
Abstract
Asbestosis is a chronic lung disease caused by inhalation of asbestos, a fibrous mineral. It is one of the most severe diseases resulting from environmental contamination. We found asbestosis in a female Japanese macaque over 25 years of age that died from senility. Clear needle-like crystals were deposited throughout the lung lobes, particularly in the perivascular areas. Asbestos bodies were observed in some of these crystals. Fibrosis without inflammation was observed in the periarterial and peribronchiolar regions. The crystals were identified as tremolite, and a total of 16,633,968 asbestos bodies and 465,334,411 tremolite fibers were observed in 1 g of dry lung tissue. No tumors or pleural adhesions were seen. This is the first report of spontaneous asbestosis in a nonhuman animal.
Introduction
Asbestos consists of 6 types of serpentine minerals belonging to serpentine and amphibole classes: chrysotile, amphibole crocidolite, tremolite, amosite, anthophyllite, and actinolite (Huang et al. 2011). Asbestos has insulating qualities and high heat and chemical resistance and has been used as an inexpensive material for various industrial purposes. Inhalation of asbestos causes asbestosis (a type of pneumoconiosis) and predisposes to lung carcinoma and mesothelioma (Mcnulty 1962). The use of asbestos has been limited or banned worldwide. Asbestos-related diseases, including tumors, may not become apparent for 10 to 40 years after exposure, and new cases are still being reported (Neumann et al. 2013). In 2012, we found an asbestos-related disease in a Japanese macaque. To date, only human asbestosis has been reported. This is the first report of a spontaneous asbestos-related disease in a nonhuman animal.
Case Report
A female Japanese macaque (Macaca fuscata) over 25 years of age presented weighing 4.5 kg, much less than the average 8-kg weight of a healthy adult female. The patient was one of approximately 60 Japanese macaques in a facility in which the macaques were free-ranging and she was the oldest member of the group. A few days prior to death, pronounced scoliosis, generalized hair loss, abnormal posture and gait, and decreased strength were noted. The macaque collapsed and died, and a necropsy was performed. The monkeys were kept under free-range conditions in an enclosure surrounded by a concrete and wire mesh wall that had been renovated in 1985. In the enclosure, the only artificial structures were a wooden jungle gym and a small artificial pond. Asbestos was not found in these areas.
