
Abstract
Through two decades of research and development, adoptive cell therapies (ACTs) have revolutionized treatment for hematologic malignancies. Many of the seven US Food and Drug Administration (FDA)-approved products are proven to be a curative last line of defense against said malignancies. The ACTs, known more commonly as chimeric antigen receptor (CAR) T-cells, utilize engineered lymphocytes to target and destroy cancer cells in a patient-specific, major histocompatibility complex (MHC)-independent manner, acting as “living drugs” that adapt to and surveil the body post-treatment. Despite their efficacy, CAR T-cell therapies present unique challenges in preclinical safety assessment. The safety and pharmacokinetics of CAR T-cells are influenced by numerous factors including donor and recipient characteristics, product design, and manufacturing processes that are not well-predicted by existing in vitro and in vivo preclinical safety models. The CAR therapy-mediated toxicities in clinical settings primarily arise from unintended targeting of non-tumor cells, potential tumorigenicity, and severe immune activation syndromes like cytokine release syndrome and immune effector cell-associated neurotoxicity. Addressing these issues necessitates a deep understanding of CAR target expression in normal tissues, inclusive of the spatial microanatomical distribution, off-target screening, and a deep understanding CAR cell manufacturing practices and immunopathology.
Keywords
Introduction
Almost 20 years of research and development went into the first chimeric antigen receptor (CAR) T-cell therapy that received Food and Drug Administration (FDA) approval for the treatment of CD19-expressing lymphoma in 2017. In the following years, five generations of CAR T-cells were developed and tested to optimize efficacy and improve safety for patients with lymphoma and leukemia, and to date, a total of 7 cell therapy products have been approved by FDA for clinical use.24,61 These therapies have been incredibly effective and have provided new hope to patients suffering from hematologic malignancies.
The source of cells (T lymphocytes for CAR T, natural killer [NK] cells for NK-CARs) can be the apheresate of either the patient (autologous) or of one or multiple unrelated donors (allogeneic). The lymphocytes are isolated, activated, transduced with a vector encoding for the CAR, expanded, and then infused into the patient. The CAR cells are considered a “living drug” due to their unique ability to respond to the conditions within the patient, ie, become activated and expand in the presence of tumor antigen-expressing cells and then contract but remain present to provide continued surveillance in the body after tumor clearance. 93
The unique advantage of CAR technology is the ability to target tumor antigen-expressing cells in a major histocompatibility complex (MHC)-independent manner. The CAR directly binds to the tumor antigen and then activates the lymphocyte via stimulation domains contained within the CAR. In the case of αβ CAR T-cells, a mixture of polyclonal CD4+ and CD8+ T-cells are included in the final drug product, and the CD4 to CD8 ratio is influenced by several factors that have not been completely characterized. 29 Both cell types contribute to elimination of target cells but by different mechanisms. The CD8+ CARs kill tumor cells in a perforin-dependent manner, whereas CD4-mediated cytolysis is primarily interferon-gamma (IFNγ) dependent, although the exact mechanism is still unclear. The percentage of lymphocytes which express the CAR depends on the viral transduction efficiency at manufacturing and can oscillate between about 50% and 90%. 95
As CAR cell therapies are “living drugs,” safety, efficacy, and pharmacokinetics are influenced by characteristics of the cell donor and the cell recipient, as well as CAR cell design and manufacturing. These features pose unique challenges in preclinical safety assessment.
Preclinical In Vivo Safety Models and Their Limited Utility in Safety Assessment of Adoptive Cell Therapies
Rodents provide several benefits in testing the safety of adoptive cell therapies (ACTs) over large animal models such as non-human primates, dogs, and swine. Rodents are easily bred and housed allowing for robust study designs. In addition, genetically modified and immunodeficient mouse strains are available allowing for expression of human target protein sequences and tumor engraftment. However, there are significant differences between rodent and human biology and immune system function.
The xenograft mouse tumor model is the most used preclinical model in pivotal pharmacology/toxicology studies for regulatory filings. The NOD SCID gamma (NSG) mouse is a rodent species accepted by regulatory authorities for use in xenograft efficacy studies, and it is characterized by a series of genetic mutations which confer severe immunodeficiency, allowing human cells or even tissue (xenograft) engraftment and growth. The selected tumor xenograft consists of either a human cell line or patient-derived tissue (the latter mostly for solid tumors studies) that expresses the specific antigen to which the CAR was specifically designed to bind.49,60,74 A standard experimental design for pharmacology/toxicology studies for regulatory filing begins with injection/transplantation of mice with the human xenograft tumor material. Depending on the average engraftment time of the specific xenograft, mice are then injected with (usually) a single dose of test article (TA), vehicle or non-transduced human lymphocytes (from the same donor as the TA) depending on the experimental group (treatment vs controls). The animals are then observed for clinical signs of toxicity. Efficacy is also assessed by in vivo bioluminescence imaging at one or more time points, granted the human tumor xenograft cells contain a reporter gene. Important limiting factors of this mouse model are the background immunodeficiency, which impacts the array of immunological reactions following TA injection, failing to inform about potential associated toxicity. In addition, long-term in vivo preclinical monitoring is not possible due to the onset of xenogeneic Graft vs Host Disease (xGvHD), especially with human αβ T lymphocytes. The xGvHD in mice is characterized by a band-like infiltration of human lymphocytes (CD3+ cells) at the epithelial/mesenchymal interface with evidence of either ongoing degeneration and loss of epithelial elements or fibrosis and hemosiderophages. Depending on the geometry of the impacted structure, the infiltrate can form cuffs around vessels or bronchioles. Depending on the severity, one or virtually any tissue or organ can be affected with important loss of function and organ failure. From the clinical standpoint, xGvHD manifests with alopecia, dry and scaly skin, and variable body weight loss. Yellowish discoloration of ear pinnae and tail can be present in case of jaundice due to interface hepatitis. The clinicopathological presentation of GvHD in humans and mice encompasses several crucial differences. For example, in mice, xGvHD in the liver is characterized by the dropout of hepatocytes of the limiting plate and unlike human disease, cholangiocytes rarely display degenerative changes.15,36,46,82 The intestine is one of the main organs affected by GvHD in humans, which is rarely affected in mice. From a safety assessment standpoint, xGvHD could also influence the anti-tumor activity of the TA (higher efficacy) or mask/overpredict off-target toxicity. Finally, the human target antigen might be different from its mouse homologue, with a consequent lack of predictivity of on-target off-tumor toxicity. 49
The Role of the Pathologist in Preclinical Safety Assessment of Cell Therapy Products
The major CAR therapy-mediated toxicities encountered in the clinic have been related to targeting of non-tumor cells (both on-target and off-target toxicities), potential for tumorigenicity/development of secondary malignancies, and effector-cell–driven immune activation syndromes such as cytokine release syndrome (CRS), immune effector-cell hemophagocytic lymphohistiocytosis-like syndrome (IEC-HS) also termed CAR macrophage activation syndrome (MAS), immune cell activation hematotoxicity (ICAHT) syndrome, and immune cell activation neurotoxicity syndrome (ICANS). Understanding the potential for targeting non-tumor cells requires in-depth knowledge of the target expression in normal (non-tumor) tissues and thorough assessment of potential off-target binding by the CAR. Determining the risk of drug product tumorigenicity and uncovering the mechanisms for effector-cell–driven immune activation syndromes requires assessment of preclinical in vivo and in vitro models and the development of fit-for-purpose biomarker assays to identify pathogenic mechanisms in patient samples. Pathologists possess a unique skill set that allows them to contribute to all these major areas of investigation.
