
Abstract
Repeated bolus intravenous (IV) administration of large doses of beta-lactams and aminoglycosides has previously been associated with the development of eosinophilic and occlusive arterial lesions limited to the lungs in calves. Reviewing 13 years worth of records from left ventricular assist device implantation studies, morphologically identical segmental arterial lesions were present in 32 of the 56 calves receiving IV antibiotics, affecting lungs (6/50), kidneys (12/56), or lungs and kidneys (14/50). In 16 of these calves, renal arterial lesions spatially colocalized with renal cortical infarctions. Lesions were noted in additional abdominal organs in 4 of the 50 calves and were exclusively present in the liver in a single calf. Similar arterial lesions were also noted in the lungs (3/4), kidneys (1/4), liver (1/4), and spleen (1/4) of unimplanted calves receiving similar IV antibiotic regimens for bacterial infections. Lesions were observed with therapeutic IV doses of cephalosporins with or without aminoglycosides over shorter intervals than previously implicated. Lesions were significantly associated with increased peripheral eosinophil counts and mildly elevated, not reduced, arterial pulse pressures. This report documents the features of an idiosyncratic drug reaction with features strongly suggestive of an acute type-I hypersensitivity in this species.
Because of their size, physiology, anatomy, cost, and tractable nature, calves are used for in vivo testing of cardiovascular support devices. In the development and preclinical in vivo testing of left ventricular assist devices (LVADs), the inflow cannula of the implanted pump is placed in the ventricular apex, and the outflow cannula is anastomosed to the descending thoracic aorta. As part of device development, the kidneys, because of their downstream location, high blood flow, and end-arterial circulation, are carefully evaluated for the presence of infarctions that could be caused by thromboembolic events related to the device. To prevent infection in chronically implanted animals, prophylactic antibiotics are administered starting prior to the first skin incision and extending for several days postoperatively. Often these animals are anticoagulated to limit device-related thrombosis, and therefore antibiotics are given intravenously (rather than intramuscularly) to avoid both intramuscular hemorrhage and artifactual elevations in serum enzymes due to skeletal muscle injury from injection.
In 1979, Majeski and Fitts described the development of eosinophilic and occlusive pulmonary arterial lesions (EOA) in female Hereford calves receiving repeated bolus intravenous (IV) administration of supratherapeutic doses of antibiotics (Majeski and Fitts 1979). Antibiotics given were penicillin (one or two million units) and streptomycin (1 or 2 g) or sodium cephalothin (12 g), and these dosages were administered over a course of 20 to 76 days. More recently, Morton et al. described a similar spectrum of lesions in male Sprague-Dawley rats receiving IV infusions of large volumes (40–80 mL/kg) of isotonic saline for 30 days (Morton et al. 1997). In both reports, lesions were limited to pulmonary arteries.
In this report, we describe morphologically identical arterial lesions not only in medium and large pulmonary arteries but also in medium and large arteries of the kidney, spleen, and liver in thirty-six of the sixty calves (60%) receiving therapeutic doses of IV beta-lactam antibiotics with and without aminoglycoside antibiotics over <1 to 22 days duration. Lesion correlations with invasive systemic blood pressures and peripheral eosinophil counts are reported. Importantly, renal arterial lesions were spatially associated with renal cortical infarctions in sixteen calves, which can be a confounder for these studies.
