
Abstract
Substance use disorders (SUD) are often attributed to upbringing and family dynamics, an assumption that places undue responsibility on parents. Mothers may be particularly susceptible to blame due to traditional gender norms around parenting. This qualitative study explored public perceptions of maternal responsibility and shame in the context of adolescent SUD. Participants were 80 Canadian adults recruited during a larger online survey. After reading a vignette describing a mother and her adolescent child with cannabis use disorder (CUD), participants answered two open-ended prompts exploring perceptions of maternal responsibility and shame. An inductive thematic analysis revealed mixed and complex opinions regarding maternal responsibility, with themes highlighting the nature and etiology of addiction, the mother’s role in prevention and recovery, societal tendencies to parent blame, and the detrimental effects of shame and stigma. The current findings highlight the need to challenge public beliefs regarding SUD to reduce parental blame and stigmatization.
Keywords
Introduction
Substance use disorders (SUD) are a prevalent health concern in Canada with diverse health and social outcomes. Statistics Canada (2015) reported the Canadian lifetime prevalence of SUD at 21%; however, this estimate may be conservative as many people with SUD avoid disclosing their condition due to fear of judgement and discrimination (Choi et al., 2014; Keyes et al., 2010). Stigma, which describes a collection of negative perceptions, attitudes, and behaviours toward a particular societal group, has adverse consequences for people with SUD, including lower rates of treatment-seeking and treatment adherence (Baker et al., 2022; Volkow et al., 2021). Parents of individuals with SUD may be stigmatized by association, a phenomenon known as courtesy stigma (Goffman, 1963); further, conceptualizations of the mother as the primary caregiver may frame mothers as particularly responsible for a child’s SUD, resulting in increased blame and stigmatization (Smith & Estefan, 2014; St-Amant & Schwind, 2022).
Public Stigma Toward SUD
Research consistently identifies SUD as more stigmatized than other mental health conditions and developmental disorders (Corrigan et al., 2006; Kulesza, 2013; Miller et al., 2022; van Boekel et al., 2013). According to Weiner’s (1995) attribution model of stigma, an individual considered more responsible for their condition is more likely to garner negative emotional responses and discrimination from the public. This concept is supported in the literature, which indicates that people who are perceived as more responsible for a mental health condition are more highly stigmatized (Corrigan et al., 2003; Martin et al., 2000; van Boekel et al., 2013). As such, SUD may be particularly stigmatized because society assigns individuals with SUD more personal responsibility (Smith & Estefan, 2014). Corrigan et al. (2006) reported that regarding a loved one’s SUD, parents were significantly more stigmatized than a sibling or child. In line with the attribution model, parents may be more stigmatized than other family members as they are seen as more responsible for the child’s behaviour and, consequently, the onset of SUD.
Parental Stigma and Blame
Parents are often blamed for the development of SUD, which may be attributed to poor parenting and unhealthy family dynamics (Corrigan & Miller, 2004; Flensburg et al., 2022). Society positions the parent as the driving force determining the successes and failures of a child; as such, parents are judged as responsible for their child’s choice to use substances and the onset of any problematic patterns of use (Smith & Estefan, 2014). Perceptions of parental responsibility are particularly strong when SUD occurs during adolescence, as parents are expected to exert a high degree of supervision and influence over their child’s behaviours at this developmental stage (Choate, 2015; Smith & Estefan, 2014). Holding the parents as solely responsible for their child’s SUD is short-sighted, as it ignores both the agency of the individual and the multitude of biological and social factors that together contribute to SUD (Nawi et al., 2021; Somani & Meghani, 2016).
Maternal Stigma and Blame
Mother blame refers to the societal tendency to view mothers as solely responsible for their child’s development, behaviour, and well-being (Jackson & Mannix, 2004). Mother blame is a long-standing and pervasive issue; in the past, mothers have been blamed for a wide range of outcomes related to their children, including economic attainment, justice involvement, neurodevelopmental disorders, and mental health conditions (Ladd-Taylor & Umansky, 1998). This tendency toward maternal blame may be rooted in sexist attitudes and gendered perceptions of the mother as the primary caregiver, a notion which is evident in multiple domains (Jackson & Mannix, 2004). Prominent theories of child development (e.g., cognitive developmental theory, learning theory, and attachment theory) have often highlighted the mother as the principal caregiver and, consequently, most responsible for the child’s healthy development (Jackson & Mannix, 2004; Phares, 1992). Public perceptions of mothers as the main caregivers are also apparent; Finley et al. (2008) found that mothers were perceived as more involved than fathers in all parenting roles (e.g. emotional development, social development, and ethical and moral responsibility) except for financial support, emphasizing the gendered nature of parenting expectations.
Maternal blame and stigma have been recorded toward mothers of children with a variety of health concerns. Research has highlighted that mothers of children with obesity, attention-deficit hyperactivity disorder (ADHD), special educational needs, schizophrenia, and autism spectrum disorder (ASD) often face stigmatization and blame for their child’s condition (Charbonnier et al., 2018; Gorlick et al., 2021; Milliken, 2001; Milliken & Rodney, 2003; Uba & Nwoga, 2016, 2016zet al., 2019). In turn, mothers often report experiencing distress and internal criticisms about their role as a parent (Charbonnier et al., 2018; Gorlick et al., 2021). Further, Gilson et al. (2021) indicate that mothers may face substantial barriers when trying to access personal, professional, and system-level support. This is especially relevant as mothers are often assigned the responsibility of monitoring their child’s health and seeking adequate health care for their child (Blum, 2007; Jackson & Mannix, 2004).
