
Abstract
Reticulum cell hyperplasia (RCH) was a term used for many years by the National Toxicology Program (NTP) to describe a certain non-neoplastic bone marrow lesion of rats. Retrospective microscopic evaluation of RCH lesions and immunohistochemistry analyses were performed to reassess and further characterize these lesions. The NTP database was searched to identify femoral bone marrow specimens diagnosed with RCH from 1981 to 2014 (n = 254). The diagnosis last occurred in 2003, after which the term “cellular infiltration” was used. Eighty-three RCH slides, spanning 22 years, representing 34 different chemicals, were selected for microscopic review, and a subset (23) was chosen for ionized calcium binding adapter molecule 1 (Iba1) immunohistochemical staining; initial investigations revealed Iba1 worked as a macrophage marker on decalcified tissue. The following diagnoses were made upon reevaluation: 36 were consistent with cellularity increased, macrophage, 22 with histiocytic sarcoma, 8 with increased myeloid cells, 4 with autolysis, and 13 were normal appearance. All 23 RCH lesions stained positive for Iba1. Fifty-eight of 83 bone marrows previously diagnosed with RCH are consistent morphologically and immunohistochemically with cells of histiocytic origin. These results will help with interpretation of historical data and demonstrates that Iba1 can be used in decalcified bone marrow sections.
Introduction
In the 1880s, scientist Elie Metchnikoff—Nobel Prize recipient (1908) and the forefather of cellular immunity—identified certain mononuclear cells as phagocytic. He recognized that these cells were important for a host’s resistance against infections and was the first to classify them as macrophages. 1,2 He also recognized the close relationship between the phagocytic cells of the spleen, liver, lymph node, and bone marrow, which led to the introduction of the term “macrophage system.” 1 It was studies of Metchnikoff and others that formed the basis for the concept of the so-called reticuloendothelial system (RES) described by Aschoff in 1924. 3 The RES was considered a body of mononuclear cells identified by their ability to uptake vital dyes and particulate matter (eg, colloidal gold, iron oxide), which at the time Aschoff thought was exclusively the result of phagocytosis. The ingestion and clearance of unwanted particulate material from the blood was deemed to be the main function of the RES. 4 At that time, the RES included reticuloendothelial cells of the lymph and blood sinuses; reticular cells of the spleen and lymph nodes; monocytes and histiocytes.
The term reticuloendothelial originated from the fact that the cells in the system were involved in forming the reticulum (ie, a netlike structure) of the lymph nodes and spleen, or were in close proximity to vascular endothelial cells. 4,5 Within years of its inception, however, the concept of the RES came under scrutiny for several reasons. For example, the term reticuloendothelial was considered inappropriate or confusing by some because vascular endothelial cells are morphologically and functionally different from histiocytes and the so-called reticular cells. In addition, the cells included in the RES did not originate from the same cell lineage. 2 It was also realized that poorly phagocytic (facultative) cells (eg, endothelial cells) can uptake substances by pinocytosis or endocytosis, thus, such labelling was unreliable as a criterion for the identification of mononuclear phagocytes. 2 Armed with a better understanding of macrophage morphology, function and kinetics, it was recommended in 1969 by Furth et al that the system be called the “mononuclear phagocytic system” or MPS. 2 The modern-day MPS components are monocytes, macrophages (histiocytes), and dendritic cells. 6
With the paucity of knowledge at the time, the function and origin of many of the cells of the RES was erroneous or confused. In particular, the term “reticular cell” was applied over the years to a variety of cells that have now been identified as lymphocytes, hematopoietic precursor cells, adventitial cells, fibroblasts, and most recently, dendritic cells, as well as being used synonymously with histiocytes. 5,7 –9 Adding to the confusion was the term “reticulum,” which was used in lieu of the term “reticular” by some investigators. In addition, throughout the years, the term “reticulum cell” was applied to cells with long cytoplasmic processes that built a network (reticular tissue or reticulum); cells that connect to or produce reticulin; or stromal cells of the hematopoietic organs. 5,7 The use of the word reticulum has been phased out or replaced as cells have been more definitively identified. For example, dendritic reticulum cells are now referred to as follicular dendritic cells and interdigitating reticulum cells are now referred to as interdigitating dendritic cells. 10 The word reticular is still used in reference to some cells in the lymph node and bone marrow, such as fibroblastic reticular cells in the lymph node and reticular cells (thought to be fibroblasts by some) of the bone marrow. 10,11
In Thelma Dunn’s 1954 publication “Normal and pathologic anatomy of the reticular tissue in laboratory mice, with a classification and discussion of neoplasms,” organs of reticular tissue included lymph nodes, thymus, spleen, and bone marrow. 12 Three so-called potentially phagocytic cells were designated as elements of reticular tissue—reticulum cells, histiocytes, and monocytes. Specifically, reticulum cells were defined as “solitary fixed cells forming the cellular elements of the reticular framework of the main reticular organs.” The 3 cell types, however, were also confoundedly referred to as a whole to be reticulum cells. According to Dunn, the condition of reticulum cell hyperplasia (RCH) developed in cases of persistent inflammation where “reticulum cells accumulate in greater numbers”—the reticulum cells being described as “free macrophages, often with vacuolated cytoplasm.” Additionally, the term macrophage or histiocytic hyperplasia was never used in Dunn’s publication. It is clear that the use of the words reticulum and reticular was fraught with confusion and uncertainty over the years.