On postmortem examination, extensive anthracosis was observed throughout the lungs with black discoloration of the cut surface. Localized areas of emphysema were seen in both lungs at the margins (Figure 1). Pleural effusion, adhesions between the thoracic wall and the visceral pleura, thickening, and neoplastic lesions of the pleura were not observed. The macaque also had mature bilateral cataracts and advanced degeneration of the thoracic and lumbar spines.
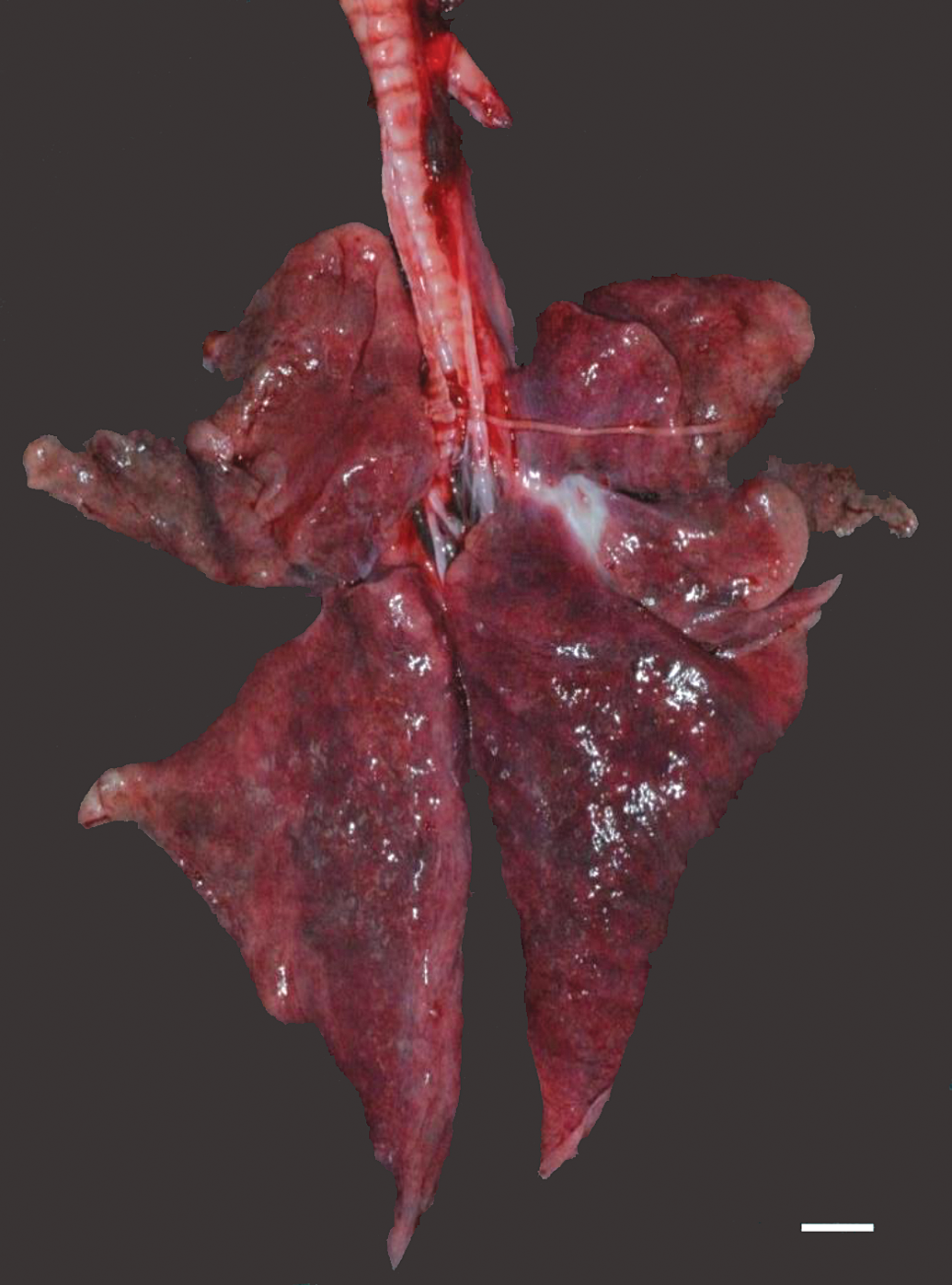
Extensive anthracosis throughout the entire lung lobe. Bar = 1 cm.
For histopathological examination, the lung tissue was fixed in formalin and embedded in paraffin using conventional methods, sliced into 3- to 5-μm sections, and stained with hematoxylin and eosin (H&E), Azan, and Berlin blue stains.
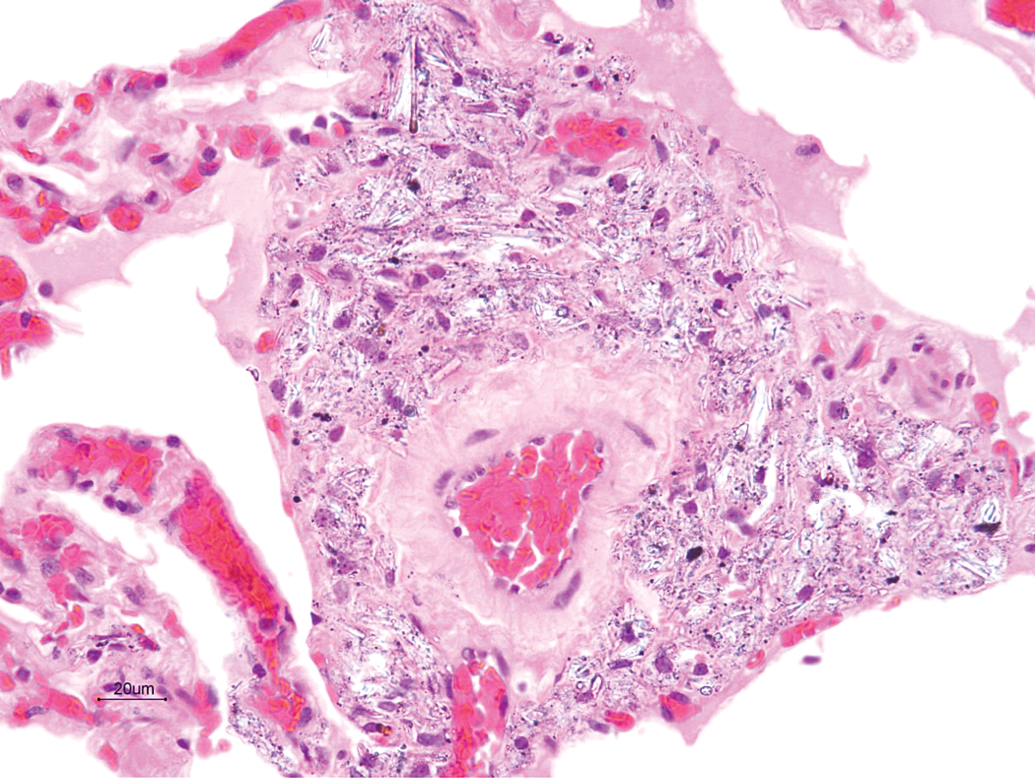
Histologically, multifocal narrowing of the alveolar spaces because of lack of perfusion and moderate diffuse congestion were observed in the lungs. Observations consistent with emphysema were detected microscopically, such as rupture of the alveolar walls and expansion of the alveolar space. Clear needle-like crystals and black granular material were deposited throughout the lung lobes, predominantly in the perivascular regions. Similar crystals were deposited in the peribronchial areas and the alveolar walls (Figure 2). Crystals were also deposited in the medulla of hilar lymph nodes, superficial cervical lymph nodes, axillary lymph nodes, and inguinal lymph nodes; and hilar lymph nodes showed the most significant degree of crystal and black granular material deposits in those lymph nodes. Some of the often-observed deposits appeared as brown dumbbell-shaped bodies (Figure 3). Similar structures were observed in the alveolar walls and spaces. A pale, homogeneous fluid containing alveolar macrophages was present in some alveolar spaces. This pale fluid showed positivity in the Periodic acid-schiff (PAS) stain, indicating that this was an alveolar surfactant. The peribronchial and perivascular areas were moderately to highly thickened with fibrosis, as shown by an Azan stain (Figure 4). The small and medium arterial walls were thickened, and edematous and connective tissue hyperplasia was observed in the perivascular areas (Figure 5). The inflammatory response was minimal and included the brown iron dumbbell-shaped bodies stained using the Berlin blue stain, confirming that they were asbestos bodies (Figure 6).