Research suggests that mothers are viewed as particularly responsible for a child’s SUD (Smith & Estefan, 2014; St-Amant & Schwind, 2022). Notably, addiction has all too often been conceptualized as a moral failure, while instilling morality has been described as a mother’s responsibility (Henderson & Dressler, 2017; Smith & Estefan, 2014). In qualitative research on mothers of children with SUD, the themes of blame, shame, and stigma are common. Mothers have reported feeling blamed by family, friends, and healthcare professionals for their child’s SUD, which caused feelings of shame and led them to distance themselves from others (Choate, 2015; Flensburg et al., 2022). Choate (2011) notes that the shame and guilt placed upon parents restrict them from reaching out to friends and family for support and are associated with negative family dynamics such as marital issues and lack of family communication. Mothers of children with SUD often engage with a range of health and social services as they attempt to support their children with their substance use. Mothers have reported that experiencing stigma, blame, and judgement from healthcare professionals has made them reluctant to access guidance and assistance, leading to feelings of abandonment (Vincent, 2010). Notably, experiencing public blame and stigma is associated with negative health and social outcomes and can prevent parents from seeking help for themselves or their child (McCann & Lubman, 2018; O’Shay-Wallace, 2020).
Adolescent Cannabis Use and Cannabis Use Disorder
As of 2023, non-medical cannabis use is legal in Canada and 23 states in the United States (Cannabis Act, 2018; National Conference of State Legislatures, 2023). Despite intentions to decrease youth access, cannabis use is still common among adolescents; in 2022, 42.8% of Canadian adolescents aged 16–19 reported using cannabis within the past 12 months (Health Canada, 2023). This statistic is concerning given that adolescents who use cannabis face an increased risk of negative health outcomes, including developing cannabis use disorder (CUD; Hall, 2015). CUD is characterized by a pattern of cannabis use that causes distress and/or impairment of functioning, increased use and cravings, tolerance and withdrawal, among other health outcomes (American Psychiatric Association, 2022). The results of a large-scale national survey of Canadian cannabis users (Health Canada, 2023) indicated that 4.7% of respondents currently met the criteria for psychological dependence on cannabis. Notably, this rate was higher among both adolescents and those whose cannabis use had started during adolescence.
In a recent qualitative study, Haines-Saah et al. (2019) explored the experiences of 16 Canadian parents (12 mothers) whose adolescent children use cannabis. Some parents described the pressure they felt to monitor their child’s activity and prevent substance use, while others noted that stigma discouraged them from disclosing their adolescent’s cannabis use or seeking social or professional support. Parents often blamed themselves for the onset of their child’s cannabis use, seemingly overlooking the multitude of other factors influencing adolescent substance use. These findings highlight the internalized blame and shame experienced by parents affected by a child’s substance use and the need to challenge the narrative that youth substance use is the fault of the parent.
In line with the attribution model of stigma (Weiner, 1995), parents may be more heavily stigmatized than other family members, as they are perceived as more responsible for their child’s behaviour and the onset of their CUD (Corrigan et al., 2006). Using an experimental vignette design, Downey et al. (2025) assessed courtesy stigma toward the parent of an adolescent child with CUD, finding that participants reported more stigmatizing attitudes toward the parent when described as a mother than a father. Given that mothers are frequently viewed as the primary caregivers (Smith & Estefan, 2014; St-Amant & Schwind, 2022), they may be particularly vulnerable to blame for their child’s substance use, due to greater attributions of responsibility. Additionally, existing literature conveys that mothers in these positions report feeling stigmatized for their child’s condition (Charbonnier et al., 2018; Gorlick et al., 2021). These considerations formed the basis for the present study.
The Current Study
In qualitative research, mothers have reported experiencing blame and stigmatization for their child’s SUD (Choate, 2015; Smith & Estefan, 2014; St-Amant & Schwind, 2022); public perspectives of maternal responsibility within this context are less established. This qualitative study expanded the literature by exploring public perceptions of maternal responsibility and shame regarding a child’s SUD. Findings may offer a more detailed understanding of the rationalizations that drive public perceptions of maternal blame in the context of SUD.
Method
Research Design
This study is part of a larger survey study examining the effect of language and parent gender on courtesy stigma toward parents of adolescents with CUD. The study received ethical approval from the Interdisciplinary Committee on Ethics in Human Research at Memorial University of Newfoundland (MUN; ID #20240404-SC). The survey was conducted online on Qualtrics. After providing written informed consent, participants read a vignette describing the relationship between a parent and their adolescent child (Jamie) with CUD. The vignette described how Jamie’s CUD had progressed, how the relationship between the parent and Jamie had changed as a result, and the parent’s efforts to support Jamie. Participants read one of four randomly assigned versions of the vignette, which varied by the language used to describe the parent (deficit-based versus neutral) and the parent’s gender (mother versus father). Deficit-based and neutral language was conceptualized based on prior research (Ashford et al., 2019; Pasman et al., 2023; Wilkens & Foote, 2019) and direct consultation with parents of children with CUD. Participants completed quantitative measures of stigma toward the parent, a demographic questionnaire, and two open-ended questions, which formed the basis for the current analyses.
