
Abstract
The identification of neurotoxicity is a critical issue in drug development, and toxicologic pathologists play an important role in this effort. Neuropathology is a specialized area of toxicologic pathology in which a substantial number of nonroutine techniques and methods have been developed, and there are undoubtedly many instances in which these specialized procedures have helped characterize a neuropathologic lesion. Routine histopathologic methods employed in general toxicologic pathology studies are needed to identify the complete range of possible neuropathologic changes; once identified, many of these changes can be better defined by specialized techniques, such as immunohistochemistry, to confirm cell types involved. Sometimes, when neurotoxicity is expected, dedicated studies can be designed a priori and optimized for detection of the anticipated effects. However, when neurotoxicity arises unexpectedly or there is uncertainty around the potential for neurotoxicity, the decision of what to do can become more difficult. Recommendations to go ahead and perform the “optimal” study design that would accommodate all the potentially useful specialized techniques for characterizing a neuropathologic change are sometimes not practical and can be unnecessary and potentially detrimental to other end points in the study. In addition, there is not always agreement on when specialized techniques would be required and which ones should be used when necessary. Two techniques in particular that are commonly recommended to help facilitate the detection of neuropathologic lesions are perfusion fixation and the Fluoro-Jade stain.
Perfusion fixation has been used as a technique in neuroscience research laboratories for years, and it is often recommended for generating optimal tissue sections for microscopic examination. Although this technique might be easy to perform in the research setting, where the primary goal is to evaluate only neural tissues, in a general toxicity setting, this procedure can become significantly more challenging to implement. Perfusion fixation is not always technically easy to perform, particularly when done in large animal species or in large numbers of rodents, and failure to perform this procedure correctly can potentially result in tissue sections of poorer quality than those that are routinely fixed by immersion. For these reasons, incorporation of perfusion fixation into a study design should not be taken lightly, particularly if it is to be incorporated into a general toxicity study in which there may be an impact on other end points being measured. If properly performed, perfusion fixation can result in more rapid fixation of the tissue as compared to immersion fixation techniques, and this certainly would be a desirable outcome if the goal is to get optimal sections for electron microscopy, although how much is really gained if the primary goal is to identify the presence or absence of pathology by routine light microscopy? Is immersion fixation sufficient when the desire is to generate samples suitable for diagnostic purposes? Despite the many questions, the perception that perfusion fixation is best is dogma within the neuroscience research community, and it is also becoming a more frequent recommendation for general toxicity studies without any real supporting evidence that such a technique is necessary. Are there certain lesions that would be potentially undetectable without the aid of perfusion fixation? To my knowledge, there have been no such instances reported in the literature. One advantage often cited in support for perfusion fixation is to help reduce the level of artifactual change, which is easily induced in neural tissues and may impair detection of treatment-related lesions. Certainly this may be an advantage, although it should also be noted that perfusion fixation does not completely eliminate this problem, and if not done properly, it can even lead to a level of artifactual change that is no better or even worse than is seen with immersion fixation, particularly where immersion fixation is carried out by skilled technical staff with minimal tissue handling and appropriate fixation procedures (adequate volume of fixative, appropriate changes of fixative, etc.). Since these aforementioned variables will have a major influence on the level of artifact in histological sections, the utility of perfusion fixation should be addressed on a case-by-case basis by the laboratory in which the procedure will be carried out.
Overall, the question is whether or not the additional effort and technical skill required to do perfusion fixation is worth the small gains this technique might provide when the goal is to evaluate neural tissues at the light microscopic level for diagnostic purposes as part of risk assessment. There may be specific examples that show perfusion fixation makes sense, and these examples certainly need to be brought forward for further discussion; however, in the vast majority of cases it is likely that routine immersion fixation would be perfectly adequate to identify all the same lesions that would be identified in perfusion-fixed tissue. The last thing we want to create is a false perception that a technique such as perfusion fixation is a requirement whenever neurotoxicity is anticipated; however, this perception seems to be what is developing.
A similar scenario sometimes develops when there is a concern for potential neurodegeneration. Although light microscopy using routine hematoxylin and eosin (H&E)–stained sections is able to detect necrotic neurons, the inclusion of a Fluoro-Jade (FJ) stain is sometimes recommended to improve the sensitivity of detection. Numerous publications have supported the conclusion that the FJ stain does highlight the same necrotic neurons identified in H&E sections, and it also has the advantage of highlighting degenerate neuronal processes and can sometimes reveal a degenerative process to be more extensive than would be indicated by H&E alone. In addition, the FJ stain has the potential advantage of allowing for a more rapid screening of sections for degenerative effects as compared to a routine H&E evaluation. However, since a routine H&E evaluation will be needed in a general toxicology study anyway (neurodegeneration is not the only neurotoxicological end point being evaluated), the benefit of FJ is less clear. Although the FJ stain has been promoted as being a more sensitive and definitive marker of neuronal degeneration, it appears to be without any apparent efforts to show that it is actually any better than the results obtained by a trained toxicologic pathologist using routine H&E–stained sections. Indeed, much of its popularity in research laboratories may stem from its utility as a simple means of allowing identification of necrotic neurons by nonpathologist technical staff and/or image analysis software. The FJ stain was originally validated against H&E and suppressed silver–stained sections (Schmued et al. 1997), although the goal was to confirm that FJ was able to detect the same degenerative process highlighted by the other staining methods and not to identify instances in which FJ may be able to detect a lesion missed by the other staining methods. Since that time, it has been suggested that FJ can aid in differentiating peracute neuronal degeneration from dark neuron artifact, and this may be the case, although even this capability does not provide justification for including FJ as a standard end point for all studies. First, how often does peracute neuronal degeneration occur without any clinical effects indicative of neurotoxicity? Second, because development of a compound typically involves a series of increasingly longer-duration studies, the rare instance of a clinically and microscopically inapparent peracute event in short-term studies would most likely become apparent in routine longer-term studies or at least provide some indication that additional methods should be implemented. Nonetheless, there is a growing perception among some people, typically those outside toxicologic pathology, that there are instances in which the FJ stain should be a requirement over or at least used concurrently with H&E–stained slides. The development of this perception is surprising, considering the lack of understanding regarding how this stain actually works or even what the potential disadvantages of this stain might be, particularly whether or not this stain ever results in false positives. In fact, I suspect that the default course of action for many toxicologic pathologists suspecting a false positive FJ stain would be to go back to the H&E for confirmation. Furthermore, even routine H&E sections viewed under a fluorescent microscope using a FITC filter (Figure 1 ) can be used for confirmation when necessary, considering that H&E–stained necrotic neurons display a level of autofluorescence that is quite similar to what can be seen with the FJ stain. As with perfusion fixation, such instances of the FJ stain providing superior results to standard methods may exist, but if so, these examples really need to be brought forward for discussion and publication. Few will question the potential advantages of the FJ stain when used appropriately, but it should not be promoted as a necessity for diagnostic purposes until proven that it really is superior to currently used methods.
