregiving that included paid caregivers or hospice care workers wished that type of support had continued after their husband’s death: “I could’ve used someone to come in for a couple more weeks to keep things normalized.” Another widow phrased it this way: “Once the patient dies, they (hospice) just drops you. Whether it’s a pastor or a nurse, just somebody to talk to—that would have been helpful.” Overall, all widows expressed the importance of needing others to support them into widowhood.
Rural–Urban Contrasts in Widows’ Perceptions
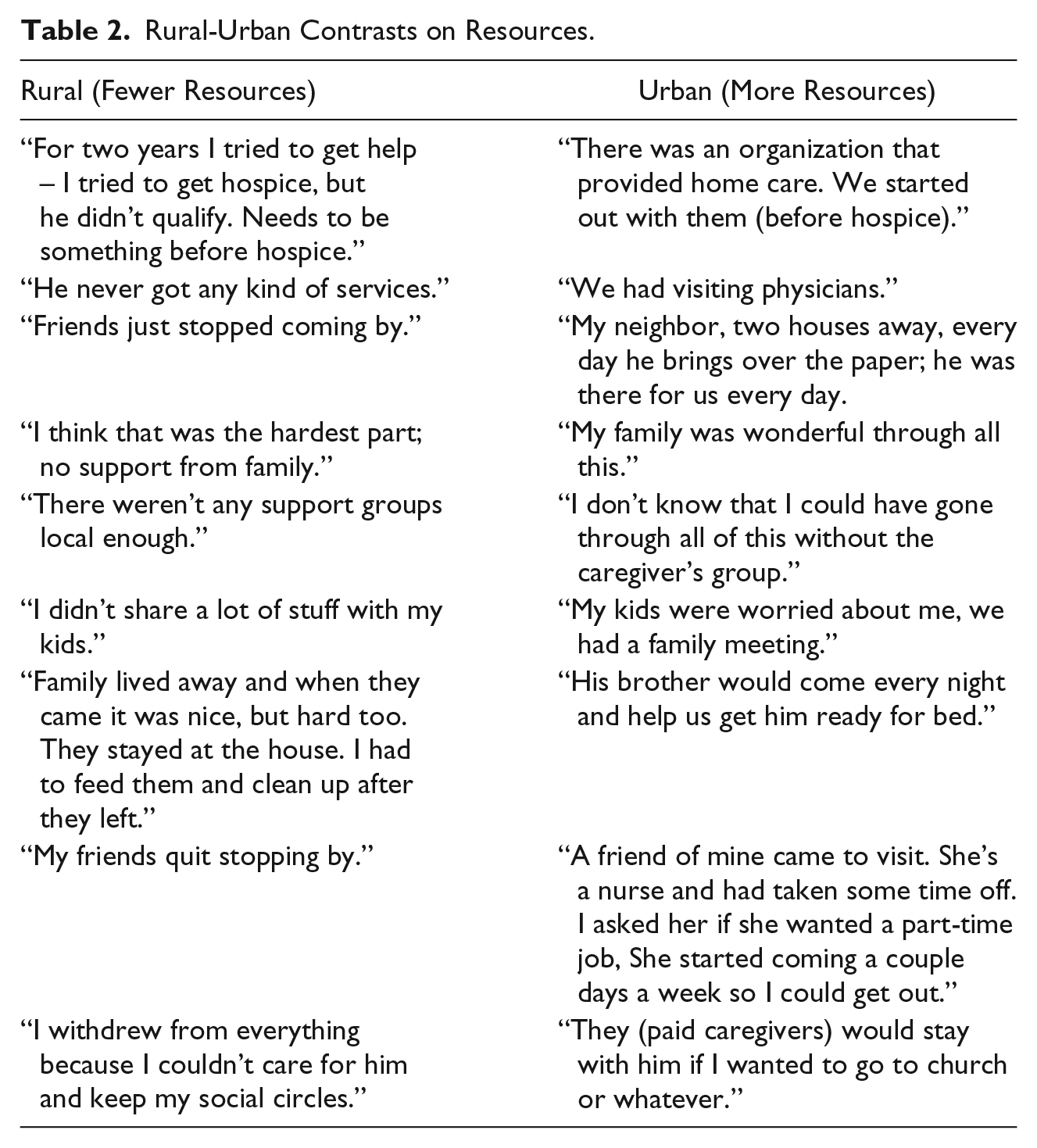
The amount and kinds of resources were different between urban and rural widows. The frequency of contacts with family members, friends, neighbors, legal/financial advisors, paid caregivers, caregiver support groups and doctors were noticeably greater among urban widows. Table 2 reveals a sample of contrasting statements among rural and urban widows. The testimonies suggest that rural widows had fewer supportive resources during the caregiver years. Along with fewer resources, rural widows experienced more financial concerns: “It (caregiving) has really impacted me financially.” The impact was felt into widowhood in the absence of their husband’s income: “I’m living on less than half. I dropped magazines and other things we use to have.” Being financially strapped was voiced as the biggest issue facing several of the rural widows: “My biggest challenge is the financial.” One rural widow was getting help from her church: “The church is helping me, I’m doing okay month to month unless something comes up.” In contrast, only one urban widow mentioned financial issues but had received support during caregiving: “I hired an elder lawyer, so that helped a lot. She knew what to do and how to get things financed.”
