
Abstract
The purpose of this article is to determine the predictors of positive and negative parenting practices among mothers of two-to-three-year-old children in Tirana, Albania. Cross-sectional data were obtained from a representative sample of 328 mothers of two-to-three-year-old children recruited through eight randomly selected public nurseries in Tirana. Results from bivariate regressions showed significant associations between the key relevant maternal characteristics and maternal parenting practices, in line with previous studies conducted in Western societies. Results from multiple regressions showed that maternal attitudes towards child maltreatment were a dominant significant predictor of negative parenting practices (punitive parenting, inconsistent parenting, and child maltreatment) and that maternal sense of parental competence was a dominant significant predictor of positive parenting practices. The findings suggest a strong, consistent link between maternal belief systems and parenting practices among mothers of toddlers in Tirana and call for the implementation of parent training programmes that address attitudes towards child maltreatment and sense of parental competence in the Albanian society.
Introduction
Parenting Practices and Their Implications
The parent–child relationship is one of the most unique bonds among humans, characterised by interdependence, power dynamics, and involuntary nature (Maccoby, 2000; Thompson, 2015). The attitudes and actions of children’s parents and the environment that they create, shape children and the course of their intellectual, psychological, behavioural, and social development (Domitrovich & Bierman, 2001; Roksa & Potter, 2011). The quality of parent–child interactions provides the foundation for the child’s capacity to self-regulate as well as for all his/her future social interactions (Barrero-Castillero et al., 2019; Bayındır & Ural, 2019; Kuczynski & Mol, 2015; Nordling et al., 2016). Parenting in the first three years of life has been established as particularly important for long-term functioning and key to public health improvement (Gustafsson & Cox, 2012; Simkiss et al., 2013).
Parenting practices can be grouped into positive and negative parenting practices. Positive parenting practices include attentive, nurturing, warm, and accepting behaviours towards children (Lachman et al., 2014; Sherr et al., 2017). Negative parenting practices include punitive, abusive, harsh, and inconsistent behaviour (Bornstein, 2015). Early positive parenting has been associated with reduced risk for conduct disorder, crime, and delinquency (Chronis et al., 2007; Loeber & Stouthamer-Loeber, 1986) as well as with reduced risk for child depression (Dallaire et al., 2006). Positive parenting has been further found to predict increased empathy and pro-social behaviour (Davidov & Grusec, 2006), as well as to be one of the most robust protective factors for children exposed to various adversities (Luthar et al., 2015). On the other hand, negative parenting has been associated with adverse early language and social skill development (Assel et al., 2002), poor school performance (Glascoe & Leew, 2010), as well as increased antisocial behaviour (Caspi et al., 2004) and increased risk of developing a broad range of mental health conditions later in life (Elgar et al., 2007).
Predictors of Parenting
The identification of predictors of parenting behaviours early in the child’s life offers the possibility of intervention before the onset of negative consequences, thus allowing for long-term efficacy and cost-effectiveness (Bakermans-Kranenburg et al., 2003; Wilson et al., 2009). The existing literature on individual predictors of parenting is substantial. The literature suggests that predictors of positive parenting include perceived parental competence (Ngai et al., 2010), parental self-efficacy (Bryanton et al., 2008; Coleman & Karraker, 1998), good perceived partner support, increased maternal education, maternal mental health (Bryanton et al., 2009), higher socio-economics status (McConnell et al., 2011), as well as maternal positive perception of the birth experience (Bryanton et al., 2008).
Negative parenting on the other hand has been associated with low levels of partner support (Kendler et al., 1997), low socio-economic status (Trentacosta et al., 2010), parental depression (Davis et al., 2011; Fujiwara et al., 2012; Glascoe & Leew, 2010), parental anxiety disorders (Kendler et al., 1997), low maternal self-control (Nofziger, 2008), high levels of maternal ADHD symptoms (Chronis-Tuscano et al., 2008), maternal substance use (Kelley, 1998), maternal emotional stress (Assel et al., 2002), inadequate social support (Cooklin et al., 2012), and exposure to violence (Westbrook & Harden, 2010). Research shows that mothers who have experienced a high number of adverse childhood experiences (ACEs), such as exposure to maltreatment and household dysfunction, report higher levels of parent-to-child aggression, thus perpetuating the intergenerational cycle of violence and trauma (Shin et al., 2022). Mothers who have experienced intimate partner violence (IPV) have been further found to be more likely to exhibit negative parenting towards their offspring (Gage & Silvestre, 2010; Herbell et al., 2020). With few exceptions (e.g. Thomson et al., 2014), the current research has however focused on specific risk factors, rather than on many potential predictors, thus making comparative evaluation among all potential predictive factors of parenting practices difficult.
Parenting Practices in Albania and in Low-and-Middle-Income Countries (LMICs)
Even though violence against children in Albania is unlawful, nearly 77% of children aged 2–14 experience physical punishment and/or psychological aggression as a form of ‘discipline’ at home, and many parents still believe that physical punishment is a necessary method in childrearing (INSTAT, 2018; Mijatović, 2018). The normalisation of child maltreatment in Albania is also embedded in common expressions, such as ‘whoever spanks you, loves you’ (Qirjako et al., 2014, p. 173). The majority of adults, including 74.8% of parents and 68.5% of teachers, report that smacking is an acceptable way to teach respect (Save the Children, 2019). Results from the Multiple Indicator Cluster Survey (MICS) in Albania (UNICEF, 2005) display that 49% of children had experienced some kind of psychological or physical punishment. More recent data from UNICEF (2014) show that toddlers are particularly affected by this phenomenon, with 72% of Albanian 2–4 year olds having experienced any form of violent discipline (either physical or psychological) in the past month. Evidence from the same source further demonstrate the vulnerability and high risk of victimisation of Albanian youth, with Albania ranking the third among all Central and Eastern European countries with the highest homicide rate of children and adolescents in 2012.
Nevertheless, the studies on domestic violence in Albania to date are of a prevalence nature. Scientific debate on family and children particularly in Albania is very recent and remains isolated, with the mechanism of transmission from parents to children not yet considered an issue (Sado et al., 2018). UNICEF (2018) further claims that there are few attempts at evidence-based policy-making in Albania. The implementation of preventive efforts informed by data has been proven to contribute to the reduction of violence against children and to its individual and social consequences (World Health Organization, 2010). However, these evidence-based preventive efforts tend to be limited to affluent countries (Murray et al., 2018a). Even though LMICs, such as Albania, are disproportionately affected by this phenomenon, they currently lack the knowledge and capacity to tackle it (Cyr & Alink, 2017; de Ribera et al., 2019). There is currently a low evidence base on child maltreatment and on the factors that influence parenting in LMICs (de Ribera et al., 2019; Stoltenborgh et al., 2015; Ward et al., 2016). Nevertheless, a key requirement for responding to the needs of populations in LMICs is to determine the extent of the problem and to identify relevant risk factors (Ezzati et al., 2002).