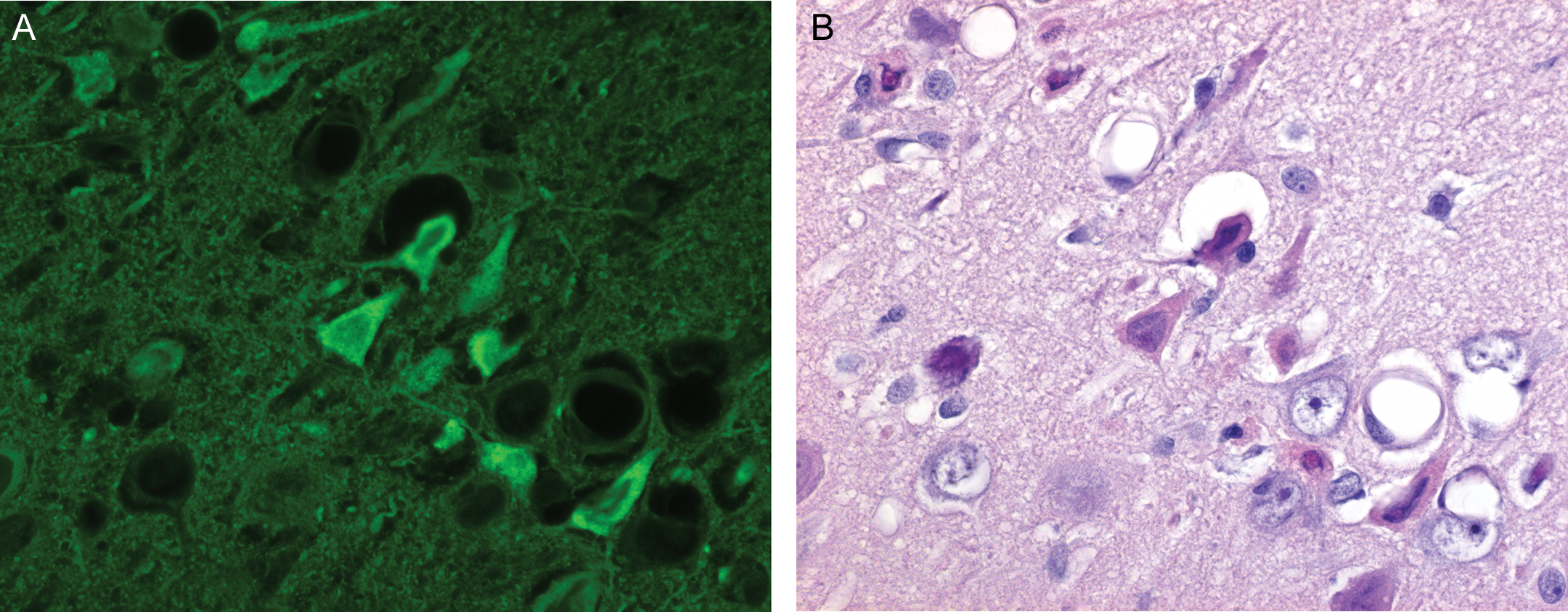
Comparison of (A) fluorescent microscopy and (B) routine light microscopy of the same hematoxylin and eosin stained section of brain illustrating necrotic neurons (400×).
Overall, these two examples highlight the larger issue that centers on the perception by groups outside the toxicologic pathology community that believe some of these specialized techniques are requirements for a thorough neuropathologic evaluation. When considering this issue, it is important to make a clear distinction between detection of a lesion and characterization of a lesion. Currently, this distinction is not well defined within the neuropathology community, and it is leading to misperceptions outside the discipline. If there are deficiencies in our standard methods and some of these supplementary techniques are required to help fill the gaps, then these issues need to be brought forward and discussed in detail. At this time, I do not feel there is a strong opinion among toxicologic pathologists that the standard methods of evaluation are inadequate for screening purposes, although it does feel like this opinion is increasingly at odds with the external environment, including regulators. Additional work and specialized procedures can always be added when necessary, and they should be. But they should also not be indiscriminately applied to any study just because of uncertainty over what is necessary, particularly when the pressure to do this additional work is being applied by those without the requisite knowledge to logically do so.