
Abstract
Chronic hyperplastic candidiasis progresses from squamous cell hyperplasia to squamous cell carcinoma (SCC); however, the oncogenic mechanism remains unclear. In the present study, we attempted to induce opportunistic Candida albicans infection and establish chronic hyperplastic candidiasis in rats by combining diabetic condition and prednisolone administration, followed by analysis of the inflammatory cells involved in the disease progression. Female Wistar Bunn/Kobori (WBN/Kob) rats were divided into 3 groups: alloxan-induced diabetic rats (A group) along with diabetic (AP group) and nondiabetic (P group) rats intermittently treated with prednisolone. Animals were euthanized at 42 weeks of age. Squamous cell hyperplasia following C. albicans infection in the forestomach was observed in almost all AP and A group rats. The lesions in the AP group were significantly more severe than those in the A group. In addition, SCC was detected in 1 AP group animal. Cluster of differentiation (CD)4-positive T cell and CD68-positive macrophage infiltration in the AP group was significantly stronger than that in the A group. These findings suggest that the combination of diabetes and intermittent prednisolone administration could induce chronic hyperplastic candidiasis without direct C. albicans inoculation and that CD4-positive T cells and CD68-positive macrophages may be highly involved in the pathogenesis of these hyperplastic lesions.
Keywords
Candida albicans constitutes a resident fungus in the human gastrointestinal tract and is known to induce oral, esophageal, and vaginal candidiasis in immune-compromised patients (Mayer, Wilson, and Hube 2013; Kabir, Hussain, and Ahmad 2012). The mucosal epithelia in chronic hyperplastic candidiasis are thickened and sometimes progress to carcinoma in patients (McCullough et al. 2002; Barrett, Kingsmill, and Speight 1998; Sitheeque and Samaranayake 2003; Williams et al. 2001; Bakri et al. 2010; Gainza-Cirauqui et al. 2013; Gall et al. 2013; Norgaard et al. 2013). However, little is currently known regarding the oncogenic mechanism leading to carcinoma from chronic inflammation. Previously, we reported that alloxan-induced diabetic rats frequently develop severe mucosal proliferative lesions upon C. albicans and bacterial infection in the forestomach and that the lesions progressed to squamous cell carcinoma (SCC) in some cases (Sano et al. 2009a; Kodama et al. 2006). Antidiabetic, antifungal, and probiotics treatments reduce the degree of these changes (Sano et al. 2009a, 2009b; Terayama et al. 2016), whereas antibiotic (tetracycline) treatment increases the incidence of proliferative lesions upon C. albicans infection (Sano et al. 2012). Additionally, we succeeded in inducing early onset proliferative and inflammatory lesions by gavage administration of C. albicans in diabetic rats (Sano et al. 2014). Therefore, these results suggest that diabetes and C. albicans infection may represent important factors for the induction of squamous cell hyperplastic lesions with chronic inflammation.
The induction of oral and systemic candidiasis in rodents by administration of immunosuppressive and antimicrobial agents is straightforward (Samaranayake and Samaranayake 2001; Costa et al. 2013; Naglik, Fidel, and Odds 2008). However, the reproduction of a chronic hyperplastic candidiasis model, using immunosuppressive agents, is difficult (Samaranayake and Samaranayake 2001) because of the delicate adjustment of dosage selection and administration frequency required for immunosuppressive agents. Animals recover from candidiasis when the effect of immunosuppressive agents is mild but suffer from systemic and invasive candidiasis leading to death when the agent effect is severe. Thus, in our previous study (Sano et al. 2014), we elucidated a method of appropriate adjustment for the dosage and frequency of immunosuppressive drugs.
Chronic inflammation is deeply involved in tumor development; and inflammatory cells, including lymphocytes and macrophages, play an important role in the development of various tumors through the production and response of cytokines, chemokines, and growth factors (Grivennikov, Greten, and Karin 2010; Coussens and Werb 2002). In particular, a rodent model for C. albicans–induced mucosal inflammation and proliferation developed in our previous study is accompanied by squamous cell proliferation and severe inflammatory response (Kodama et al. 2006; Sano et al. 2014); therefore, identification of these inflammatory cells may be necessary to clarify the relationship between C. albicans infection–derived chronic inflammation and the development of SCC.
In the current study, we attempted to establish a model for chronic hyperplastic candidiasis caused by opportunistic rather than induced C. albicans infection through the combination of diabetic condition and prednisolone administration. We also aimed to utilize this model to identify inflammatory cells involved in the progression of mucosal epithelial hyperplasia.
Materials and Methods
Animals and Diet
Female WBN/Kob rats (Rattus norvegicus) were obtained from Japan SLC, Inc. (Shizuoka, Japan). They were reared (5 animals per cage) in a barrier-sustained animal room maintained at a temperature of 24 ± 2°C with a relative humidity of 60 ± 20% and a 12-hr light/dark cycle and ventilated at least 12 times/hr with sterilized fresh air. All rats were housed and reared in stainless mesh cages. To protect against infection, the cages were changed once or more each week. Rats were given a pelleted diet (CRF-1; Oriental Yeast, Tokyo, Japan) and chlorinated water ad libitum. The study was approved by the Committee for Animal Experiments of Setsunan University.
Preliminary Studies: Dosage and Frequency of Prednisolone in Alloxan-induced Diabetic Rats
Preliminary study 1
A total of 16 female WBN/Kob rats aged 10 weeks were administered a single dose of alloxan (Sigma-Aldrich Japan, Tokyo, Japan) via the tail vein, at a dosage of 45 mg/kg body weight (Terayama et al. 2016). The alloxan dosage was determined as that which allowed an extensive period of survival after the development of signs of continuous hyperglycemia and glycosuria. Furthermore, 2 weeks after administration of alloxan, groups of 4 diabetic rats were each treated with single subcutaneous injections of prednisolone (Kyoritsu Seiyaku Corporation, Tokyo, Japan) at a dose of 100, 50, 25, or 10 mg/kg body weight, respectively. Animals were observed for 2 weeks after prednisolone treatment. Within 2 weeks after prednisolone treatment, all rats (100%) in the 100- and 50-mg/kg dosage groups, 2 rats (50%) in the 25-mg/kg dosage group, and 3 rats (75%) in the 10-mg/kg dosage group died of severe gastrointestinal bleeding and acute nephrotoxicity.
Preliminary study 2
Acute alloxan renal toxicity reportedly continues 1 week after treatment (Terayama et al. 2017). Thus, the interval of dosing alloxan and prednisolone was extended from 2 to 4 weeks, so that diabetic rats treated with alloxan might completely recover from the effect of renal toxicity (Terayama et al. 2017). The prednisolone dosage used was 10 mg/kg, the minimum lethal dosage determined in preliminary study 1. We treated 4 female WBN/Kob rats with alloxan as in the preliminary study 1. After 4 weeks, they were further subcutaneously injected with 10 mg/kg prednisolone. The combined treatment of the 2 agents showed no lethal activity, and all 4 rats (100%) survived 2 weeks after prednisolone treatment.
Main Study: Experimental Design
The experimental design for intermittent prednisolone administration in alloxan-induced diabetic rats is shown in Figure 1. A total of 44 female WBN/Kob rats were divided into 3 groups: 15 alloxan-induced diabetic rats (A group), 18 alloxan-induced diabetic rats intermittently treated with prednisolone (AP group), and 11 nondiabetic rats intermittently treated with prednisolone (P group).
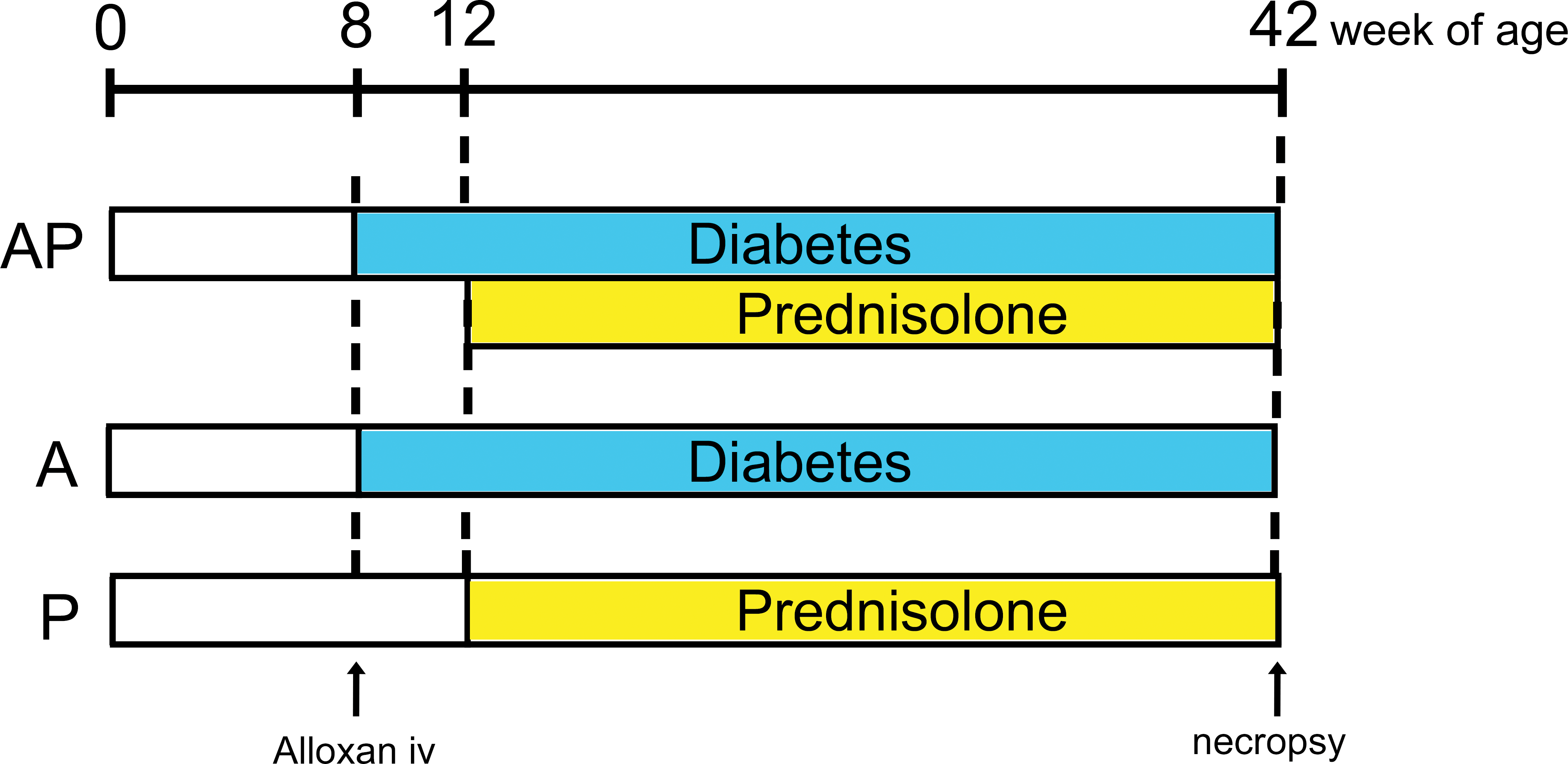
Experimental design. Schematic representation of the experimental design to analyze the effects of the combination of diabetes and intermittent prednisolone administration.
A single dose of alloxan was administered to 33 rats (AP and A groups) aged 8 weeks via the tail vein at a dosage of 45 mg/kg body weight (Sano et al. 2014). After 4 weeks, 18 diabetic rats (AP group) as well as the previously untreated 11 rats (P group; aged 12 weeks) received subcutaneous injections of prednisolone at a dose of 10 mg/kg body weight once every 2 weeks. Timings of alloxan administration (8 weeks of age) and prednisolone dosage (10 mg/kg body weight) were determined from the results of the preliminary studies.
