
Abstract
The purpose of the study was to describe trajectories of relationship satisfaction across the transition to parenthood, and identify predictors of these trajectories. This study is based on the Norwegian Mother, Father, and Child Cohort Study (MoBa). Mothers (N = 43,517) reported on their relationship satisfaction at five timepoints from 17 weeks gestation to 5 years postpartum, as well as sociodemographic, psychological, and behavioral covariates. Latent Trajectory Modeling revealed 5 trajectories of relationship satisfaction: “stable very high” (18.05%), “stable high” (43.47%); “stable moderate” (17.21%); “high falling” (3.38%); and “low falling” (4.02%). Predictors of group membership were identified using multinomial logistic regression. Significant predictors included unplanned pregnancy, maternal social support, maternal history of depression, maternal history of abuse, postnatal depression, financial stress, sexual satisfaction, and child negative emotionality. These results may help identify families at risk of declining relationship satisfaction, and aid in targeting interventions aimed at improving satisfaction during this vulnerable transition.
Predictors of Relationship Satisfaction Across the Transition To Parenthood
A high-quality couple relationship serves as an important bedrock for the family system, contributing to the wellbeing of both parents and children (Fishman & Meyers, 2000; Leidy, Parke, Cladis, Coltrane, & Duffy, 2009; Proulx, Helms, Buehler, 2007). Conversely, poor relationship quality takes a toll on the mental health of partners (Don & Mickelson, 2012) and their children (Buehler et al., 1997; Harold & Sellers, 2018). Women may be particularly vulnerable to relationship stressors during the transition to parenthood, when they are at greatest risk of developing depression (Howard et al., 2014). Mental health struggles may, in turn, impinge on spouses’ parenting abilities and lead to even greater family dysfunction (Baranov, Bhalotra, Biroli, & Maselko, 2020; Fishman & Meyers, 2000; Lovejoy, Graczyk, O’Hare, & Neuman, 2000). It is therefore important to understand the determinants of relationship satisfaction during this critical life phase.
Relationship satisfaction tends to decline steadily over time for all couples (VanLaningham, Johnson, & Amato, 2001), but research suggests a sharper decline for couples with children, coinciding with the transition to parenthood (Keizer & Schenk, 2012; Twenge, Campbell, & Foster, 2003). Declines in relationship satisfaction are reported by both partners after the birth of the first child (Mitnick, Heyman, & Smith Slep 2009; Twenge et al., 2003), and number of children has been found to be inversely related to marital satisfaction (Twenge et al., 2003). The vulnerability-stress-adaptation (VSA) model of marriage suggests that variations in marital quality over time are influenced by a combination of partners’ enduring vulnerabilities, the stressful events they face, and their ability to respond adaptively to those stressors (Karney & Bradbury, 1995). The birth of a child, though joyous, constitutes a significant stressful life event, as both members of a couple must adjust to their new roles as parents and grapple with the increased responsibilities, sleep deprivation, and loss of freedom that accompanies parenthood. The addition of a child has been characterized as a “crisis” for couples, as they must necessarily reorganize the family structure around the introduction of a new member (Lawrence, Rothman, Cobb, Rothman, & Bradbury, 2008; LeMasters, 1957). In line with the vulnerability-stress-adaptation model, the transition itself is not likely to be the only influence on couples’ satisfaction during this time. Rather, additional external stressors, existing vulnerabilities, such as partners’ baseline mental health, and the different ways in which couples adapt to this transition are likely to play a role in couples’ satisfaction. Factors that have been associated with greater declines in relationship satisfaction across the transition to parenthood include whether the pregnancy was planned (Lawrence et al., 2008), vulnerabilities including postpartum psychiatric issues (Whisman, Davila, & Goodman, 2011; Zelkowitz & Milet, 1996), stressors such as more challenging infant temperament (Kluwer, 2010; Lawrence et al., 2008), and adaptation issues such as perceived imbalance in division of household labor (Dew & Wilcox, 2011), and low paternal childcare involvement (Lee & Doherty, 2007).
