
Abstract
A 32-month-old male common marmoset had a firm and white-colored mass in the duodenal wall. The cut surface was smooth and grayish white in color. Histologically, the mass consisted of a proliferation of spindle cells with an oval to spindle-shaped nucleus and scant eosinophilic cytoplasm in a loose myxoid or fibrotic background. Most of the lesion displayed no specific growth pattern whereas some of the cells concentrated around the vessels and created an onion-bulb structure. Additionally, marked inflammatory cellular infiltration, mainly eosinophils, was observed throughout the lesion. Immunohistochemically, the spindle cells were positive for vimentin, α-smooth muscle actin, fascin, and cyclin D1, and negative for S-100, factor VIII–related antigen, and c-kit. These histological and immunohistochemical features did not meet any differential diagnoses such as gastrointestinal stromal tumor, inflammatory myofibroblastic tumor, solitary fibrous tumor/hemangiopericytoma, smooth muscle tumor, schwannoma, and hemangiosarcoma. Collectively, the authors diagnosed the mass as a lesion that corresponded to an inflammatory fibroid polyp (IFP) in humans. IFP is defined as a mesenchymal proliferation composed of spindle stromal cells, small blood vessels, and inflammatory cells, particularly eosinophils, and is currently classified as a nonneoplastic lesion. To the best of our knowledge, this is the first case of spontaneous IFP in nonhuman primates.
Keywords
Introduction
The common marmoset (Callithrix jacchus) is a popular experimental animal bred in well-established colonies, small in size, with relatively rapid generational turnover, is abundant in the wild, and has low zoonotic risk (Abbott et al. 2003; David, Dick, and Hubbard 2009; Tardif et al. 2006). While several background lesions and spontaneous tumors have been published in common marmosets, the varieties of the lesion are relatively limited when compared to those in rodents (Betton 1984; Kaspareit et al. 2006; David, Dick, and Hubbard 2009). Here, we encountered a spontaneous lesion considered to be an inflammatory fibroid polyp (IFP) in the duodenum of a common marmoset. IFP is generally regarded as a non-neoplastic lesion, which infrequently occurs in the gastrointestinal tract in humans (Odze and Goldbrum 2009). IFP has been reported in many articles and the diagnostic criteria have been established in human pathology, whereas few reports are available in the animal pathology field. We believe this is the first case of spontaneous IFP in nonhuman primates.
Case Report
All procedures were performed under the rules for animal experiments according to the Japanese guideline of animal experiments (Science Council of Japan 2006), and “Regulations for the Use of Animals in Research” approved by the Daiichi Sankyo Institutional Committee of Animal Experiments. A male common marmoset (Callithrix jacchus) was introduced to our laboratory via CLEA JAPAN, Inc. (Tokyo, Japan). Atovastatin was orally administered with a high-fat diet to examine its efficacy. The dosage levels of atorvastatin were 1, 3, and 10 mg/kg/day and each treatment period did not exceed 6 days. It was euthanized at 32 months of age by exsanguination under ketamine anesthesia 6 months after the final dosing, due to the termination of the study. The animal had never been administered other agents and showed no abnormal clinical signs or parasitic infection in the laboratory tests.
A mass was incidentally found in the duodenal wall during the autopsy. It was trimmed and fixed in 10% neutral buffered formalin. Sections obtained from paraffin-embedded tissue were stained with hematoxylin and eosin (HE). To clarify the presence of collagen fibers in the stroma, Masson’s trichrome staining (MT) was performed. The sections were stained for eosinophils with Luna’s method (LM) and aldehyde fuchshin staining (AF). Additionally, immunohistochemistry was performed for antihuman antibodies such as vimentin, α-smooth muscle actin (α-SMA), fascin (known as a dendritic cell marker; Pantanowitz et al. 2004), factor VIII–related antigen (FacVIII), S-100, c-kit, cyclin D1, CD34, and CD35 using a two-step peroxidase 3,3′-diaminobenzidine staining technique with a DAKO Envision+ Kit (Dako Japan, Tokyo, Japan), according to the manufacturer’s instructions. Counterstain was performed with hematoxylin. Immunohistochemical information including antibody dilutions and known target cells are listed in Table 1. Furthermore, for transmission electron microscopy, tissue samples were retrieved from the paraffin-embedded block. The deparaffinized block was treated via rehydration with descending alcohols, postfixation in 1% osmium, and redehydration with a graded series of ethanols and QY-1 (Nisshin EM, Tokyo, Japan), as well as infiltration and embedding in Epon 821.