Normal Tissue Expression Profiling of Therapeutic Targets in Support of Cell Therapy
Antigen-specific targeting by cytotoxic cells through various modalities have emerged as effective therapeutic approaches to eliminate antigen-expressing target cells in the context of oncology indications and are now under consideration for controlling subsets of pathogenic cells in non-oncology indications, such as autoimmune diseases. These modalities can include tumor-associated antigen (TAA)-specific redirection of cytotoxic T-cells (CTLs) or NK cells, including CAR and T-cell receptor (TCR) cell therapy. Given how effective these modalities are, precise understanding of target expression outside of cells of therapeutic interest (ie, normal tissue expression) is key to contextualize safety risks and favorable risk to benefit profiles. This topic was covered as a “points to consider” for target expression profiling (TEP) workflows in support of discovery and development of innovative therapies, with an emphasis on cell-killing modalities.
Understanding target expression in normal tissues is predicated on a robust workflow of tissue section-based research typically done in a bespoke Molecular Pathology laboratory. Gene (in situ hybridization—ISH) and protein (immunohistochemistry—IHC) are the cornerstones of the TEP data package, as they provide spatially resolved data with microanatomical context and must be informed by and integrated with in silico and data sciences deliverables. Decisional molecular pathology data require fit-for-purpose, qualified workflows and assay development to ensure sufficient specificity and sensitivity to appropriately cover the target biology and organs/cells/species of interest.
Molecular Pathology scientists provide essential subject matter expertise (SME) to assay development and to ensure modern, innovative data-generation approaches. Pathologists provide SME that is key to ensuring the workflow is fit-for-purpose and medically, diagnostically sound and to inform application of the results into decision-making. Together, these SMEs are bigger than the sum of their parts and form an effective and inconclusive collaborative team.
Intentional and strategic parsing of the normal TEP workflow is essential to ensure the timely and decisional quality of the results, clear communication and fit-for-purpose of the data set. It is highly recommended to have a workflow clearly spelled out in writing, with clear roles and responsibilities, clear touchpoints and needs for input from stakeholders and collaborators, and clear deliverables/output (format, scope, etc). Delivering normal TEP at scale with consistent timeliness and quality absolutely requires it.
The following structure is proposed as points to consider for this workflow.
Feasibility Assessment
Goals: Assessment of readiness and technical feasibility of experiments.
Information needed: Therapeutic hypothesis, target(s), and modalities under consideration. Literature and databases (eg, bulk or single-cell RNAseq gene expression, proteomics, protein).
Assessment of Reagents: Tissues (full format and/or TMA, fixed and/or frozen, species, quality controlled for fixation, anatomical coverage, normal vs diseased states), IHC antibodies, and ISH probes.
Suitable Controls: Orthogonally qualified cell pellets, peptide arrays, tissues.
Experimental Design: Informed by the project questions—which species to study, TMA vs full format, need for multiplex/cell ID, and need to rule out off-target/close family members.
Once the above is available and has been considered, the lab is ready to begin the assay development phase.
Assay Development
Goals: Fit-for-purpose assay that can specifically detect expression of a protein and/or gene with sufficient sensitivity, in the sample matrix and species of interest.
Molecular Pathology scientists iterate in the lab to identify and qualify which reagent(s) and conditions can detect the target with sufficient sensitivity in the matrix and species of interest.
Scientists must confirm the assay is fit-for-purpose for the context of use with confidence as high as needed to ensure later results are interpretable and defensible scientifically.
Iterative assay development until conditions are sufficient to move to data-generation phase.
Data Generation
Goals: Application of fit-for-purpose TEP assays to generate data with sufficient coverage and granularity of tissue microanatomy and cell identification, of sufficient quality and confidence for decisional application on project support and regulatory submissions.
It is recommended that TEP data are generated and captured following structured raw data-generation principles to enable cross target comparison and databasing compatibility. For instance, raw data forms that systematically include annotations of positive/negative, pattern (membrane, cytoplasmic, nuclear, other), clearly defined scores (+1, +2, +3, etc), organ, structure, and cell ID using medical controlled lexicon (eg, epithelial cell, exocrine acini, pancreas).
As data emerge, additional wet lab activities may be necessary—eg, to confirm specificity with ISH; to confirm cellular ID beyond morphology (application of multiplex immunohistochemistry (IHC) or immunofluorescence (IF) with molecular ID markers).
Iterative data generation until the data package is sufficient to move to data communication phase.
Data Communication
Goals: Clear, concise, and complete account of where the target of interest is expressed (protein and/or gene) and the materials and methods used to derive them.
Format: Informal communication using PowerPoint slides are frequently used to communicate across internal stakeholders. Formal technical reports, typically published in regulated repositories, are used for official communications such as inclusion in regulatory submissions.
Scientists and pathologists supporting TEP studies must ensure the deliverables are fit-for-purpose for the project needs, are timely and of decisional quality.