Less is known about how relationship satisfaction may change in the long term, beyond the immediate transition to parenthood. Some studies suggest that relationship satisfaction could recover as children age and parents regain freedoms temporarily lost to the demands of rearing young children. For example, one meta analysis suggested that differences in marital satisfaction between parents and nonparents were greater for parents of infants versus parents of children over two years old (Twenge et al., 2003). Keizer & Schenk (2012) examined relationship satisfaction reported by both partners over a 12-year period and found that parents’ relationship satisfaction followed a u-shaped curve, with declines in marital quality reported after the birth of the first child, followed by subsequent recoveries beginning approximately seven years after the birth of the first child. However, this study examined a single trajectory of relationship satisfaction, and was limited to couples who stayed together over the entire duration of the study. Results of another prospective study suggested that childrearing-related stressors in early childhood can “cast long shadows” over relationship satisfaction in the long term, and eventually predict relationship dissolution (Helland, von Soest, Gustavson, Røysamb, Mathiesen 2014).
To examine longer term changes in relationship satisfaction, and predictors of these changes, it may be important to assess whether the shape of trajectories of relationship satisfaction differs meaningfully between couples—for example, satisfaction may recover for some couples, but not others. Whereas some research has examined predictors of baseline relationship satisfaction and change in satisfaction over time (i.e., intercept, slope, and sometimes quadratic trend, of a common trajectory of relationship satisfaction; Umberson et al. 2005; Lawrence et al. 2008; Keizer & Schenk 2012), less research has examined changes in relationship satisfaction using a latent trajectory approach—that is, allowing for several subgroups following different patterns of relationship satisfaction over time, within the larger population. Proulx and colleagues (2017) conducted a review of studies using such approaches to examine marital quality (including constructs such as satisfaction, happiness, and conflict). Overall, they found evidence for several distinct trajectories of marital satisfaction, including stability, decline, and, less often, recovery (Proulx, Ermer, & Kanter, 2017). Out of 17 studies, only one focused on the transition to parenthood (Don & Mickelson, 2014). This study employed a sample size of 104 couples, followed from pregnancy to 9 months postpartum. The authors found that all couples in the sample experienced decreases in relationship satisfaction over the transition to parenthood, with new mothers following one of two trajectories—moderate decline, or steep decline. More research using this approach is needed, following mothers beyond the immediate postpartum period, to assess trajectories of relationship satisfaction as couples navigate later stages of parenthood.
Given the high rate of divorce and relationship dissolution, and the negative impact of interparental conflict on parent and child wellbeing, identifying factors that predict declines (and potentially, recoveries) in relationship satisfaction may provide a target for prevention and intervention strategies to foster resilience for families during this transition. The aims of the present study were therefore to (1) identify distinct trajectories of relationship satisfaction across the transition to and early years of parenthood in a large cohort of Norwegian women and (2) identify pre- and postnatal predictors and correlates of these trajectories from a wide range of potential covariates across multiple domains, including personal vulnerabilities and external stressors.
Method
Sample
Data were drawn from the Norwegian Mother, Father, and Child Cohort Study (MoBa), a population-based pregnancy cohort study conducted by the Norwegian Institute of Public Health (Magnus et al., 2016). Participants were recruited from all over Norway from 1999 to 2008. The women consented to participation in 41% of the pregnancies. The cohort now includes 114,500 children, 95,200 mothers and 75,200 fathers. The current study is based on version 12 of the quality-assured data files released for research in 2020. The establishment of MoBa and initial data collection was based on a license from the Norwegian Data Protection Agency and approval from The Regional Committees for Medical and Health Research Ethics. The MoBa cohort is now based on regulations related to the Norwegian Health Registry Act. The current study was approved by The Regional Committees for Medical and Health Research Ethics (#2013/2061). Participants were recruited by a postal invitation sent in advance of a routine ultrasound offered to all pregnant women in Norway at 17–18 weeks gestation. Paper questionnaires were sent by post at each time point. Participants differed from non-participants on several variables, with women younger than 25 years, women with more than two previous births, smokers, and those with pregnancy and birth complications underrepresented in the MoBa sample (Nilsen et al., 2009). In order to focus on the transition to parenthood among first-time mothers and their married or cohabiting partners, we excluded women who already had at least one child, and those who did not live with the father of the baby at the time of recruitment, resulting in a final sample size of N = 43,517.