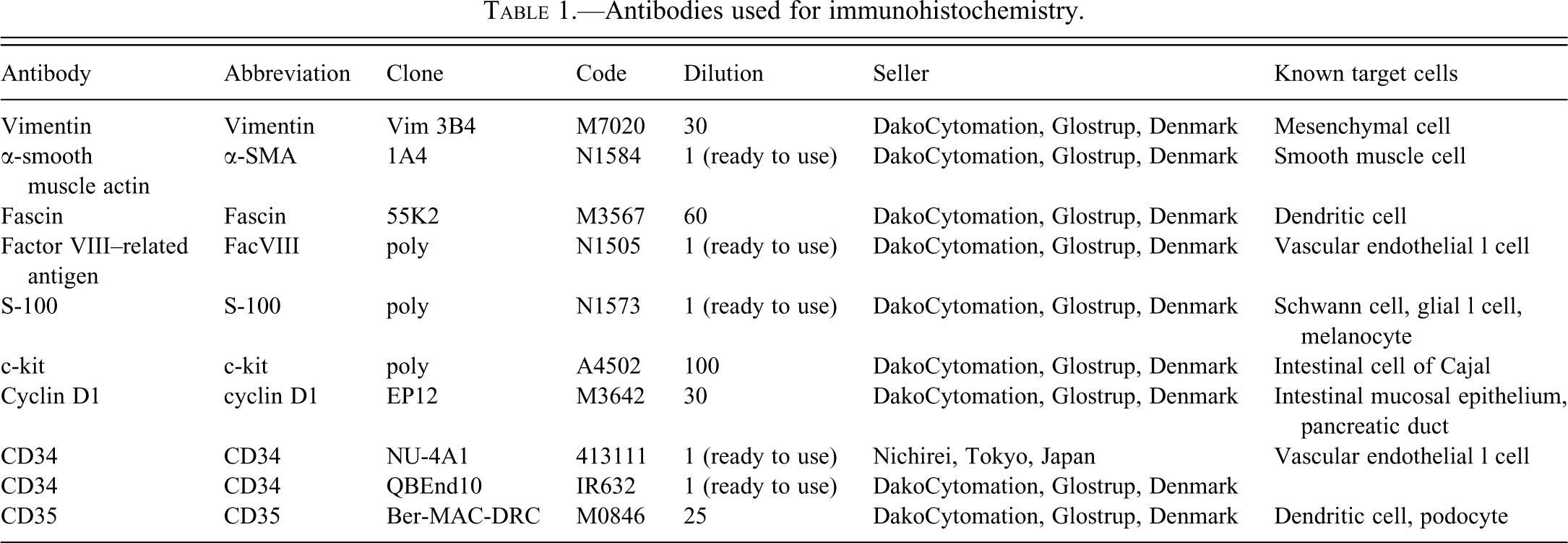
Antibodies used for immunohistochemistry.
Macroscopically, the mass was firm, 2 × 2 × 1.5 cm3 in size, and grayish white in color. The cut surface was smooth, grayish white in color, and confined to the duodenal wall (Figure 1). The duodenal papilla and common bile duct were not recognized. Microscopically, the lesion was located in the submucosa without clear demarcation from the adjacent tissue including the pancreatic lymph node and pancreas. The overlying mucosa showed ulceration, and the underlying smooth muscle layer was split and focally atrophied. There were no necrotic or hemorrhagic areas. Most of the mass consisted of a proliferation of spindle cells and did not show specific proliferation patterns such as interwoven, herringbone, nuclear-palisading, or fascicular patterns. The spindle cells had an oval to spindle-shaped nucleus with a single or a few brilliant nucleoli and scant eosinophilic cytoplasm and were embedded in myxoid or fibrotic substances which proved to be collagen fibers by MT (Figure 2A). Nuclear atypia of the cells was slight, and no mitoses were observed. In addition to those findings, there were many single-layered fragile vessels in a few areas. Some of them were surrounded concentrically by the spindle cells, and onion-bulb structures were formed (Figure 2B). There were also medium-sized vessels with a tunica media (Figure 2C). Additionally, marked inflammatory cell infiltration was observed throughout the lesion. Almost all cells were segmented leukocytes which had eosinophilic granules, and proved to be eosinophils by LM and AF (Figure 2D). Lymphocytes and/or plasmocytes were occasionally aggregated, resembling focal lymphoid follicles.