Rural-Urban Contrasts on Resources.
However, rural widows mentioned one resource that the urban widows never mentioned: the internet. Rural widows used virtual resources such as web-sites and Facebook to get information on dementia during the caregiver years and in grief support during widowhood: “I meet them on Facebook, through the iPad.”
Discussion
This study identified widows’ perceptions of their transition from spousal dementia caregiving to widowhood. The sample included both rural and urban widows, and the majority were at least two years into bereavement. Neither time since the husband’s death nor geographic location mattered as the themes were consistent across all widows with the only exception being fewer resources during spousal dementia caregiving for rural women. While the literature is sparse on the post-spousal dementia caregiver experience, there is data to support ongoing difficulties in moving forward in life and getting back to a healthy state for up to 10 years post-caregiving (Corey & McCurry, 2018). As transitions are characterized by critical points and events (Meleis, 2010), future research should consider a sample of widows similar in timing from the spouse’s death to better grasp the trajectory of this experience.
The caregiving experience was expressed in the themes: 24/7 Care, Watch the Man Go Down, Build a Network, Spiritual Support, and No Regrets/Some Regrets. The widows’ perceptions are consistent with the dementia caregiver literature (AA, 2019). The first two themes, “24/7 Care” and “Watch the Man Go Down”, support the finding that spousal dementia caregiving is demanding and stressful (National Alliance for Caregiving and the AARP Public Policy Institute, 2015). “Build a Network” referred to resources used by widows during caregiving that afforded them respite and support. The most common resource at the end of the disease trajectory was long-term care (truer for urban rather than rural). This supports a reported rise of respite among dementia caregivers since 1999 as more resources became available (Wolff et al., 2018). Respite was used to attend caregiver support groups, go shopping or complete other business matters. Attendance at monthly caregiver support group meetings was very important to those who had access to this resource to cope with the demands of spousal dementia caregiving. Dementia caregiver support groups are a time to share stories and get information on how to provide dementia care (Dementia Care Central, 2019). Getting caregivers respite should continue to be a priority.
“Spiritual Support” (prayer, belief system, and rituals) was important to all widows in the study. Spiritual health can seriously impact one’s ability to cope with their caregiver role (O’Brien, 2018) and should be assessed and supported by nurses. This could be an important opportunity for nurses who are engaged in providing holistic care of body, mind, and spirit to faith-based communities like the widows in this study. Finally, the theme “No Regrets/Some Regrets” supports the need for forgiving self for being inpatient and a theme to consider in care provision and future research.
The transition from caregiving to widowhood was reflected in the themes, “Time for Me Now” and “Loneliness”. Intense loneliness might be a unique process to widows’ post-dementia caregiving experience (Arruda & Paun, 2017; Corey & McCurry, 2018). In a comparison study among dementia caregivers, bereaved dementia caregivers and non-caregivers, levels of loneliness in the bereaved dementia caregiver group remained similar to dementia caregivers, whereas non-caregivers’ levels improved (Robinson-Whelen, Tada, MacCallum, McGuire & Kiecolt-Glaser, 2001). This might be explained by longer years in the caregiver role, greater levels of caregiver burden, stress (AA, 2019) and pre-death grief associated with dementia caregiving (Arruda & Paun, 2017). More research is needed to fully understand the concept of loneliness post-spousal dementia caregiving.
“Time for Me Now” meant engaging in activities that widows desired and finding ways to improve their health. The impetus might be years of self neglect accrued while caregiving (DiGiacomo et al., 2013). Zhang, Mitchell, Bambauer, Jones and Prigerson (2008) found that adverse health behaviors, such as lack of exercise among bereaved dementia caregivers might increase post-loss depression. As such, nurses should support healthy behaviors not only during the caregiver years but also into widowhood. Additionally, for many widows, reaching out to support other caregivers and using their past experiences in caregiving was another meaningful way to spend their time now. Similarly, Corey and McCurry (2018) reported how former dementia caregivers sought to replace caregiving with new caring roles. This might be an important area to explore in future research for its benefit not only widows but caregivers alike. In terms of transition theory (Meleis, 2010), this finding might suggest a healthy transition to widowhood as widows bring forth their prior experience and skills in caregiving to benefit others.