Reticulum cell hyperplasia was a term used for many years by the National Toxicology Program (NTP) to describe a certain non-neoplastic bone marrow lesion of rats. Diagnosis of this lesion indicated the presence of focal to broadly diffuse areas of large cells characterized by an abundant cytoplasm that may contain vacuoles or appear foamy with irregular, indistinct cell borders and a round to bean-shaped nucleus. Review of the NTP database revealed that the term RCH was first used by the NTP in 1975. The term is no longer utilized at the NTP and a cursory reevaluation of previous RCH lesions was consistent with histiocytic cellular infiltration (current NTP terminology) or cellularity increased, macrophage (INHAND terminology). 13 The goal of the current study was to microscopically reevaluate previously diagnosed RCH lesions of rat bone marrow and perform immunohistochemical (IHC) staining to further assess and characterize the cells of this lesion. This study was not designed to investigate the prevalence, incidence or significance of RCH in NTP studies. Since the archived bone marrow tissue was acid-decalcified for processing, a preliminary study evaluating the efficacy of several IHC histiocytic markers on decalcified bone marrow specimens was performed.
Materials and Methods
Preliminary Study
Animal use was in accordance with the Guide for the Care and Use of Laboratory Animals 14 in a facility accredited by the Association for Assessment and Accreditation of Laboratory Animal Care. Since it is known that many IHC markers do not work well with hydrochloric acid decalcified bone marrow tissue, 15 a preliminary study was performed to evaluate the ability of the histiocytic markers, ED2 (CD163), CD68, and ionized calcium binding adapter molecule 1 (Iba1; Table 1), to stain bone marrow of decalcified rat femurs. Three female Sprague Dawley rats were euthanized (CO2/O2 inhalation) and both femurs immediately collected and fixed in 10% nonbuffered formalin for 48 hours. Following fixation, one femur from each of the 3 rats was decalcified for 24 hours with Decal™ Decalcifier (Decal Chemical Corp, Suffern, New York), which is a combination hydrochloric acid, EDTA (gentle) decalcifier. The other femur from each rat was decalcified for 4 hours using a hydrochloric acid method (RDO Rapid Decalcifier; Apex Engineering Products Corporation, Aurora, Illinois). For comparison, the core bone marrow tissue from the 2 femurs of another rat were removed intact (ie, scooped out), fixed solely in formalin, and processed for paraffin embedding. Of the 3 stains, Iba1 was the only IHC marker that positively stained all 3 bone marrow fixation methods (data not shown). Therefore, only Iba1, and not ED2 and CD68, was used in the main study.
Details of the Immunohistochemistry Staining Methods.