Measures
Relationship Satisfaction
Mothers reported on relationship satisfaction at six time points (17 weeks gestation; 30 weeks gestation; 6 months postpartum; 18 months postpartum; 36 months postpartum; and 5 years postpartum) using a 5-item version of the Relationship Satisfaction Scale, developed for use in the MoBa study. Mothers rated how well each statement (“I am very happy with our relationship”; “My partner is generally understanding”; “I am satisfied with my relationship with my partner”; “my partner and I have problems in our relationship” (reversed); “we agree on how our child should be raised”) described their relationship on a 6-point scale (from “agree completely” to “disagree completely”). The 10-item version of the scale has demonstrated good psychometric properties in previous research, including good internal consistency (Røysamb et al., 2014) and high convergent validity with the Quality of Marriage index (Norton, 1983), a widely used measure of marital quality (Dyrdal, Røysamb, Nes, & Vittersø, 2011; Røysamb et al., 2014), and has also been shown to predict future breakup/divorce (Røsand, Slinning, Røysamb, & Tambs, 2013). The 5-item version was empirically derived by selecting, using multiple regression and factor analysis, the items which explained most of the variance in the full index; the resulting short version correlates 0.97 with the original scale (Røysamb, Vittersø, & Tambs, 2014). The mean rating at each time point was used in trajectory analysis (described below).
Mothers were asked about their relationship status at each timepoint; however, phrasing of the questions differed slightly between timepoints. Mothers were therefore considered to have divorced or separated if they reported, at 6 months postpartum, that they did not have a boyfriend, spouse, or partner, or if they reported that they were not living with a boyfriend/spouse/partner at 18 months, 36 months, or 5 years postpartum.
Predictors and Correlates
The following variables were considered as predictors and correlates of relationship satisfaction across the transition to parenthood.
17 weeks gestation
Length of the relationship was assessed at the time of recruitment by asking participants how long they had had a sexual relationship with the baby’s father. Participants reported on their marital status—for the present study we compared mothers who were married vs. cohabiting with the baby’s father during the pregnancy. Maternal and paternal education were assessed, comparing parents who had completed education beyond high school to those who had not.
Mothers reported their usual work schedules; hours of work per week was categorized into four groups (<22.5 hours; 22.6–30 hours; 30.1–37.5 hours; >37.5 hours) based on previous work with this sample (Kristensen, Nordhagen, Wergeland, & Bjerkedal, 2008). Mothers’ work-related stress was assessed using 8 items, for example, “my work is very stressful”; “my work demands a lot of me”; “I learn a lot at work” (reversed). Participants responded to each statement on a 4-point scale (“agree”; “mostly agree”; “mostly disagree”; “disagree”); item scores were summed to create a total work stress score.
Both partners reported their gross income before taxes; we considered families to have low income if they reported a combined gross income of less than 300,000 NOK per annum, based on previous work (Winkvist et al., 2015). As a second measure of financial stress, participants were asked whether it was possible for the household to manage without the pregnant partner’s income (dichotomized; “yes”/“no”).
Expectant mothers’ alcohol use in the first trimester of pregnancy was self-reported and categorized according to previously established guidelines (Never; 1–3 times per month; 1 time per week or more; Kvalevaag et al., 2013) Smoking was also self-reported (yes/no).
Social support was assessed via three questions: “Do you have anyone other than your husband/partner you can ask for advice in a difficult situation”; “How often do you meet or talk on the telephone with your family (other than your husband/partner and children) or close friends?” and “Do you often feel lonely?” with responses on a three-point scale. We defined social support as the mean of responses to these questions, as in previous work (M. C. Magnus et al., 2018).
Maternal history of depression was assessed using the Kendler Lifetime History of Depression Scale (Kendler, Neale, Kessler, Heath, & Eaves, 1993), which asks participants if they have experienced each of 5 common symptoms of depression (“felt depressed or sad”; “had problems with appetite or eaten too much”; “been bothered by lack of energy”; “blamed yourself and felt worthless”; “had problems with concentration or had problems making decisions”), for 2 weeks or more, at any point over the lifetime. In accordance with DSM-III criteria, those who reported having experienced 3 or more symptoms simultaneously (necessarily including the first symptom relating to feelings of sadness/depression) were considered to have a history of depression. Maternal lifetime history of physical and sexual abuse was assessed by asking participants to agree or disagree with the following statements: “you have been subjected to physical abuse”; “you have been forced to have sexual intercourse.”
Finally, we also considered whether the pregnancy was planned or unplanned, as reported by mothers at intake.