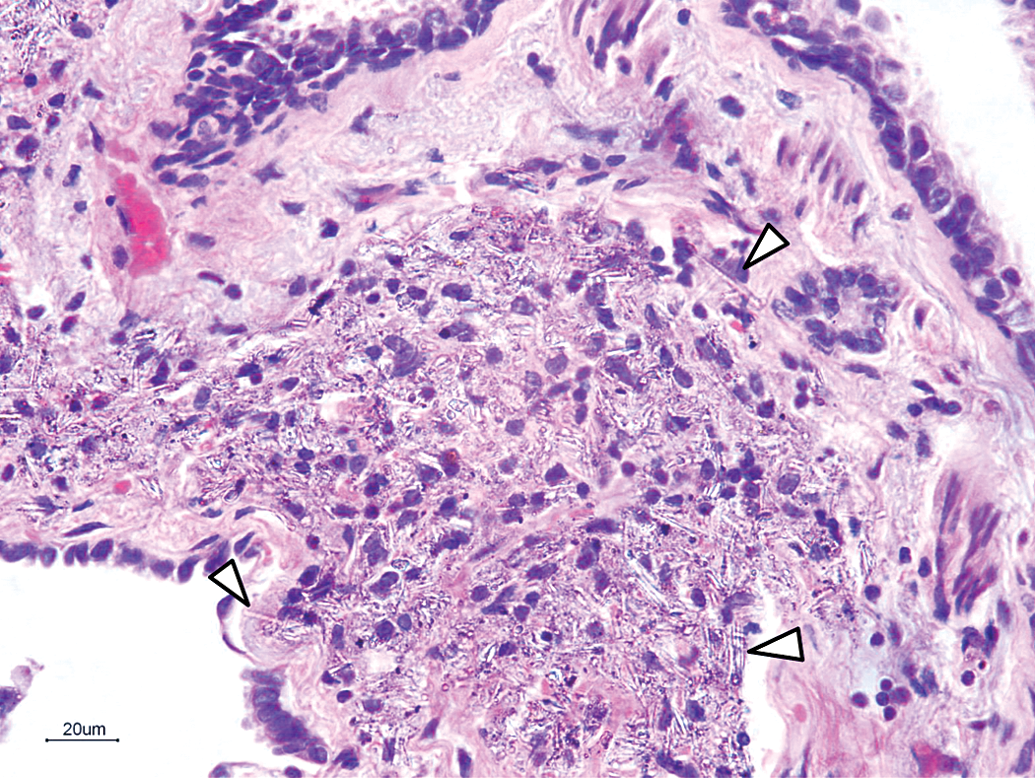
Thickened peribronchiolar areas with needle-like deposits. Some needle-like deposits are indicated by arrow heads; hematoxylin and eosin (H&E) stain.