Study Aims
Although research on parenting and child maltreatment has advanced in many ways over the past decades, the complexity of this issue leaves many critical questions demanding further attention, particularly in rather under-studied societies (Nadan et al., 2015). The exact mechanisms through which mothers parent and/or maltreat their children are not yet fully known (Schelbe & Geiger, 2017). For example, there is little empirical research examining how parental belief systems and cognitions shape parenting (Sigel et al., 2014). Moreover, little is known about how a mother’s own temperament, personality, and/or poor regulation and psycho-social functioning – not necessarily tied to the challenges associated with her parental roles – influence her parenting practices. Developmental scientists have been recently suggesting researchers to examine the well-being of ‘mothers as persons’ (Luthar et al., 2015, p. 273), rather than as solely confined within their roles as caretakers.
The aim of this article is hence twofold. First, it builds on the existing knowledge of predictors of maternal parenting practices by investigating a wide variety of potential predictors based on previous studies, such as maternal exposure to violence, maternal mental well-being, personality characteristics, attitudes towards maltreatment, sense of parental competency and demographic information, without focussing on any particular group of characteristics. Scrutinising all potential predictors simultaneously allows for the identification of the most prominent predictors of parenting practices. Second, it presents novel data on the link between maternal parenting practices and maternal characteristics in a LMIC such as Albania. Since the dataset employed in the present study is cross-sectional, conclusions regarding the direction of the relationship between independent predictors and dependent outcomes need to be drawn with caution.
Methods
Study Design and Sample
The questionnaire design of this study has been partly informed by the Evidence for Better Lives Study (EBLS), a comparative birth-cohort study led by the Violence Research Centre at the University of Cambridge (see Valdebenito et al., 2020). However, the present study is focused on mothers of toddlers rather than the period of pregnancy, as is the case in EBLS. This is a cross-sectional study which took place in Tirana, the capital and most populous city in Albania (INSTAT, 2018). With an area of 41.8 square kilometres, it is located in the centre of the country, and it is the leading economic and political centre in Albania. Its population in 2020 amounted to 850,530 inhabitants (Bashkia Tiranë, 2020). Tirana has 34 public nurseries and 11 administrative units, which Dumani et al. (2017) have grouped into four main clusters based on these units’ socio-economic developmental level. Public nurseries were the location of participant recruitment. Eight out of the 34 public nurseries in Tirana were selected to participate in the study. The sample consists of 328 mothers of two-to-three-year-old toddlers, who were registered in Tirana’s public nurseries.
The nurseries were the unit of randomisation, and they were randomly selected based on the socio-economic status of the geographical area in which they were located. Three main steps were followed to select the final target sample of eight nurseries. First, all the 34 public nurseries in Tirana were grouped by the 11 administrative units. Second, the nurseries were allocated the developmental cluster score of the administrative unit they were located in. Each developmental cluster was given a number from one to four. Third, two nurseries per cluster were selected through systematic random sampling, with the sampling fraction per cluster being calculated by dividing two with the total number of nurseries in each respective cluster. Mothers of two-to-three-year-old children were contacted in each of the chosen nurseries based on convenience and availability, with the number of participants per nursery ranging from 38 to 45. Four inclusion criteria guided the recruitment of mothers: (1) They had to live in the same administrative unit as the nursery at hand; (2) They had to have at least one child aged two to three years old; (3) Their toddler had to be registered in the nursery at hand; (4) The mother had to be older than 18 years of age. The overall participation rate was 84%.
Instruments and Measures
Dependent Variables
Punitive Parenting
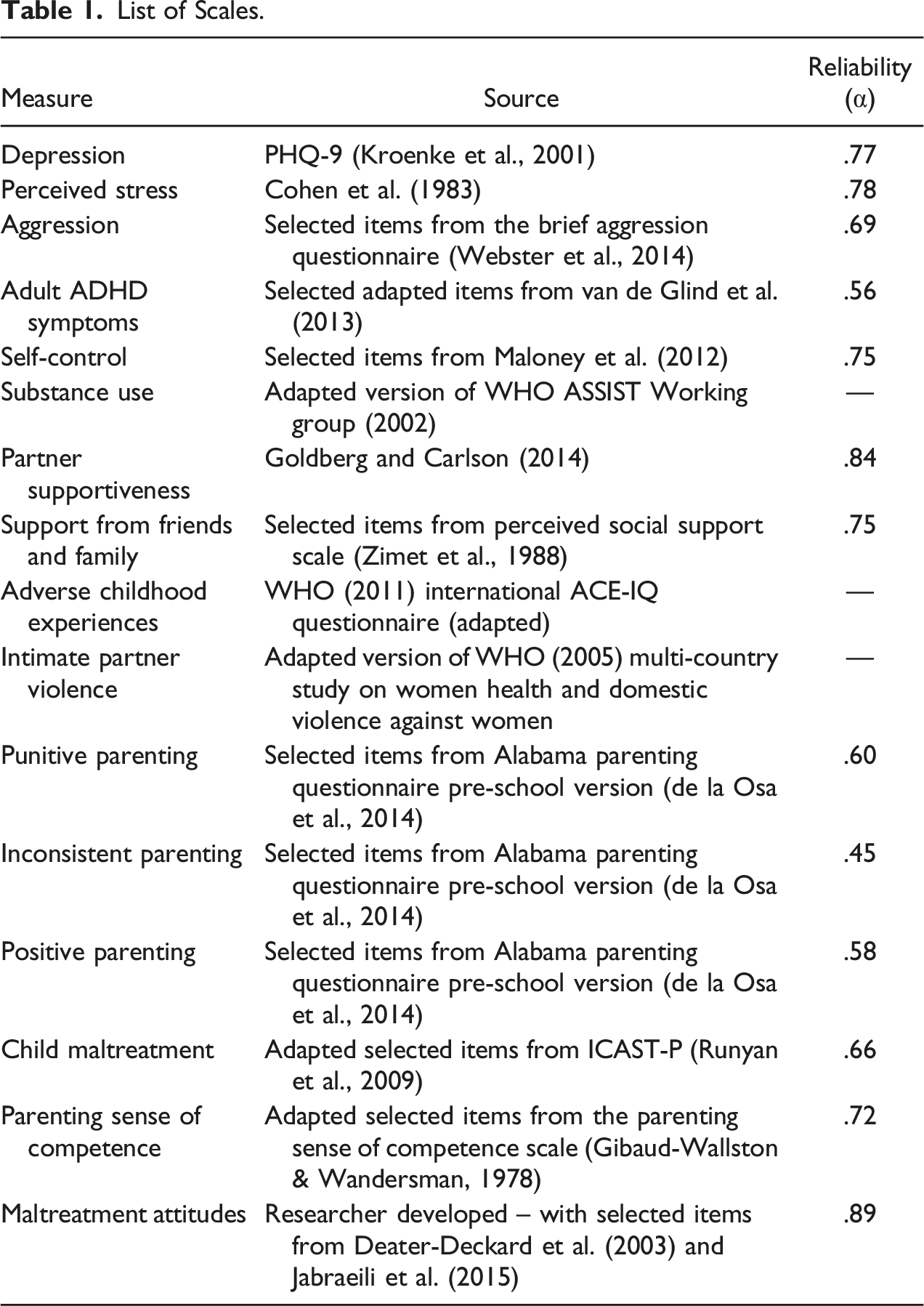
List of Scales.