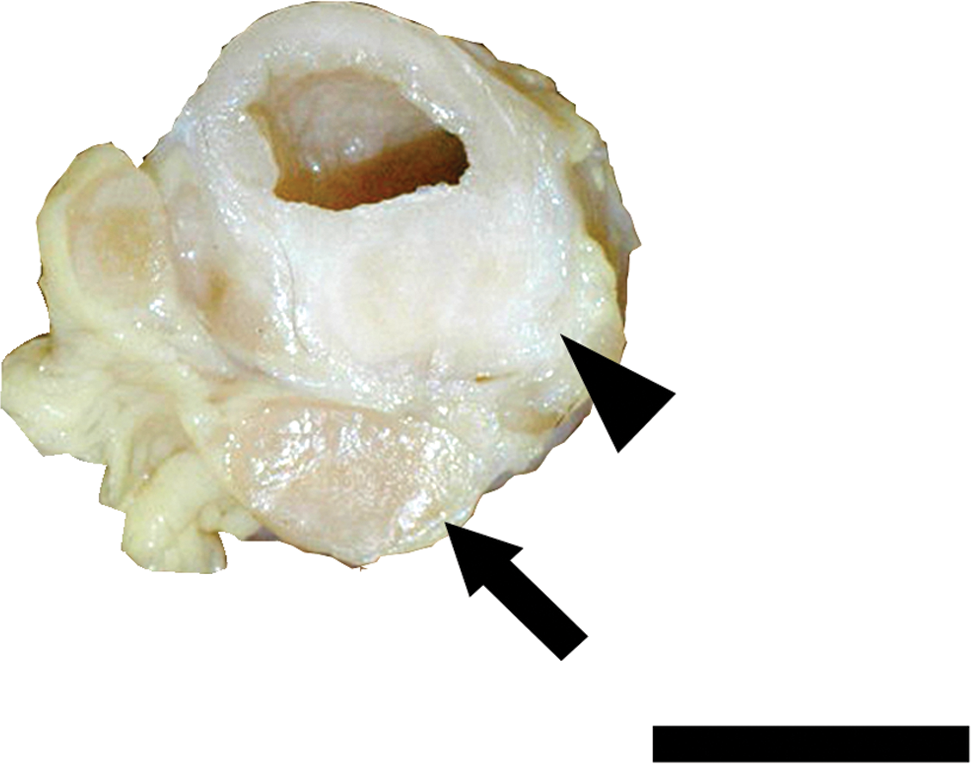
Macroscopic appearance of the duodenum with a mass. The cut surface (arrowhead) was smooth and grayish white in color. Pancreatic lymph node (arrow) is also shown; Bar: 2 cm.
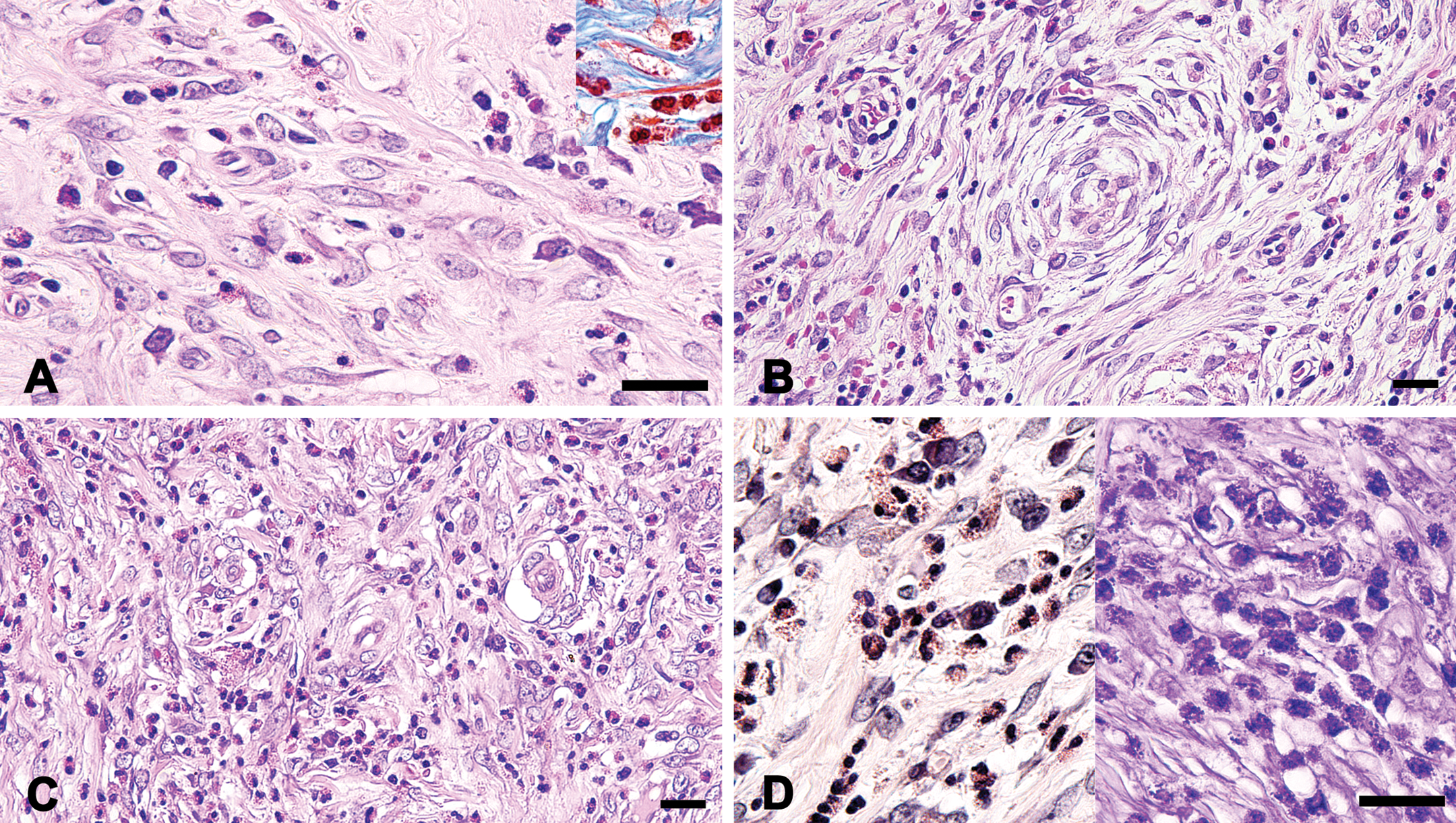
Histological appearance of the lesion. Most of the mass consisted of a proliferation of spindle cells in a myxoid or collagenous background. Segmented leukocytes were also observed; HE staining; Inset, Masson’s trichrome staining (A). In a few areas of the mass, many small vessels and concentrated spindle cells (onion-bulb structures) were seen; HE staining (B). There were medium-sized vessels with tunica media; HE staining (C). Granules in segmented leukocytes were stained in red-orange by Luna’s method (left) and in per se by Aldehyde Fuchshin staining (right) (D); Bars: 20 µm (A–D).
The results of immunohistochemistry are shown in Table 2. Immunohistochemically, the spindle cells exhibited diffuse positive reaction for vimentin, α-SMA, and fascin (Figures 3A, 3B, and 3C, respectively). For cyclin D1, focal immunoreactivity was obtained (Figure 3D). FacVIII, S-100, and c-kit were negative. On the other hand, the endothelia of vessels were positive for vimentin, fascin, FacVIII, and cyclin D1. Vascular smooth muscle cells were positive for vimentin, α-SMA, and cyclin D1. Immunohistochemistry for antihuman CD34 and CD35 had no crossreactivities. Ultrastructurally, most of the spindle cells were surrounded by wide spaced and sparse collagen fibrils. The cells had an oval-to spindle-shaped nucleus with a slight groove in the nuclear membrane. The cytoplasm contained well-developed rough endoplasmic reticula and a small number of mitochondria. Representative ultrastructural appearances of the spindle cells are shown in Figure 4A and B.