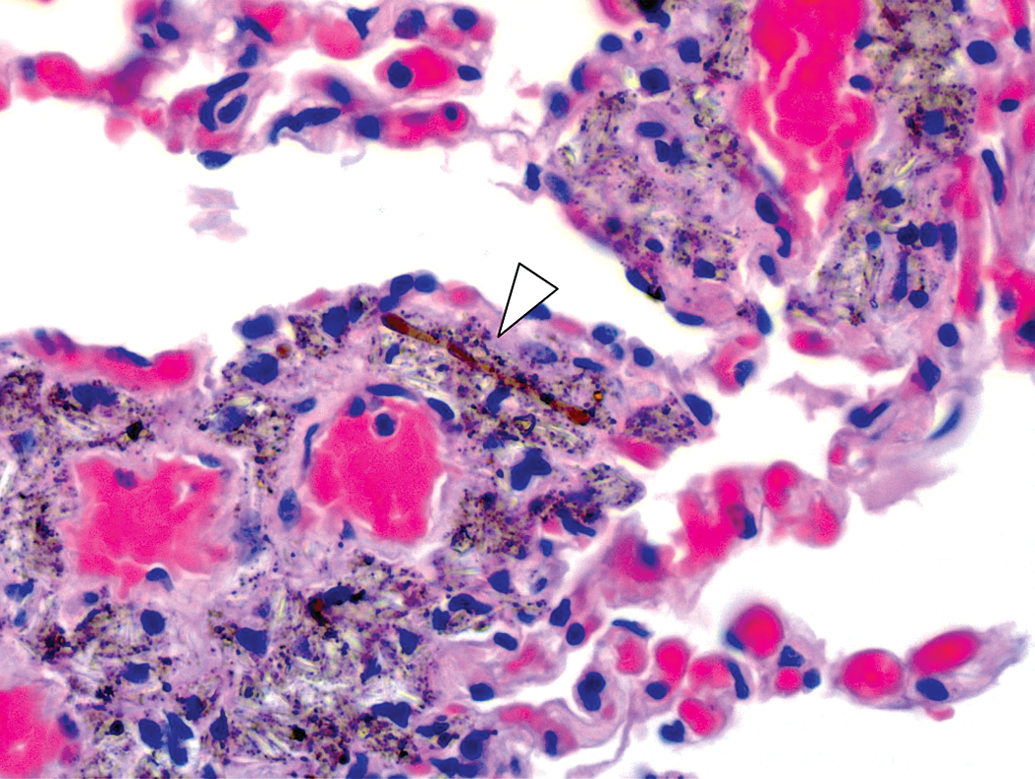
Dumbbell-shaped structures within the needle-like deposits (arrow head). hematoxylin and eosin stain (H&E).
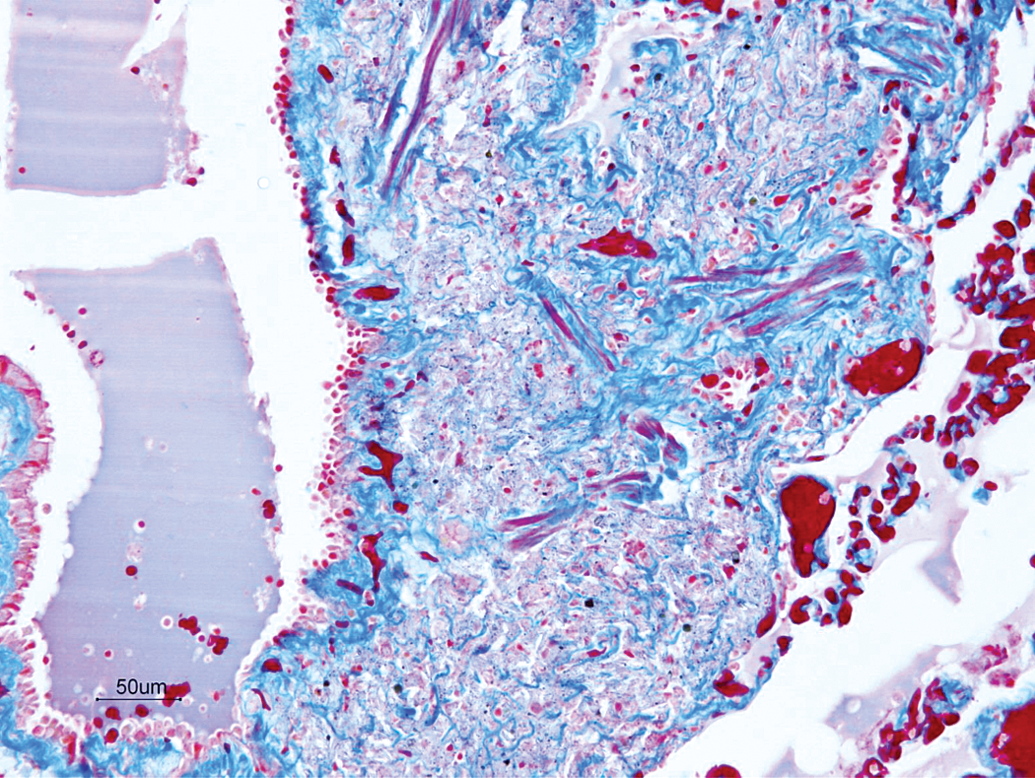
Peribronchiolar fibrosis. Azan stain.
Needle-like deposits around the perivascular area; hematoxylin and eosin stain (H&E).