Vignettes are widely used in research aimed at understanding public attitudes toward SUD and mental health conditions (Link et al., 2004). Vignettes offer participants situational context, enhancing experimental realism and allowing researchers to assess participants’ intentions, attitudes, and behaviours (Aguinis & Bradley, 2014; Link et al., 2004). Vignette-based methods have also been employed in recent stigma research (Al Dharman et al., 2022; Manago & Mize, 2024). While most frequently employed in quantitative research, vignettes are also valuable in qualitative explorations of attitudes and perceptions of complex health issues (Jackson et al., 2015). By presenting a well-defined scenario, vignettes enable participants to express their views on a phenomenon within a specific context, rather than relying on abstract or generalized perceptions of a particular population; within qualitative research, this allows for the collection of richer, more detailed responses (Gray et al., 2017).
The current study analysed qualitative data collected from a subset of survey participants, namely, those who read the vignette (see Supplemental File) describing a mother (Carole) using deficit-based language. Data from this condition were chosen for analysis as it was expected to elicit more stigmatizing attitudes based on prior findings on maternal blame (Jackson & Mannix, 2004; Smith & Estefan, 2014) and the effect of language on stigma (Ashford et al., 2019; Kelly & Westerhoff, 2010). We analysed qualitative data from a single vignette condition to control for contextual differences that may have existed between conditions.
Participants
Demographic Characteristics of Participants
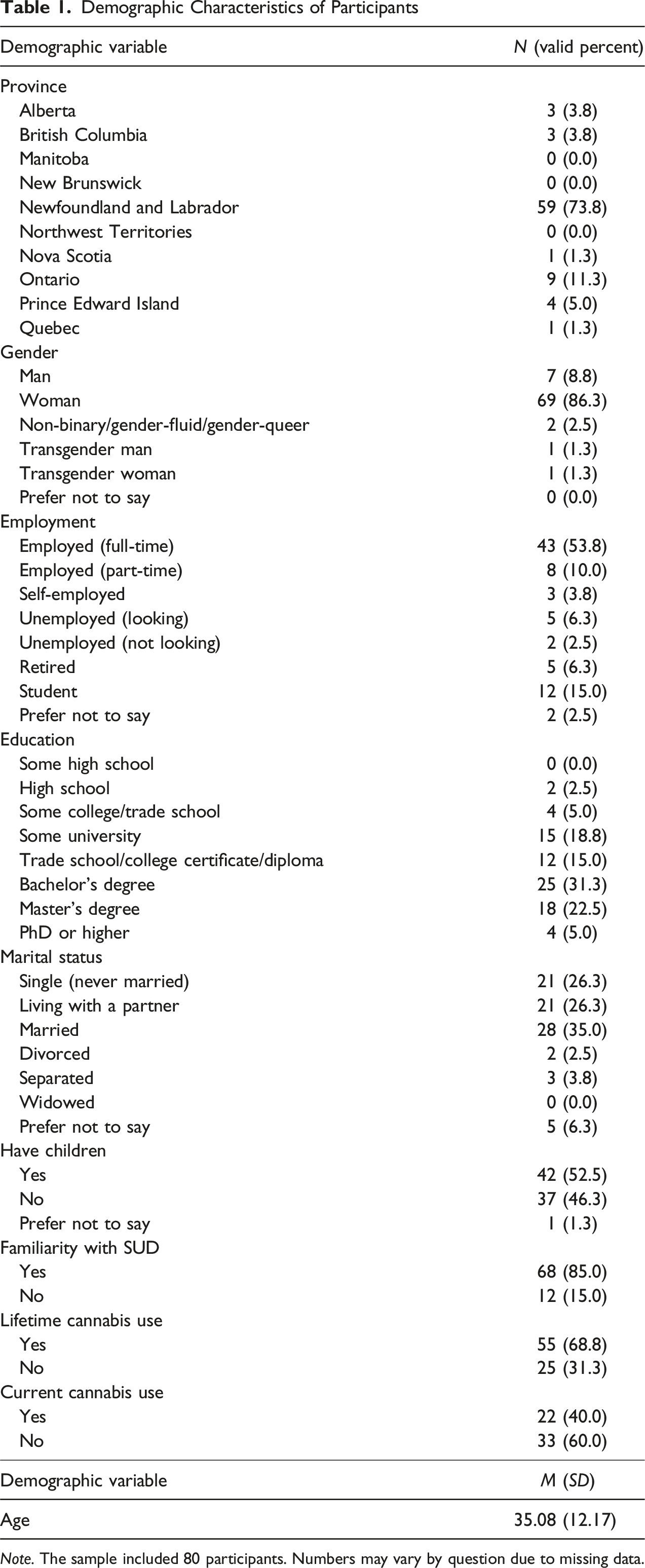
Note. The sample included 80 participants. Numbers may vary by question due to missing data.