At the end of the experiment (42 weeks of age), all rats were anaesthetized through intraperitoneal injection of ketamine hydrochloride (40 mg/kg body weight; Ketalar, Sankyo, Tokyo) and xylazine hydrochloride (10 mg/kg body weight; Seractal, Bayer Japan, Tokyo) for histopathological examination.
Glucosuria and Glycemia Monitoring
Fresh urine samples were collected from each animal. Urinary glucose levels were semiquantitatively measured using a urine test paper (Wako Pure Chemical Industries, Osaka, Japan) every day from day 1 to day 3 after alloxan dosing, once every week for 1 month after the first week, and once every month thereafter from the fresh urine obtained from all rats. Blood glucose levels were also semiquantitatively measured by the glucose oxidase method (Glutest E; Sanwa Kagaku, Aichi, Japan) once every month from the fourth week after dosing, using blood samples from the tail vein. Samples of fresh urine and blood from the tail vein were collected between 1:00 and 4:00 p.m. Diabetic condition was diagnosed as positive from the urine test and upon results of over 300 mg/dl from the blood glucose test.
Histopathological Analysis
Moribund and dead animals (a total of 6 rats) of the AP groups were euthanized and necropsied during the examination period; some of their organs were unavailable for histopathological examination because of cannibalism or autolysis. The remaining 38 rats were euthanized by exsanguination from the abdominal aorta under deep anesthesia at the end of each scheduled period. The entire alimentary tract was immediately removed following necropsy. The organs of the 38 rats were immersed in 10% phosphate-buffered formalin solution immediately after necropsy. Formalin-fixed organs were trimmed, dehydrated by automated processor, and embedded in paraffin wax. Sections (4-µm thick) of tissue specimens were stained with hematoxylin–eosin and periodic acid-Schiff reaction for histopathological examination. Unfixed samples of the forestomach were embedded in optimum cutting temperature (OCT) compound (Sakura Finetek Japan, Tokyo, Japan) and were quickly frozen in hexane cooled with liquid nitrogen. Frozen sections (5-µm thick) were cut using an OTF5000 cryostat (Bright Instruments Ltd., Luton, UK) at a cabinet temperature of −23°C and immunohistochemically stained.
All lesions were evaluated and scored by 2 investigators (K.O. and Y.T.), using our previous analytical criterion for the forestomach, tongue, cheek, gingiva of the molar palate, and esophagus (Kodama et al. 2006; Sano et al. 2014; Terayama et al. 2016). The severity of proliferative lesions in the forestomach squamous epithelia was evaluated by the 4-grade grading system used in previous reports, that is, grade 0, slight change; grade 1, mild change; grade 2, moderate change; and grade 3, severe change. Suppurative inflammation indicated neutrophil infiltration in the mucosal surface. Chronic inflammation indicated lymphocyte and plasma cell infiltration in the submucosa and lamina propria. The severity of suppurative inflammation and chronic inflammation was graded into 4 levels of inflammatory cell infiltration of the mucosal surface, submucosa, and lamina propria, respectively: grade 0, scarce (0%); grade 1, focal change (<10%); grade 2, multifocal changes (10–30%); and grade 3, diffuse change (30–60%). The severity of C. albicans infection was graded into 3 grades according to C. albicans infiltration area of the mucosal surface: grade 0, scarce (0%); grade 1, focal change (<10%); and grade 2, multifocal changes (10–30%). Severity of proliferative lesions, inflammatory changes, and C. albicans infections in the tongue, cheek, gingiva of the molar palate, and esophagus was graded into 2 grades: grade 0, no change compared to control animals; and grade 1, slight to mild changes.
Immunohistochemical Analysis
Immunohistochemical analysis was performed for identification of the protein of proliferative index (Ki-67) and inflammatory cells (CD68, CD3, CD45, and myeloperoxidase), using representative forestomach sections. The sections were deparaffinized in xylene and rehydrated through graded ethanol at room temperature. Rehydrated sections were treated following the protocol shown in Table 1 to retrieve the antigens. Solutions and washes were prepared between the various steps, using 0.05M tris-buffered saline (pH 7.6) with 0.01% Tween 20 (TBST). Nonspecific endogenous peroxidase activity was blocked by exposure to 0.03% hydrogen peroxidase in 100% methanol for 5 min, and masking was conducted with 5% goat serum albumin in phosphate-buffered saline for 5 min at room temperature. Incubation was carried out overnight at 4% using the respective primary antibody (Table 1; Furukawa, Nagaike, and Ozaki 2017). The slides were subsequently rinsed with TBST, treated for 60 min at room temperature with the secondary antibody (Table 1), and incubated in a diaminobenzidine solution. As a negative control, mouse or rabbit isotype immunoglobulin, diluted to the same concentration, was substituted for the primary antibody. The Ki-67 positive index was estimated as a percentage of Ki-67-labeled nuclei/1,000 squamous cells near the limiting ridge in the stomach. The evaluation of inflammatory cell infiltration in the horny layer, squamous epithelia, lamina propria, muscularis mucosae, and submucosa was as follows. The severity of the CD68-positive macrophage and CD3-positive T cell infiltration was evaluated by a grading system divided into 5 grades, as grade 0, negative (0%); grade 1, weak expression (<10%); grade 2, moderate expression (10–30%); grade 3, strong expression; grade 4, significantly strong expression (30–60%). The severity of CD45-positive B cell and myeloperoxidase-positive neutrophil infiltration was evaluated by a grading system divided into 3 grades, as grade 0, negative (0%); grade 1, weak expression (<10%); and grade 2, moderate expression (10–30%).
Antibodies Used in This Study.

Immunofluorescence Double Staining of CD4+/CD3+ and CD8+/CD3+
Immunofluorescence double staining was performed to assess the number of CD4+/CD3+ and CD8+/CD3+ T cells. The frozen sections were fixed in acetone for 10 min and washed with TBST. Nonspecific endogenous peroxidase activity was blocked by exposure to 0.03% hydrogen peroxidase in 100% methanol for 5 min, and masking was conducted with 5% goat serum albumin in phosphate-buffered saline for 5 min at room temperature. Incubation was carried out overnight at 4% using an anti-CD3 antibody (diluted 1:800, Dako, Glostrup, Denmark) and an anti-CD4 antibody (diluted 1:100, Serotec, Kidlington, UK) or an anti-CD3 antibody (diluted 1:800, Dako) and an anti-CD8 antibody (diluted 1:200, Serotec). The slides were subsequently rinsed with TBST, treated for 60 min at room temperature with Alexa Fluor 488- or 594-conjugated secondary antibodies (Invitrogen, Carlsbad, CA), and rinsed with TBST. Then, nuclei were counterstained with 4′,6-diamidino-2-phenylindole (DAPI; Invitrogen). As a negative control, mouse or rabbit isotype immunoglobulin, diluted to the same concentration, was substituted for the primary antibody. The number of double-positive cells per 100 mm2 was calculated.
Statistical Analysis
The results obtained were expressed as the means ± standard deviation. An unpaired Student’s t-test was performed for statistical analysis of the Ki-67 positive index and the cell number for CD4+/CD3+ and CD8+/CD3+ cells, and the Mann–Whitney U test was performed to compare histopathological findings. When the calculated p value was less than .05, the difference was considered statistically significant. Statistical analysis was performed using the StatMate III program (ATMS, Tokyo, Japan).
Results
General Conditions and Monitoring of Glucosuria and Glycemia
Of the AP group, 6 rats died or were euthanized between 12 and 36 weeks of age. The cause of death was attributed to severe gastrointestinal bleeding in 3 cases, urinary tract infection in 1 case, and sepsis in 1 case but was unknown in 1 case.
Body weight gradually increased in the A and P groups, whereas that of the AP group gradually decreased (Figure 2a). In the AP and P groups, body weight decreased in the week after prednisolone treatment but increased again in the second subsequent week. These changes in the AP and P groups repeated until the time of scheduled necropsy. The mean body weight in the AP group was significantly lower than that in the A and P groups (p < .001), but no significant differences were observed between the A and P groups.
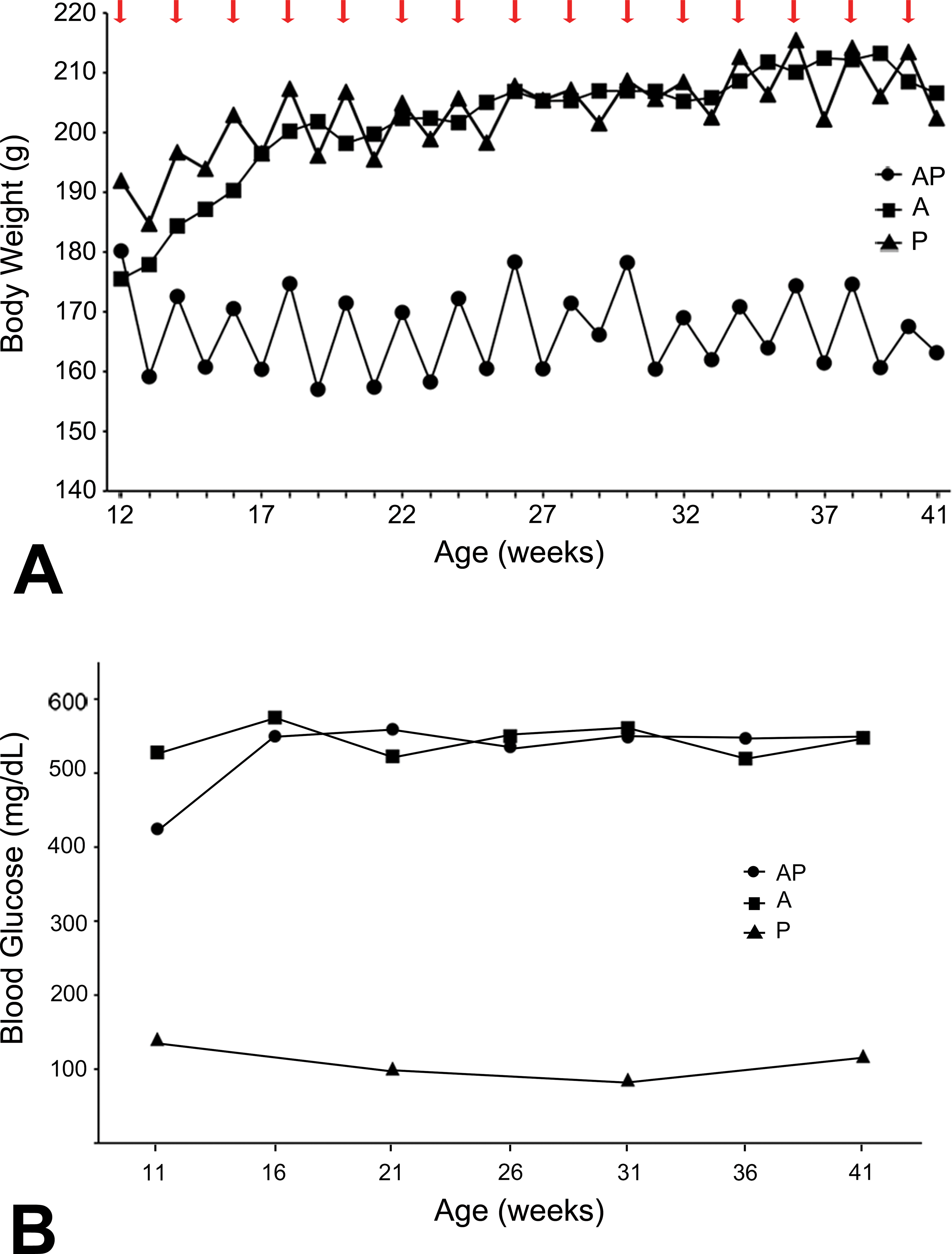
Monitoring of body weight and glycemia. Changes of average body weight (a) and blood glucose (b) in AP, A, and P groups. Red arrows show the week of prednisolone treatment.