Communication materials must provide all the necessary details for reconstruction of the experiments used to generate the data, following data integrity principles and rigorous laboratory record keeping practices.
Communication materials must include details to address questions such as:
What is the target profile (pattern of spatial distribution, which cells, in which organs, in which species)?
What are species differences? This is critical as they may impact their application as experimental models.
In summary, antigen-specific targeting by cytotoxic cells through various modalities are effective therapeutic approaches with unique safety considerations. A robust understanding of target expression in normal tissues is key to contextualizing safety risks and favorable risk to benefit profiles for this modality. This knowledge is a product of a well-planned workflow that integrates literature, databases and harnesses the expertise and capabilities of a bespoke investigative pathology laboratory to generate gene and protein expression information with anatomical and cellular spatial resolution. Outlined above are points to consider and a suggested workflow that ensures the timeliness and decisional quality of data sets based on fit-for-purpose assays with qualified performance on sensitivity and specificity and context of use (species, tissue matrix, anatomical coverage).
Off-Target Screening of Biologics and Chimeric Antigen Receptor T-Cells: New Food and Drug Administration Guidance and Challenges
The safety assessment of biologics is paramount in their development and clinical application. The recently released FDA guidance in January 2024 has introduced new perspectives and challenges to off-target screening of cell therapies like CAR T-cells. 19 The methodologies, challenges, regulatory considerations, and frequently asked questions in off-target screening of biologics in general are discussed, emphasizing the latest FDA guidance and the advantages of a combined approach.
Safety Considerations for Biologics
Biologics, including antibodies, nanobodies, and single-chain variable fragments (ScFvs), typically exhibit toxicity due to exaggerated pharmacology or immunogenicity. However, off-target effects, where biologics bind to unintended antigens, may pose significant risks. For CAR T-cells, the risk of cell distribution and persistence in off-target sites must be explored, in addition to inappropriate cell differentiation, changes in cell behavior, uncontrolled proliferation, and immune reactions.
Regulatory Guidance and Assessment Strategies
The FDA’s January 2024 guidance on CAR T-cells 19 outlines comprehensive strategies for assessing potential on-target/off-tumor and off-target toxicities. The key points include as follows:
On-Target Off-Disease Effects: The guidance emphasizes understanding the potential for CAR T-cells to affect non-tumor tissues that express the target antigen, besides off-target binding.
Assay Types: Sponsors are encouraged to use a combination of assays, including tissue-based (ie, Tissue Cross Reactivity [TCR] studies) and cell/protein array-based assays, functional assays on cell lines (cytotoxicity/cytokine release tests), and even relevant animal models (in vivo studies) to thoroughly assess off-target effects.
Method Integration: The FDA advocates for an integrated approach, combining multiple methodologies to provide a robust safety assessment and best inform the strategy to devise in clinical trials.
Challenges of Tissue-Based Assays (Cross-Reactivity Studies)
Tissue Cross-Reactivity Studies are screening assays based on immunohistochemical techniques performed on frozen tissue sections. More specifically, for CAR T-cells, investigators typically use the monoclonal antibody or ScFv from which the antigen recognition domain cell is derived.
In-depth understanding of the design and major practical aspects have been published, 56 and regulatory agencies have also provided some guidance, such as the tissue list to investigate and some quality endpoints.16,21,22,43 In essence, TCR projects are usually split into a preliminary study or phase to develop/optimize and qualify the IHC method and the main Good Laboratory Practices (GLP) study, performed before, during or after the toxicity studies, prior to clinical trials.
Although TCR studies have been conducted for over 20 years, some questions remain about the best approaches and the most frequently asked questions about TCR studies in the development of biologics in general are listed in Table 1.
Frequently asked questions poorly covered in the literature regarding TCR studies and biologic in general.

When it comes to the qualification of IHC methods, there are currently no specific and standardized guidelines, at least in the preclinical field, leading to variability in methodologies across different laboratories. As a result, practices can vary significantly from one site to another. The IHC can be considered analogous to an enzyme-linked immunosorbent assay (ELISA) assay performed on tissue sections. However, when comparing the validation parameters for ELISA assays, the differences are substantial. The key parameters highlighted in the literature are specificity, sensitivity, and tissue section stability. 10 Those requirements can be rephrased differently: it is crucial to develop a sensitive method with low background noise and adequate morphological preservation. Achieving this involves selecting relevant positive control systems and ensuring the sensitivity of the detection system. In addition, the quality and availability of the tissues are paramount. Managing tissue quality involves rigorous quality control, appropriate storage, and compliance with national regulations on anonymity, consent, and biological safety.
Cell-Based Assays and Protein Arrays
Cell-based assays and protein arrays are becoming increasingly popular for off-target screening due to their ability to provide detailed insights into protein-protein interactions. Technologies like Retrogenix (Charles River, High Peak, UK) and Integral Molecular (Philadelphia, Pennsylvania) use cell-based systems, whereas the HuProt technology employs protein arrays. These platforms allow for the screening of thousands of human membrane and secreted proteins, identifying potential off-target interactions effectively.
The Retrogenix assay is a powerful cell-based screening method used to identify off-target interactions. The principles of this assay include as follows:
Library Construction: A comprehensive library of expression vectors encoding approximately 6500 human membrane and secreted proteins is constructed.
Reverse Transfection: These vectors are spotted onto specialized slides, and HEK293 cells are seeded over the slides. As the cells grow, they become transfected with the vectors, resulting in the overexpression of the encoded proteins on the cell surface.
Binding Assay: The test article, such as a CAR T-cell or ScFv, is added to the transfected cells. The interaction between the CAR T-cells and the expressed proteins is monitored using fluorescently labeled detection reagents.
Detection and Analysis: Specific binding events are detected through fluorescence readouts. Hits are identified by comparing the binding profile of the test article to control samples, revealing potential off-target interactions.
Secondary Screening: Primary hits are further validated through secondary screens and additional assays, such as flow cytometry, to confirm the specificity of the interactions.