Materials
Qualitative data comprised responses to two open-ended survey questions that explored perceptions toward Carole, the mother depicted in the vignette: 1. Do you think that Carole (the mother) is responsible for Jamie’s (her child’s) cannabis use disorder? Why or why not? 2. Do you think Carole (the mother) should feel ashamed because of Jamie’s (her child’s) cannabis use disorder? Why or why not?
Qualitative Analysis
The data were analysed using a thematic analysis approach (Braun & Clarke, 2006). We used an inductive, ‘data-driven’ approach during analysis, deriving themes from the data rather than organizing the text by a pre-existing schema. Data were analysed manually in Microsoft Excel by three graduate students, T.G.J.A., B.B.H., and I.D.M.; all coders had prior experience with qualitative research methods, as did M.K.D., who oversaw the analysis process. The coders first read through the data to familiarize themselves with the content, making notes of initial thoughts and ideas throughout; next, each coder went through the data line by line, generating initial codes. Initial codes were compared, and differences were resolved through discussion and group consensus. The agreed-upon codes were compiled into a codebook, and the dataset was re-coded according to these parameters. Given the extensive overlap of codes in the responses to the two open-ended questions, the data were combined and analysed together. Codes of similar meaning were then organized into initial themes, which were revised through an iterative review process, resulting in the final themes. We followed the guidelines for inter-coder reliability by Cofie et al. (2022) to maximize coding consistency and validity of the findings. The guidelines involved having multiple coders, including at least one with prior qualitative analysis experience, employing the same analysis framework across coders, using a codebook, and establishing final coding through discussion and collective agreement.
Results
The results outline perceptions of maternal responsibility and shame regarding adolescent CUD. Some participants spoke of maternal responsibility and shame within the context of the vignette, referring specifically to the mother, Carole, and her child, Jamie; others discussed these concepts in a broader sense, highlighting the complex reality of substance use and the influence of societal structures. While the vignette described Jamie with gender-neutral pronouns, many participants assumed the adolescent’s gender and referred to them accordingly in responses. Five major themes, each with several sub-themes, emerged from the data: (1) The Mother is Responsible, (2) The Mother is Not Responsible, (3) Ambivalence About Maternal Responsibility, (4) Maternal Shame, and (5) The Mother’s Perspective.
The Mother is Responsible
About half of the participants perceived Carole as responsible for her child’s CUD in some capacity. Within perceptions of maternal responsibility, three sub-themes emerged: (i) The Mother as “Enabler”, (ii) Failing to Intervene, and (iii) Neglecting Parental Duties.
The Mother as “Enabler”
A common sentiment was that Carole’s actions allowed or even encouraged Jamie’s CUD to continue. The mother was frequently described as “enabling” her child. Participants questioned Carole’s tolerance of cannabis use in the home, stating that “allowing easy access to cannabis by allowing Jamie to smoke at home is not going to make her want to stop” (P61). It was suggested that the mother provided her child with too much support, particularly in the form of household chores and financial support. One participant stated, “I do feel she facilitates Jamie to continue in his disorder by providing excessive support that Jamie should be challenged to take responsibility for” (P43). Some participants perceived the mother’s parenting style as permissive of continued substance use, leading to judgements of responsibility: “I think that Carole enables her daughter to continue using cannabis, so at this point, she is responsible for the problem” (P76).
Failing to Intervene
The mother was frequently blamed for failing to step in and prevent her child’s CUD from progressing; it was suggested that Carole should have recognized the warning signs, intervened earlier, or placed Jamie in rehab. One participant said: The mother should have been able to identify the issue when Jamie was younger and put an end to it then. It shows she was using a hands-off parenting approach. If she had paid more attention, the usage could have stopped at an earlier age (P50).
Further, the mother was tasked with uncovering the underlying cause of Jamie’s disorder, with one participant stating, “she could be trying to find out why her daughter is turning to a substance in the first place” (P61). Some participants attributed Jamie’s CUD to inadequate parental supervision. It was suggested that “if the mother had monitored her child’s daily activities, she would have been able to stop this behaviour before it got worse” (P49).
Parental Duties
Discussions of maternal responsibility often focused on the mother’s failure to fulfil her parental duties. Participants envisioned a good parent as both role model and teacher: “parents play an important role in shaping their children’s behaviour. Parents have the responsibility to supervise and educate them to make correct decisions” (P29). It was suggested that Carole had failed in this regard, with one participant remarking, “Carole didn’t educate Jamie or insert herself enough in his life” (P78). The mother was also positioned as a negative influence, with one participant suggesting that Carole “showed Jamie that regular cannabis use was okay and normal during her childhood” (P66), while another surmised that Carole was supplying Jamie with cannabis. Participants spoke of Carole’s failure to maintain boundaries with her child, identifying a “complete lack of control or authority” (P33) and the need to establish and enforce rules. It was also emphasized that as the mother, Carole was responsible for getting Jamie professional help: “As Jamie is technically a child, it is Carole’s responsibility to get Jamie the help they need” (P15).
The Mother is Not Responsible
Many participants expressed the belief that the mother was not responsible for her child’s CUD, highlighting numerous other contributing factors that should be considered. These perspectives generated four subthemes, namely, (i) The Nature of Addiction, (ii) Risk Factors, (iii) Personal Responsibility, and (iv) Mitigating Harms.