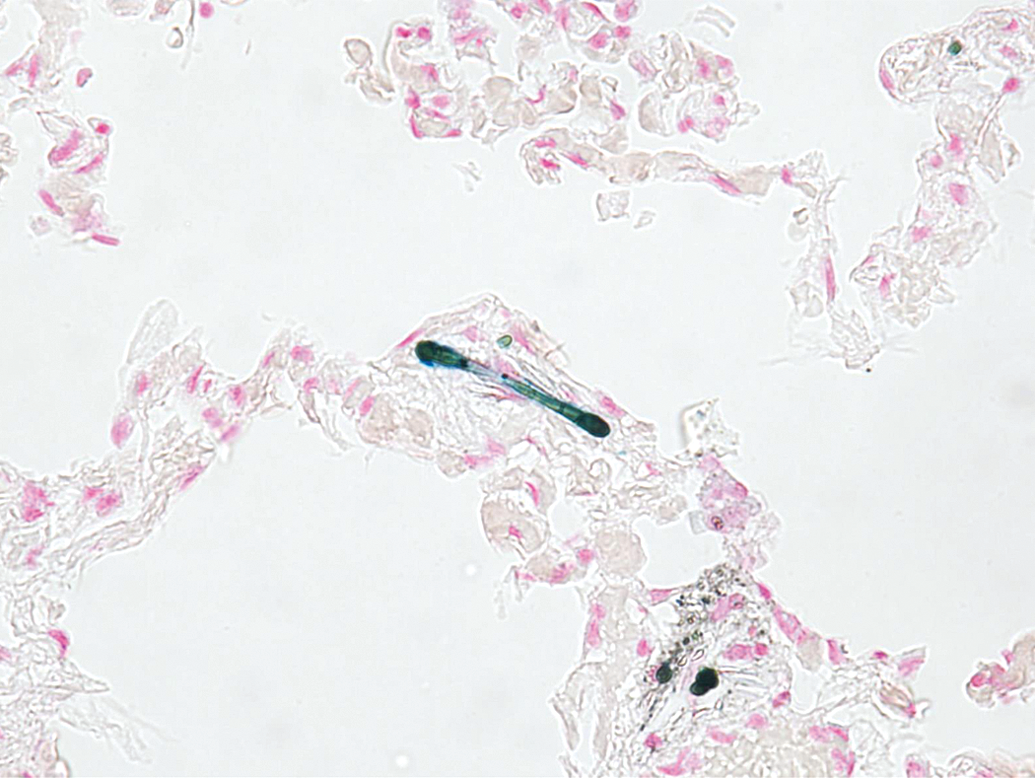
The dumbbell-shaped structures stained blue and contained Fe3+. Berlin blue stain.
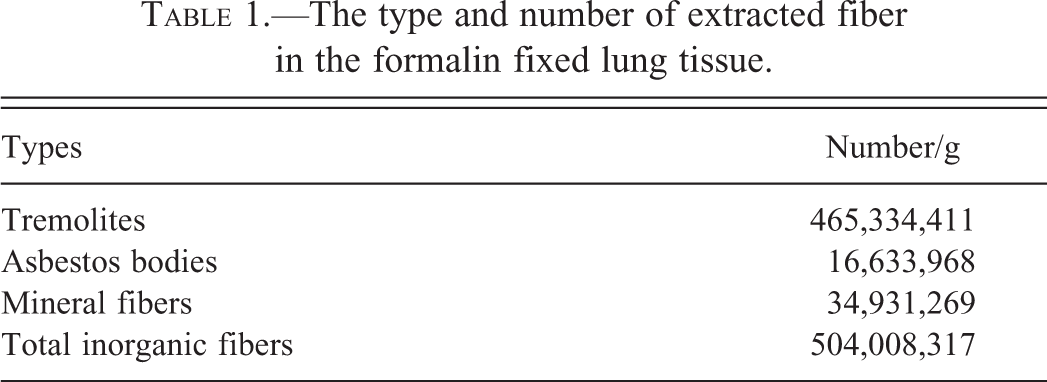
To identify the deposits, we extracted the asbestos from the formalin-fixed lung. Approximately 1 g of the lung tissue was dried. The tissue was immersed and dissolved in 150 ml of a 12% hypochlorous acid solution. The solution was centrifuged at 1,500 revolutions per minute (rpm) for 5 min, the supernatant was decanted, and the precipitate was mixed with 20 ml of chloroform. Next, 20 ml of 50% ethanol was added, stirred well, and centrifuged again at 800 rpm for 10 min to remove the carbon powder floating between the ethanol and the chloroform layers. The insoluble deposits were prepared in a 1-ml suspension of 95% ethanol and collected using a 5-μm filter. The deposits were observed using a low vacuum scanning electron microscope (Miniscope® TM3030 [Hitachi high tech, Kawasaki, Japan]). The extracted deposits exhibited elongated straight rod-like forms, often covered entirely by brown dumbbell-shaped deposits (Figure 7). We also examined the samples by X-ray diffraction using an energy dispersive X-ray analyzer Quantax70 (Hitachi High-Tech). The diffraction spectrum pattern of the deposits was consistent with tremolite (Figure 8). Results of the phase difference dispersion microscopy quantitative analysis revealed 16,633,968 asbestos bodies; 504,008,317 total fibers; 465,334,411 tremolite fibers; and 34,931,269 inorganic fibers in 1 g of dried lung tissue (Table 1, Figure 9). Five other monkeys from the same enclosure died. The reasons for death were heat-related illness because of excessive movement in 2 of the 5 cases, and tetanus in the other cases. However, asbestos deposition was not observed upon histopathological examination of their lungs.