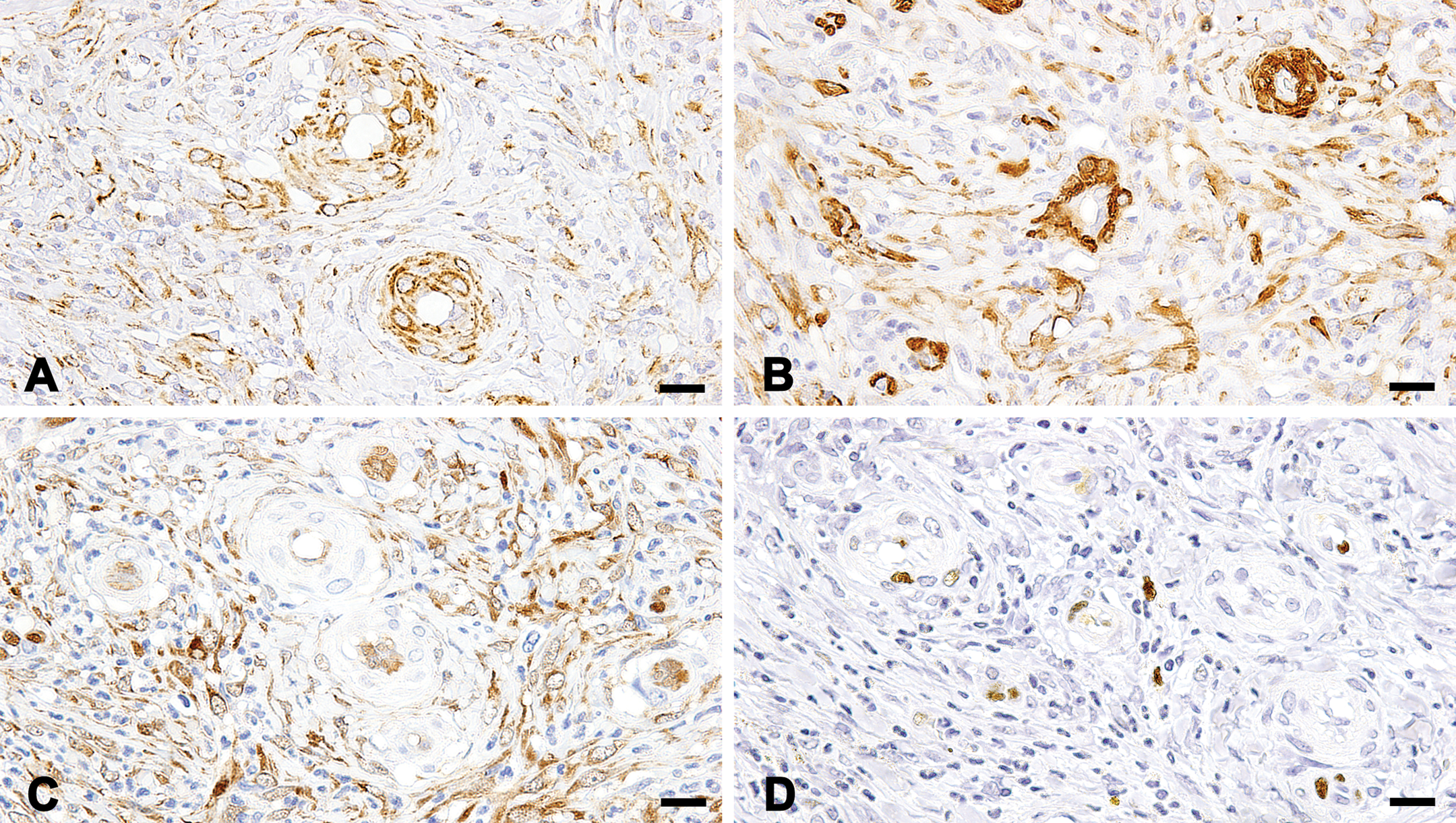
Immunohistochemistry for vimentin (A), α-smooth muscle actin (B), fascin (C), and factor VIII–related antigen (D). Vimentin; the spindle cells, endothelia, and vascular smooth muscle cells were positive (A). α-smooth muscle actin; the spindle cells and vascular smooth muscle cells were positive, whereas the endothelia were negative (B). Fascin; the spindle cells and endothelia were positive, whereas vascular smooth muscle cells were negative (C). Cyclin D1; the spindle cells, endothelia, and vascular smooth muscle cells were focally positive (D). Bars: 20 µm (A–D).