The Nature of Addiction
When asked about the mother’s responsibility, participants often spoke of the nature of addiction as a medical illness. One participant mentioned that CUD “is an addiction, and like any other illness, there are aspects that are out of the individual’s control” (P22). There was also discussion of how addiction is not controllable or preventable but rather “can happen to anyone” (P30). Speaking to the nature of addiction, one participant said, “CUD does not discriminate. Anyone can develop a CUD and it is not the fault of the mother” (P23).
Risk Factors
Participants often referred to the numerous factors that influence the likelihood of developing SUD. One participant said, “substance use disorders are complex, and there are multiple contributing factors including societal and peer influences, personal, genetic and psychological factors” (P45). Personal risk factors, such as an individual’s childhood, exposure to traumatic events, and mental health, were also discussed. It was suggested that Jamie’s CUD “may be a coping mechanism to deal with underlying issues” (P53). Social influence, particularly that of peers, was seen as a significant contributor to adolescent behaviour: “teens spend a lot of time with their peers, and social influence and pressure can be hard for teens” (P41). The impact of cannabis legalization in Canada was also discussed, with one participant remarking, “the government has made it much easier for youth to access marijuana by legalizing it” (P51). Additionally, it was highlighted that CUD does not develop for a singular reason but rather due to a series of factors: “There are too many variables to place blame on one person here. Micro decisions over time led to this bigger outcome” (P74).
Personal Responsibility
When discussing CUD, participants often spoke of Jamie’s personal responsibility. One participant said, “While Carole is the parent and has influence over her child’s life, Jamie is old enough to make his own decisions… At the end of the day, Carole is not responsible for Jamie’s choices” (P56). Participants acknowledged that there is a limit to parents’ control over their children’s actions, particularly during adolescence; one said, “mothers try to set a positive example, but it can be a struggle to get teens to listen” (P41). Another stated, “I think kids are going to find cannabis regardless of what their parents do” (P26). Discussions of personal accountability conveyed the importance of willingness to change, highlighting that a parent cannot make their child seek help if they are not ready: “Jamie is responsible for managing their disease, not Carole. Carole can offer help, but Jamie must choose to accept it” (P70).
Mitigating Harms
It was frequently suggested that Carole’s parenting approach served to minimize the damages caused by Jamie’s CUD. By supporting Jamie, Carole was seen as preserving the parent–child relationship and the unity of the family. One participant said, “Carole is continuing to love and care for her son, and even though she may voice her disapproval, giving him ultimatums will only push him away from her” (P68). Another participant emphasized the importance of continued parental support, suggesting that cutting Jamie off “would likely significantly impact their relationship and could lead to the deterioration of the family” (P4). It was also suggested that Carole was promoting the safety of her child and reducing harms: “By allowing Jamie to consume cannabis in her home, Carole is removing the desire for Jamie to hide the cannabis use and potentially put herself into dangerous situations” (P28).
Ambivalence About Maternal Responsibility
A significant proportion of participants expressed mixed opinions regarding maternal responsibility. Some suggested that the mother was partially responsible: “Carole is by no means solely responsible for Jamie’s cannabis use disorder; however, lack of discipline, enabling, and lack of consequences only encourage Jamie to use” (P24). A common attitude was that while the mother was not responsible for the development of her child’s CUD, she was responsible for the continuation of the disorder: I don’t feel [Carole] is responsible for Jamie’s cannabis use disorder developing, as there are a wide variety of reasons he may have begun using. However, I do think she bears some responsibility for allowing it to continue and happen in her home. She also holds some responsibility for enabling the behaviour and making it “easier” for Jamie to continue using (P6).
Other participants gave contradictory statements on the mother’s responsibility. When asked if Carole was responsible for her child’s CUD, one participant said, “Yes and no. Yes, because perhaps she didn’t educate Jamie or insert herself enough into his life. And no, because parenting is hard and there will be things that are out of your control” (P78).
Maternal Shame
Very few participants stated that the mother should be ashamed because of Jamie’s CUD; those few who endorsed this opinion felt that the mother had not done enough to help her child. One participant suggested that some feeling of shame was needed, namely, “enough to make an active change and continue to seek help” (P50). However, the majority of participants indicated that the mother should not feel ashamed. Three sub-themes were noted: (i) Shame is Unproductive, (ii) Stigma Toward Substance Use Disorders, and (iii) Parental Blame.
Shame is Unproductive
Participants expressed the belief that shame regarding a loved one’s SUD is not constructive and only worsens outcomes. It was noted that shame alienates people: “shame doesn’t help anyone find solutions. It just causes people to hide” (P47). Shame was also described as an ineffective motivator for change. On the contrary, it was suggested that feeling shame may harm relationships and discourage help-seeking: “I do not think Carole should be ashamed, or she may avoid seeking guidance” (P31).
Stigma Toward Substance Use Disorders
In discussions of maternal shame, several participants discussed the destructive effects of stigma. One participant wrote that “substance use disorders, in particular, continue to be highly stigmatized and ‘taboo' in our society” (P45), while another noted that the impact of stigma is felt by the entire family. Regarding the stigma toward SUD, it was noted that “that kind of judgemental attitude is what might cause people to be hesitant to seek help” (P15).