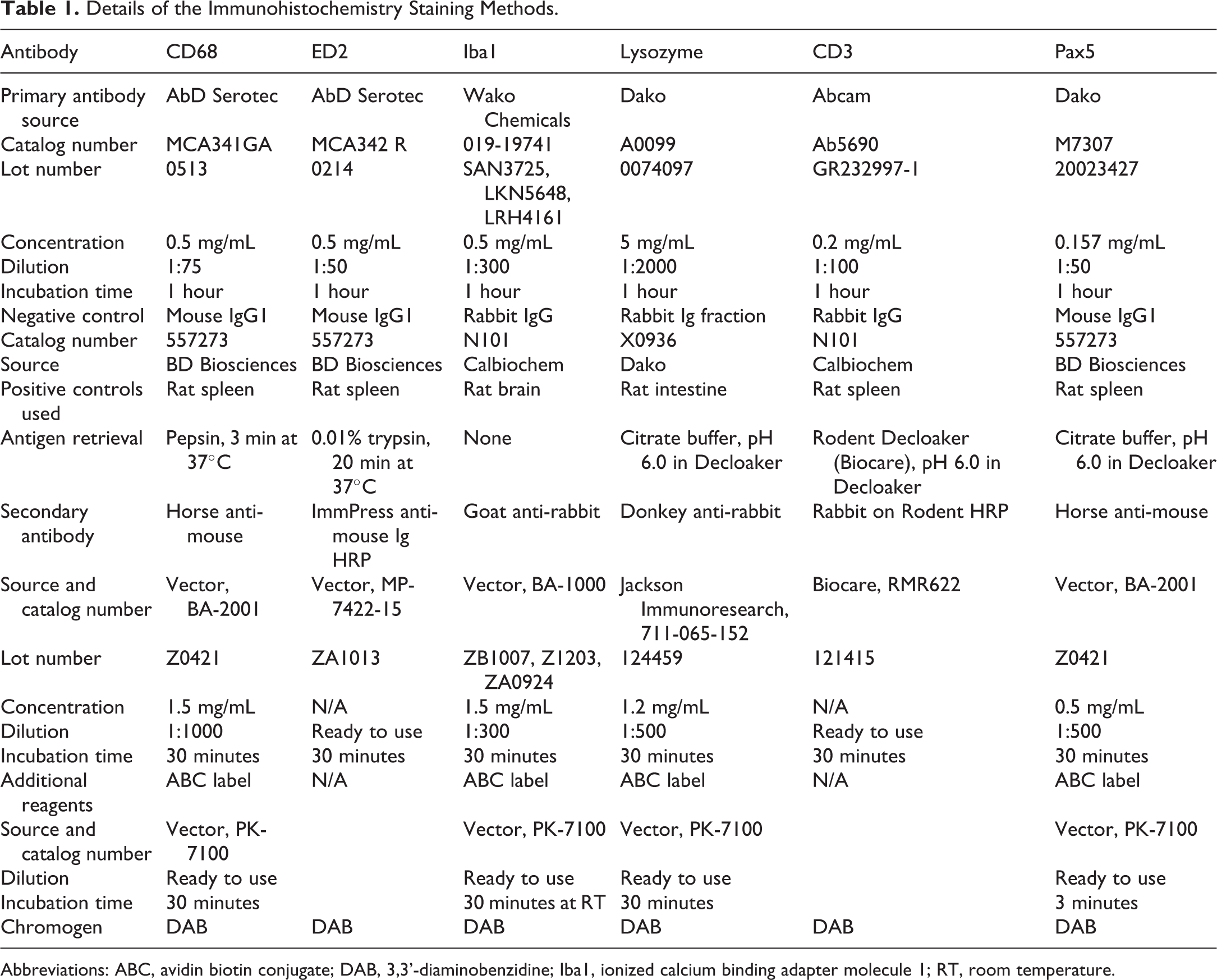
Abbreviations: ABC, avidin biotin conjugate; DAB, 3,3’-diaminobenzidine; Iba1, ionized calcium binding adapter molecule 1; RT, room temperature.
Main Study
National Toxicology Program’s Toxicology Data Management System Enterprise (TDMSE) database was searched to identify rat femoral bone marrow specimens diagnosed with RCH between the years of 1981 and 2014. A total of 254 rat bone marrow specimens were identified (all in F344/N rats) as being diagnosed with RCH in the TDMSE database—the majority of which (213) were between the years 1981 and 1989. The diagnosis of RCH last occurred in 2003, after which the term “cellular infiltration” was exclusively used. Of the 254 bone marrow specimens diagnosed with RCH, 83 were selected for microscopic review (Supp Table 2) of the archival hematoxylin and eosin (H&E) slide. The slides for review were chosen to represent a variety of years, chemicals, and severity grade, and spanned 22 years encompassing 34 chemicals and included 3 severity levels (mild, moderate, severe); slides included control and treated animal groups. Because paraffin tissue blocks dated before 1985 were disposed of per NTP protocol at the time, tissue block availability was limited for studies with start dates on or before 1983. Thus, of the 83 reevaluated archival slides, 23 available specimens (see results section) were chosen for IHC staining with Iba1 antibody (Supp Table 2). Based on tissue block availability, specimens were chosen to represent various years, chemical, and dose groups. In addition to Iba1, sections were also stained with lysozyme, and the lymphocyte markers of CD3 and Pax5 (Table 1) with the understanding that these stains may fail to work on the acid-decalcified archival paraffin tissue blocks. For IHC slide preparation, the paraffin blocks were sectioned at a thickness of 3 µm. Archival H&E and immunohistochemically stained slides were evaluated by authors M.C.C. and K.S.J.