Integration of Cell-Based and Tissue-Based Assays
Combining cell-based assays with TCR studies provides a comprehensive approach to off-target screening. Although TCR studies offer subcellular context, cell-based assays detail protein-protein interactions. This integrated approach aligns with the FDA’s 2024 guidance, enhancing the robustness of safety evaluations and can be combined with a bioinformatic analysis. This bioinformatic analysis will inform, for example, on RNA and protein expression levels in human tissues, disease traits associated with the protein, and the frequency of genome variations across ethnic populations. A practical illustration of the combined approach can be seen in a recent poster presentation, 54 which highlights the synergy between TCR studies and Retrogenix cell-based assays. Combining the TCR and Retrogenix results, the study offered a comprehensive view of the antibody’s off-target profile. The TCR study provided subcellular localization information, whereas the cell-based assay and bioinformatics added molecular and functional insights.
Advantages of the Combined Approach
Complementary Data: Tissue-based assays provide spatial information about where potential off-target binding occurs, whereas cell-based assays offer molecular details about the interactions, especially for membrane and secreted proteins. Cell-based assays may be performed in place of a TCR study when an IHC method cannot be developed or to further characterize positive hits. Conversely, tissue-based assays provide a morphological context and additional information (cytoplasmic binding).
Increased Confidence: Using both methods increases confidence in the safety data, as it combines histological and molecular perspectives, reducing the risk of overlooking potential off-target effects.
Regulatory Compliance: Following the FDA’s recommendations, an integrated approach ensures thoroughness, meeting regulatory expectations and facilitating smoother approval processes.
Comprehensive Risk Assessment: The combination allows for a more detailed risk assessment, covering a broader range of potential off-target sites and interactions.
Utility: The combined approach is interesting for all biologics and CAR T-cells, in particular for innovative constructs, for new not well-characterized targets and when there is no relevant preclinical species.
Functional Assays on Cell Lines
Based on TCR and/or protein array results and/or in silico expression analysis, functional assays on cell lines play a crucial role in de-risking any identified off-target potential organ/tissue/cell type. For example, CAR T-cells can be co-cultured with human healthy cells/induced pluripotent stem cells to assess potential safety risks. Doing so, target expression is verified, and CAR T-cell–mediated cytotoxicity and T-cell activation are assessed. These assays evaluate the functional impact of the test article on various cell types, by monitoring any off-target interactions that may affect non-target cells and providing insights into potential cytotoxicity and activation (cell proliferation) effects.
In Vivo Models
As indicated in the FDA guidance, in vivo studies using immune-deficient animal models, such as cell line-derived xenografts (CDXs) and patient-derived xenografts (PDXs), may further inform on CAR T-cell activity and off-target effects. These models allow for the assessment of tumor growth, cytokine production, biodistribution, persistence, and potential off-target accumulation, providing critical data for clinical trial designs.
The new FDA guidance underscores the importance of a multifaceted approach to off-target screening for biologics, particularly CAR T-cells. By leveraging tissue-based assays, cell-based assays, functional assays on cell lines, and in vivo models, researchers can comprehensively evaluate potential off-target effects, ensuring adherence to regulatory standards and minimizing patient risks. This integrated approach is vital for advancing the development of safe and effective biologic therapeutics.
Risk of Chimeric Antigen Receptor Cell Tumorigenicity
In November 2023, the FDA issued a warning concerning tumorigenicity of CAR T-cell products based on 20 cases of T-cell malignancies, including CAR+ lymphoma, in patients treated with B-cell maturation antigen (BCMA) or CD19 autologous immunotherapies reported from clinical trials and/or post-marketing surveillance. Consequently, the FDA stated that the 15-year follow-up observational safety studies should be extended to life-long monitoring of treated patients.20,66 The FDA warning impacts viral vector products, suggesting the concern for tumorigenic transformation to be with integrating vectors such as Retrovirus (γ-RV) and Lentivirus (LV). Both viral vectors integrate “randomly” within the host genome with a long-lasting effect. The γ-RV preferentially integrates near transcriptional start sites such as regulatory elements (promoters, enhancers), DNA-se hypersensitivity sites (sites of open chromatin, hence accessible), and CpG islands (CpG islands may avoid DNA methylation). Moreover, integration occurs only in replicating cells. The LV integration preference changes depending on cell activity status of transduced cells (eg, different integration between resting and activated CD4+ T-cells). Viral vector integration can induce proto-oncogenes.
A panel of experts in the cell therapy field replied to the warning with a paper summarizing the currently available information regarding tumorigenicity associated with CAR T-cell administration and compiling questions still unanswered by the FDA. 58 Overall, although secondary neoplasia due to CAR T-cell therapy has occurred, the overall risk remains lower than that of other anti-neoplastic modalities. As of early 2024, about 34,400 patients in total were treated with FDA-approved CAR T-cell therapies, and so far, only 20 of them have developed a CAR-related T-cell lymphoma. 58
Secondary malignancies in patients with B-cell neoplasia, regardless of CAR T treatment, have a high incidence due to exposure to genotoxic chemotherapy, radiotherapy, and risk factors such as abnormal immune system and age. The most common secondary malignancies following CAR T-cell therapy in the clinics are non-melanomatous skin cancers and the average time of onset is about 9 months from the infusion. Most lymphomas observed after CAR T therapy have had the same phenotype as the primary malignancy so although several have been CAR+, they have been considered unrelated to the administered immunotherapy and instead were thought to be due to the presence of patient-derived neoplastic cells in the starting apheresate.27,49,58,66
The potential sources of tumorigenesis within CAR T-cells are host/patient related such as the presence of subclinical cell clones with transformative potential or residual neoplastic cells in the apheresate with risk of transduction.27,49,58,83 Although with the autologous product, the risk remains limited to the single patient, when donor cells (eg, NK cells) are used for allogeneic products intended to be “off the shelf,” hence suited for many different patients, the associated risk can potentially increase sensibly. As already mentioned above the age, the immune status and the replicative state of the cells of the donor are risk factors. A targeted mitigation strategy could include stratification of the donors based on health status (including ideally also blood screening for at least common blood neoplasms/pretransformative conditions, besides the current infectious disease panel), use of differentiated lymphocytes instead of peripheral blood mononuclear cells (PBMC), and age. During manufacturing, the transduction of the cells with viral vectors and their integration sites are another critical point. Insertion site analysis and cytokine-independent growth assays can be informative about the intrinsic risk of transformation and proliferation of the target-cell population. 41
In a few CAR T-cell preclinical toxicity studies, an atypical proliferation of human lymphocytes has been observed obliterating one or more organs and leading to sudden death or clinical deterioration and the need for euthanasia based on humane endpoints. The proliferation consists of sheets of rather monomorph round cells (approximately 10 µm in size), forming a space-occupying lesion. The proliferating cells display immunohistochemical positivity for human CD3, frequent mitosis effacing more often tissues like spleen and liver, resembling a round cell tumor. Limited investigation has been carried out on the proliferating cell subtype/s, clonality, and molecular signature. 74 Consequently, the possible role of vector transduction in determining or contributing to such proliferation remains to be elucidated.