Inconsistent Parenting
Inconsistent parenting was measured via five items selected out of seven items from the sub-scale ‘Inconsistent Parenting’ of the Alabama Parenting Questionnaire Pre-school Version (Clerkin et al., 2007; de la Osa et al., 2014). The main criteria for choosing the items were the items’ factor loadings as presented in the study conducted by de la Osa et al. (2014). The items that scored highest in the ‘Inconsistent Parenting’ factor were selected to measure ‘Inconsistent Parenting’ in the current study. Items are ranked on a 5-point Likert scale: Never = 1; Almost never = 2; Sometimes = 3; Often = 4; Always = 5. The respondents were give no time-frame, implying that frequency of inconsistent parenting was measured throughout the toddler’s life-course. Mean scores were calculated to build the ‘inconsistent parenting’ composite measure (α = .45). 2 Possible scores range from 1 to 5 with higher scores indicating higher levels of inconsistent parenting.
Positive Parenting
Positive parenting was measured via five items selected out of 12 items from the sub-scale ‘Positive Parenting’ of the Alabama Parenting Questionnaire Pre-school Version (Clerkin et al., 2007; de la Osa et al., 2014). The main criteria for choosing the items were the items’ factor loadings as presented in the study conducted by de la Osa et al. (2014). The items that scored highest in the ‘Positive Parenting’ factor were selected to measure ‘Positive Parenting’ in the current study. Items are ranked on a 5-point Likert scale: Never = 1; Almost never = 2; Sometimes = 3; Often = 4; Always = 5. The respondents were given no time-frame, implying that frequency of positive parenting was measured throughout the toddler’s life-course. Mean scores were calculated to build the ‘positive parenting’ composite measure (α = .58). Possible scores range from 1 to 5 with higher scores indicating higher levels of positive parenting.
Child Maltreatment
15 adapted items out of the 45 items of the ISPCAN Child Abuse Screening Tool Parent Version (ICAST-P) were used to capture maternal abusive behaviour towards her toddler (see Runyan et al., 2009). Parents are asked about omissions in care and about acts of discipline or violence towards the index child. The present study only focuses on physical discipline (4 items), psychological discipline (8 items), and neglect (3 items) throughout the toddler’s life-course. All items in this survey are ranked on a 5-point Likert scale: Never = 0; Once or twice = 1; Three to five times = 2; Six to ten times = 3; More than 10 times = 4. Mean scores were calculated to build the ‘child maltreatment’ composite measure (α = .66). Possible scores range from 0 to 4 with higher scores indicating higher levels of child maltreatment.
Independent Variables
Maternal Depression
The Patient Health Questionnaire (PHQ-9) was used to measure the severity of depressive symptoms experienced by the mother in the last month (Kroenke et al., 2001). Questions measure anhedonia, dysphoria, sleep disturbances, fatigue, changes in eating, low self-esteem, concentration difficulties, hypo-or-hyper-active behaviours, and thoughts of suicide in the past month. Each item is rated on a 4-point Likert scale: Not at all = 0; Several days = 1; More than half the days = 2; Nearly every day = 3. Mean scores were calculated to build the depression composite measure (α = .77). Possible scores range from 0 to 3 with higher scores indicating more severe depressive symptoms.
Maternal Perceived Stress
The level of maternal stress in the past month was measured by the Perceived Stress Scale (PSS) (Cohen, 1994; Cohen et al., 1983; Cohen & Williamson, 1988). This scale consists of ten items that measure how stressful certain life situations are rated by respondents during the last month, via a 5-point Likert scale. Nevertheless, in accordance with the EBLS team, the scale was adapted to a 4-point Likert scale: Not at all = 1; Several days = 2; More than half the days = 3; Nearly every day = 4. Mean scores were calculated to build the stress composite measure with four items being reverse-coded (α = .78). Possible scores range from 1 to 4 with higher scores indicating higher levels of stress.
Maternal ADHD Symptoms
ADHD symptoms were measured via five items. Three of the items in this section are adapted from the ASRS (see Adler et al., 2006), while the remaining two are adapted from the age 20 wave of the Zürich Project on the Social Development from Childhood to Adulthood (z-proso). This strategy was also followed by the EBLS team (see Murray et al., 2022). The five items measured how the mother behaved or felt in the past month, including concentration levels, stillness, distraction, and procrastination. This measure was a 5-point frequency scale: Never = 1; Rarely = 2; Sometimes = 3; Often = 4; Always = 5. Mean scores were calculated to build the ADHD symptoms composite measure (α = .56). Possible scores range from 1 to 5 with higher scores indicating higher levels of maternal ADHD symptoms.
Maternal Aggression
Aggression was measured using an adapted version of the Brief Aggression Questionnaire. The original Brief Aggression Questionnaire consists of 12 items and uses four sub-scales to measure the trait of aggression. The four sub-scales are physical aggression, verbal aggression, anger, and hostility (Webster et al., 2014). This study focuses on three sub-scales, namely, physical aggression, anger, and hostility; and employs six items in total, two items per sub-scale. When choosing the items, the items with the highest factor loadings in the study conducted by Webster et al. (2014) were prioritised. While the original scale uses a 10-point Likert-type scale, this study employs a 5-point Likert scale: Never = 1; Rarely = 2; Sometimes = 3; Often = 4; Always = 5. Mean scores were calculated to build the aggression composite measure (α = .69). Possible scores range from 1 to 5 with higher scores indicating higher levels of maternal aggression.
Maternal Self-Control
Self-control was measured through seven out of 13 items of the Brief Self-Control Scale, a survey measuring operational aspects of self-control (Maloney et al., 2012). Actions and thoughts related to temptation, self-discipline, and impulsive behaviour, among others, are scored using a 5-Likert Scale: Not at all = 1; Slightly = 2; Somewhat = 3; Mostly = 4; Very much = 5. Mean scores were calculated to build the self-control composite measure with six items being reverse-coded (α = .75). Possible scores range from 1 to 5 with higher scores indicating higher levels of self-control.