Results
The following diagnoses were made upon reevaluation of the 83 slides (Supp Table 2): cellularity increased, macrophage (36), histiocytic sarcoma (HS; 22), increased myeloid cells (8), autolysis (4), and normal (13). Cellularity increased, macrophage was defined as focal areas of large cells characterized by an abundant cytoplasm that may contain vacuoles or appear foamy with irregular, indistinct cell borders and a round to reniform nucleus (Figure 1). These cells were intermixed with the normal bone marrow cells. Histiocytic sarcomas effaced the normal architecture of the bone marrow and were composed of sheets of closely packed polygonal to round cells with indistinct cell borders, moderate to abundant eosinophilic, variably vacuolated cytoplasm. Moderate anisocytosis and anisokaryosis was present. Multinucleated giant cells were sometimes observed. Increased myeloid cells was diagnosed when there was an overall increase in the number of myeloid cells. Normal cellularity and increased myeloid cells are common diagnoses and easily identified on H&E slides, thus it was decided that staining these particular diagnoses with IHC markers would not be more informative or add value. Of the remaining diagnoses of cellularity increased, macrophage and HS, 23 representative specimens were selected for IHC; 14 of the 23 had been reevaluated as cellularity increased, macrophage and 9 with HS. All 23 slides stained positive for Iba1 (Figures 1 and 2). While our positive control materials demonstrated the assays worked properly, none of the selected sections stained positive for CD3, Pax5, or lysozyme.
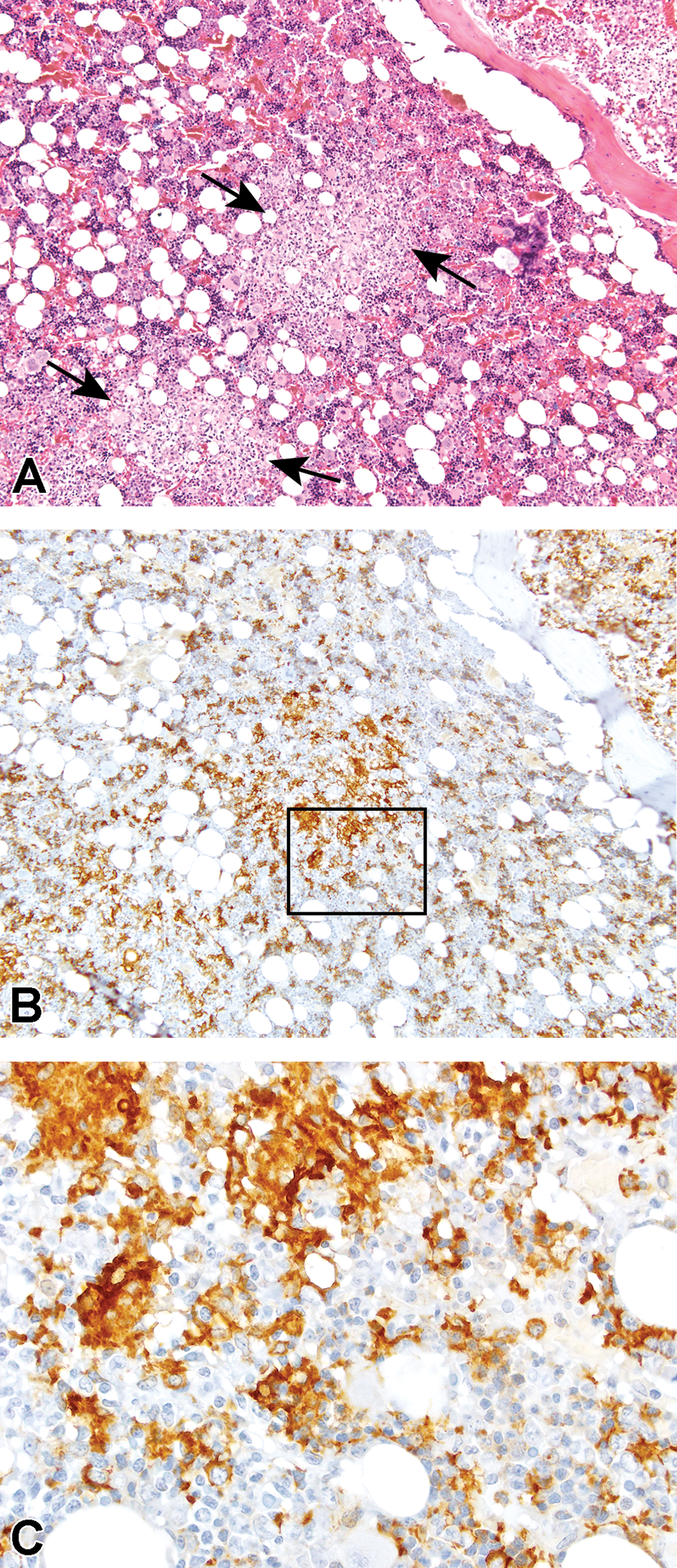
Hematoxylin and eosin (A) and Iba1 (B and C) staining of rat bone marrow lesion previously diagnosed as reticulum cell hyperplasia, mild. Microscopic reevaluation and positive Iba1 staining were consistent with cellularity increased, macrophage (arrows). Box in plate B represents the area of plate C. Plates A and B original objective ×10. Plate C original objective ×40. Iba1 indicates ionized calcium binding adapter molecule 1.