Materials and Methods
All procedures were approved by the Institutional Animal Care and Use Committee, and animals were housed in facilities accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International. Veterinary care was in accordance with The Guide for Care and Use of Laboratory Animals (8th Edition; 2011). All necropsy records for calves receiving LVAD devices between 1998 and 2011 were reviewed. Calves were 3- to 5-month-old Holstein–Friesian steers or bulls obtained from two different sources. Beginning in 2007, calves were vaccinated for shipping fever (Express 5-HS, Boehringer Ingelheim, Ridgefield, CT), Moraxella bovis (Ocu-Guard MB-1, Boehringer Ingelheim), and rabies (Rabvac 3, Fort Dodge, Fort Dodge, IA), dewormed with ivermectin pour-on, given parenteral supplemental vitamin E and selenium (Mu-Se injection, Schering-Plough Animal Health, Summit, NJ), and fed a coccidiostat (monensin) on arrival. All calves tested negative for bovine viral diarrhea virus (BVDV) by ear notch immunohistochemistry. Prior to 2007 calves were not vaccinated, fed a coccidiostat, or BVD tested, and were treated for parasites only on a clinical presentation. After acclimation, calves intended for LVAD implantation were given 1 g IV bolus cefazolin sodium (Novaplus, Novation, Vancouver, BC) and slow IV infusion of either 80 or 120 mg tobramycin (Sicor Pharmaceuticals, Irvine, CA) or 80 mg gentamicin 1 hr prior to induction of anesthesia; then every 6 hr postoperatively for 7 to 10 days. Under general anesthesia, a left lateral thoracotomy was performed to implant an LVAD. Pumps tested were from four different manufacturers with multiple different sizes and designs including pulsatile, continuous, and mixed flow operation. During LVAD implantation, the left mammary artery was catheterized for invasive blood pressure monitoring, recorded hourly in the postoperative interval. Some calves were anticoagulated with IV warfarin, titrated to effect. Other calves were not anticoagulated as part of the study. Automated blood cell counts were performed at regular intervals on a Heska CBC-Diff veterinary hematology system (Loveland, CO) and confirmed with a manual differential. If the animal’s hematological data indicated no infection, the animal was weaned off of tobramycin first, followed by cefazolin usually 0 to 4 days later. Calves were put back on cefazolin and aminoglycoside or given ceftiofur sodium (Ceftiflex, Med-Pharmex, Pomona, CA) 2.2 mg/kg IV bolus once daily or ampicillin (Sandoz Inc., Princeton, NJ) 1 g IV slowly over 15 min four times daily as needed based on clinical evidence of infection.
At termination of study, animals were anesthetized with methohexital and euthanized with IV pentobarbital and phenytoin sodium. Four nonimplanted calves that received IV antibiotic regimens therapeutically for spontaneous bacterial infections, and using the same antibiotic dosage schedules, were euthanized for diagnostic necropsies performed for herd health status. These four calves were not anticoagulated. Gross necropsy was performed and tissues were immersion fixed in 10% neutral buffered formalin. For diagnostic necropsies of unimplanted calves, complete tissue sets were collected including brain, eye, heart, lung, liver, kidneys, spleen, rumen, reticulum, omasum, abomasum, small and large intestine, cecum, adrenals, and tongue. For experimental necropsies of implanted calves, because of device routing, brain/eye was not sampled unless neurologic signs were present. Kidneys were always sampled. Additional tissues were taken when grossly abnormal or for studies of greater than 2 days duration. Tissues were processed in an automated Tissue-Tek VIP processor and paraffin-embedded with a Tissue-Tek TEC embedding station (Sakura Finetek, Torrance, CA). Sections were cut at 6 µm for routine hematoxylin and eosin (H&E) staining. Selected sections were additionally stained with Luna’s stain for eosinophils, Verhoeff-van Gieson stain for elastin, or Masson’s trichrome for collagen and elastin. All images were obtained with an Olympus BX51 microscope and DP71 digital camera using MicroSuite Basic 2.6 imaging software (Center Valley, PA). All slides were reviewed by a single board certified veterinary pathologist (TKC).
For immunohistochemistry, slides were deparaffinized and heat-induced antigen retrieval was performed in citrate buffer. Endogenous peroxide was blocked, and slides were incubated for 1 hr at room temperature with mouse monoclonal antibodies to alpha smooth muscle actin (α-SMA, Dako clone 1A4, 1:50) or smoothelin (Abcam ab8969, 1:200) followed by biotinylated secondary antibody using a Vector Elite ABC kit and DAB chromagen. Slides were counterstained with Mayer’s hematoxylin.