Parental Sense of Competence
The mother’s parental sense of competence was measured via 10 adapted selected items from the Parenting Sense of Competence Scale (PSOC) (Gibaud-Wallston & Wandersman, 1978). The PSOC is an instrument commonly used to measure parental self-efficacy and satisfaction with parenting (also see Johnston & Mash, 1989; Ohan et al., 2000; Oltra-Benavent et al., 2020). The PSOC is a 17-item scale, with 2 sub-scales: satisfaction and efficacy. When choosing the items, representation from the two sub-scales and factor loadings from previous studies were prioritised. While in the original version each item is rated on a 6-point Likert scale, this study employs a 5-point Likert scale: Strongly disagree = 1; Disagree = 2; Neutral = 3; Agree = 4; Strongly agree = 5. Mean scores were calculated to build the ‘parental sense of competence’ composite measure with five items being reverse-coded (α = .72). Possible scores range from 1 to 5 with higher scores indicating higher levels of the mother’s parental sense of competence.
Maltreatment Attitudes
This scale consisted of 15 items and measured the mother’s attitude towards child physical maltreatment, emotional maltreatment, and neglect. The five items on endorsement of spanking by parents were retrieved from Deater-Deckard et al. (2003). The five items on the attitude towards emotional maltreatment and the five items on the attitude towards neglect were developed by the author, with certain items taken from Jabraeili et al. (2015). Each item is rated on a 5-point Likert scale: Strongly disagree = 1; Disagree = 2; Neutral = 3; Agree = 4; Strongly agree. Mean scores were calculated to build the ‘maltreatment attitudes’ composite measure (α = .89). Possible scores range from 1 to 5 with higher scores indicating higher levels of maltreatment attitudes embraced by the mothers.
Maternal Adverse Childhood Experiences (ACEs)
Maternal adverse experiences before the age of 18 were measured via 18 adapted items out of 31 items of the ACE-International Questionnaire (World Health Organisation, 2011). The 18 items included in the current study belonged to the following nine domains: (1) living with substance abusers; (2) living with household members who were mentally ill or suicidal; (3) living with household members who were imprisoned; (4) parental separation or divorce, one or no parents; (5) violence against household members; (6) emotional abuse; (7) physical abuse; (8) sexual abuse; (9) physical neglect. The first four domains, which consist of five items, ask yes/no questions, while the items in the rest of the domains are rated on a 4-point Likert scale: Never = 1; Once = 2; A few times = 3; Many times = 4. The ACEs composite measure consists of the sum scores of the first five items and the dichotomised versions of the rest of the 13 items.
Intimate Partner Violence
Exposure to IPV during the mother’s lifetime was measured using an adapted scale extracted from the World Health Organisation’s (2005) Multi-country Study on Women’s Health and Domestic Violence Against Women (also see Garcia-Moreno et al., 2006). Seven items measure controlling behaviour by the current partner, six items measure physical IPV, four items measure emotional IPV, and three items measure sexual IPV (No = 0; Yes = 1). The composite measure of lifetime IPV was calculated by summing up the yes/no items on controlling behaviour as well as the items on physical, emotional, and sexual IPV. Possible scores range from 1 to 20 with higher scores indicating higher exposure to IPV.
Control Variables
Control variables included in the regression models involved the following: father’s quality time spent with the child (ordinal, but treated as continuous), age of the child in months (open answer, continuous), mother experienced birth complications (0 = no; 1 = yes), mother’s age in years (open answer, continuous), mother’s educational level (0 = below undergraduate degree; 1 = undergraduate degree or above), mother’s marital status (0 = not married; 1 = married), household income (ordinal, but treated as continuous), lifetime maternal substance use [0 = no; 1 = yes; measured via four adapted items taken from the Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST), a screening questionnaire developed by the World Health Organisation (2002)], maternal support from friends and family [measured by nine out of 12 items of the Multidimensional Scale of Perceived Social Support (MSPSS), developed by Zimet et al. (1988), using a 5-point Likert-type scale. The composite measure was calculated through mean scores (α = .75), with higher scores indicating higher levels of support from friends and family], maternal support from the partner [measured via the Partner Supportiveness Scale (Goldberg & Carlson, 2014), a five-item survey, each rated on a 5-point Likert scale. The composite measure was calculated through mean scores (α = .84), with higher scores indicating higher levels of support from the partner], and the mode of questionnaire delivery (measured by two dummy variables: the first variable was coded as 0 = self-completed, 1 = face-to-face interview; the second variable was coded as = self-completed, 1 = online interview).
Translation and Data Collection
The instruments were translated in whole by four individuals, who were native Albanian speakers, proficient in English, and who were familiar with psychometrics as well as the health sector. Three modes of questionnaire delivery were employed to collect the data: face-to-face interview (N = 170), self-completed (N = 116), and online interview (N = 42). 3 While the initial plan was to only conduct face-to-face interviews, adaptations had to be made due to the COVID-19 pandemic as well as the participants’ availability. Even though it is not ideal to have heterogenous modes of data collection, this approach might be valuable insofar that it helps us better understand how different modes of data collection may affect response levels. The data collection process was carried out by the author and lasted from September 2020 to May 2021.
Data Analysis
Characteristics of the study population were described using counts and percentages for categorical variables and means (SD) for continuous variables. Some continuous variables were also transformed into dummy variables to get a better understanding of prevalence rates. Four ordinary least square (OLS) linear regression models were built to examine the association between the four dependent variables measuring parenting practices (punitive parenting, inconsistent parenting, positive parenting, and child maltreatment) as well as all the independent variables. Bivariate regression models measured the link between dependent variables and each individual predictor and control variable separately, while multiple regression models measured the association between the dependent variables and all predictor and control variables simultaneously. This would allow us to better understand and compare the predictive power of each independent variable on its own, as well as to identify the independent variables with the highest and most significant predictive power when all the independent variables are considered together. Identifying the predictors with the highest significance would help us target our efforts in terms of prevention and intervention.
Tests to see whether the independent variables for each of the four multiple regression models were not highly correlated and met the assumption of collinearity indicated that multicollinearity was not a concern (MVIF = 1.57). As suggested by the literature, VIFs between 1 and 5 indicate that there is a moderate correlation, but it is not severe enough to warrant corrective measures (Daoud, 2017). When running the regression models, multiple imputation was used as a method of handling missing data. There were no visible patterns of missing values, hence suggesting that these values were missing at random. Thirty-seven imputations were run to primarily address the missing values in the ‘household income’ (nmiss = 37) variable. The reason behind the high level of missingness in this variable was related to the fact that 35 mothers preferred not to answer the question regarding household income. All analyses were conducted using STATA IC Release16. Materials and analysis code for this study are available by emailing the corresponding author.
Ethical Considerations
Ethical approval and institutional access were obtained from the Institute of Criminology, University of Cambridge and the General Directory of Nurseries and Kindergartens at the Municipality of Tirana. Permission to conduct the study was also obtained by each director of the eight nurseries selected to participate in the study. Before starting the data collection process, all participating mothers were given information sheets and asked to sign an informed consent form.
Results
Describing the Study Population
Descriptive Data of the Dependent, Independent, and Control Variables.