Parental Blame
Participants described society’s tendency to place undue blame on parents while ignoring other factors; as one participant stated, “there are so many different other influences on a person than that of their parents” (P73). It was also mentioned that parents may internalize perceptions of blame: “parents, especially mothers, tend to self-blame and take all the responsibility for all their child’s mistakes” (P41). Another participant said, “It’s easy to feel ashamed when it’s your own child, because you feel like their actions are a direct reflection of your parenting” (P27). Participants reflected on the pressures of parenting, with one saying, “as a mother, you feel you have a responsibility to raise your children right” (P77). It was further suggested that while the mother should not feel ashamed, she likely would due to the “societal norms and expectations that surround parenting” (P73).
The Mother’s Perspective
Participants often took the mother’s perspective, imagining how she might feel. It was argued that the mother was doing her best in a challenging situation with no clear answers. One participant said, “It seems like a situation of a mother who has tried her best but doesn’t know what to do or where to go and is probably exhausted” (P8). It was suggested that Carole blames herself for her child’s CUD and feels “like a failure” (P28), even though the situation is out of her control. Further comments expressed that the mother likely second-guessed her choices and the way that she handled her child’s CUD. Participants attributed a variety of emotions to the mother, including exhaustion, overwhelm, disappointment, and helplessness.
Discussion
This study examined public perceptions of maternal responsibility and shame regarding a child’s CUD, revealing diverse perspectives. Our findings contribute to knowledge of public perceptions regarding the etiology of SUD, contributing risk factors, and the extent to which a parent can mitigate these factors. Conceptualizations of the roles and responsibilities of mothers highlight the societal pressures and blame imposed on parents in the face of a child’s substance use. Further, discussions of parental shame and stigma and their detrimental consequences underscore the need to challenge public perceptions toward people with SUD and their families.
A significant proportion of participants perceived the mother as at least partially responsible for her child’s CUD. Of those who endorsed maternal responsibility, many labelled the mother’s ongoing support of her child as “enabling”. Allowing cannabis use in the home was seen as permissive of, or even encouraging, continued use. These beliefs reflect the literature on public perceptions of parents of individuals with SUD as enablers (Gruber & Taylor, 2006; Wilkens & Foote, 2019). Family members who seek support are advised by friends and family that they need to stop “enabling” their child, sending a message that the parent is doing something wrong, while providing no solutions or support (Flensburg et al., 2022; Wilkens & Foote, 2019). This accusatory advice is also prevalent when consulting treatment providers, which may prevent parents from pursuing adequate care for their child. The idea that individuals with SUD need “tough love” is pervasive, and any offering of support is seen as facilitating continued substance use (Pasman et al., 2023). On the contrary, research suggests that social and family support leads to better treatment outcomes for those with SUD (Dobkin et al., 2002; Stevens et al., 2015). Labelling parents of a child with SUD as enabling is harmful as it may discourage them from providing support that may improve their child’s long-term outcomes.
Many participants placed blame on the mother for failing to intervene in the face of her child’s CUD. This finding highlights the perception that parents have the capacity to prevent or resolve a child’s substance use (Smith & Estefan, 2014), indicating a lack of understanding of the nature of addiction. Several participants expressed the opinion that the mother should have put her child into rehab, reflecting the attitude that the parent is responsible for ensuring adolescent recovery (Villatoro et al., 2018). While SUD treatment during adolescence may require extensive parental involvement, this understanding of the parent as the enforcer of recovery overlooks the importance of individual agency and readiness to change (Mathis et al., 2009; Opsal et al., 2019). Further, mothers of adolescents with SUD have indicated in qualitative research that attempts to control their child’s substance use were largely unsuccessful and damaging to the relationship (Orford et al., 2010; Usher et al., 2007).
Participants often stated that the mother was not fulfilling her parental duties. It was suggested that the mother should have been a better role model and educator, with the implication that this could have prevented adolescent substance use. Some participants spoke of the mother’s responsibility to set strict boundaries and enforce consequences when they are broken. This sentiment that parents must supervise and control their child’s actions to prevent substance use has been reported in prior research (Choate, 2015; Smith & Estefan, 2014). Further, numerous participants described the mother’s responsibility to identify the cause of her child’s substance use problems. This notion that a SUD has a single, readily identifiable cause points to an oversimplification of the factors contributing to addiction. Further, the idea that responsibility for uncovering the supposed “cause” of addiction is placed on the shoulders of the mother rather than a healthcare professional is doubly concerning. Interestingly, some participants made assumptions about the mother that were not detailed in the vignette, inferring that the mother provided her child with cannabis, used cannabis herself, or had a history of addiction. These assumptions further reinforce how society views substance use as the parents’ fault, while the numerous roles and responsibilities imposed on the mother highlight the immense pressure that society places on mothers (Smith & Estefan, 2014).