30 weeks gestation
Mothers were asked whether they had experienced each of 8 specific adverse events (e.g., “have you lost someone close to you”; “have you been involved in a serious traffic accident, house fire, or robbery”) in the past 12 months, as well as how severely they had been affected by it (“Not too bad”; “painful/difficult”; “very painful/difficult”)
Postpartum predictors
Infant sleep duration was assessed at 6 months with the question “How many hours in total does your child sleep per 24 hours?” (response options: “less than 8 hours,” “8-10 hours” ’11-13 hours,” “13-14 hours,” “more than 14 hours”). Due to small cell sizes, the first two response options (<8 hours, 8–10 hours) were collapsed for analyses. Child temperament was assessed at 6 months using 7 items from the “fussy/difficult” subscale of the Infant Characteristics Questionnaire (ICQ-6). Respondents rated each statement (e.g., “the child is easily upset”; “the child requires a lot of attention”) on a 7-point scale from “completely disagree” to “completely agree.” Difficult temperament at 18 months was assessed using the “Emotionality” subscale of the Emotionality, Activity, and Shyness questionnaire (EAS; Mathiesen & Tambs, 1999). This subscale is made up of 3 statements pertaining to children’s displays of anger and sadness (e.g., “your child reacts intensely when upset”), with response options on a 5-point scale from “very typical” to “not at all typical.” Item scores are summed to create a total emotionality score, with higher scores indicating less emotionality.
Maternal postnatal depression/anxiety was assessed at 6 months using a shortened form of the Symptom Checklist (SCL-8; Tambs & Røysamb, 2014). Family financial stress was assessed at the chronic (difficulty meeting basic needs) and acute level (difficulty paying a large unexpected bill) at 6 months postpartum.
At 18 months postpartum, mothers reported on the length of their maternity leave as well as the length of their partner’s parental leave, in weeks. For the purpose of the present study, we converted length of leave to months. Mothers reported on their satisfaction with the sexual relationship using the question: “how satisfied are you with your sex life,” with response options on a 5-point scale from “very dissatisfied” to “very satisfied.” We also considered mothers’ subsequent pregnancy, self-reported at 18 and 36 months postpartum.
Analysis
To identify groups of mothers with distinct profiles of relationship quality over time, latent class growth modeling (LCGM) was conducted using the TRAJ procedure in Stata. This procedure allows for unequal spacing between measurements (Jones, Nagin, & Roeder, 2001), as was the case for this study, and handles missing data using full information maximum likelihood. Participants were included in the trajectory modeling if they (a) were cohabiting or married for the duration of the study period and (b) had at least 1 prenatal and 1 postnatal measure of relationship satisfaction. The final trajectory model was selected based on 3 criteria: (1) Maximizing the Bayesian Information Criterion (BIC) value; (2) Ensuring average posterior probabilities of at least 0.70 in each class; and (3) interpretability/utility of the groups. Women who reported divorce or separation during the study period were not included in the trajectory models, but served as their own group in predictive models.
Predictors and correlates of group membership were examined using multinomial logistic regression, using the modal group as the reference category.
Attrition in MoBa, particularly as it relates to relationship satisfaction, has been previously described (see Gustavson, Nilsen, Ørstavik, Røysamb 2014). Mothers with missing information at 5 years postpartum tend to have lower levels of education, are less likely to be married, and report slightly lower relationship satisfaction (with missingness accounting for approximately 0.1% of the variance in relationship satisfaction) compared to mothers who responded to the 5-year questionnaire (Gustavson et al., 2014). To account for missing data (due to attrition or non-response) on predictors and covariates (ranging from 1.47% for low income at 17 weeks to 58.55% for difficulties coping with unexpected bills; see supplementary Table S1), we employed multiple imputation by chained equations, with relationship satisfaction included as an auxiliary variable; estimates were pooled across 10 imputed datasets. Predictors were entered hierarchically based on time of assessment, beginning with those measured at 17 weeks gestation.