All quantitative results were compared by student’s unpaired t test using Graphpad software. Results are reported as mean
Results
Gross renal cortical infarctions, consisting of firm areas of cortical pallor with depression of the capsular surface, were present in sixteen LVAD-implanted calves (Figure 1). On cut surface, arcuate and radial arteries were sometimes noted to have prominent thickened white walls (Figure 2). By histologic examination, there were wedge-shaped areas of nephron dropout and atrophy with glomerulosclerosis, florid interstitial fibrosis, and chronic mononuclear inflammatory cell infiltrates (Figure 3). These lesions were spatially associated with tortuous and redundant arcuate and radial arteries displaying prominent thickening of the wall with resultant compression and occlusion of the lumen and marked intimal and adventitial eosinophil infiltration. There was no evidence of recent or remote thrombosis observed in these vessels. An additional four calves had areas of renal cortical infarction in which no spatial relationship to renal EOA lesions could be identified. Lesions were segmental in distribution, with affected arteries frequently adjacent to morphologically normal arteries. The endothelial cells were prominent, plump, and increased in number (hypertrophy and hyperplasia), with marked compression or complete occlusion of the lumen, often narrowing to an irregular sawtooth slit (Figures 3–6). The subintimal space between the endothelium and the internal elastic lamina (IEL) was infiltrated and expanded by variable (often numerous) plump spindloid cells in a variably loose to mature collagenous extracellular matrix (Figure 4). The media was variably expanded by increased numbers of concentrically arranged plump smooth muscle cells in a scant collagenous stroma, with mild-to-moderate expansion of the adventitia by rings of concentric loose fibrosis. Large numbers of eosinophils infiltrated the adventitia and surrounding parenchyma, as well as the intima and to a lesser extent the media (Figure 5). Eosinophils were occasionally degranulated. There was attenuation and fragmentation of the IEL as well (Figure 6), with complete loss of the IEL in advanced lesions. Fibrinoid necrosis, karyorrhectic debris, and lymphocytes were conspicuously absent from these arterial lesions.

Similar eosinophilic and occlusive arterial lesions were present in large, medium, and small pulmonary arteries of the lung, and medium and small arteries of the liver and spleen, with no associated infarctions (not shown). Lung arterial lesions appeared earlier than renal lesions and underwent evolution with duration of drug treatment and study length. Very early stage lesions, such as those observed in an acute study (euthanized 7 hr postantibiotic administration and after 3 hr pump run time) were notable for the remarkable edematous appearance, particularly within the media (Figure 7). Smooth muscle cells showed minimal hypertrophy or hyperplasia but are widely separated by abundant clear to faintly eosinophilic amorphous proteinaceous material. Endothelial cell hypertrophy and intimal and medial eosinophil infiltration were prominent. By 17 days, there was notable subintimal spindle cell infiltration with mild smooth muscle cell hypertrophy and hyperplasia (Figure 8). Adventitial eosinophil infiltration was also markedly increased. By 30 days, there was marked medial smooth muscle cell hyperplasia and hypertrophy (Figure 9). Bronchial arteries, as identified by the absence of a well-developed external elastic lamina, were unaffected.

By immunohistochemistry, subintimal spindle cells of the EOA lesions were positive for α-SMA (Figure 10) but negative for smoothelin, a specific marker of smooth muscle differentiation (Figure 11), indicating a myofibroblastic phenotype. By contrast, the plump hypertrophied spindle cells of the media were both α-SMA and smoothelin positive.

Demographic features of all the calves reviewed are presented in Table 1. Arterial lesions were observed in conjunction with pulsatile and nonpulsatile flow devices from four different manufacturers, as well as four unimplanted calves, indicating that the devices themselves were not associated with arterial lesion development. Arterial lesions have not been observed in routine diagnostic necropsies performed at this institution on nonstudy calves, euthanatized for humane considerations, which did not receive IV antibiotics (n = 12 during same 13-year period, data not shown). There was no significant difference in study duration between calves with and without EOA lesions (28.40
Study demographics and incidence of arterial lesions.

Note: EOA = eosinophilic occlusive arteritis; NE = not examined. Does not include renal infarcts in which lesions did not spatially cosegregate with arterial EOA lesions.
aOne calf also received intravenous (IV) cefazolin.
bThe short study calf (0.25 days) did not receive an aminoglycoside.
cOne unimplanted calf received only cefazolin (no aminoglycoside). Two calves also received IV ceftiofur and one calf also received IV ciprofloxacin.
dEOA lesions in spleen, rumen, and pancreas.
eOne calf also received IV ceftiofur, one calf also received IV ampicillin, and one calf received both ceftiofur and ampicillin. A third calf received IV ciprofloxacin.
fEOA lesions in liver and spleen.
gThe unimplanted calf received only 7 days IV ceftiofur (no cefazolin or aminoglycoside).
hOne calf also received IV ciprofloxacin.
iEOA lesions only present in liver.