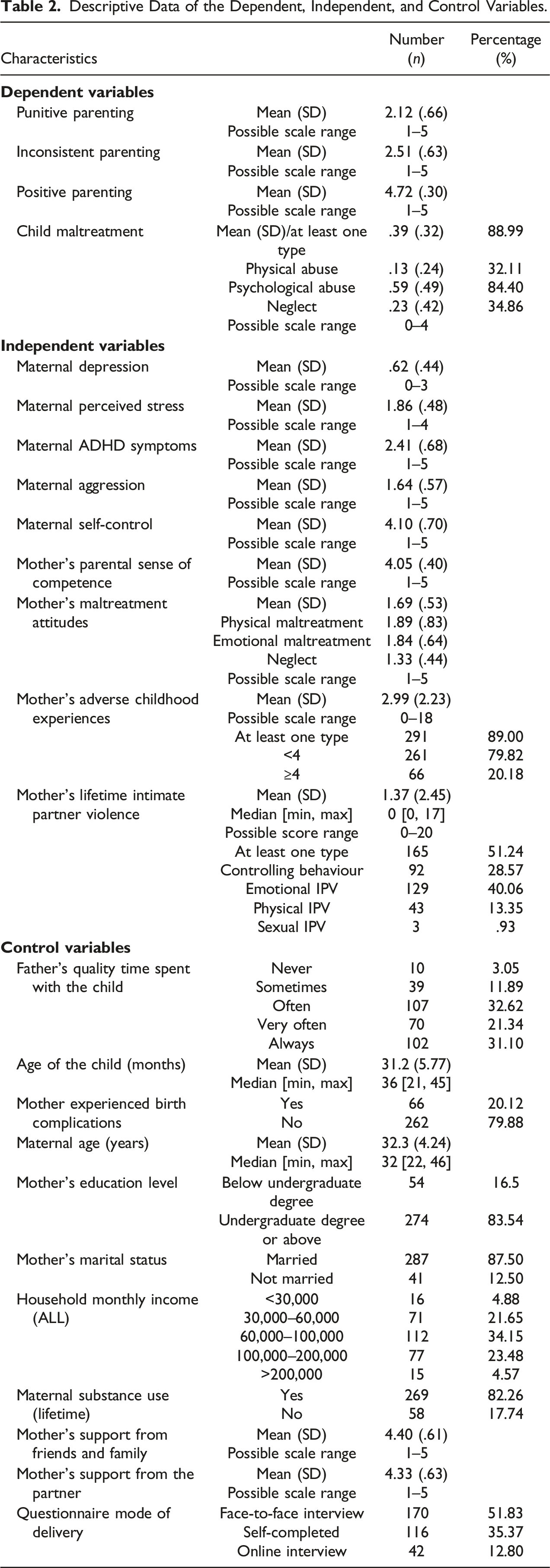
Most mothers had experienced at least one type of ACE (89%), with 20.18% of mothers having experienced four ACEs or more. 51.24% had experienced at least one type of IPV (controlling behaviour, emotional, physical, or sexual violence) in their lifetime, with 28.57% of mothers enduring controlling behaviour from their partners, 40.06% having experienced emotional IPV, 13.35% physical IPV, and .93% sexual IPV. In terms of parenting practices, the reported mean of positive parenting (M = 4.72) 5 was higher than of punitive parenting (M = 2.12) and of inconsistent parenting (M = 2.51). As far as child maltreatment is concerned, the mean of mother-reported psychological abuse towards her toddler (M = .59) was higher than the mean of physical abuse (M = .13) and the mean of neglect (M = .23). Almost 89% of mothers had used at least one type of child maltreatment towards their toddler. 32.11% had used physical abuse, 84.4% had used psychological abuse, and 34.86% had neglected their toddler at least once. However, generally, mothers had high disapproval of child maltreatment (M = 1.69; SD = .53).
Predictors of Punitive Parenting
Bivariate and Multiple Regression Results for Predictors of Positive and Negative Parenting.
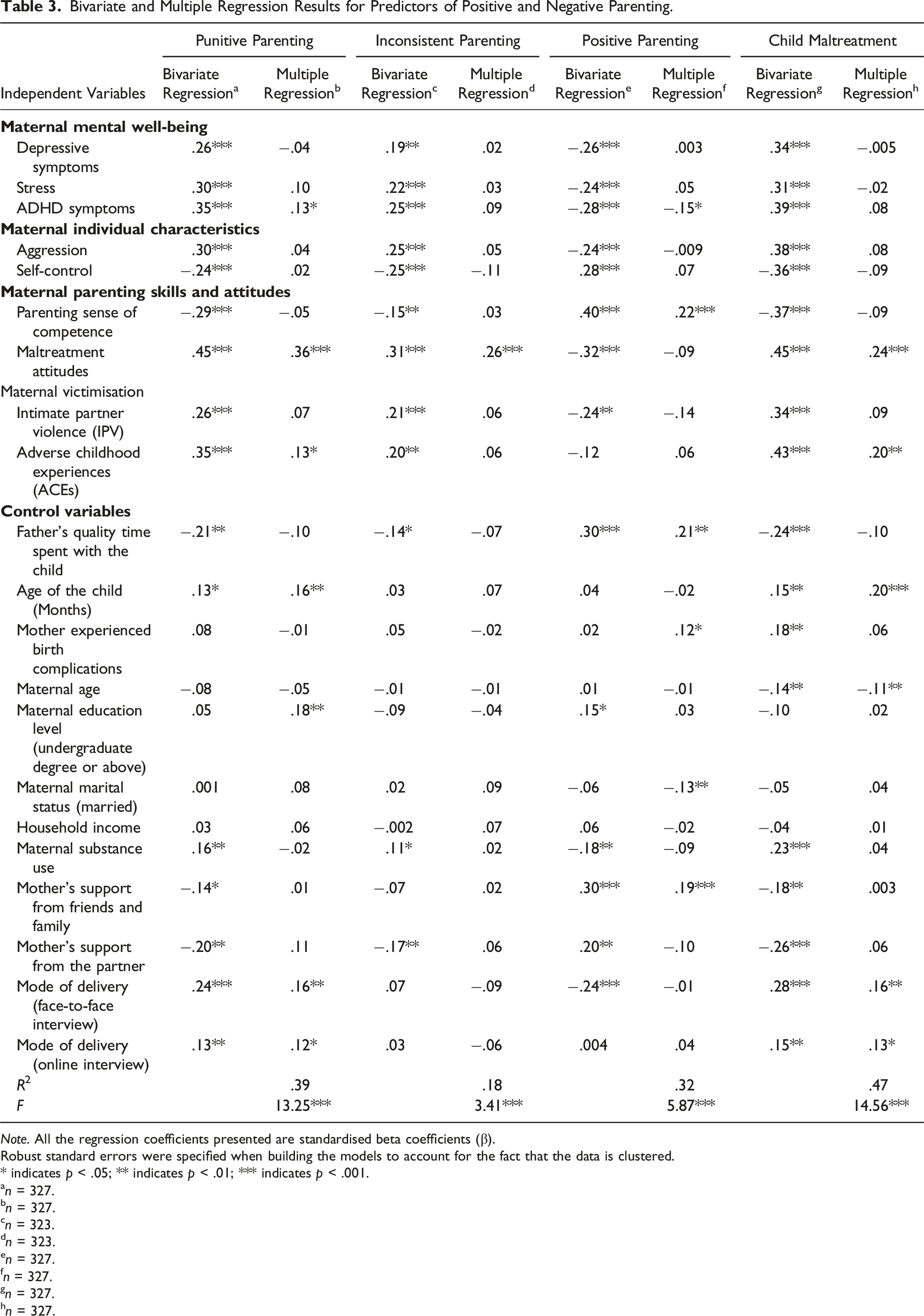
Note. All the regression coefficients presented are standardised beta coefficients (β).