Severe hyperglycemia (>300 mg/dl) and glucosuria (>500 mg/dl) continued for 34 weeks from the day of alloxan treatment to the time of scheduled necropsy in all rats of the AP and A groups (Figure 2b). In contrast, all rats in the P group exhibited normal blood and urine glucose levels during the experimental period.
C. Albicans–induced Mucosal Proliferation Is Enhanced by Prednisolone Administration
Squamous cell hyperplasia in the forestomach was characterized by a multilayered epithelium and thickening mucosa with hyperkeratosis, and the lesion was observed in almost all rats of the AP and A groups (Figures 3a, b and 4). The incidence and severity of these proliferative lesions in the AP group were the highest among all groups and were significantly enhanced compared to those in the A and P groups (p < .001). Moderate (grade 2) to severe (grade 3) proliferative changes were detected in 10 of 12 cases (83.3%) in the AP group (Figure 4), and the lesion progressed to SCC in 1 case (Figure 3d). In contrast, only moderate (grade 2) proliferative changes were observed in 5 of the 15 cases (33%) in the A group, and no proliferative change was detected in the P group (Figures 3c and 4). Although the Ki-67 positive index as a proliferation marker was slightly enhanced in the AP compared to that in the A group, this difference did not reach significance (Figures 5 and 6).
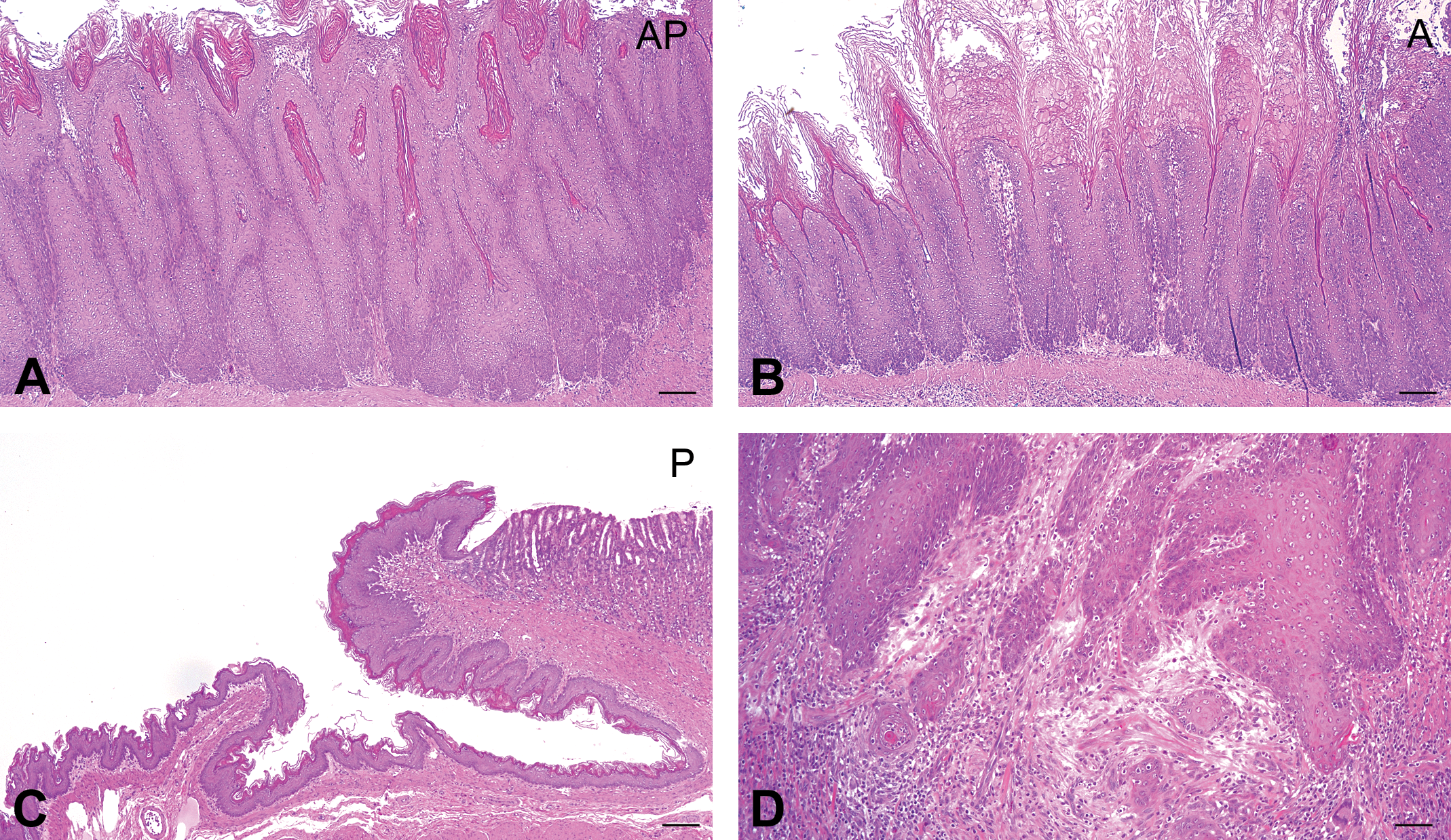
Candida albicans -induced mucosal proliferation is enhanced by the administration of prednisolone. (a) Severe hyperplasia of forestomach mucosal squamous epithelium in the AP group. (b) Mild hyperplasia of mucosal squamous epithelium in the A group. (c) Normal forestomach mucosa in the P group. Hematoxylin–eosin stain. Scale bar: 100 μm (d) Squamous cell carcinoma in the AP group. Hematoxylin–eosin stain. Scale bar: 100 μm.
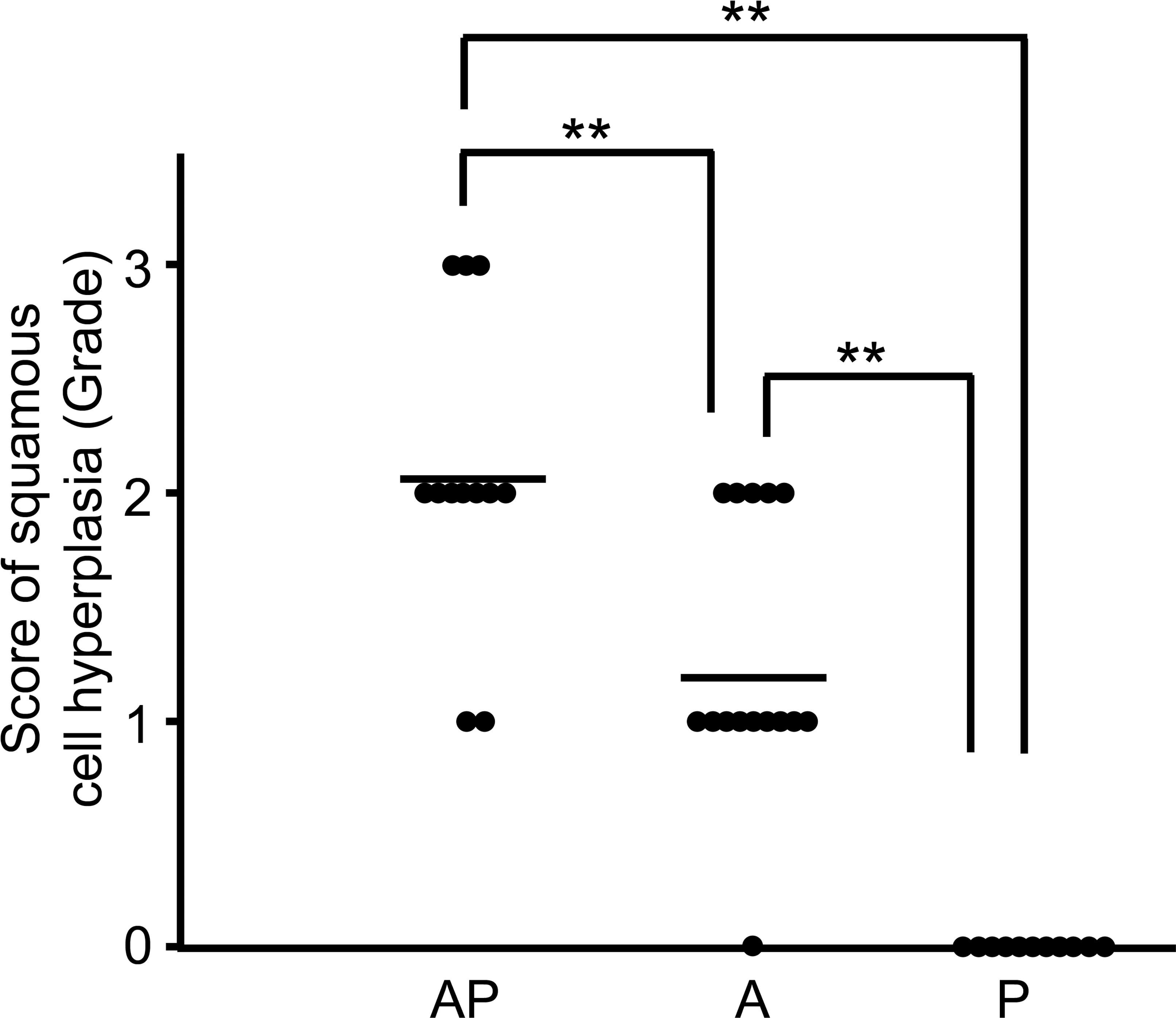
Scores of squamous cell hyperplasia in the AP, A, and P groups. The bar indicates the mean value (**p < .01).
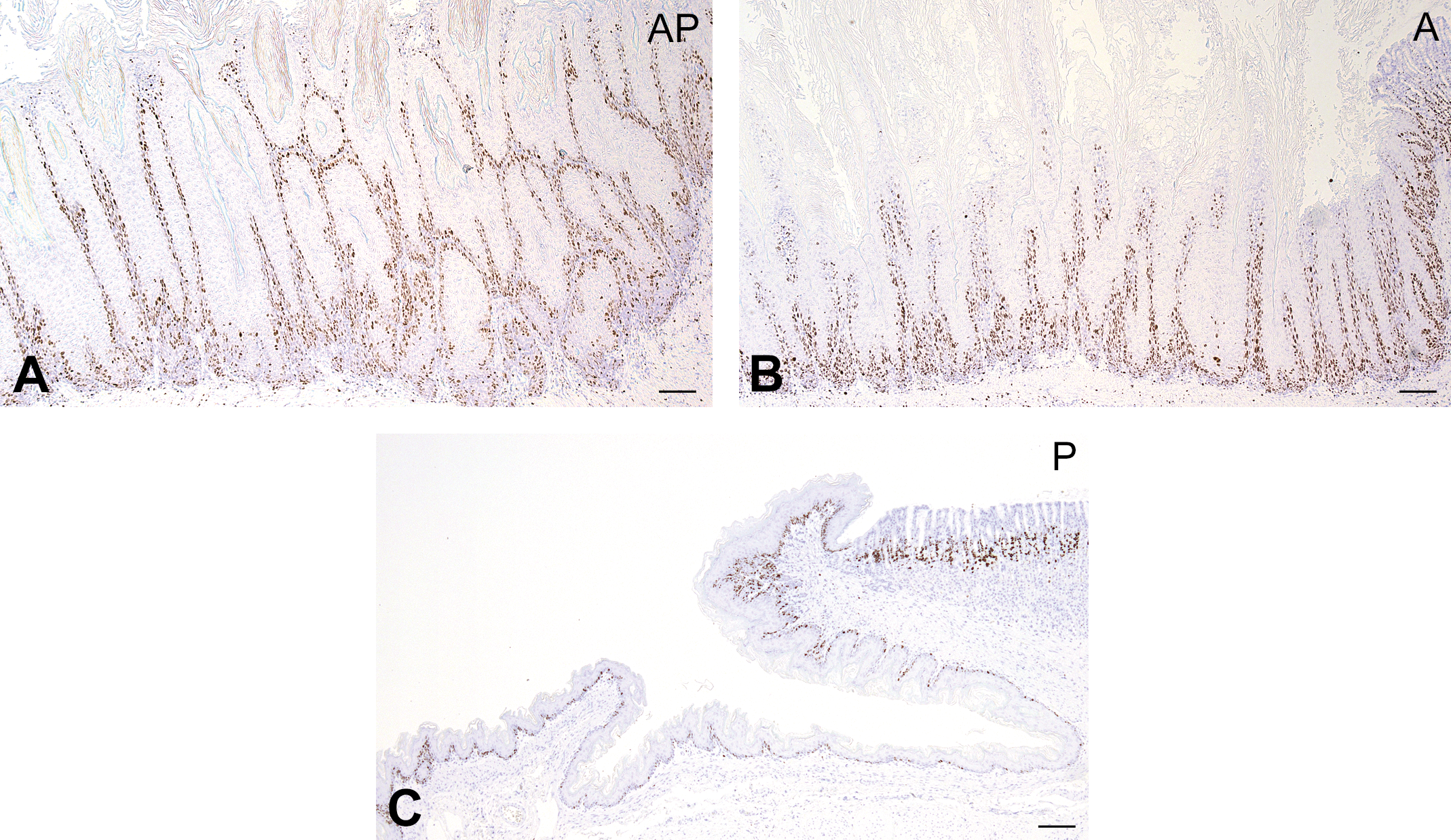
Ki-67-positive mucosal epithelium induced by Candida albicans. (a–c) Ki-67-positive cells in the forestomach. Immunohistochemical staining. Scale bar: 100 μm.