All of the calves received IV administration of at least one cephalosporin. One of these calves received only a single IV dose of cefazolin (given 5 days prior to euthanasia) because it developed urticaria responsive to diphenhydramine and dexamethasone within 30 min of drug administration. All but one of the calves with EOA lesions received cephalosporins by bolus administration. This practice of rapid administration was discontinued for the most recent study, to no apparent effect. There was no significant difference in duration of cefazolin administration between calves with or without EOA lesions (7.06
Postantibiotic peripheral eosinophilia, defined as peripheral blood eosinophil count greater than 2,400/µL (Latimer, Mahaffey, and Prasse 2003), was present in three of the thirty-five calves with EOA lesions, and a fourth was nearly above the threshold (2,337/µL). In the implanted calves that did not develop peripheral eosinophilia, eosinophil counts did increase in the postoperative period following antibiotic administration (Figure 12). Peripheral eosinophilia was not observed in any calves in which EOA lesions were absent. Peak postantibiotic eosinophil count was significantly higher in calves with EOA lesions than in those without lesions (733.49

Peripheral blood eosinophil counts (per µL) for left ventricular assist device (LVAD)-implanted calves with eosinophilic and occlusive pulmonary arterial (EOA) lesions. Pre = preoperative day. PO = postoperative day. *Calf was started on intravenous (IV) ceftiofur on preoperative day 9 for a potential bacterial infection of the jugular catheter site. Kidney-only group indicates lung was not examined by histology.
Invasive systemic systolic, mean, and diastolic blood pressure values were recorded for implanted calves (Table 2 and Figure 13). Average systolic blood pressure was significantly higher (123.44
Invasive blood pressure recordings for left ventricular assist device (LVAD)-implanted calves.

Note: All values were recorded from the left internal mammary artery and reported in millimeter of mercury. Number in parentheses after group is number of observations. Standard deviation is given for each value. Kidney-only group indicates lung was not examined by histology.
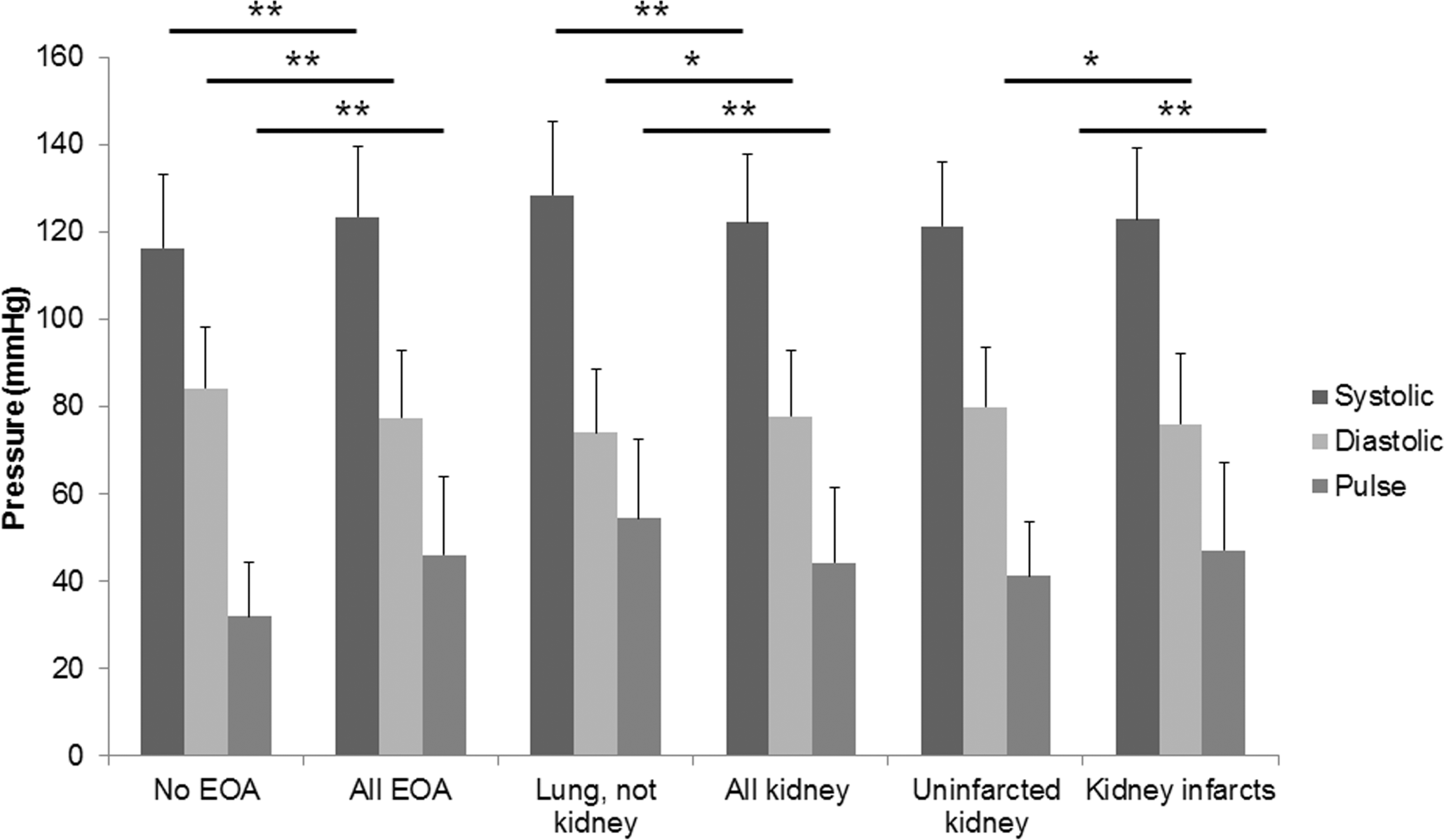
Mean invasive systemic blood pressure recordings for all left ventricular assist device (LVAD)-implanted calves as stratified by group. *p < .05. **p < .01.