Robust standard errors were specified when building the models to account for the fact that the data is clustered.
* indicates p < .05; ** indicates p < .01; *** indicates p < .001.
an = 327.
bn = 327.
cn = 323.
dn = 323.
en = 327.
fn = 327.
gn = 327.
hn = 327.
In the multiple regression model, which included all the predictors simultaneously, only maternal ADHD symptoms (β = .13, p < .05), maltreatment attitudes (β = .36, p < .001), maternal adverse childhood experiences (β = .13, p < .05), age of the target child (β = .16, p < .01), maternal education level (β = .18, p < .01), as well as the delivery mode being in the form of face-to-face interviews (β = .16, p < .01) and online interviews (β = .12, p < .05) rather than self-completed were positively significantly associated with punitive parenting (see Table 3, Column 1.2). No variables were negatively significantly associated with punitive parenting in the multiple regression model. The multiple regression equation with ‘punitive parenting’ as an outcome variable was significant [F (21, 302.9) = 13.25, p < .001)], with an R 2 of .39. The sample size both in the bivariate and multiple regressions was 327.
Predictors of Inconsistent Parenting
In the bivariate regressions, inconsistent parenting was significantly predicted by maternal depressive symptoms (β = .19, p < .01), stress (β = .22, p < .001), ADHD symptoms (β = .25, p < .001), aggression (β = .25, p < .001), maltreatment attitudes (β = .31, p < .001), intimate partner violence (β = .21, p < .001), adverse childhood experiences (β = .20, p < .01), maternal substance use (β = .11, p < .05) in a positive direction, and by maternal self-control (β = −.25, p < .001), the mothers’ parental sense of competence (β = −.15, p < .01), father’s quality time spent with the child (β = −.14, p < .05), support from the partner (β = −.17, p < .01) in a negative direction (see Table 3, Column 2.1).
In the multiple regression model, only maternal maltreatment attitudes (β = .26, p < .001) were positively significantly associated to inconsistent parenting, with no variables being negatively significantly associated to inconsistent parenting (see Table 3, Column 2.2). The multiple regression equation with ‘inconsistent parenting’ as an outcome variable was significant [F (21, 298.9) = 3.41, p < .001)], with an R 2 of .18. The sample size both in the bivariate and multiple regressions was 323.
Predictors of Positive Parenting
The bivariate analyses in Column 3.1, Table 3, showed that positive parenting was significantly positively associated with maternal self-control (β = .28, p < .001), the mother’s sense of parental competence (β = .40, p < .001), the father’s quality time spent with the target toddler (β = .30, p < .001), the mother’s education level (β = .15, p < .05), the mother’s support from friends and family (β = .30, p < .001), and the mothers’ support from the partner (β = .20, p < .01). The bivariate analyses also showed that positive parenting was negatively associated with maternal depressive symptoms (β = −.26, p < .001), stress (β = −.24, p < .001), ADHD symptoms (β = −.28, p < .001), aggression (β = −.24, p < .001), maltreatment attitudes (β = −.32, p < .001), intimate partner violence (β = −.24, p < .01), substance use (β = −.18, p < .01), and the questionnaire being delivered face-to-face rather than self-completed (β = −.24, p < .001).
The multiple regression in Column 3.2, Table 3, displayed that positive parenting was significantly positively associated with the mother’s parental sense of competence (β = .22, p < .001), the father’s quality time spent with the target toddler (β = .21, p < .01), the mother having experienced birth complications (β = .12, p < .05), and the mother’s support from friends and family (β = .19, p < .001). The multiple regression also portrayed that positive parenting was significantly negatively associated with maternal ADHD symptoms (β = −.15, p < .05) and the mother being married (β = −.13, p < .01). The multiple regression equation with ‘positive parenting’ as an outcome variable was significant [F (21, 302.9) = 5.87, p < .001)], with an R 2 of .32. The sample size both in the bivariate and multiple regressions was 327.
Predictors of Child Maltreatment
In the bivariate regression analyses (Table 3, Column 4.1), child maltreatment was significantly positively predicted by maternal depressive symptoms (β = .34, p < .001), stress (β = .31, p < .001), ADHD symptoms (β = .39, p < .001), aggression (β = .38, p < .001), maltreatment attitudes (β = .45, p < .001), intimate partner violence (β = .34, p < .001), adverse childhood experiences (β = .43, p < .001), age of the toddler (β = .15, p < .01), whether the mother had experienced birth complications (β = .18, p < .01), maternal substance use (β = .23, p < .001), as well as the questionnaire being delivered through face-to-face interview (β = .28, p < .001) and online interview (β = .15, p < .01). The significant negatively associated predictors were the following: self-control (β = −.36, p < .001), the mother’s sense of parental competency (β = −.37, p < .001), father’s quality time spent with the target toddler (β = −.24, p < .001), maternal age (β = −.14, p < .05), mother’s support from friends and family (β = −.18, p < .01), and mother’s support from the partner (β = −.26, p < .001).
In the multiple regression model (Table 3, Column 4.2), child maltreatment was positively significantly predicted by maltreatment attitudes (β = .24, p < .001), maternal adverse childhood experiences (β = .20, p < .01), age of the child (β = .20, p < .001), as well as the questionnaire being delivered via face-to-face interviews (β = .16, p < .01) and online interviews (β = .13, p < .05) rather than self-completed. The only negatively significantly associated predictor of child maltreatment was maternal age (β = −.11, p < .01). The multiple regression equation with ‘child maltreatment’ as an outcome variable was significant [F (21, 303.0) = 14.56], with an R 2 of .47. The sample size both in the bivariate and multiple regressions was 327.