The characterization of such proliferation and understanding of its pathogenesis by the preclinical pathologist might provide insight on its translatability to human patients. Approaches such as determining vector copy number within tumor samples, molecular localizations studies to confirm transduction of tumor cells, and lentiviral integration site analysis may be used to further investigate the potential role of vector integration in such cases.
Effector-Cell–Driven Immune Activation Syndromes
Although CAR T-cell therapies have been transformative for patients with certain refractory and relapsed heme malignancies, they can be associated with significant safety issues related to hyperstimulation of T-cells. Effector-cell–driven immune activation syndromes include the CRS, 32 IEC-HS also termed CAR MAS, 37 ICAHT syndrome, 79 and ICANS. 78 Preclinical safety assessment and risk prediction can be challenging for these immune activation syndromes due to lack of adequate in vitro and in vivo models, and patient characteristics that are not recapitulated in animals such as tumor burden, previous therapies, and co-morbidities. Limitations of current in vitro and in vivo models to predict CAR T-cell pharmacology and safety have recently been reviewed.53,59,77,84,85
Cytokine Release Syndrome
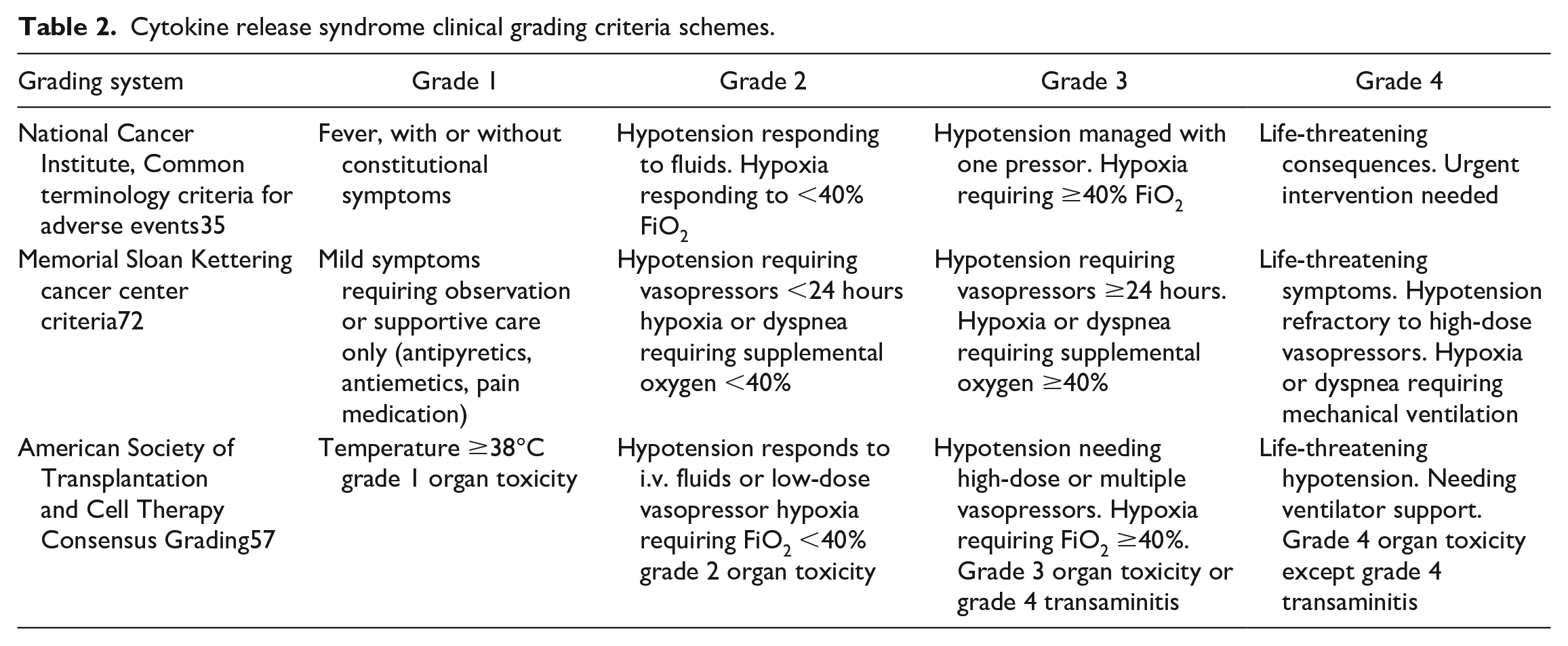
Cytokine release syndrome is a potentially life-threatening and dose-limiting toxicity observed with redirected T-cell therapies including CAR therapies. Several clinical grading criteria have been developed to assist in diagnosis, staging and clinical management of CRS (Table 1).35,57,72,88 Mild clinical signs are often initiated with fever and constitutional symptoms that can be managed with antipyretics and supportive therapy. These signs may progress to more significant changes centered on vascular dysfunction and injury resulting in progressive vasodilation, hypotension, and hypoperfusion that may require vasopressors and supplemental oxygen. In severe cases, hypoperfusion may result in end organ injury to the liver, kidneys, heart, and/or lungs. The central role of vascular injury in the pathogenesis of severe CRS is supported by biomarker analysis demonstrating increases in serum angiopoietin 2 (ANG2) and use of the endothelial activation and stress index (EASIX) as a prognostic marker for high-grade CRS.7,11,51 Elevated circulating levels of key proinflammatory lymphokines produced by activated CAR T-cells including tumor necrosis factor alpha (TNF-α), IFNγ, interleukin (IL)-2, and granulocyte-macrophage colony-stimulating factor (GM-CSF) may directly impact systemic vasculature or further activate bystander cells to produce additional cytokines such IL-6 and IL1-beta. 32 In addition to supportive measures, therapies directed at blocking specific cytokines such as use of the anti-IL6 receptor monoclonal antibody tocilizumab or more broadly immunosuppressive approaches such as use of corticosteroids have shown benefit in more severe cases. 32
Several patient and product characteristics have been associated with increased clinical risk and severity of CRS. Patient characteristics associated with increased risk and severity include high tumor burden, tumor type, lymphodepletion regime, baseline thrombocytopenia, and elevated serum C-reactive protein and/or ferritin. 91 Pre-existing endothelial activation and stress may identify patients at increased risk and may quantified using an EASIX score calculated from baseline lactate dehydrogenase (LDH), C-reactive protein (CRP) or creatinine, and platelet count. 51 Many of these patient characteristics are not duplicated in in vitro or in vivo models. Product characteristics that may also impact CRS risk include product dose, product target, CAR intracellular stimulatory domains, armored features, T-cell product phenotypic characteristics, and manufacturing process. 32 These product risk factors largely relate to rapid CAR T-cell activation and expansion that then drive excessive lymphokine production.