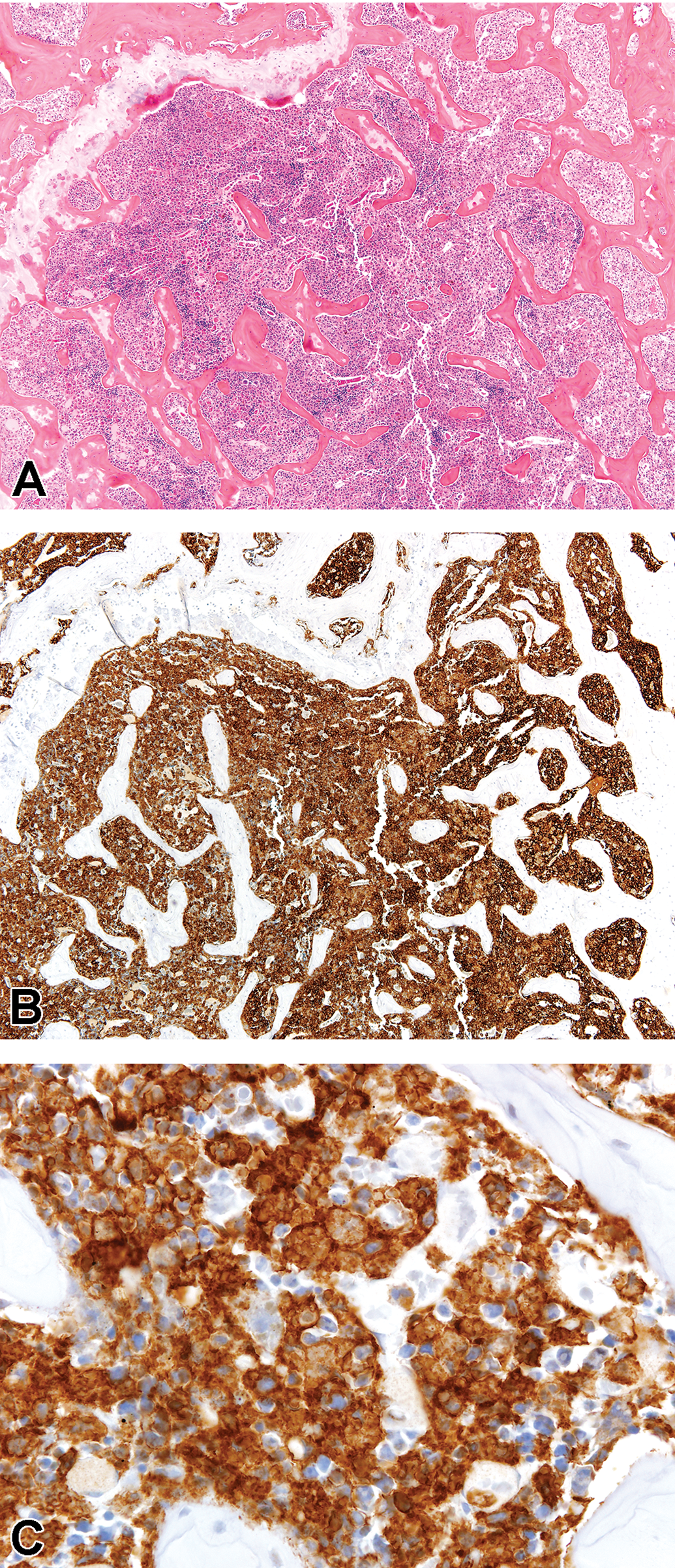
Hematoxylin and eosin (A) and Iba1 (B and C) staining of rat bone marrow lesion previously diagnosed as reticulum cell hyperplasia, moderate. Microscopic reevaluation and positive Iba1 staining were consistent with a histiocytic sarcoma. Plates A and B original objective ×10. Plate C original objective ×40. Iba1 indicates ionized calcium binding adapter molecule 1.