Discussion
Using cross-sectional data from a representative sample of 328 mothers whose two-to-three-year-old toddlers were registered in public nurseries in Tirana, Albania, various relevant variables related to maternal psychological well-being, individual characteristics, behavioural tendencies, and inter-personal relationships were entered in bivariate and multiple regression analyses to ascertain the predictors of positive and negative parenting. In general, results from the bivariate associations confirm findings from previous studies which have found a link between maternal mental well-being, ACEs, parental self-efficacy, exposure to IPV, substance use, social support, support from the partner, and levels of positive and negative parenting (Assel et al., 2002; Bryanton et al., 2008, 2009; Davis et al., 2011; Fujiwara et al., 2012; Gage & Silvestre, 2010; Herbell et al., 2020; Shin et al., 2022; Westbrook & Harden, 2010). Moreover, results from the bivariate regressions suggest that maternal individual characteristics such as aggressive tendencies and self-control are significantly associated with both negative and positive parenting practices. This is a rather interesting finding which adds to the literature that explores the influence of a mother’s temperament and/or self-regulation on her parenting practices (Belsky & Barends, 2002; De Haan et al., 2009; Huver et al., 2010).
The bivariate analyses also showed that apart from support from the partner, the father’s quality time spent with the child was negatively associated with the mothers resorting to punitive parenting, inconsistent parenting, as well as to child maltreatment. The father’s quality time spent with the child was also positively associated with the mother using positive parenting practices, both in the bivariate and multiple regression analyses. In addition to previous studies which have highlighted the important role of the father–child relationship in child development (e.g. Barker et al., 2017; Ramchandani et al., 2013), the finding from this study suggests that the father–child relationship could affect the child also indirectly through its link to the mother–child relationship. This finding is particularly important for the Albanian culture, given its patriarchal structure and traditional gender roles with the father typically being seen as the head of the household and the mother as the caregiver and nurturer (Zhupa, 2013). The importance of the father–child relationship and its impact on the mother’s parenting, as highlighted in the current study, further sheds light on the need to encourage Albanian families to build healthier, less hierarchical and more interdependent relationships among the parents and the children.
Regarding maternal age, previous studies indicate conflicting findings on its association with violence against children (Pearson et al., 2022), with some findings showing that lower maternal age predicts negative parenting (Kendler et al., 1997; Trentacosta et al., 2010) and others that it predicts positive parenting (Bryanton et al., 2018). The current study adds clarity to the literature by showing that maternal age is a negative significant predictor of child maltreatment, both in the bivariate and multiple regressions, meaning that the older the mother the less likely she is to resort to child maltreatment. However, maternal age does not seem to have a significant association with either punitive, inconsistent, or positive parenting in the present study. An additional finding of interest in the current study was the lack of effect of the ‘household income’ variable on all the parenting outcomes and the little to no effect of the ‘maternal education’ variable. This result is in contrast with other studies in the Balkan region, which have found that wealth and the education level of parents is significantly related to the use of non-violent methods of disciplining children (Petrovic et al., 2016).
Another finding worth noting with regards to the bivariate regression models is the significant link that the mode of questionnaire delivery has on the four outcome variables. While Ward et al. (2018) found higher disclosure rates of child maltreatment in self-completion than in interviewer-based data collection modes, the present study suggests that mothers tended to report higher rates of punitive parenting and child maltreatment in the face-to-face and online interview as compared to when the survey was self-completed. The findings further show that the mothers had the tendency to report significant lower rates of positive parenting in the face-to-face interview as compared to when they completed the survey on their own. The mode of delivery being face-to-face as compared to self-completed remained a significant predictor of maternal reporting of punitive parenting and child maltreatment even in the multiple regression models. Several reasons might explain these findings.
First, during the in-person and/or online interviews, the mothers had the space to develop trust and an emotional connection with the researcher. The lack of a trustworthy human connection might have propelled the mothers into feeling suspicious or embarrassed to disclose the truth in the self-completed version of the questionnaire. It can be argued that the presence of an interviewer encourages respondents to feel relaxed and therefore more forthcoming (e.g. Lee, 1993; Sykes & Hoinville, 1985). Second, during the interviews, the mothers might have felt that they had the time to reflect on their answers while also having the opportunity to require more explanation or clarity. In the self-completed version however, the mothers might have filled in the survey hastily without reading the items properly and reflecting on them thoroughly. It is of worth to note that the mothers completed the questionnaire at home or at work (while being advised to be alone), not in the researcher’s presence. The ‘uncontrolled’ setting could have also played a role in the mothers’ responses. Third, the outcomes could have also been impacted by the ‘interviewer effect’, whereby the mothers might have presumed that the researcher had certain expectations from the interview and was searching for data that looked a particular way. Fourth, since the participants were not randomly assigned to each mode of delivery group, there could have been an inherent difference in the characteristics of the participating mothers that opted out for telephone interview versus self-completed questionnaire versus face-to-face interview.
As far as the multiple regression models are concerned, we see that the proportion of the variance of ‘inconsistent parenting’ explained by the independent variables as well as the model fit is quite low when compared to the other outcomes. One reason that might explain this discrepancy is the low Cronbach’s alpha value of the ‘inconsistent parenting’ variable, thus raising doubts about the validity and reliability of the findings from the second model. It is useful to note that other studies administering the Alabama Parenting Questionnaire have also found lower alpha values for the ‘inconsistent parenting’ sub-scale in comparison to the other sub-scales (e.g. see Sebre et al., 2020; Liang et al., 2021), thus suggesting that ‘inconsistent parenting’ has lower construct validity than the other Alabama Parenting Questionnaire scales. The model fit of the regression analyses for the ‘positive parenting’ outcome was also rather low. This result can be attributed to the fact that the ‘positive parenting’ variable is notably left-skewed, which lives little space for the independent variables to have an influence on its variation. Nevertheless, when examining the ‘punitive parenting’ and ‘child maltreatment’ outcomes, we see that the R 2 and F values are higher and the significance of the predictor variables comparatively similar. This result is noteworthy insofar that it adds to the literature on the overlap and distinction of ‘child maltreatment’ and ‘punitive parenting’ instruments (see Backhaus et al., 2022).
A further observation of interest in the multiple regression models is the consistent significance of mothers’ attitudes towards child maltreatment across the negative parenting outcomes (punitive parenting, inconsistent parenting, and child maltreatment) and the significance of mothers’ sense of parental competence for positive parenting practices. Not only are these two variables highly significantly associated with the respective outcomes, but they also take precedence over most of the other relevant independent variables. The descriptive statistics results implied that mothers in the present study expressed high disapproval of child maltreatment, while the rates of punitive parenting and child maltreatment were quite substantial. Data from UNICEF (2014) further suggest that many households practise physical punishment even though they do not regard it as an appropriate form of discipline, thus implying that parents resort to impulsive decisions due to depletion of their own cognitive and emotional self-regulation resources even when they rationally acknowledge that maltreating children is not right or effective. Similar findings are reported by Lansford and Deater-Deckard (2012), who showed that across 24 developing countries, a larger proportion of parents report using corporal punishment than believe that it is necessary to use corporal punishment in child-rearing. Analogous results were found in a study carried out in Bosnia and Herzegovina, Northern Macedonia and Serbia, which demonstrated that most of the respondents believed that physical punishment was not necessary to raise their children properly, but less than 30% practiced only non-violent discipline at home (Petrovic et al., 2016).