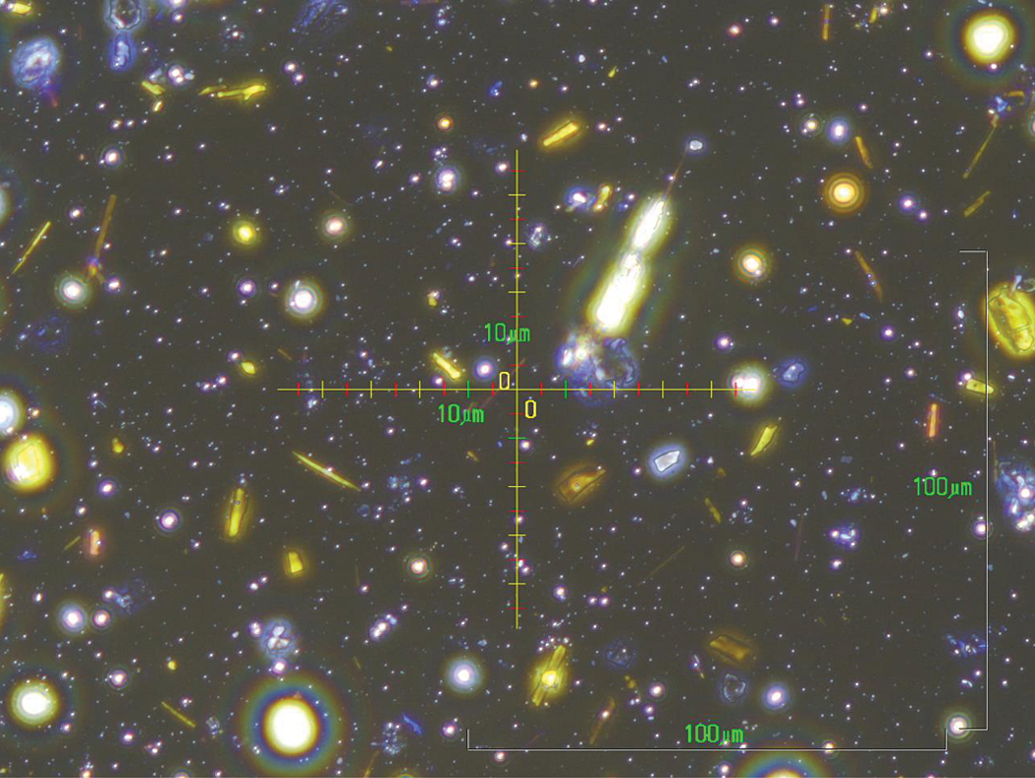
The yellow-colored fibers are tremolites and the large bright structures in the center are asbestos bodies as seen with a phase-contrast microscope.

The asbestos bodies are dumbbell shaped and node like with fine straight fibers in the core as seen with the scanning electron microscope. Bar = 10 µm.
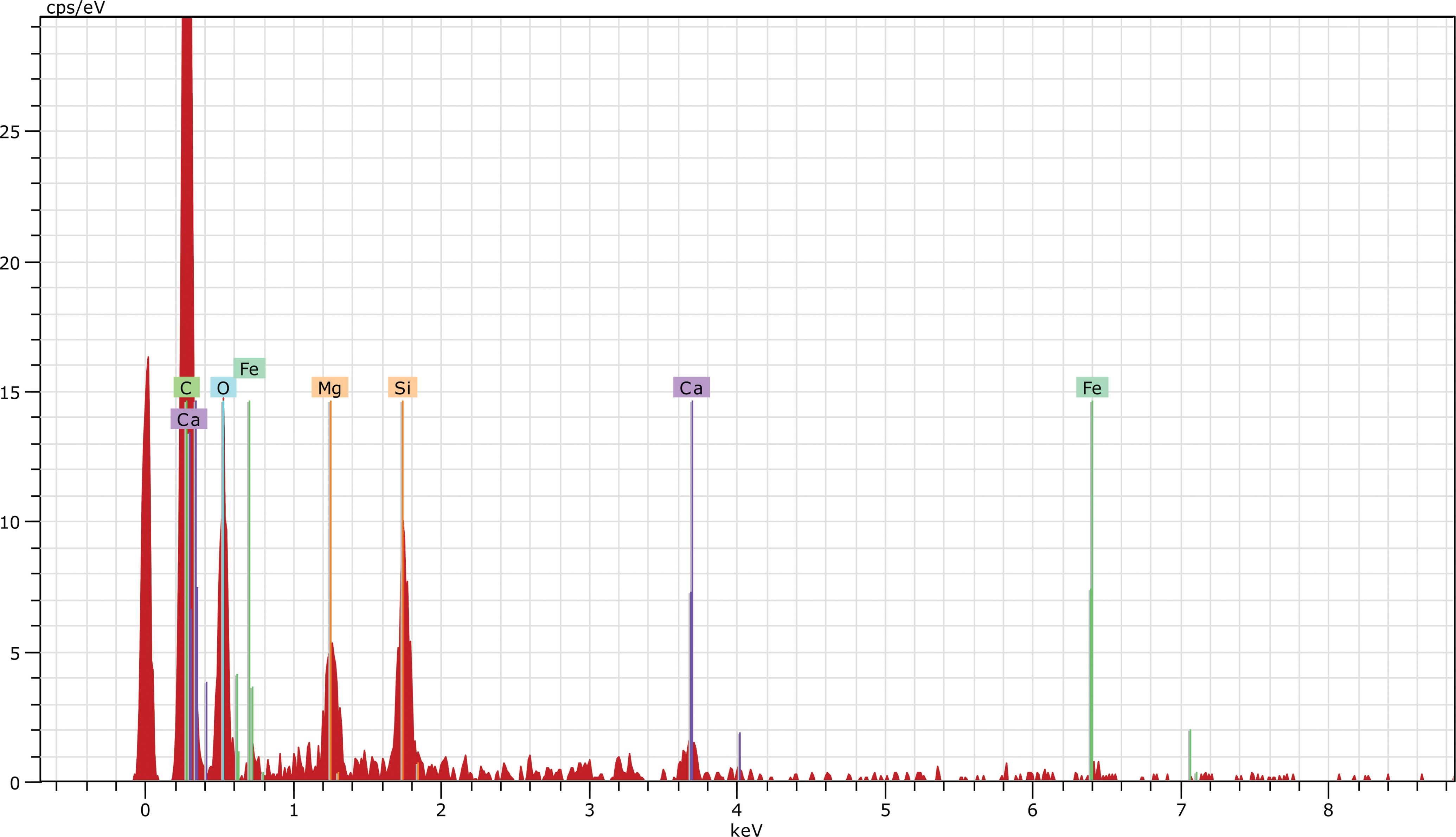
The X-ray diffraction; the spectral pattern is consistent with tremolite.
The type and number of extracted fiber in the formalin fixed lung tissue.