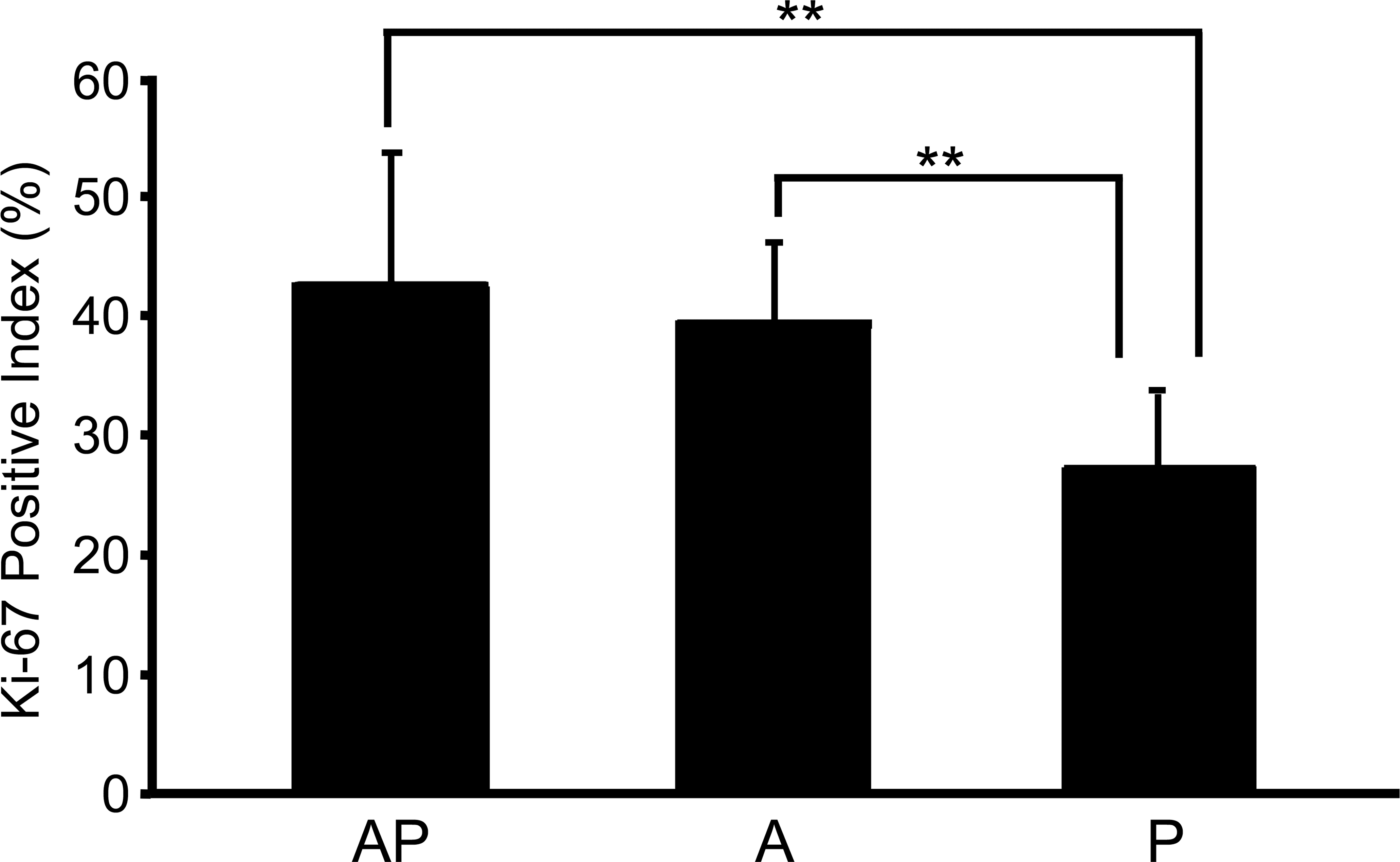
Comparison of the Ki-67 positive index for mucosal squamous epithelium in the AP, A, and P groups (**p < .01).
C. Albicans Infection and Suppurative Inflammation of the Mucosal Surface
Neutrophil and macrophage infiltration (suppurative inflammation) in the mucosal surface with squamous cell hyperplasia was slightly enhanced in the AP group compared to that in the A group (p = .016; Figures 7 and 8). These infiltrating cells in the mucosal surface were identified as myeloperoxidase-positive neutrophils and CD68-positive macrophages. C. albicans showed dimorphism such as yeast and hyphal forms and were usually observed along with bacterial colonies in the keratinous layer of the mucosal surface in almost all rats of the AP and A groups (Figures 9 and 10). Hyphal form C. albicans were seen to have invaded into the epithelia from keratin with increasing severity of squamous cell hyperplasia; the severity in the AP group was higher than that in the other 2 groups.
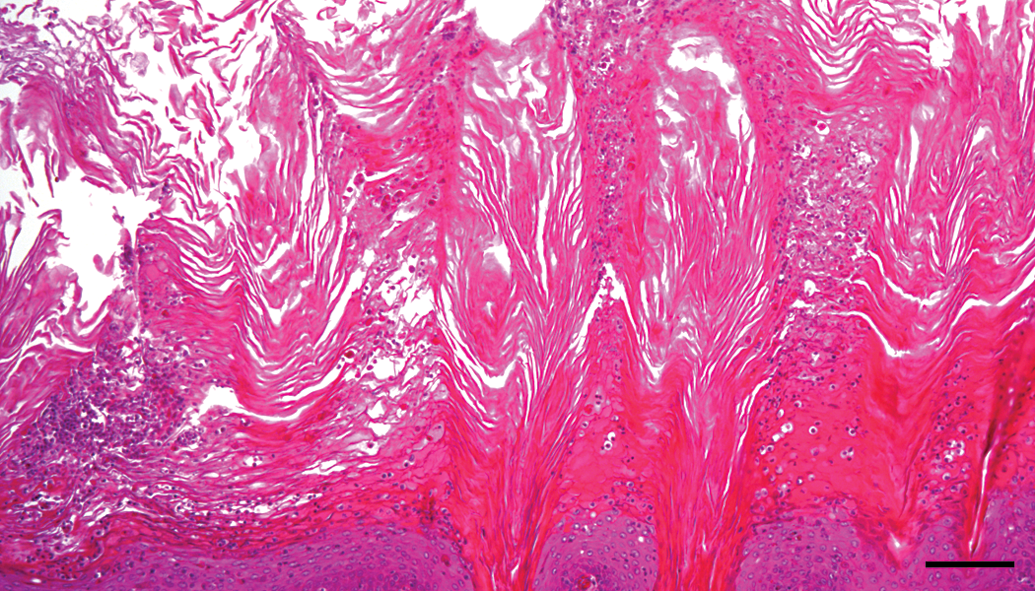
Suppurative inflammation in the mucosal surface. Neutrophil and macrophage infiltration in the hyperplastic mucosal surface of the AP group. Hematoxylin–eosin stain. Scale bar: 50 μm.