Discussion
Fifty-three out of 83 reevaluated archival slides previously diagnosed with RCH were consistent morphologically with cells of histiocytic origin. All the specimens chosen for IHC stained positive for Iba1. Whether the original diagnoses of RCH were meant to indicate an increase in so-called (nonhistiocytic) reticulum cells or, instead, histiocytic cells (eg, macrophages) is not known, as macrophages were referred to as reticulum cells by some investigators in years past. In some instances, the term RCH was used for lesions that were morphologically consistent with a HS. In these cases, RCH was modified with “marked” or “moderate” severity grade. Histiocytic sarcoma was not diagnosed in any other tissues of these animals, which may help explain the diagnoses of RCH instead of HS, as it used to be thought that HS could not have arisen solely from the bone marrow. 16 Overall, the diagnosis of RCH in NTP toxicity and carcinogenicity studies was relatively low and occurred in control animals with some frequency. Thus, the current finding of low numbers of HCs will not affect the outcomes of previous NTP studies.
Upon reevaluation, some of the marrows diagnosed with RCH were consistent with increased myeloid cells, or autolysis. At low magnification, focal areas of increased myeloid cells appear pale in appearance and could conceivably be interpreted as areas of histiocytic infiltration. Slides of low cellular quality due to autolysis were observed to have areas reminiscent of histiocytic infiltration, but due to the quality of the slide and the purposes of this study, it was decided not to interpret these particular specimens as anything but autolytic. A low number of marrows appeared normal with no apparent lesions identified.
Ionized calcium binding adapter molecule 1 is an actin cross-linking protein involved in microglia/macrophage membrane ruffling and phagocytosis. 17 Ionized calcium binding adapter molecule 1 has been shown to be expressed on rat microglial cells, monoblastic cells of rat hematopoietic cell lines, and macrophages in rat livers. 18 –21 It is regarded as a “pan-macrophage marker” in mice, because it has been shown that all subpopulations of macrophages express it with the exception of alveolar macrophages. 22 The results of our study reveal that, similar to mice, Iba1 is expressed on macrophages that reside in or migrate to the bone marrow. Additionally, the results of our study revealed that the Iba1 marker can be used on decalcified specimens. To rule out the possibility of lymphocytic lesions, CD3 and Pax5 IHC markers were also applied to the specimens. No positive staining was observed on the slides, including the resident lymphocytes, and is thought to be because of the decalcification process done during processing; the same was true of lysozyme stain, which was chosen to confirm macrophages. The lack of CD3, Pax5, and lysozyme staining was not unexpected, but nonetheless attempted for completeness. Despite this, the positive Iba1 expression confirmed a histiocytic origin, and Iba1 is not known to stain cells of lymphocytic origin. The results of our study support that the cells of lesions previously diagnosed as RCH are morphologically and immunohistochemically consistent with cells of histiocytic origin. These results will help with interpretation of historical data and demonstrates that Iba1 can be used in decalcified bone marrow sections for the identification of cells of histiocytic origin.
Supplemental Material
Supplemental Material, Supp_Table_2 - Previously Diagnosed Reticulum Cell Hyperplasia in Decalcified Rat Bone Marrow Stain Positive for Ionized Calcium Binding Adapter Molecule 1 (Iba1): A Monocytic/Macrophage Cell Marker
Supplemental Material, Supp_Table_2 for Previously Diagnosed Reticulum Cell Hyperplasia in Decalcified Rat Bone Marrow Stain Positive for Ionized Calcium Binding Adapter Molecule 1 (Iba1): A Monocytic/Macrophage Cell Marker by Michelle C. Cora, Kyathanahalli S. Janardhan, Heather Jensen, Natasha Clayton and Gregory S. Travlos in Toxicologic Pathology
Footnotes
Acknowledgments
This research was supported by the NIH, National Institute of Environmental Health Sciences. The authors thank Drs. Cynthia Willson and Mark Cesta for their careful review of the manuscript and Beth Mahler for her assistance with the photomicrographs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.