While many participants attributed responsibility to the mother, a similar proportion expressed that the mother was not responsible for her child’s CUD. A common theme was the concept of addiction as a disease which cannot be “caused” by a person. This perspective aligns with the Disease Model of Addiction, which posits that prolonged substance use causes structural changes in the brain, leading to compulsions and loss of control demonstrated in addiction (Leshner, 1997). The understanding of addiction as a medical disease directly opposes moral models, which perpetuate stigma and judgement by viewing addiction as a character weakness (Smith & Estefan, 2014). Participants also highlighted that addiction could happen to anyone, a sentiment which counters the false and stigmatizing rhetoric that SUD only occurs in “dysfunctional” family units (Corrigan & Miller, 2004; Flensburg et al., 2022).
Looking beyond maternal responsibility, participants discussed the constellation of factors that can contribute to the development of addiction. Participants suggested that SUD may be related to genetic, family history, mental health, and societal influences, findings that align with prior research (Nawi et al., 2021; Somani & Meghani, 2016). Peer influence was highlighted as a major factor contributing to adolescent SUD, a finding which is well-documented in the literature (Foster & Spencer, 2013; George & Vaccarino, 2015; Watts et al., 2024). Several participants identified the legalization of cannabis, particularly the increase in its accessibility and normalization in society, as a risk factor for adolescent substance use. Preliminary research indicates that youth cannabis use rates have remained largely stable since legalization in 2018 (Nguyen et al., 2023). Nonetheless, participants’ discussions of the numerous contributing factors for CUD emphasize the complex nature of addiction and demonstrate the shortsightedness of blaming parents for their child’s substance use.
Many participants spoke of the importance of personal choice regarding SUD. While it is important to understand that SUD is not something that a person chooses, it is also imperative that people with SUD not be treated as helpless or unable to change (Racine et al., 2017). In line with the topic of personal choice, participants spoke of readiness to change as a key factor in recovery from SUD, a finding which is supported by prior research (Gaume et al., 2017; Krebs et al., 2018). Participants also discussed the limitations of parental control, particularly during the adolescent years. In a qualitative study of parents of adolescents with SUD (Usher et al., 2007), this limit of parental control was a key theme; parents expressed that controlling their children’s substance use was a near impossibility, adding that their best hope was to minimize the negative effects of substance use as best they could.
Within the current findings, participants’ perceptions of maternal responsibility varied greatly. Beliefs that the mother was allowing her child’s CUD to continue or had failed to prevent its development align with public assumptions that substance use problems result from poor parenting (Corrigan & Miller, 2004; Smith & Estefan, 2014), which may perpetuate mother blame (Jackson & Mannix, 2004). Further, these perspectives assign a high level of responsibility to the mother, which, according to the attribution model of stigma (Weiner, 1995), may increase stigmatizing and discriminatory attitudes. Conversely, other participants did not assign responsibility to the mother, acknowledging the complex nature of addiction, diverse contributing factors, and the importance of individual choice and readiness for change. Such perceptions of substance use shift the responsibility away from the mother, which, in line with the attribution theory, may decrease maternal blame and stigmatization.
A common sentiment was that the mother was taking steps to minimize the harms associated with her child’s SUD. Participants mentioned the importance of maintaining the parent–child relationship, suggesting that threats and ultimatums would only cause more damage. These findings echo the sentiments of Canadian parents of adolescents who use cannabis, who emphasized the importance of maintaining a strong relationship with their child to provide continued support and guidance (Haines-Saah, 2019). Some participants felt that the mother’s continued support of her child was protective against adverse substance use outcomes. Particularly, it was suggested that by offering her child a ‘safe space’ to use cannabis at home, the mother was preventing an escalation to riskier substance use. The importance of harm reduction has been highlighted in qualitative research, where parents of adolescents with SUD discuss their efforts to minimize the negative effects of their child’s substance use behaviours (Usher et al., 2007).
Participants frequently expressed contradictory opinions on maternal responsibility. Notably, while about half of the participants attributed some level of responsibility to the mother, very few stated this directly (e.g. “he mother is responsible”). More often, initial statements that the mother in the vignette was not responsible for her child’s CUD were followed up with comments that the mother was enabling her child, should have intervened sooner, or did not adequately protect or support her child. These opposing statements regarding maternal responsibility may stem from social desirability bias, where participants did not want to outright blame the mother, and instead expressed their judgement in a roundabout way. This response pattern further emphasizes the implicit societal tendency to blame parents for youth SUD (Corrigan & Miller, 2004; Flensburg et al., 2022; Wilkens & Foote, 2019).
The overwhelming majority of participants felt that the mother depicted in the vignette should not feel ashamed because of their child’s CUD, with many highlighting that shame is not conducive to positive change. This attitude aligns with research that shame negatively impacts individuals with SUD and their families (Flensburg et al., 2022; McCann & Lubman, 2018). Qualitative research on parents of adolescents with SUD highlights how feelings of shame prevent parents from disclosing their child’s condition (Choate, 2015; Usher et al., 2007). Parents have described withdrawing from friends and family and avoiding consulting with healthcare providers to avoid judgement. On this topic, participants often spoke of the stigma and blame that society places on parents impacted by SUD. Society’s penchant for blaming parents has been well documented in the literature (Jackson & Mannix, 2004; O’Shay-Wallace, 2020). For parents, experiencing stigma is associated with numerous negative outcomes, including social alienation, poor mental health, and avoidance of treatment for themselves and their child (McCann & Lubman, 2018; O’Shay-Wallace, 2020), emphasizing the need to challenge public perceptions of the parent’s role in SUD.