Senile plaques are formed in the brains of Old World monkeys at 25 years of age or older (Yue et al. 2014). To estimate the approximate age of the macaque, the brain was examined using the Gallyas–Braak method and anti-Aβ40 and anti-Aβ42 antibody immunohistochemistry (Braak et al. 1988). Typical senile plaques and cerebrovascular amyloidosis were observed throughout the cerebrum (Figure 10).
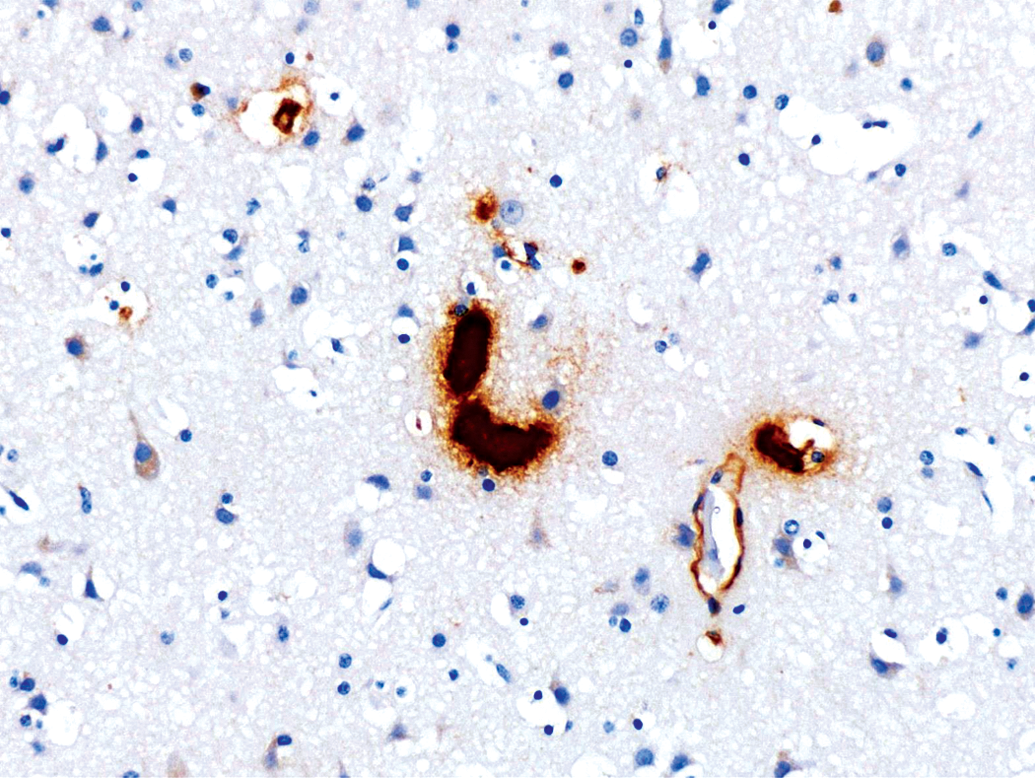
Senile-plaque observed in the cerebrum and deposited of Aβ amyloid in the wall of cerebral blood vessel for immunohistochemical method of using anti-Aβ42 antibody.