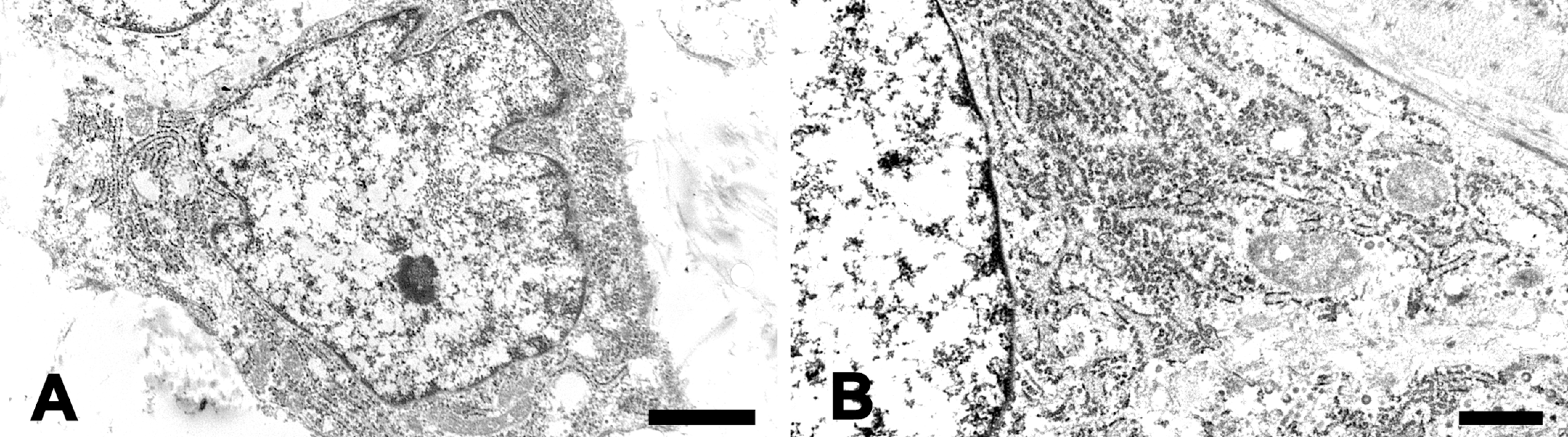
Representative ultrastructural appearance of the spindle cell. The cell had an oval nucleus with slight groove in the nuclear membrane (A). The spindle cell contained well-developed rough endoplasmic reticula and a small number of mitochondria in the cytoplasm (B). Bars: 2 µm (A), 1 µm (B).
Summary of immunohistochemical findings.
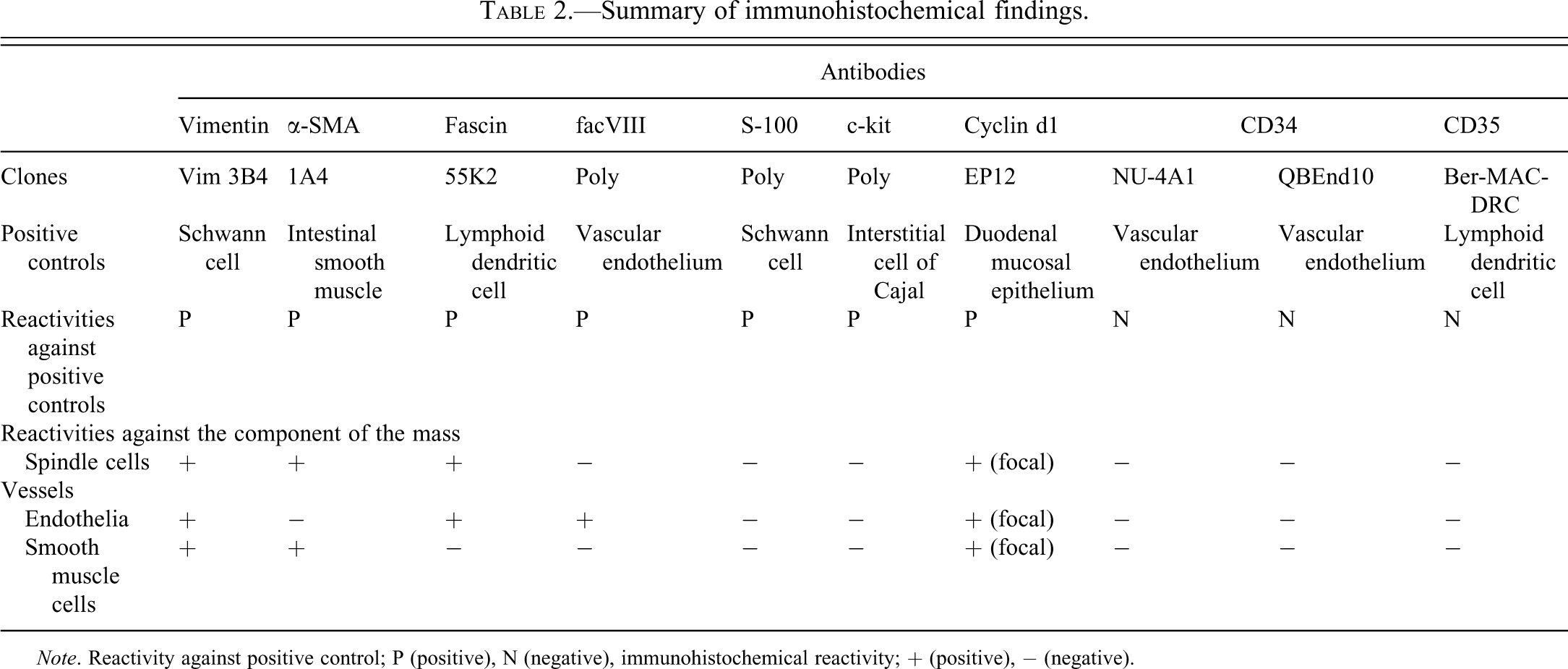
Note. Reactivity against positive control; P (positive), N (negative), immunohistochemical reactivity; + (positive), − (negative).