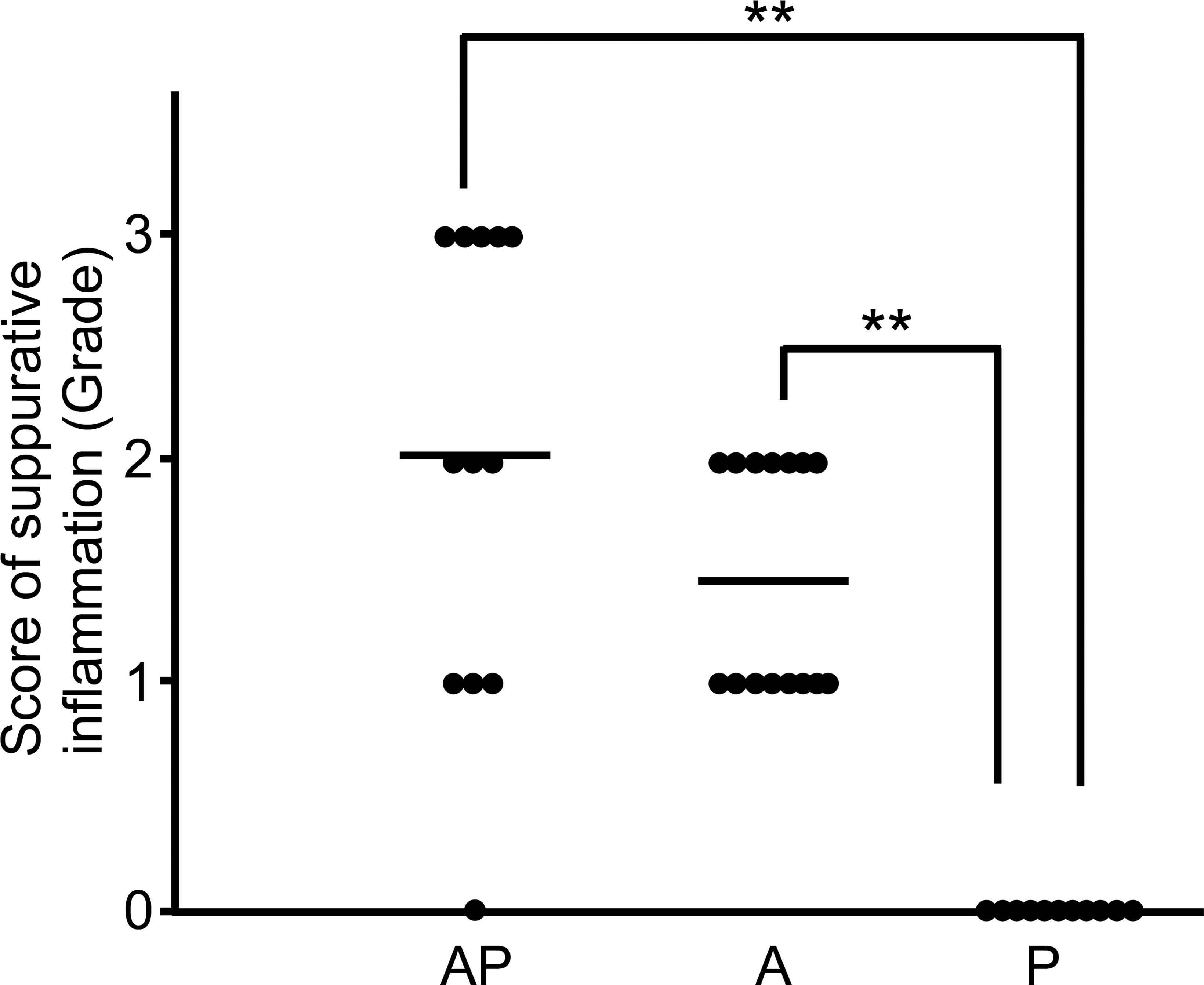
Comparison of scores for suppurative inflammation in the AP, A, and P groups. The bar indicates the mean value (**p < .01)
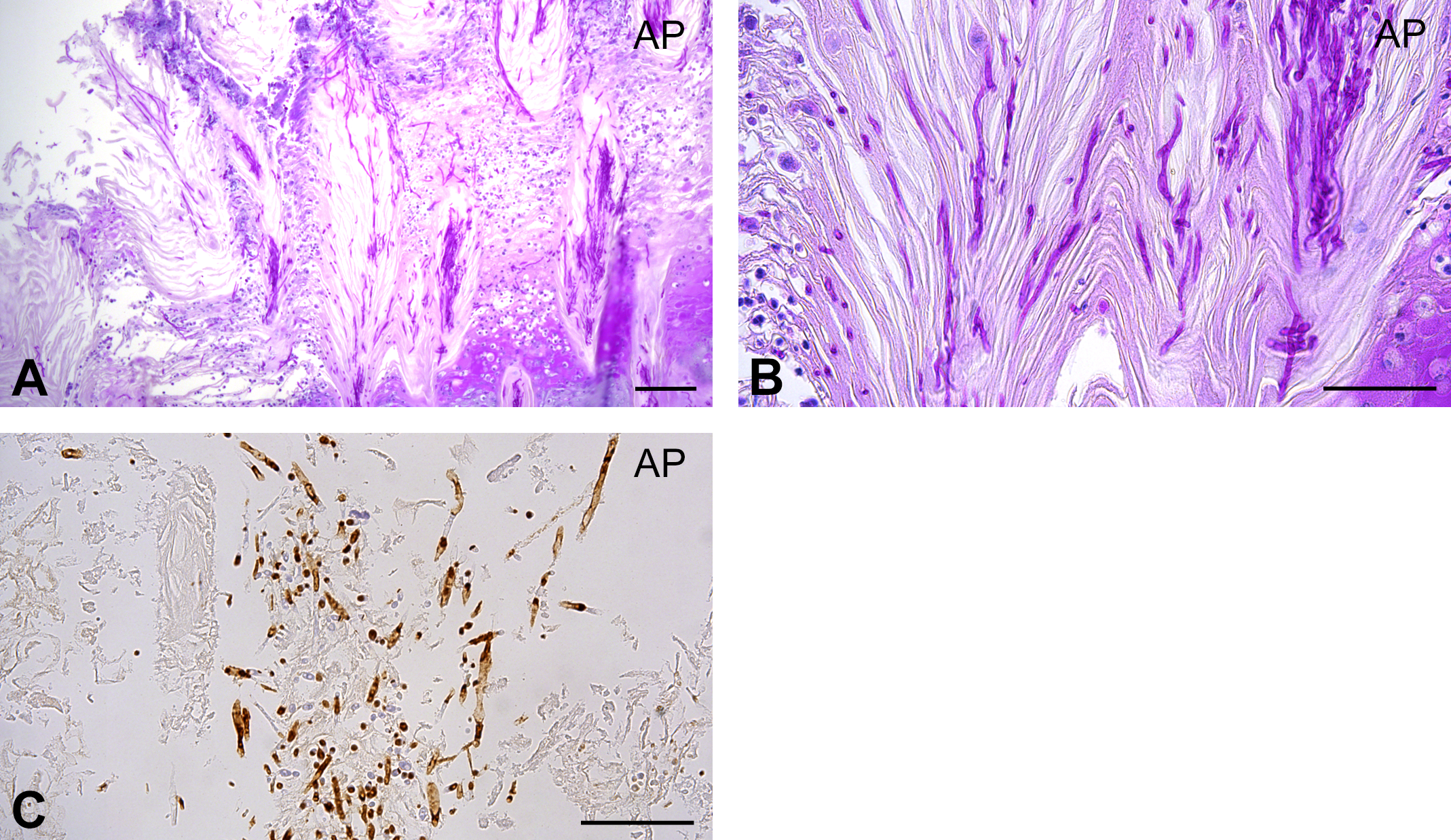
Candida albicans infection in the mucosal surface. (a and b) C. albicans infection in the AP group. Periodic acid-Schiff reaction. Scale bar: 50 μm. (c) Fungi positive for the C. albicans antigen in the AP group. Scale bar: 50 μm.
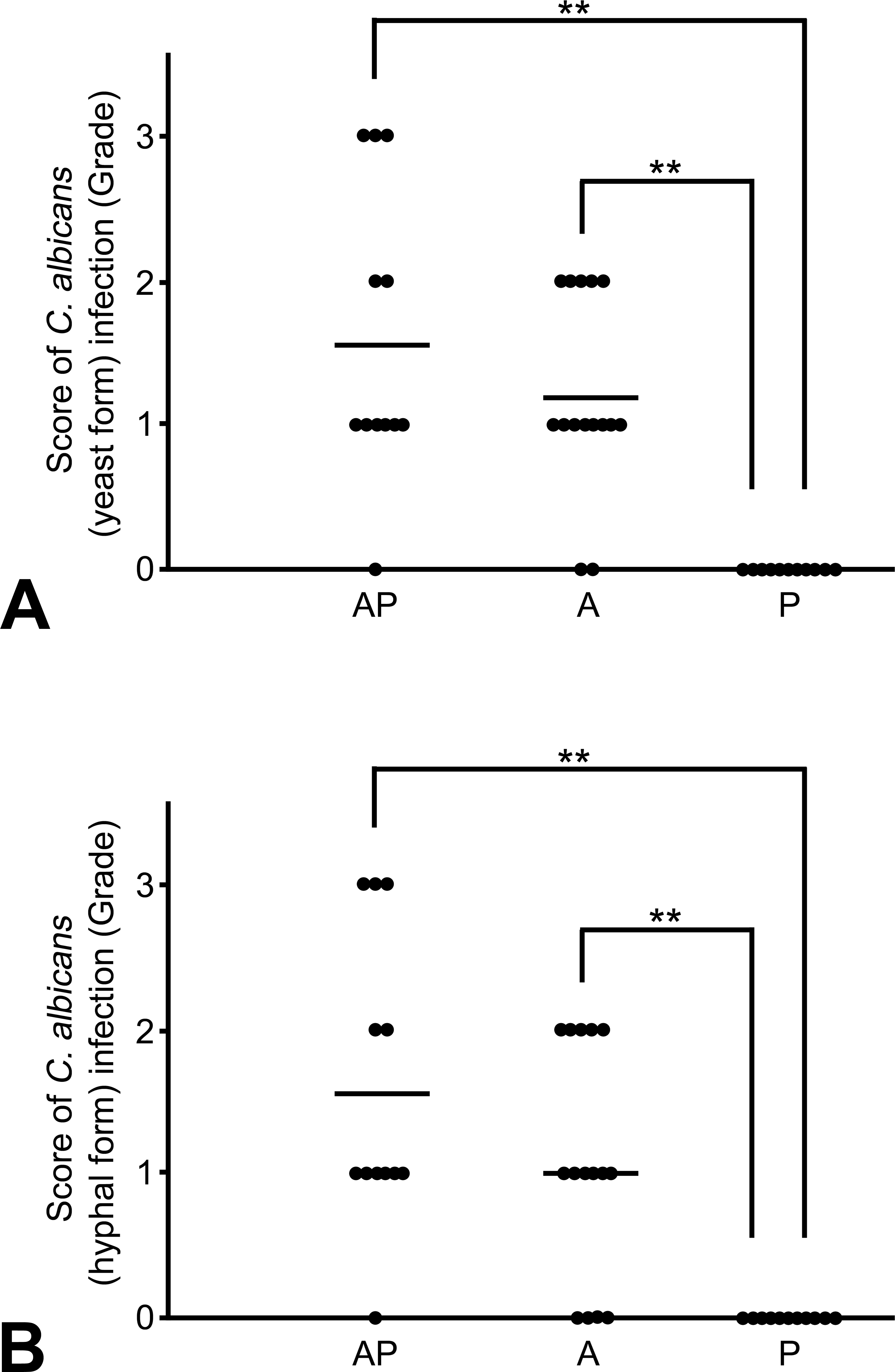
Score of Candida albicans yeast form (a) and hyphal form (b) infection in the mucosal surface. The bar indicates the mean value (**p < .01).
Exacerbated Chronic Inflammation with C. albicans Infection Is Correlated with an Increase in the Number of T Cells and Macrophages
The submucosa and lamina propria under squamous hyperplasia exhibited many infiltrated lymphocytes and plasma cells in almost all rats of the AP and A groups. Lesion severity was highest in the AP group among all groups (p < .01), whereas chronic inflammation was not observed in the P group (Figures 11 and 12). CD3-positive T cells were observed in the squamous epithelia, lamina propria, muscularis mucosae, and submucosa; and their number was significantly increased in the AP group compared to that in the A group (p < .01; Figures 13 and 14). CD4+/CD3+ and CD8+/CD3+ T cells were detected in the squamous epithelia, lamina propria, and submucosa; and their numbers were increased in the AP group compared to that in the A group (p < .05 and p < .01, respectively; Figures 15 and 16). Furthermore, in the AP group, the number of CD4+/CD3+ T cells exceeded that of CD8+/CD3+ T cells and showed marked increase in the submucosa. In addition, CD68-positive macrophages were detected in the squamous epithelia, lamina propria, muscularis mucosae, and submucosa, and their number was significantly increased in the AP group compared to that in the A group (p < .05; Figures 17 and 18). In particular, CD68-positive macrophages were more abundant in the muscularis mucosae and submucosa of the AP group. CD45-positive B cells were observed in the lamina propria, muscularis mucosae, and submucosa; and their number was slightly increased in the AP group compared to that in the A group, although this difference was not significant.
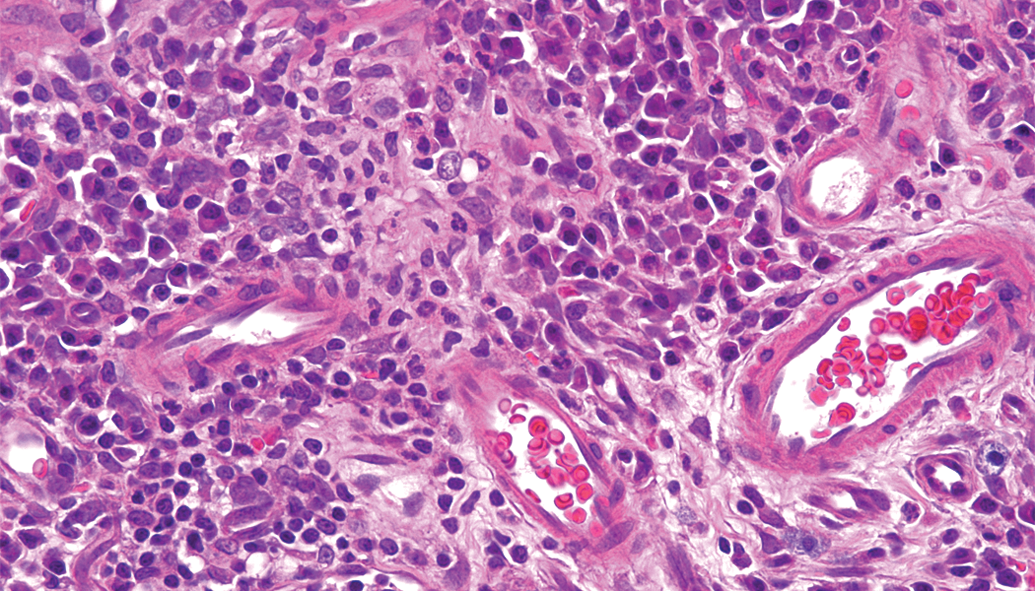
Chronic inflammation in the submucosa. Lymphocyte and plasma cell infiltration in the submucosa and lamina propria under squamous hyperplasia of the AP group. Hematoxylin–eosin stain. Scale bar: 50 μm.