Despite this discrepancy, the multiple regression analyses suggest that favourable attitudes towards child maltreatment are significantly associated with negative parenting practices even when other relevant factors are taken into consideration. Establishing relations between cognitions and practices in parenting has proved elusive with these relations appearing only weak (e.g. Okagaki & Bingham, 2005; Sigel & McGillicuddy-De Lisi, 2002). The finding from the current study is however in line with the results reported by Kochanska et al. (1989), whereby significant associations were found between authoritarian parental attitudes and harsh discipline strategies. Given that the nature of the collected dataset in the present study is cross-sectional, caution needs to be exercised regarding to the direction of the relationship between child maltreatment attitudes and negative parenting practices. While it can be argued that favourable attitudes towards child maltreatment are a consistent significant predictor of negative parenting practices even when accounting for other relevant factors, it can also be the case that maternal negative parenting practices shape mothers’attitudes towards child maltreatment. Under Festinger’s (1962) theoretical framework of cognitive dissonance, mothers may attempt to reduce cognitive dissonance by adapting their attitudes to their behaviour.
The significant association between positive parenting practices and maternal levels of parental sense of competence, even after accounting for other relevant variables, further demonstrates the link between maternal cognitive patterns and parental behaviour. While the causal direction still remains an issue, previous research conducted in the West has found that parental self-efficacy beliefs are both a powerful direct predictor of specific positive parenting practices and a mediator of the effects of most of the correlates of parenting quality, including maternal depression, child temperament, social support, and poverty (Albanese et al., 2019; Coleman & Karraker, 1998). A study conducted by Bornstein et al. (2018) further concluded that mothers who were more knowledgeable, satisfied, and attributed successes in their parenting to themselves when their toddlers were 20 months of age, engaged in increased supportive parenting during joint activity tasks 2 years later when their children were 4 years of age. The findings from the present study call for the need of maternal change of beliefs and parenting behaviour within the Albanian society, ideally through the widespread implementation of parent training programmes which are either in their infancy or still lacking in Albania (see Dai et al., 2018). Systematic reviews of randomised and quasi-randomised evaluations suggest that parenting programmes can increase positive parenting, reduce punitive parenting, and decrease child behaviour problems in children from birth to 12 years old (e.g. Barlow et al., 2010; Furlong et al., 2012).
Three additional independent variables that were significant predictors in more than one multiple regression model were: maternal ADHD symptoms, maternal ACEs, and age of the child. While maternal ADHD symptoms are a positive significant predictor of ‘punitive parenting’ and a negative significant predictor of ‘positive parenting’, maternal ACEs are a positive significant predictor of ‘punitive parenting’ and ‘child maltreatment’. The later finding is in line with the literature that explores the continuity of violence from one generation to another, a phenomenon also known as the cycle of violence (Britto et al., 2017; Widom & Wilson, 2015). As previously mentioned, empirical studies in other parts of the world have indeed also shown that mothers who have experienced a high number of ACEs report higher levels of parent-to-child aggression (Shin et al., 2022). The finding regarding the significant predictive power of maternal ADHD symptoms for punitive and positive parenting practices, when all other relevant factors are controlled for, adds to the current evidence base that has demonstrated that mothers with higher levels of ADHD Symptoms report lower levels of involvement and positive parenting and higher levels of maladaptive parenting practices (Chronis-Tuscano et al., 2008). Nevertheless, rarely has this literature focused on the impact of ADHD symptoms on the parenting of toddlers specifically, with this link being under-recognised, under-studied, and under-addressed in LMICs (Fayyad et al., 2017; Murray et al., 2022). The age of the child, on the other hand, is only positively associated to punitive parenting and child maltreatment, thus suggesting that the older the child, within the toddlerhood years, the more likely are the mothers to use harsh parenting practices.
Strengths and Limitations
The main strengths of this study are related to the fact that it makes use of a probabilistic rather than a convenience sampling method, to the relatively high overall participation rate (84%), to all the data being collected by the author, and to it presenting novel data on the predictors of parenting practices in Albania. The limitations are concerned with the limited sample size, the delivery of the questionnaire through three different modes of data collection, the restricted possibility of generalising the findings to all Albanian mothers and toddlers, the study outcomes being self-reported, as well as with the fact that this is a cross-sectional rather than a longitudinal study, which thus prevents one from drawing causal conclusions about the data. The low Cronbach’s alpha value of the ‘inconsistent parenting’ variable and the left-skewness of the ‘positive parenting’ variable can be considered as two further limitations of this study.
Conclusion
This study was an initial attempt at uncovering the unexplored predictors of positive and negative parenting practices among mothers of toddlers in Tirana, Albania. Among others, the bivariate regression analyses found a link between maternal age, mental well-being, ACEs, exposure to IPV, substance use, social support, support from the partner, aggressive tendencies, self-control, and levels of positive and negative parenting. Results from multiple regression models showed that maternal attitudes towards child maltreatment were a dominant significant predictor of negative parenting practices (punitive parenting, inconsistent parenting, and child maltreatment) and that maternal sense of parental competence was a dominant significant predictor of positive parenting practices. The results from multiple regression analyses further demonstrated that the mothers’ reporting of punitive parenting and child maltreatment was significantly predicted by the mode of delivery being face-to-face as compared to self-completed, even when other relevant factors were controlled for.
In terms of implications for practice, findings from the current study suggest a need for supporting mothers as individuals and as women through psychological support, gender equality initiatives, and freedom from violence more broadly. The findings further call for the implementation of parental support groups and parent training programmes in the Albanian society to help change maternal belief systems regarding effective parenting practices and healthy early child development. Previous research has shown that the cycle of abuse is broken when social services such as support groups, mentoring programmes, or therapeutic interventions are provided for parents who are deemed at risk of abusing their children (Grille, 2008; Hall et al., 1998; Hunter & Kilstrom, 1979).
In terms of implications for research, it is advisable for future empirical research in the field of parenting to consider administering solely one mode of data collection in order to allow for consistency in results as well as for higher validity and reliability of findings. Moreover, it would also be interesting for future research on methodological issues to further examine the impact that the mode of questionnaire delivery can have on self-reported sensitive information, for example, through conducting rigorous randomised controlled trials or propensity score matching. It would be particularly of worth to investigate these methodological issues in LMICs given that most identified studies to date on the impact of delivery mode on the reporting of sensitive information have been conducted in HICs. Future studies should further consider increasing the sample size and taking a longitudinal approach to data collection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Cambridge Trust and Newnham College, University of Cambridge.