Discussion
Eosinophilic and occlusive arterial lesions observed in these calves are morphologically identical to those reported previously limited to the pulmonary arteries of calves receiving long-term and high-dosage bolus IV antibiotics (Majeski and Fitts 1979). In that study, lesions were observed in calves receiving either penicillin/streptomycin (n = 10) or sodium cephalothin (n = 1) for 20 to 76 days. Lesions were not observed in five control calves that were chronically catheterized but did not receive antibiotic therapy. Unlike the previous study, lesions reported here were observed in the systemic arteries of the kidneys, liver, and spleen, were observed to initiate as soon as 7 hr after drug administration, and were associated with therapeutic doses of drugs given over shorter intervals. Possible explanations for the differences observed between the previous study and ours include animal breed, sex, and specific drugs used. While Majeski and Fitts report a peripheral eosinophilia accompanying lesion development, they provide neither a definition (cutoff) for eosinophilia nor do they report eosinophil counts except for one calf, in which the maximum value is approximately 1,500 cells/µL. Although only three calves in our study demonstrate an eosinophil count outside of the reference range, postantibiotic peripheral eosinophil counts were significantly higher in calves with than without EOA lesions.
Hypertension appears to play no role in lesion development. Although there were systemic blood pressure differences between many of the different groups of calves that did in fact reach statistical significance, these changes are unlikely to be biologically significant. The systolic and diastolic values observed for all groups were within the normal ranges reported previously for unanesthetized Holstein–Friesian calves (Weber et al. 1971) as well as for unimplanted control calves reported in other studies (Kihara et al. 2003). Further, the ranges of the values observed show significant overlap with each other, and the differences often amount to less than 10 mmHg. Finally, many of the differences observed are difficult to reconcile from a pathogenesis perspective. For instance, it is difficult to explain mechanistically why a relatively higher systemic systolic blood pressure would favor the development of pulmonary EOA lesions while sparing the kidney.
While differences in systemic systolic, mean, and diastolic blood pressure between groups were inconsistent and of limited magnitude, the presence and distribution of lesions correlated with increased rather than diminished pulse pressures. Two previous studies have attributed the presence of similar proliferative arterial lesions in the kidneys of LVAD-implanted calves specifically to the use of nonpulsatile continuous-flow type devices. Kihara et al. report similar lesions to those described here, including mural infiltrates of eosinophils, in Jersey calves, and note a positive relationship between decreased systolic and increased diastolic pressures and lesion development (Kihara et al. 2003). Ootaki et al. report intimal, medial, and adventitial hyperplasia of the renal arcuate and interlobular arteries, with mononuclear inflammatory cell infiltration of the adventitia only, in Holstein–Friesians (Ootaki et al. 2008). Neither study reports pulmonary nor other organ lesions. Both studies conclude that reduced pulsatility, as measured by reduced pulse pressure and pulsatility index, is responsible for lesion development. In the present study, lesions were present in animals with pulsatile, continuous, and mixed flow devices, as well as in unimplanted calves. Further, lesions were noted to develop temporally first in the pulmonary arteries, despite device routing such that pump outflow is to the descending thoracic aorta only. Although pulsatility index was not examined, animals with EOA lesions in this study in fact had significantly higher pulse pressures than unaffected calves. The pulse pressures recorded in the animals in this study with EOA lesions (46.01