There are several in vitro and in vivo approaches that may be used to investigate CRS, and although these approaches may have value in understanding the mechanism of CRS, they need to be used cautiously in risk or safety assessment as they have significant limitations. 53 In vitro approaches may be used to look at cytokine production from CAR T and bystander cells; however, these do not duplicate the pharmacokinetic aspects of the “living drug.” In addition, it is difficult to translate in vitro cytokine production levels to in vivo effects, and the assays are highly dependent on the effector-cell to target-cell ratio. Moreover, there is a lack of influence from and on systemic tissues and an absence of complex negative feedback loops that operate to control excess cytokine production. For these reasons, translation of findings from in vitro models to understand patient CRS risk is difficult.
Humanized mouse models are the backbone of preclinical efficacy studies of CAR T-cell therapies. In these models, human tumor xenograft-bearing immunocompromised NOD-scid-gamma (NSG) mice are dosed with human CAR T-cell product to examine effects on tumor growth and elimination. 52 However, translation of CRS safety implications from humanized mouse models to human patients is difficult and is generally not assessed preclinically for CAR T therapies.59,77 Limitations are that xGvHD drives expansion and biodistribution of both CAR positive and negative cells during and after tumor control.52,77 There is a complex interplay between and mismatch of human/mouse cytokines and cytokine receptors in these models which may not replicate CRS pathogenesis. Moreover, the profiles of human and murine-derived cytokines are different from that observed in human patients. There is poor development of secondary lymphoid organs and deficient myeloid engraftment which may alter the impact of bystander cells to amplify or control lymphokine production. More complex models using different mouse strains such as NSG MHCI/II double knockout mice to decrease xGvHD and the CD34 humanized NSG-SGM3 mice expressing human IL3, GM-CSF (CSF2), and stem cell factor (SCF) (KITLG) to enhance myeloid engraftment and T-regulatory cell function have been developed. However, these do not correct many of these underlying deficiencies to model CRS risk.40,55,94
Non-human primate (NHP) models have been described to investigate CRS and ICANS pathogenesis and may be more relevant than humanized mouse models.4,62,89 Such models also have limitations and in general have not been a requirement from Health Authorities in regulatory submissions. In these models, human CAR T-cell product cannot be used as these cells are immediately rejected and instead, primate CAR T-cells must first be generated. For this, a surrogate vector with an simian immunodeficiency virus (SIV) capsid is required due to viral restriction factors such as TRIM5 or one must use a non-restrictive primate species such as a pigtail macaque. Surrogate vectors continue to utilize elements optimized for human T-cells such as human CD3 zeta and costimulatory domains which may not interact with NHP signal pathways in similar fashion. In addition, factors known to increase risk of CRS in human patients may not be recapitulated in NHP models. For example, there is an absence of tumor burden to drive CAR T-cell expansion in vivo, and there are differences in human and NHP CAR product phenotype. Finally, there is an absence of previous therapies and co-morbidities which may impact CRS. Nonetheless, in models using an SIV surrogate lentiviral vector engineered to express an anti-CD20 CAR, CAR T-cell expansion, depletion of target B-cells, and clinical signs associated with elevated serum IL-6, IL-8, IL-1RA, CXCL9, and Interferon-inducible T cell alpha chemoattractant (I-TAC) levels have been observed. 89
Immune Effector-Cell Hemophagocytic Lymphohistiocytosis-Like Syndrome
The IEC-HS is a hyperinflammatory entity distinct from CRS characterized by cytopenia, hyperferritinemia (>2 times the upper limit of normal), coagulopathy with hypofibrinogenemia, and elevated transaminases. 37 This condition, also termed CAR MAS, is less common than CRS, may develop several days to weeks following resolution of CRS symptoms and may require different intervention strategies. 28 The incidence varies dependent on the cancer epitope targeted, CAR T-cell product administered, and neoplastic condition treated. Excess macrophage activation through increased and prolonged elevations in IFNγ has been implicated in the pathophysiology of IEC-HS. 86
Immune Cell Activation Hematotoxicity Syndrome
Cytopenias (neutropenia and thrombocytopenia) and subsequent increased risk for infectious disease and major bleeds are an important cause of non-relapse morbidity and mortality in CAR T-cell therapy patients.26,50,68 The cause of cytopenia in patients receiving CAR T-cell therapies is complex and may involve the use of lymphodepletion regimes, previous chemotherapeutic drugs, neoplastic infiltration of the bone marrow, and the impact of proinflammatory cytokines on hematopoietic stem and progenitor cells. Multivariate analysis has revealed that higher CRS grade, higher peak CRP, and longer duration of elevated CRP are associated with increased risk of prolonged hematotoxicity. 65 Moreover, recent studies have reported that severe CRS and higher IL-6 serum concentrations were associated with prolonged cytopenia following CAR T-cell therapy.47,63,64 Sustained increases in proinflammatory cytokines such as IFNγ may displace hematopoietic stem cells from the bone marrow niche and lead to loss of activated hematopoietic stem and progenitor cells.25,47 Like CRS, preclinical in vitro and in vivo models to assess IEC-HS and ICAHT risk and its mitigation are currently lacking.