Discussion
Asbestosis is a form of pneumoconiosis caused by exposure to a high concentration of asbestos and characterized by a diffuse stromal fibrosis starting in the peribronchiolar area (Cullinan and Reid 2013; Kishimoto 2014). Thickened pleural plaques, diffuse pleural thickening, benign asbestos pleural effusion, lung carcinoma, and mesothelioma are typical sequelae (Liu, Cheresh, and Kamp 2013; Kishimoto 2014). The presence of asbestos bodies provides clear evidence of a previous asbestos exposure (Iuchi 2009). The asbestos body is rod-like, thick at both ends, and is described as dumbbell shaped. Asbestos exists in the center and is coated with an iron-containing protein (Shukla et al. 2003). It takes a long time for asbestos bodies to form, and uncoated asbestos fibers are much more frequently observed than asbestos bodies (Craighead et al. 1982). In our patient, ultramicroscopic observation confirmed that the many needle-like deposits in the lung were asbestos, and the iron dumbbell-shaped structures were asbestos bodies. Using X-ray diffraction, the needle-like deposits were identified as tremolite, one of the forms of asbestos. The toxicity of asbestos varies with the form, but all forms are toxic and carcinogenic (Churg and Wiggs 1984; Hodgson and Darnton 2000). This patient was diagnosed with asbestosis because of fibrosis and asbestos deposits in the periarterial and peribronchiolar areas and the alveolar walls. We propose that the observation of crystals in some lymph nodes suggests that the crystals moved from the site of deposition to the lymphatics running parallel to the vessels, thereby explaining why crystals were found in the perivascular and peribronchial regions. Pleural thickening, pleural effusion, and neoplastic lesions were not seen. The expression of asbestos-related diseases is associated with the type and amount of asbestos and the duration of exposure (Kishimoto 2014). Tremolite and crocidolite are highly carcinogenic (Churg and Wiggs 1984). Workers compensation certification standards in Japan specify concentrations equal to or greater than 5,000 asbestos bodies/g and 200,000 fibers/g in the lung. Our case was considered a very high exposure because the concentration of asbestos bodies was about 3,300 times and the concentration of fibers was about 2,300 times higher than these standards. Further, the patient lived a long time after the exposure because a long period is required to form asbestos bodies. Thus, although this patient had high concentrations of carcinogenic asbestos that had been deposited for a long period of time, neoplastic lesions were not observed.
The cause of asbestos-related disease is associated with oxygen radicals, but the mechanism is not understood (Kamp et al. 1992). In rats, tumors can be induced by intraperitoneal asbestos administration, but it is very difficult to induce tumors by inhalation (Shin and Firminger 1973). Tumor development has not been observed in monkeys in either short-term or long-term experimental exposures (Platek et al. 1985). Asbestosis develops over a course of many years, and lung carcinoma and mesothelioma take several decades to develop in humans (Hodgson and Darnton 2000; Kishimoto 2014). In our patient, extensive senile plaques and cerebrovascular amyloidosis in the brain, cataracts, and degenerative spondylosis were observed, so this patient was estimated to be quite elderly; however, tumor-related lesions were not observed. The absence of tumor development may have been due to a short exposure or species differences. Given these observations in addition to the severe wasting, the cause of death of this patient was considered to be weakness and circulatory failure due to senility; therefore, asbestosis was the indirect cause of death.
This patient had several lesions that are similar to those found in human asbestosis, such as multifocal narrowing of the alveolar space, emphysema, and hypersecretion of alveolar surfactant; thus, we propose that this patient’s lesions were similar to those observed in human asbestosis, such as emphysema.
Currently, there is no asbestos in the enclosure and there was no deposition of asbestos in the other monkeys that died. This facility was renovated at 1985, so considering that this patient may have been over 27 years of age, the exposure may have occurred at the old facility. Records of the design and specifications of the old facility were not available so the source of the exposure could not be identified. This is the first reported case of spontaneous asbestosis in an animal.
Footnotes
Acknowledgments
We thank Mr. Kazuhiko Kimura and Mr. Hiroaki Ito, Hitachi High-Tech, Kawasaki, Kanagawa, Japan, for scanning electron microscopy and X-ray diamator technical support, and Mr. Takayuki Okada, Japan Industrial Safety and Health Association, Minato-ku, Tokyo, Japan, for expertise and the quantitative asbestos determination. We also thank Ms. Elika Takahashi, Laboratory of Veterinary Pathology, School of Veterinary Medicine, Azabu University, for Gallyas-Braak method and immunohistochemical staining.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contribution
All authors (KT, AK, YU) contributed to conception or design; data acquisition, analysis, or interpretation; drafting the manuscript; and critically revising the manuscript. All authors gave final approval and agreed to be accountable for all aspects of work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.