Participants often empathized with the mother in the vignette regarding the challenging situation that she was facing. Participants spoke of the emotional burden that a child’s SUD might have on a mother, highlighting feelings of fear, uncertainty, shame, and hopelessness. In prior research, parents impacted by a child’s substance use have spoken to similar emotional impacts (McCann & Lubman, 2018; O’Shay-Wallace, 2020). The emotional toll of adolescent SUD on parents highlights the importance of allocating appropriate supports and therapeutic interventions for parents. Further, research indicates that treating adolescent SUD using a family therapy approach may yield superior results to individual treatment (Baldwin et al., 2012; Liddle et al., 2001).
This study has several strengths and limitations. Our study benefited from a large sample size, allowing us to capture a variety of experiences, attitudes, and viewpoints. However, despite our efforts to collect a diverse sample during recruitment, it must be noted that most participants in this study identified as women; perspectives may have differed had there been more gender diversity in our sample. Additionally, most participants indicated some level of postsecondary education; research suggests that a higher level of education is associated with less stigmatizing attitudes toward people with mental illness and SUD (Keyes et al., 2010; Sandhu et al., 2019). As such, the perspectives and attitudes captured in our findings may not reflect those of the larger Canadian public.
In the current study, participants discussed maternal shame and responsibility in the context of a fictionalized scenario described in a vignette. The vignette depicted CUD, which is generally less stigmatized than other SUDs (Brown, 2015; Palamar et al., 2012); it is possible that attitudes toward the mother may have differed substantially had a more stigmatized substance been depicted. Further, the language in the current vignette included terms considered stigmatizing to parents of children with SUD (e.g. “enabling”), which may have contributed to increased perceptions of responsibility. However, it is noteworthy that in the context of this language, many responses were still supportive and empathetic toward the mother. Still, the attitudes expressed in this study are tied to the context of the vignette and may not reflect participants’ views of all mothers impacted by a child’s SUD. Nonetheless, participants often spoke of factors beyond the contents of the vignette, discussing the diverse range of factors that contribute to SUD, the societal pressures and blame placed on parents, and the harmful impact of shame and stigma on well-being, highlighting that the findings have relevance beyond the specific context of this study.
The current findings have several implications. The results revealed perceptions that the mother could have prevented her child’s CUD and that it was her responsibility to find a resolution. Such perceptions of the mother as primarily responsible for her child’s SUD may perpetuate maternal blame and stigma (Flensburg et al., 2022; Jackson & Mannix, 2004). Conversely, participants in the current study who did not assign responsibility to the mother often spoke of the numerous other factors influencing SUD. Notably, research suggests that increased education on SUD and its causes is associated with decreases in stigmatizing attitudes (Crapanzano & Vath, 2017; Murphy & Russell, 2022). The current findings highlight the need to educate the public on the etiology of SUD, as a better understanding of the diverse factors contributing to SUD may shift perceptions of blame away from the mother. Further, healthcare providers working with mothers impacted by a child’s SUD should avoid making gendered assumptions that the mother is the primary caregiver. Service providers should also avoid using terms such as “enabler” or “codependent”, which assigns undue responsibility to caregivers and may damage the patient–provider relationship (Wilkens & Foote, 2019).
Conclusion
The present study provides valuable insights into public perceptions of maternal responsibility in relation to a child’s CUD. The results highlight the diverse perspectives and attitudes that the public holds toward adolescent CUD, parenting, and maternal responsibility and blame. These findings have important implications for challenging the harmful stigma experienced by family members of children with SUD. Perceptions of responsibility are intrinsically linked to stigmatizing attitudes; as such, understanding how the public attributes responsibility to parents affected by a child’s SUD may allow us to identify and challenge perceptions that contribute to stigma. Greater public awareness and education regarding the etiology and risk factors for SUD may decrease the harmful narrative that SUD results from parental failure. The perspectives outlined by participants may also provide clinicians and other healthcare providers with a great awareness of the emotional and psychological burden that mothers face when raising a child with CUD, highlighting the need to facilitate greater support and resources for parents.
Supplemental Material
Supplemental Material - Mothers of Adolescents With Cannabis-Use Disorder: Exploring Public Perceptions of Maternal Responsibility
Supplemental Material for Mothers of Adolescents With Cannabis-Use Disorder: Exploring Public Perceptions of Maternal Responsibility by Molly K. Downey, Olivia C. Bishop, Taylor G. J. Anthony, Brooke B. Hiscock, Isobel D. McMahon, Ashlee R. L. Coles, and Nick Harris in Journal of Family Issues
Footnotes
Acknowledgements
The authors would like to thank the participants who took the time to contribute to this research, as well as the parents whose lived experiences informed this study.
Ethical Consideration
This study was approved by the Interdisciplinary Committee on Ethics in Human Research at Memorial University of Newfoundland (ICEHR # 20240404-SC) on June 22, 2023. Participants gave written consent prior to completing the study.
Funding
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data from this study are not openly available, as they contain potentially sensitive data from human research participants. The deidentified data are available from the author upon reasonable request and with the permission of the Interdisciplinary Committee on Ethics in Human Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.