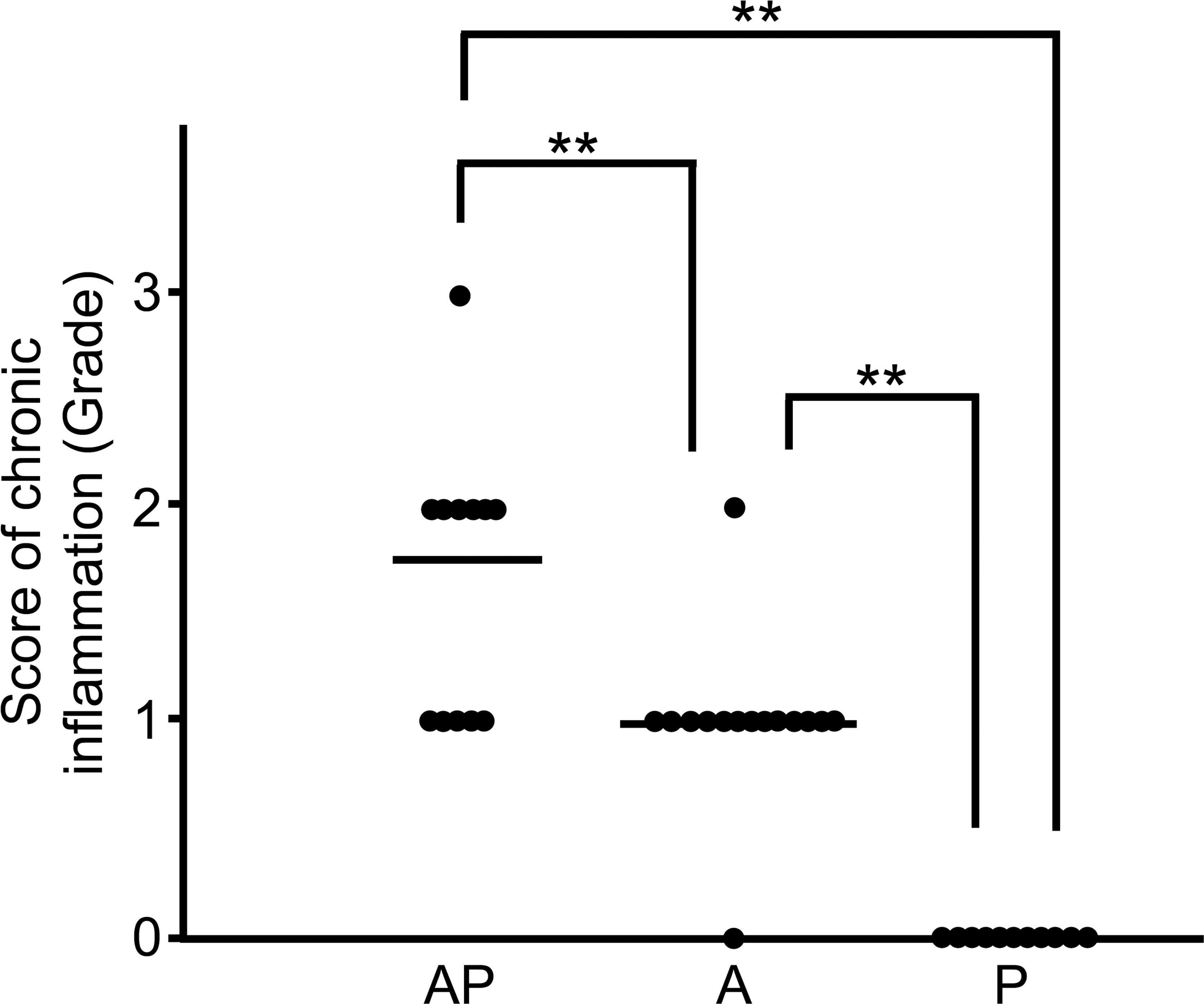
Score of chronic inflammation in the AP, A, and P groups. The bar indicates the mean value (**p < .01).
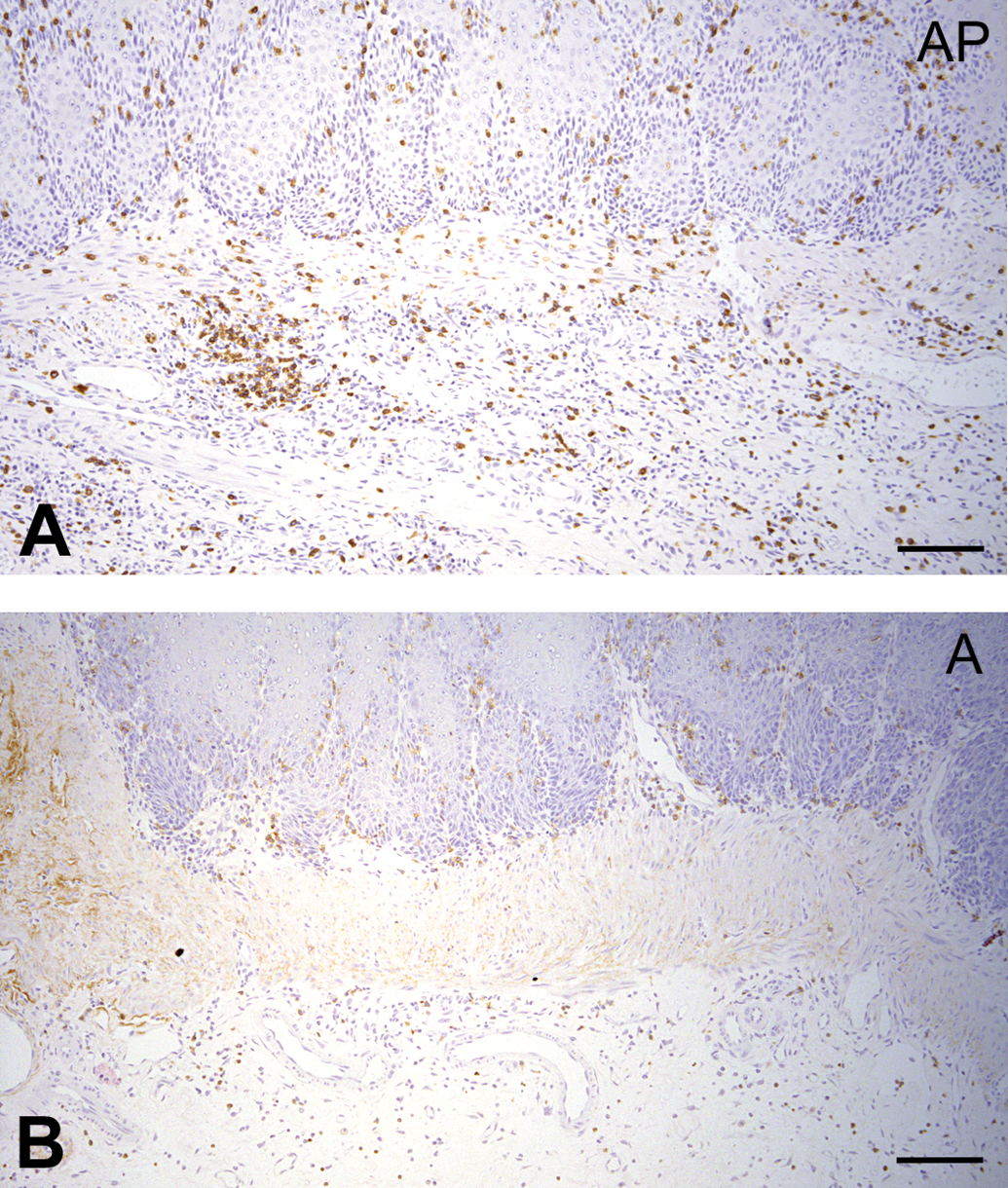
CD3-positive T cells are increased in the AP group. (a) Strong expression of CD3 in the AP group. (b) Weak expression of CD3 in the A group. Immunohistochemical analysis. Scale bar: 50 μm.
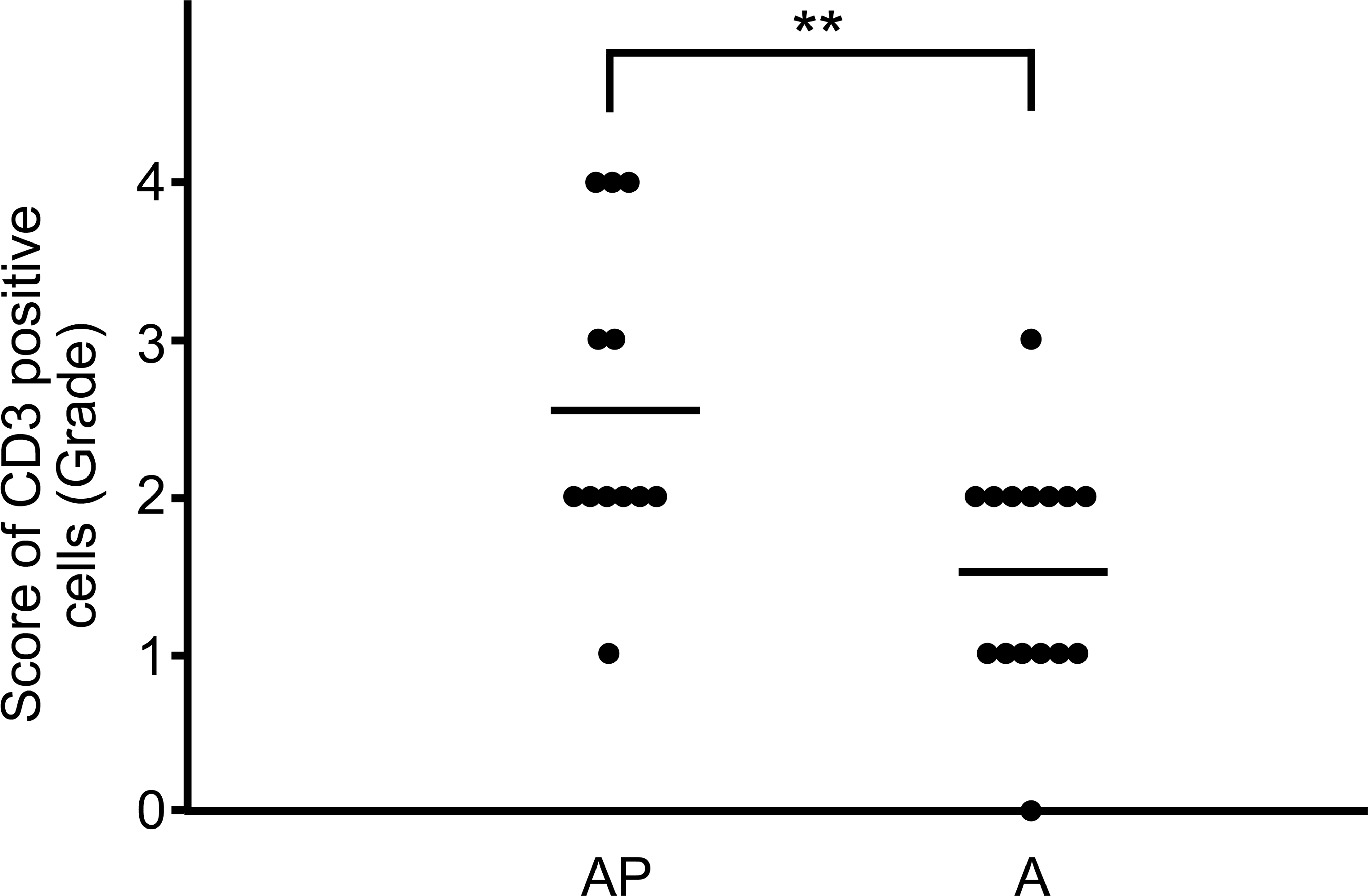
Score of CD3-positive T cells in the AP and A groups. The bar indicates the mean value (**p < .01).