In the present case, a proliferation of the spindle cells with an onion-bulb structure around fragile vessels, marked infiltration of eosinophils, and aggregation of lymphocytes were seen as characteristic structures. These histological appearances corresponded to those of IFP in humans (Odze and Goldbrum 2009; Daum et al. 2010). The findings of immunohistochemistry and electron microscopy did not conflict with the criteria of IFP (Daum et al. 2010; Navas-Palacios et al. 1983). Thus, the lesion was diagnosed as an IFP.
IFP was first reported as a polypoid fibroma for cryptogenic gastric granulomatous lesion with eosinophil (Konjetzny 1920). Subsequently, similar lesions have been diagnosed with different names, such as hemangioendothelioma, inflammatory pseudotumor, granuloma with eosinophilic infiltration, fibroma with eosinophils, and so on, until detailed histological characteristics of the lesion in the stomach were manifested (Vanek 1949). The nomenclature was established in 1953, and IFP is now generally accepted as a nonneoplastic lesion in humans (Helwig and Ranier 1953; Odze and Goldbrum 2009). In humans, IFP tends to be found incidentally in the submucosa or lamina propria of the stomach or the small bowel with occasional ulceration of the adjacent mucosa. However, the incidence in the duodenum is low: 1% of the total occurrence in the gastrointestinal tract (Wysocki, Taylor, and Windsor 2007).
Typical histological features of IFP have been demonstrated as follows: (1) an exuberant, noncapsulated, localized proliferation of mononuclear spindle-shaped cells with an inflammatory infiltration often dominated by eosinophils, (2) vascular construction with a network of variably sized blood vessels, (3) concentric arrangement of spindle-shaped cells providing an “onion-bulb”-like appearance around vessels, and (4) an aggregation of lymphocytes sometimes providing a lymph node-like structure (Wysocki, Taylor, and Windsor 2007; Trillo and Rowden 1991). Moreover, detailed classification based on the histological subtypes has been suggested, although it seems to be uncommon. For example, classical fibrovascular, nodular, sclerotic, and edematous IFPs, and their coexisting pattern in one lesion have been reported (Kim and Kim 1988). Immunohistochemically, the spindle cells of IFP are known to be positive for vimentin, CD34, CD35, cyclin D1, and fascin, whereas the stainabilities for α-SMA, HHF-35 (actin muscle), CD68, and Mac 387 (antimacrophage antibody) are variable (Pantanowitz et al. 2004; Santos Gda et al. 2004; Daum et al. 2010; Odze and Goldbrum 2009). On the contrary, c-kit, a typical marker for the gastrointestinal stromal tumor (GIST), is negative (Santos Gda et al. 2004; Pantanowitz et al. 2004; Daum et al. 2010). Although the present case did not show crossreactivity for CD34 and CD35, positive reactions for vimentin, fascin, and cyclin D1 in the spindle cells corresponded to the above characteristics. In human cases, IFP has been reported to express cyclin D1 diffusely (Pantanowitz et al. 2004), whereas the present case did not. It was unclear why the stainabilities (positive cell ratio) were different between human and the present case. However, the result was also considered to be supportive for the diagnosis.
There are a few reports dealing with the ultrastructural features of IFP, but not limited to the spindle cell. The lesion consists of loose granulofibrillar material comprising of extracellular space, and the spindle cell had abundant and generally uniform rough endoplasmic reticulum. Prominent arborizing vasculature and small capillaries without apparent lumina have also been demonstrated (Navas-Palacios et al. 1983). Our case was not in conflict with these characteristics.