The exact pathogenesis of these lesions is not known. The presence of eosinophils, occasionally degranulated, in conjunction with a loose edematous stroma consistent with a release of vasoactive amines, is highly suggestive of a hypersensitivity reaction, as is the clinically documented urticaria in one calf following administration of a single dose of cefazolin. Because there was no apparent relationship between duration of antibiotic therapy and development of lesions, this appears to be an idiopathic reaction, consistent with an allergy. Eosinophils are well-described inducers of endothelial cell activation (Eustace, Nadasdy, and Choi 1999). Concentric hypertrophy and fibrosis may develop secondarily to turbulent flow and localized hypertension in the affected vessels, or following tissue destruction mediated by eosinophils. Lesions share many features with those observed in dogs and cats infected with Dirofilaria immitis, in which the immune response to the nematode parasite and its bacterial endosymbionts plays a critical role in lesion development (Simon et al. 2007; McCracken and Patton 1993; Maxie and Robinson 2007). In humans, eosinophilic vasculitis is prominent in Churg Strauss syndrome, a protean disease of unknown etiology associated with allergic reactions, including atopy and asthma, as well as administration of leukotriene receptor antagonists (Eustace, Nadasdy, and Choi 1999; Currie, McKinlay, and Kerr 2008). Although Churg Strauss is associated with peripheral eosinophilia and can have significant renal involvement (the second most common cause of death), arteritis is prominently necrotizing. While eosinophils can be a prominent feature of the segmental obliterative arteritis of Buerger’s disease, the proliferation is luminal to the intact IEL, which is commonly reduplicated (Lie and Michet 1988; Kim et al. 2000). Arterial proliferative lesions, limited to the lungs and without eosinophils, have been previously reported in calves with idiopathic pulmonary hypertension (Pringle et al. 1991). Consistent with hypertensive lesions in other species, there was fibrinoid necrosis of the vessel walls, a feature absent in the lesions reported here. Systemic proliferative arterial lesions have also been reported in adult Holstein–Friesians with cardiomyopathy (Bradley et al. 1991). The hearts in the animals reported here demonstrated no myopathic changes.
A constellation of pulmonary arterial lesions morphologically similar to those reported here has also been described in rats receiving long-term IV infusion of large volumes of isotonic saline (Morton et al. 1997). The authors suggest that hemodynamic events (increased or turbulent flow or increased arterial pressure) may be responsible, but such an explanation seems unlikely, given the relatively small volumes (5 mL) bolused to calves weighing over 100 kg in our study. Further, switching from bolus administration to slow infusion in the most recent calf studied did not prevent lesion development. Significant differences from lesions described herein include the absence of luminal occlusion or fragmentation of the IEL in rats.
Adverse drug events resulting from immune-mediated reactions to cephalosporins are well documented. These include drug reaction with eosinophilia and systemic symptoms (DRESS) and drug-induced acute interstitial nephritis (AIN; Perazella and Markowitz 2010; Picard et al. 2010; Cacoub et al. 2011). Eosinophilia is a classic finding in both syndromes, although renal involvement is interstitial or tubulointerstitial with prominent lymphocytic infiltrate, features absent in these cases. DRESS can also occasionally cause interstitial pneumonia. Cutaneous rashes and fever are prominent features of DRESS and frequent in AIN, while arteritis is not a feature of either syndrome. Finally, T lymphocytes, particularly CD8+, are prominent features of DRESS and AIN but were notably absent in these calves.
In this study, we have shown that IV administration of therapeutic doses of cephalosporin antibiotics in calves, with or without IV aminoglycosides, can lead to eosinophilic occlusive arteritis lesions in the systemic as well as pulmonary circulation. Further, lesions affecting the end arteries of the kidney may result in cortical infarctions. This can be a significant confounder in the design and interpretation of medical device studies in calves. Further studies to elucidate the mechanism and pathogenesis of these unusual idiopathic lesions are necessary.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research supported by National Institutes of Health/National Heart, Lung, and Blood Institute grants 5 RO1 HL081119-04 and 2 RO1 HL60276-10.
Acknowledgments
The authors thank Bradley Doxtater for gross photography, and Weifang Lin and Ellen Mullady for histologic specimen preparation. Drs. Ronald P. Wilson and Elizabeth Carney as well as numerous laboratory animal medicine residents and calf sitters provided clinical care for study animals. Dr. Richard Zaino provided invaluable critical review of the article.