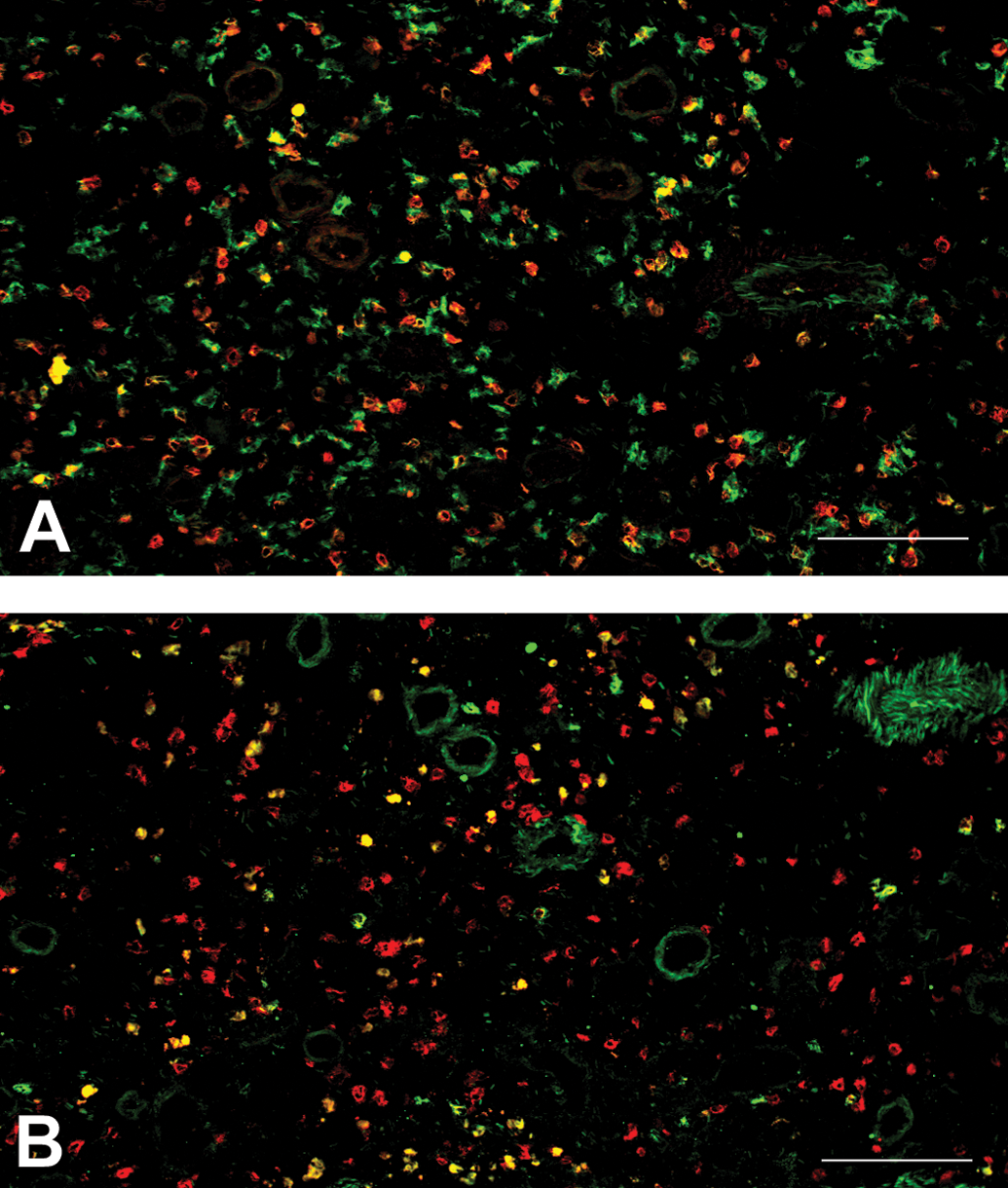
The number of CD4+/CD3+ T cells exceeds that of CD8+/CD3+ T cells. (a) CD4-positive T cells (yellow) presenting as double positive for CD4 (red) and CD3 (green). (b) CD8-positive T cells (yellow) presenting as double positive for CD8 (red) and CD3 (green). Immunofluorescence double staining. Scale bar: 50 μm.
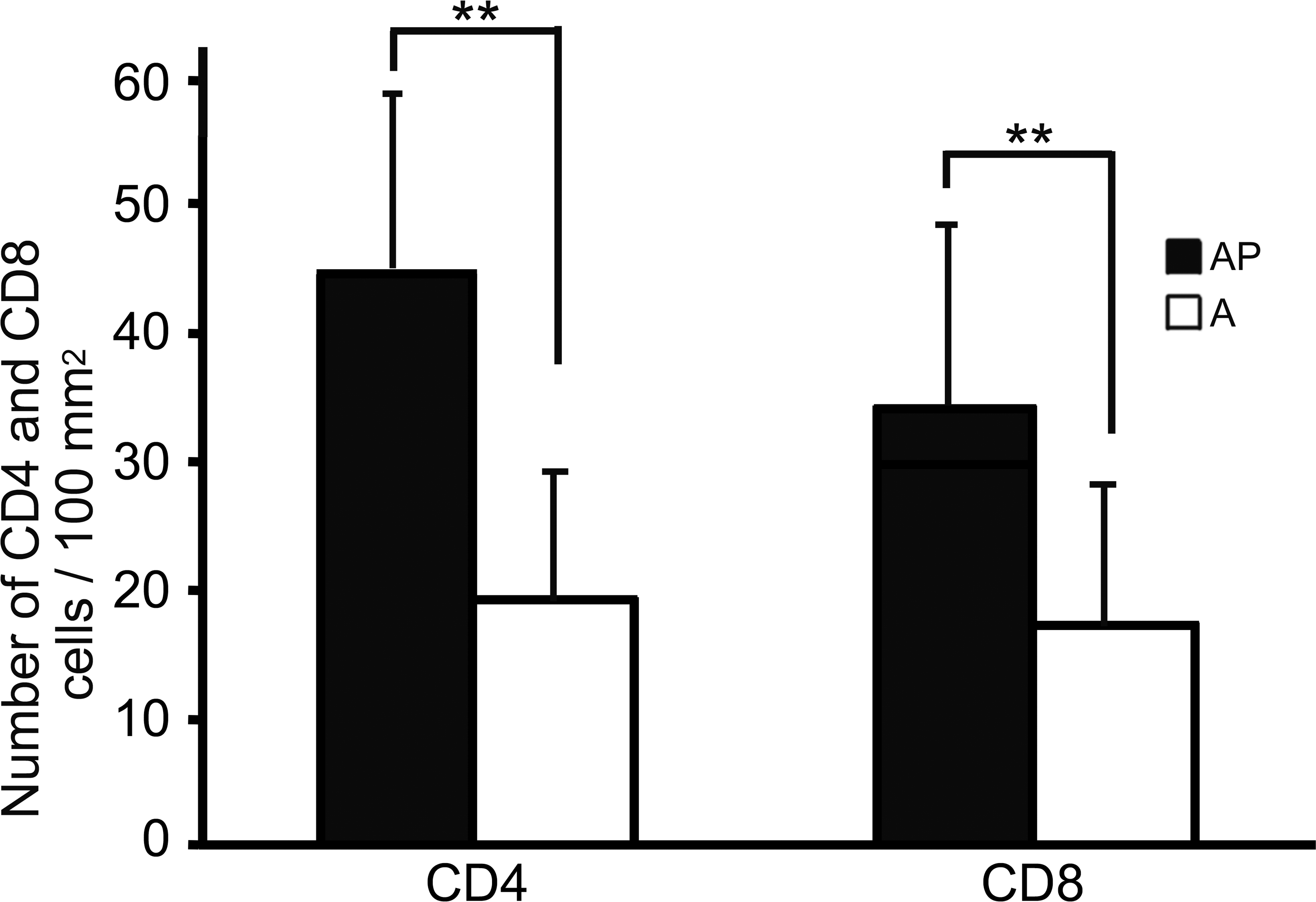
Comparison of the number of CD4+/CD3+ and CD8+/CD3+ T cells in the AP and A groups (**p < .01).
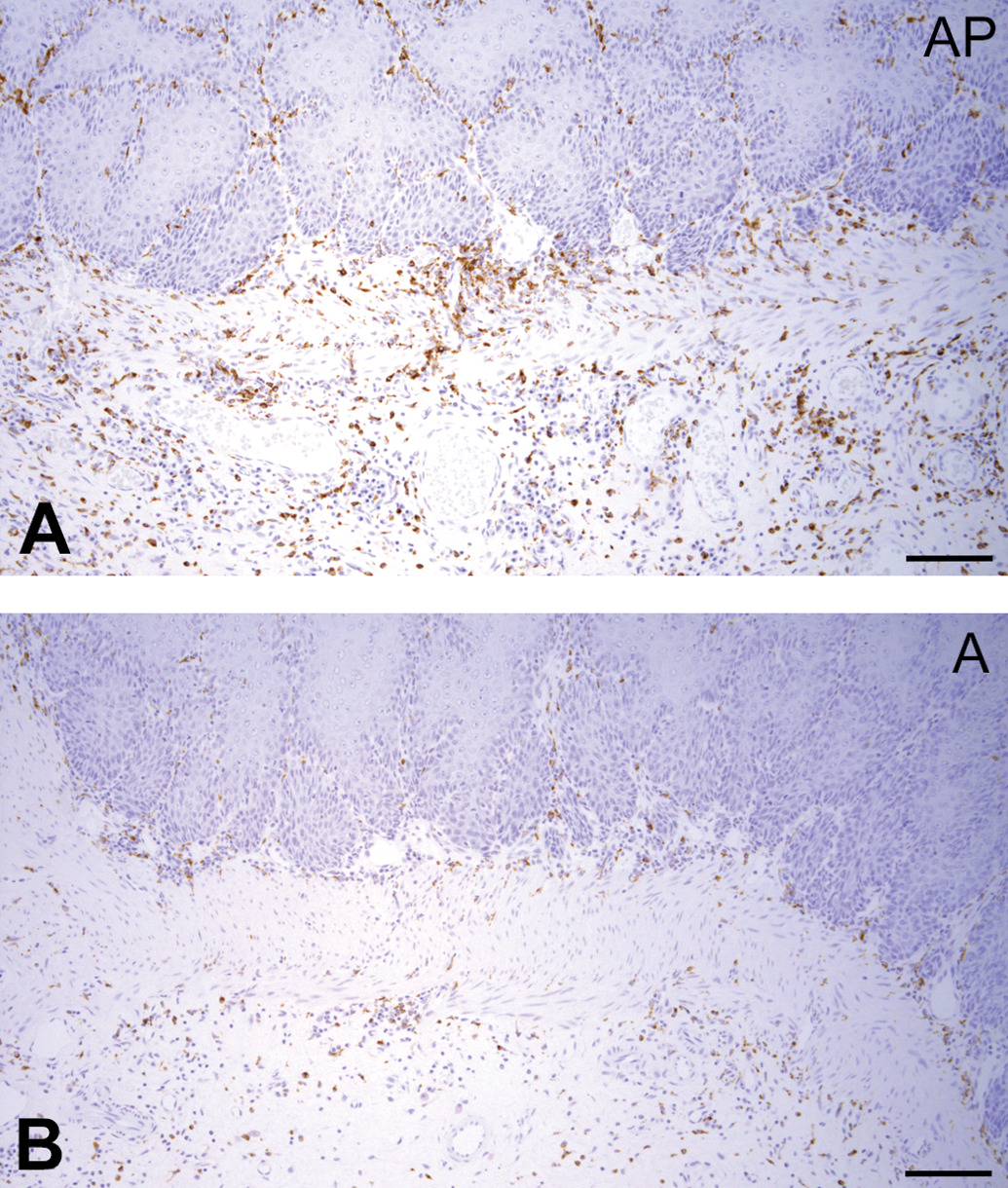
CD68-positive macrophages are increased in the AP group. (a) Strong expression of CD68 in the AP group. (b) Moderate expression of CD68 in the A group. Immunohistochemical analysis. Scale bar: 50 μm.