In the present case, the final diagnosis was conducted based on its histological characteristics in combination with immunohistochemistry. However, the following differential diagnoses were addressed: GIST, inflammatory myofibroblastic tumor (IMFT), solitary fibrous tumor/hemangiopericytoma, smooth muscle–derived tumor, schwannoma, and hemangiosarcoma. According to the present histopathological characteristics including eosinophil infiltration and immunohistochemical specificity, all of these tumors can be excluded. For example, GIST can be discarded due to the absence of typical histological patterns and prominent eosinophil infiltration. Furthermore, a negative result was obtained for c-kit in the present case, which is generally positive for GIST (Benjamin, Hawk, and Turnbull 1977). Although no obvious immunohistochemical differences between IFP and IMFT have been reported, IMFT is known to lack the onion-bulb structure and eosinophil infiltration (Makhlouf and Sobin 2002). Solitary fibrous tumor/hemangiopericytoma can be eliminated by the absence of staghorn-like vessels. Immunohistochemical reactivities for vimentin, α-SMA, and fascin are common in smooth muscle tumors (Kefeli et al. 2009). However, abundant collagen fibers shown by MT are inconsistent with their diagnostic criteria. Finally, the lack of immunoreactivity for S-100 or FacVIII indicates that schwannoma and hemangiosarcoma can be excluded from the diagnosis, respectively.
The pathogenesis of IFP is a matter of debate. Several factors (parasite infection, immune defection, and vascular inflammation) provoking IFP have been suggested without robust evidence (Wysocki, Taylor, and Windsor 2007). The origin of the spindle cell is also unclear. On the basis of a recent study, the cell has been proposed to originate from fascin-positive dendritic cells or CD34-positive perivascular cells (Pantanowitz et al. 2004). Positive immunoreactivity for fascin in our case might support the theory in part. IFP has been treated as a nonneoplastic, reactive pseudotumor with its benign biological behavior in clinical pathology. However, the neoplastic nature of IFP has been demonstrated by the identification of platelet-derived growth factor α-receptor mutation, which is robust evidence of tumoral proliferation (Calabuig-Farinas et al. 2009). There is even the term inflammatory fibroid tumor, and consensus has not been reached as to whether the lesion is neoplastic or nonneoplastic (Wysocki, Taylor, and Windsor 2007; Calabuig-Farinas et al. 2009; Lasota et al. 2009).
Statins (atorvastatin and fluvastatin) are known to induce hyperplasia and/or inflammation in the gallbladder of beagles and rhesus monkeys at 8 mg/kg or more (Hartman et al. 1996; Walsh, Albassam, and Clarke 1996). The possibility arises that the atorvastatin treatment evoked the lesion in any of the mechanisms. However, there were no histological findings in the liver and gallbladder in the present case. Additionally, the treatment period in the previous reports was much longer (26 weeks) than that of the present case. Although species difference in sensitivity needs to be marked, it is considered that there is no causal relationship between drug administration and the occurrence of the lesion. On the other hand, the involvement of the duodenal papillae with the lesion is unclear. Several cases of duodenal IFP formed in close range of the papil of Vater have been reported in humans, while the pathogenesis is undetermined (Wysocki, Taylor, and Windsor 2007; Yoshimura et al. 2010). It might be possible that focal abnormality in the duodenal papillae is involved in the initial formation of IFP. In the present case, however, accurate location of the structure was not confirmed and the relationship between them was not clarified. To clarify it, further investigations are required.
In human epidemiology, IFP generally occurs in the sixth decade in both sexes, and the incidence of gastric IFP in females is quite high as compared to those of other generations in females and males (Ozolek et al. 2004; Pantanowitz et al. 2004). In this regard, the present case might be worthy of remark, because the animal was a 32-month-old male which corresponds to a young or middle-aged man.
In animals, IFP has been mentioned as a spontaneous lesion in the cecum of a rabbit and in the stomach of a hypereosinophilic syndrome rat model (Sano et al. 2001; Pizzi, Hagen, and Meredith 2007). However, detailed identification including immunohistochemistry has not been performed in either case. To the best of our knowledge, this is the first case of spontaneous IFP in nonhuman primates. We believe this report will contribute to the establishment of diagnostic criteria of IFP in animals.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.
Abbreviations
Acknowledgments
The authors are grateful to Keiko Okado and Yoshikazu Ishii, Daiichi-Sankyo RD NOVARE Co., Ltd., for their technical assistance in the slide preparation for electron microscopy. All authors are employed by Daiichi-Sankyo.