Underlying Immune Synapse Defects in Pathogenesis of Cytokine Release Syndrome and Related Hyperinflammatory Syndromes
The redirected T-cell cytolytic synapse is not a conventional immune synapse and has been termed a non-classical cytotoxic synapse. 12 Work has now begun to understand differences in structure and function of these non-classical synapses and how CAR design might influence synapse formation and downstream signaling. There are several mutations recognized in genes responsible for cytotoxic effector function which are associated with failed target cell-killing and exaggerated cytokine responses. The best characterized of the resulting conditions is type 2 familial hemophagocytic lymphohistiocytosis caused by a mutation in the perforin gene. 45 Infants with this condition develop a rapidly fatal CRS/MAS upon contact with common childhood infections. Imaging studies have demonstrated that although T-cells in this condition are able to engage target cells, they are unable to kill the virally infected cells and instead go through repeated cycles of calcium flux resulting in persistent-activation and excessive cytokine production. 48 These findings suggest that defects in CAR-mediated immune synapse formation may also underlie upstream events in redirected T-cell CRS pathogenesis.
The cytotoxic synapse consists of complex spatially and temporally organized domains leading to reorganization of the cytoskeleton and activation of numerous signaling pathways. In vitro data indicate that the cytolytic synapse formed between effector and target cells with redirected T-cell therapies including CAR therapies may be dysfunctional and associated with reduced efficiency and excess T-cell activation and cytokine production. The non-classical cytotoxic synapse is disorganized forming a multifocal signaling cluster rather than the spatially and temporally organized single cluster observed with a true TCR-mediated cytotoxic synapse.12,17 A well-defined peripheral supramolecular activation complex (pSMAC) does not form and LFA-1, a key pSMAC adhesion molecule at the effector-cell target-cell interface, does not form a distinct ring structure. 3 As a result, T-cell activation kinases, Lck and ZAP70, do not coalesce into a clearly defined structure. Construct engineering and pharmacological intervention may improve synapse effector function and reduce T-cell activation and cytokine production. Such approaches could improve efficacy and mitigate risk of CAR T-cell therapy hyperinflammatory syndromes.
Immune Effector-Cell–Associated Neurotoxicity
The ICANS is a significant complication associated with CAR T-cell and T-cell activating therapies. Clinically, ICANS manifests with a range of neurological symptoms such as encephalopathy, confusion, aphasia, myoclonus, and other central nervous system (CNS) disorders. The American Society for Transplantation and Cell Therapy (ASTCT) has developed a specific grading scale to standardize the assessment and management of ICANS, reflecting its clinical importance. 57
Epidemiology of Immune Cell Activation Neurotoxicity Syndrome
The incidence of neurotoxicity following CAR T-cell therapy ranges from 37% to 77%. Symptoms typically begin 3 to 10 days after infusion and usually last between 1 and 19 days. 31 Although most cases are reversible, approximately 1% to 3% can be fatal despite aggressive medical management. 30 Clinically, aphasia is the most frequently observed symptom, followed by headache and encephalopathy. Other neurological manifestations may include delirium, hallucinations, ataxia, focal weakness, paresis, peripheral neuropathy, seizures, increased intracranial pressure, and cerebral edema. 31
Clinical Assessment of Immune Cell Activation Neurotoxicity Syndrome
The clinical screening and grading of ICANS severity includes assignment of an immune effector-cell–associated encephalopathy (ICE) score. The ICE score assessment includes testing orientation, level of attention, ability to name common objects, and to follow simple commands. In addition to the ICE score, factors involved in assigning an ICANS severity grade include patient level of consciousness, presence of seizures, motor findings (weakness, paresis), and elevated intracranial pressure. 57
The CNS diagnostic modalities such as magnetic resonance imaging (MRI), electroencephalogram (EEG), and cerebrospinal fluid (CSF) analysis are commonly employed in ICANS assessment, but findings tend to be non-specific. The MRI is often normal, but local hypoperfusion, T2/fluid-attenuated inversion recovery (FLAIR) hyperintensities, and/or cerebral edema have all been described. In severe ICANS cases, MRI may reveal vasogenic edema, leptomeningeal enhancement, or multifocal microhemorrhages. 8 The EEGs typically show generalized background slowing, abnormal rhythms, periodic discharge patterns, and occasionally, seizure activity. 6 Analysis of CSF usually reveals pleocytosis and increased protein. Histopathological findings from patients who have succumbed to ICANS, although seldom reported, align with severe MRI findings, including microthrombi, microhemorrhage, perivascular mononuclear cell infiltrates, gliosis, and expansion of perivascular spaces/leakage of fibrinous fluid into surrounding neuroparenchyma (consistent with cerebral edema).34,92
Pathogenesis of Immune Cell Activation Neurotoxicity Syndrome
Although the pathogenesis of ICANS has not been determined, predisposing factors and predictive biomarkers suggest that immune cell activation and endothelial cell dysfunction play a role in disease development.