The themes for resources used in the transition from spousal dementia caregiving to widowhood were “Keep Reaching In” and “Spiritual Support”. “Keep Reaching In” was a plea for help by widows. Consistent with other research (Burton et al., 2008), widows who isolated themselves during spousal dementia caregiving perceived more barriers when re-connecting with others post-caregiving. Intrinsically, nurses can explore these barriers and work with widows on ways to reconnect with others. Further, it was suggested by a few widows that formal caregivers (hospice and paid caregivers) might continue to visit them following the loss of their husbands. This intervention could be considered in future research.
“Spiritual Support” continued to be important to widows. This concurs with others who found the benefits of religiosity (religious practices) on outcomes during caregiving and into widowhood (Almberg et al., 2000; Bergman et al., 2011; Chan et al., 2013). Furthermore, in one of the largest and geographically diverse studies on spirituality among dementia caregivers (N = 1,229), decreased rates of depression and complicated grief were found in those who engaged in spiritual practices and beliefs (Hebert, Dang, & Schulz, 2007). More investigation of the benefits of spirituality among post-spousal dementia caregivers is warranted (Arruda & Paun, 2017).
Patterns emerged that suggested rural–urban contrasts among widows. Rural widows perceived fewer resources in the caregiver years and less help from family and friends. Consistent with rural nursing theory, rural persons tend to be self-reliant due to geographical isolation and less open to “outside” help (Long & Weinert, 2018). That rural widows desired more help from family refutes findings in a study among rural caregivers in Tasmania (Orpin, Stirling, Hetherington, & Robinson, 2014). In that study, caregivers did not want help from family and friends even to the extreme of actively excluding those (Orpin et al., 2014). Additionally, rural widows experienced financial hardships that continued into widowhood. Keene and Prokos (2008) found similar findings in their study. One explanation is the high out-of-pocket costs of dementia care not covered by Medicaid, Medicare or other sources (AA, 2019). Another reason might be that the annual income of urban widows was higher than the rural widows. Future research should include financial and social resources’ effects on the post-spousal dementia caregiving experience.
Another contrast was the amount of respite that was greater for urban than rural widows. This finding is consistent with the work of Kosloski et al. (2002). When the psychological health of rural caregivers is thought to be lower than in urban caregivers (Bien, Wojszel, & Sikorska-Simmons, 2007), this finding might exacerbate worse outcomes in rural widows. Yet several of the rural widows in our study reported using the internet, via Facebook and blogs, to feel connections with others whom they shared experiences of loss with. Perhaps rural widows, due to geographical isolation, might utilize and be amenable to more virtual interventions and could be explored in future research.
There are strengths and limitations in our study. The sample size was adequate as redundancy of information was achieved. Serial, qualitative interviews are recommended to grasp the full understanding of the transition of spousal dementia caregiver to widowhood. We experienced a 100% retention rate to suggest that the widows in the study wanted to share their experience. However, our results are limited to Caucasian widows and future studies need strategic approaches to recruit minority women. Additionally, the transferability of the findings is limited to less educated widows based on the educational level of this sample. Recruitment through churches may have influenced the theme of “Spiritual Support,” and recruitment through support groups may have influenced the spousal dementia caregiving experience and transition into widowhood. There are few studies that have examined this trajectory in post-spousal dementia caregivers to determine critical points and events. For example, Hebert et al. (2007) found among 100 spouses, there was greater depression, anxiety, and complicated grief up to two years if they felt less prepared for their spouse’s death. Additionally, with so few rural-urban comparison studies, our results suggest the need for more research to identify unique differences so appropriate nursing care and resources can be implemented.
Based on this study’s findings, nurses need to render more support to older women caring for husbands with dementia as well as in their transition to widowhood. Assisting them to build a network of resources is important. For rural women, seeking support from trusted others might be particularly important as a source of added assistance (Long & Weinert, 2018). Assessing the health of older women during and after spousal dementia caregiving is very important. Initiating conversations when the husband’s needs exceed what the wife can give emotionally or physically needs to occur for appropriate care of the patient. For rural women, the conversation might differ than that for urban women by focusing on how caregiving is affecting the rural woman’s ability to work rather than on quality of life and longevity (Long & Weinert, 2018). Assessments for depression should continue into widowhood, and appropriate referrals and counselling offered as needed. Based on the use of virtual resources by rural widows in this study, nurses need to support these strategies.
In summary, despite the burdens widows’ voiced when caring for their husbands and the consequential loneliness they felt post-spousal dementia caregiving, they were forging ahead to restore their health and establish a new identity. Nurses have an opportunity to guide them in a healthy transition to widowhood. More research is urgently needed to assist nurses to implement best practices. Rural caregivers/widows might need additional nursing support and resources.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Work reported in this publication was supported by the National Institutes of Health Common Fund and Office of Scientific Workforce Diversity under three linked awards RL5GM118981, TL4GM118983, 1UL1GM118982 administered by the National Institute of General Medical Sciences.