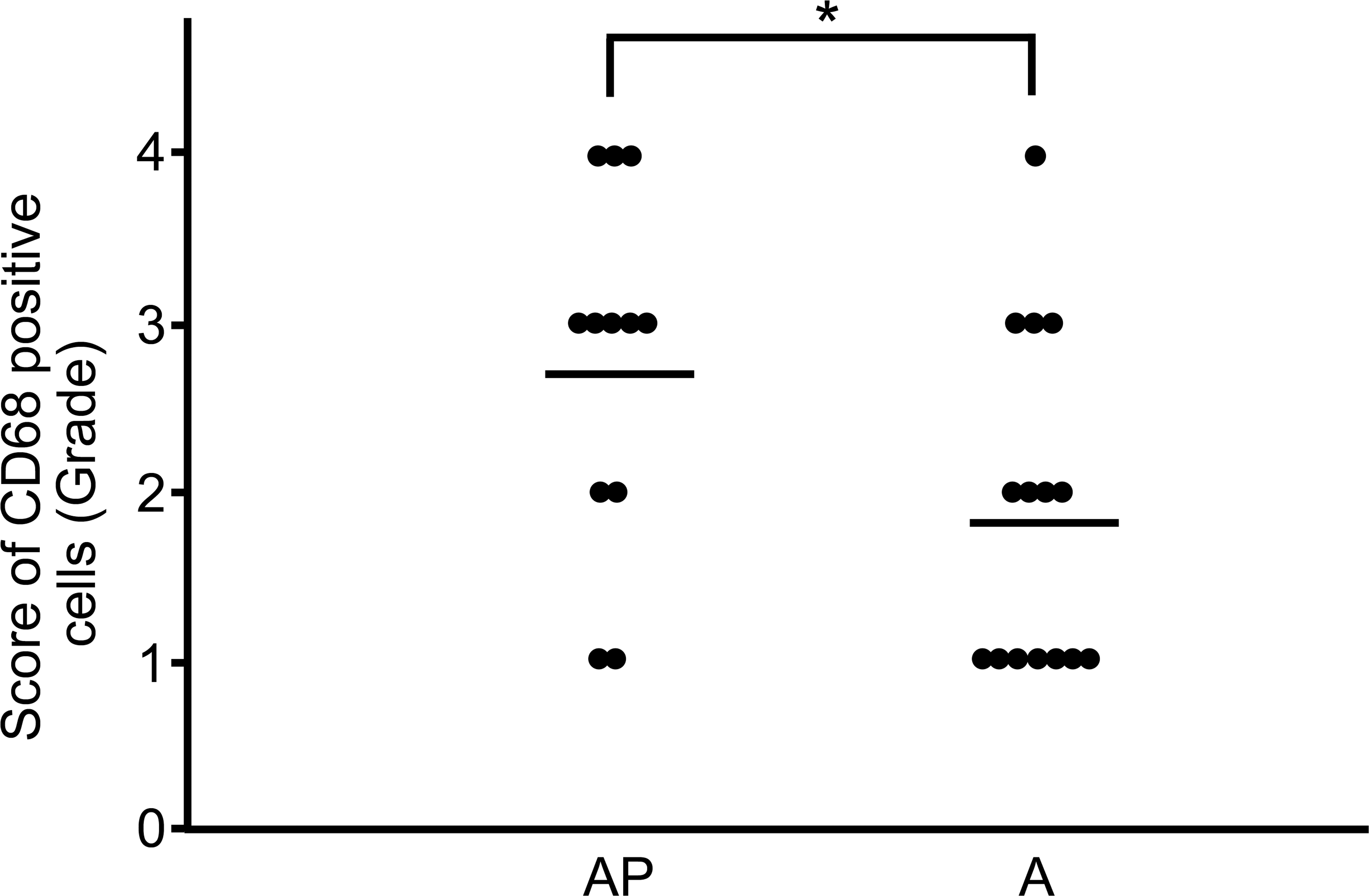
Score of CD68-positive macrophages in the AP and A groups. The bar indicates the mean value (*p < .05).
Proliferative Lesions of the Upper Gastrointestinal Tract Other Than the Forestomach
The severity of squamous cell hyperplasia and chronic inflammation with C. albicans infection in the mucosae of the tongue and cheek in the AP group was significantly enhanced compared to those in the A and P groups (p < .05), and the severity in the tongue mucosa was especially higher in the AP group. Epithelial hyperplasia of the gingiva and palate mucosa was observed in the AP and A groups; however, no significant difference was observed between these 2 groups. In the distal esophagus close to the cardia, squamous cell hyperplasia was also evident, but no significant difference was detected among the 3 groups. In the upper esophagus, these lesions were rarely observed in any group.
Discussion
In this study, we succeeded in inducing opportunistic chronic C. albicans infection and establishing an animal model for severe chronic hyperplastic candidiasis by combining a diabetic condition with intermittent prednisolone administration.
Our previous reports indicate that alloxan-induced diabetic rats exhibit mucosal proliferative lesions with chronic inflammation and some lesions progress to SCC in the forestomach after more than 50 weeks with the diabetic condition (Kodama et al. 2006). Notably, diabetes and C. albicans are considered to be deeply involved in the pathogenesis of mucosal proliferative and inflammatory changes because the lesions are suppressed by antidiabetic and antifungal treatment (Sano et al. 2009a, 2009b). In the current study, by intermittently administrating a low dosage of prednisolone in alloxan-induced diabetic rats, proliferative lesions opportunistically infected with C. albicans could be initiated and enhanced in all diabetic rats. In nondiabetic animals, opportunistic C. albicans infection has been known to be caused by the administration of high-dose immunosuppressive agents including prednisolone (Costa et al. 2013; Farah, Lynch, and McCullough 2010). However, in the present study, intermittent administration of low-dosage prednisolone (10 mg/kg) did not induce opportunistic fungal infection and mucosal proliferative changes in nondiabetic rats because prednisolone treatment at the used dosage could not induce sufficient immunosuppression in the healthy state. Conversely, diabetes increases susceptibility to various types of infections and acts additively to increase immunosuppressive activity in humans (Wilson, Tomlinson, and Reeves 1987). Thus, the combination of diabetes and intermittent prednisolone treatment was able to induce severe chronic hyperplastic candidiasis in our rat model.
Oral and gastrointestinal candidiasis in rodents is known to be induced by immunosuppressive dosages of prednisolone upon C. albicans inoculation; however, squamous cell hyperplasia and/or SCC cannot be induced because the duration of C. albicans infection is too short (Takakura et al. 2003; Abe 2004; Ishibashi et al. 2007). However, as severe oral candidiasis is rapidly formed 48 hr after administration of immunosuppressive dosages of prednisolone (Okada et al. 2013), it is clear that C. albicans infection is established in an immunosuppressed condition of short duration. In the present study, the body weight was decreased during the first week of prednisolone treatment but increased during the second subsequent week. Thus, the effect of prednisolone might disappear during the week following prednisolone treatment. In comparison, the administration of low-dosage prednisolone to diabetic rats may further lower immunity, which is suppressed by the diabetic condition immediately after treatment, thus allowing the establishment of C. albicans infection that could not be induced in nondiabetic rats. However, C. albicans infection gradually disappeared 2 weeks after prednisolone treatment in diabetic rats; thus, the next prednisolone treatment might allow reinfection of C. albicans. By repeating this cycle, persistent C. albicans infections may develop in diabetic rats intermittently treated with prednisolone; it is also highly possible that the squamous hyperplasia with chronic inflammation was exacerbated by the repetitive infection with C. albicans.
In humans, chronic hyperplastic candidiasis is known to develop to dysplasia from hyperplasia and ultimately progress to carcinoma (McCullough et al. 2002; Barrett, Kingsmill, and Speight 1998; Sitheeque and Samaranayake 2003; Williams et al. 2001; Bakri et al. 2010; Gainza-Cirauqui et al. 2013; Gall et al. 2013; Norgaard et al. 2013). In our previous study, chronic hyperplastic candidiasis progressed to SCC in diabetic rats, as observed in human disease (Kodama et al. 2006). In the present study, the development of SCC was reproduced over a much shorter period compared to that in the previous study. Furthermore, immunohistochemical analysis for squamous hyperplastic lesions as representative of precancerous lesions revealed that the numbers of CD4-positive T cells and CD68-positive macrophages were increased with enhancement of mucosal proliferative lesions. The chronic inflammation induced by persistent microbial infection forms and develops a microenvironment wherein lymphocytes and macrophages mainly infiltrate as part of the normal host defense, and which is also involved in the tumorigenesis and growth and/or survival of tumor cells (Grivennikov, Greten, and Karin 2010; Landskron et al. 2014). The most frequently infiltrated immune cells in the tumor microenvironment are T cells and tumor-associated macrophages (TAMs). T cells are known to be involved in tumor promotion, progression, and metastasis, and TAMs are reported to be obligatory for angiogenesis, invasion, and metastasis (Condeelis and Pollard 2006; Hanada et al. 2006; Langowski et al. 2006; Roberts et al. 2007). In addition, CD4-positive T cells have been shown to play an important role in the mechanism by which TAMs enhance tumor promotion in SCC of oral, esophagus, skin, and breast cancer (DeNardo et al. 2009; Daniel et al. 2003; Mori et al. 2011; Hatogai et al. 2016). In the present study, no clear evidence was obtained regarding whether CD4-positive T cells regulate macrophages and directly relate to tumorigenesis; however, the increase in the number of both cell types may be involved in the enhancement of proliferative lesions. Therefore, it is probable that continuous CD4-positive lymphocyte and macrophage infiltration affects the microenvironment of mucosal hyperplastic lesions and induces tumorigenesis arising from hyperplasia.
In conclusion, we succeeded in establishing a novel animal model for severe chronic hyperplastic candidiasis by combining diabetes and intermittent prednisolone administration. This severe candidiasis could be induced by opportunistic infection without direct administration of C. albicans and persisted over a long duration. Furthermore, our results suggest that it is probable that CD4-positive T cells and CD68-positive macrophages play an important role in the microenvironment of mucosal hyperplasia and are involved in the tumorigenesis arising from squamous hyperplasia.
Footnotes
Acknowledgments
We would like to thank Yusuke Nakajima, Yuto Fukatsu, and the staff at the Laboratory of Pathology in Setsunan University for their kind help and assistance during these experiments.
Author Contribution
Authors contributed to conception or design (YT, KO); data acquisition, analysis, or interpretation (YT, TM, KO); drafting the manuscript (YT, TM); and critically revising the manuscript (KO). All authors gave final approval and agreed to be accountable for all aspects of work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.