Role of Immune Activation in the Pathogenesis of Immune Cell Activation Neurotoxicity Syndrome
The CRS and ICANS are closely related. Most patients who develop ICANS have previously experienced CRS, with ICANS symptoms typically emerging shortly after the peak and subsequent decline of CRS. Like CRS, factors such as receiving high doses of CAR T-cells, having a high tumor burden, or experiencing rapid and/or persistent expansion of CAR T-cells in the peripheral blood increase the likelihood of developing ICANS. 9 Furthermore, biomarkers of immune activation, including rapid increases in IL-6 levels and elevated levels of C-reactive protein, ferritin, and lactate dehydrogenase in the peripheral blood, also indicate a higher risk of ICANS.2,39,81 Although the link between CRS and ICANS is most prominently documented in CAR T-cell therapy, the association between immune activation and neurotoxicity is not a new concept. Neurotoxicity syndromes like ICANS have been observed for the past 40 years in patients undergoing T-cell activating therapies. For instance, a condition known as “OKT3 encephalopathy” has been noted in organ transplant recipients.70,75,76,80 The OKT3, a monoclonal antibody used to counter acute organ transplant rejection, activates CD3 on T-cells, triggering cytokine release and subsequent T-cell depletion from the bloodstream. Some patients treated with OKT3 have exhibited neurological symptoms such as somnolence, reduced mental function, seizures, multifocal cerebral blood flow deficits, and generalized edema approximately seven days after administration. Similarly, patients treated with recombinant IL-2 or IL-2-activated T-cells have shown neurological, behavioral, and cognitive impairments around 3 to 4 days following treatment. Notably, clinicians have observed several common features between post-IL-2 infusion neurotoxicity and transient ischemic attacks.5,13
Role of Endothelial Cell Dysfunction
Two independent seminal reports have associated ICANS with endothelial cell dysfunction.34,81 Elevated biomarkers indicative of endothelial dysfunction and consumptive coagulopathy, such as ANG2, von Willebrand factor, prolonged activated partial thromboplastin time, activated thrombin clotting time, D-dimers, reduced plasma fibrinogen, and thrombocytopenia, have been observed in patients with ICANS. The presence of microthrombi and microhemorrhages in the brains of these patients suggests that endothelial dysfunction, due to immune activation, could be a contributing factor to ICANS. However, a subsequent study on pediatric ICANS patients indicated no clear link between endothelial dysfunction and neurotoxicity. 33
Role of Therapeutic Target in the Pathogenesis of Immune Cell Activation Neurotoxicity Syndrome
The ICANS has been observed in association with various therapeutic targets such as CD19, BCMA, CD22, and GPRC5D, with the most frequent occurrences noted in therapies targeting CD19. Several hypotheses have been proposed to explain this observation. One reason could be the higher number of approved CD19-targeting therapies compared to other targets, potentially leading to a perceived increase in ICANS cases associated with CD19. In addition, CD19’s widespread expression on normal B-cells might mimic the effects seen in therapies used in high tumor burden scenarios, which are known to predispose patients to ICANS. A recent publication reports that CD19 is expressed on a rare subset of pericytes in the brain. 71 However, this finding is primarily based on single-cell RNA sequencing of fetal brain tissues, and the relevance of this finding in postnatal brain is questionable. Additional evidence presented by the authors, such as immunohistochemical labeling for CD19 in brain sections, does not convincingly show that CD19 is expressed by pericytes in adulthood.
Preclinical In Vivo Models of Immune Cell Activation Neurotoxicity Syndrome
Several animal models of ICANS have been documented in scientific literature (Tables 2 and 3). However, only one mouse model and a non-human primate model have recapitulated many of the clinical characteristics of ICANS.
Cytokine release syndrome clinical grading criteria schemes.
Animal models of neurotoxicity that have been described in the literature.

Infusion of Mouse-Derived Anti-CD19 Chimeric Antigen Receptor T-Cells Into Immunocompetent Non-Tumor-Bearing Balb/c Mice
In this mouse model, neurological dysfunctions such as impaired postural adjustment, balance issues, and reduced exploratory behavior were observed. 18 These symptoms were linked histologically to the presence and severity of multifocal microhemorrhages in the brain. Further studies using two-photon in vivo imaging revealed that these hemorrhages resulted from the blockage of medium-sized cerebral capillaries by increased leukocyte rolling and adhesion to the endothelial lining. The model did not assess blood flow in capillaries outside the brain or markers of endothelial dysfunction. Despite its potential to enhance understanding of ICANS pathogenesis, the model’s reliance on a proprietary lentiviral vector for producing mouse anti-CD19 CAR T-cells limits its wider use in the field.
Infusion of Rhesus Monkey-Derived Anti-CD20 Chimeric Antigen Receptor T-Cells Into Immunocompetent Non-Tumor-Bearing Rhesus Monkeys
In this non-human primate model, symptoms such as tremors, lethargy, and slowed or ataxic movements were observed in monkeys 7 to 10 days after the infusion of CAR T-cells. 90 In addition, convulsions were noted in one subject. The variability in the severity of neurological signs was significant, mirroring clinical observations, with the most severely affected animals showing elevated levels of ferritin and lactate dehydrogenase. However, it is important to note that many of the observed clinical signs could be indicative of general sickness behaviors. Assessments such as serum chemistry, coagulation panels, and markers of endothelial cell activation were not conducted in this study. Owing to high costs and ethical considerations, the widespread application of this model in studying ICANS pathogenesis and developing intervention strategies is limited.
Alternative Models for Studying Immune Cell Activation Neurotoxicity Syndrome Pathogenesis
To date, the complexity of published preclinical in vivo models of ICANS has hindered detailed studies of specific factors contributing to disease pathogenesis. The research community could benefit from simpler models that focus on immune and endothelial cell activation to clarify their roles in neurotoxicity. For instance, a surrogate molecule for OKT3 that is effective in mice could be utilized to explore the occurrence of neurotoxicity during straightforward T-cell activation, helping to pinpoint factors that increase the likelihood and severity of the disease.1,23,38 In addition, exploring the pathways of CD40 and TLR7 agonism is promising, as both have been shown to induce effects in mice that resemble ICANS pathology.14,42,69,73,96
The ICANS frequently occurs following therapies that activate immune cells. Although it is usually self-limiting, it can sometimes become severe or even fatal. The ICANS is associated with CRS and may also involve endothelial cell activation. The mechanisms underlying its pathogenesis are still being explored. Currently, there are only a few in vivo preclinical models available for studying its pathogenesis and testing intervention strategies.
Conclusion
Over the past two decades, CAR T-cell therapies have significantly advanced the treatment of hematologic malignancies, offering highly targeted, patient-specific interventions. Despite CAR T-cell’s transformative potential, these non-traditional therapies face substantial challenges, including complex safety assessments and the management of toxicities related to off-tumor effects and immune responses. Continuous advancements in understanding CAR target biology, improving manufacturing processes, and refining preclinical models are essential to enhance the safety and efficacy of CAR T adoptive cell therapies.
Footnotes
Author Contributions
All authors conceived, wrote, and revised the ideas presented within this manuscript.
Declaration of Conflicting Interests
FG works at Charles Rivers Laboratories the vendor of Retrogenix technology. The author(s) declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.