Results
Trajectories of Relationship Satisfaction
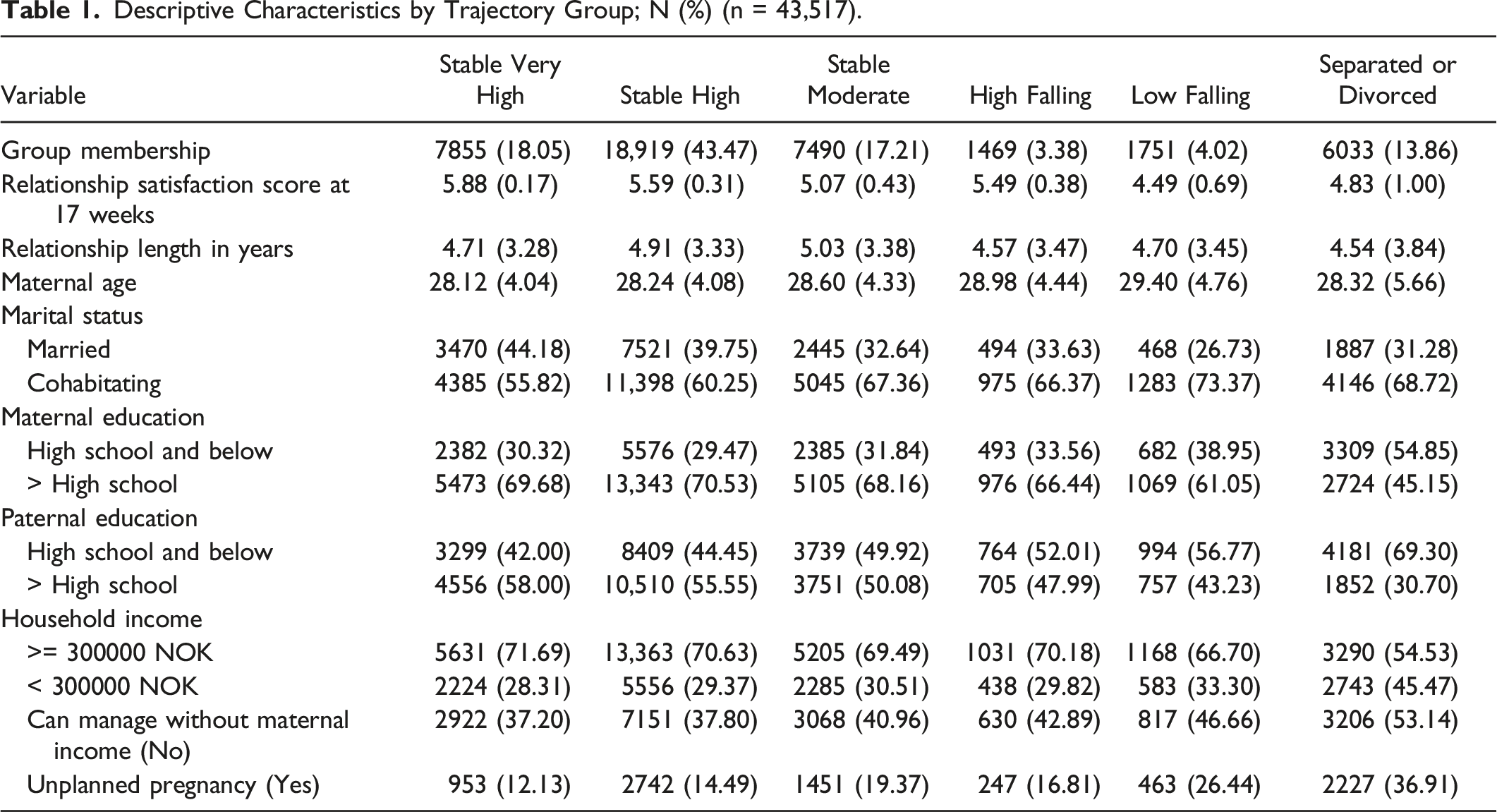
Based on the criteria identified above, we identified 5 trajectories of relationship satisfaction across the transition to parenthood (Figure 1). Details on model selection are shown in supplementary Table S2. The five trajectories represented “stable very high” (18.05%), “stable high” (43.47%); “stable moderate” (17.21%); “high falling” (3.38%); and “low falling” (4.02%) satisfaction. Descriptive statistics for the five groups, plus the group of mothers who reported divorce or separation during the study period (13.86%), are presented in Table 1. Trajectories of Relationship Satisfaction between 17 weeks’ Gestation and 5 Years Postpartum. Descriptive Characteristics by Trajectory Group; N (%) (n = 43,517).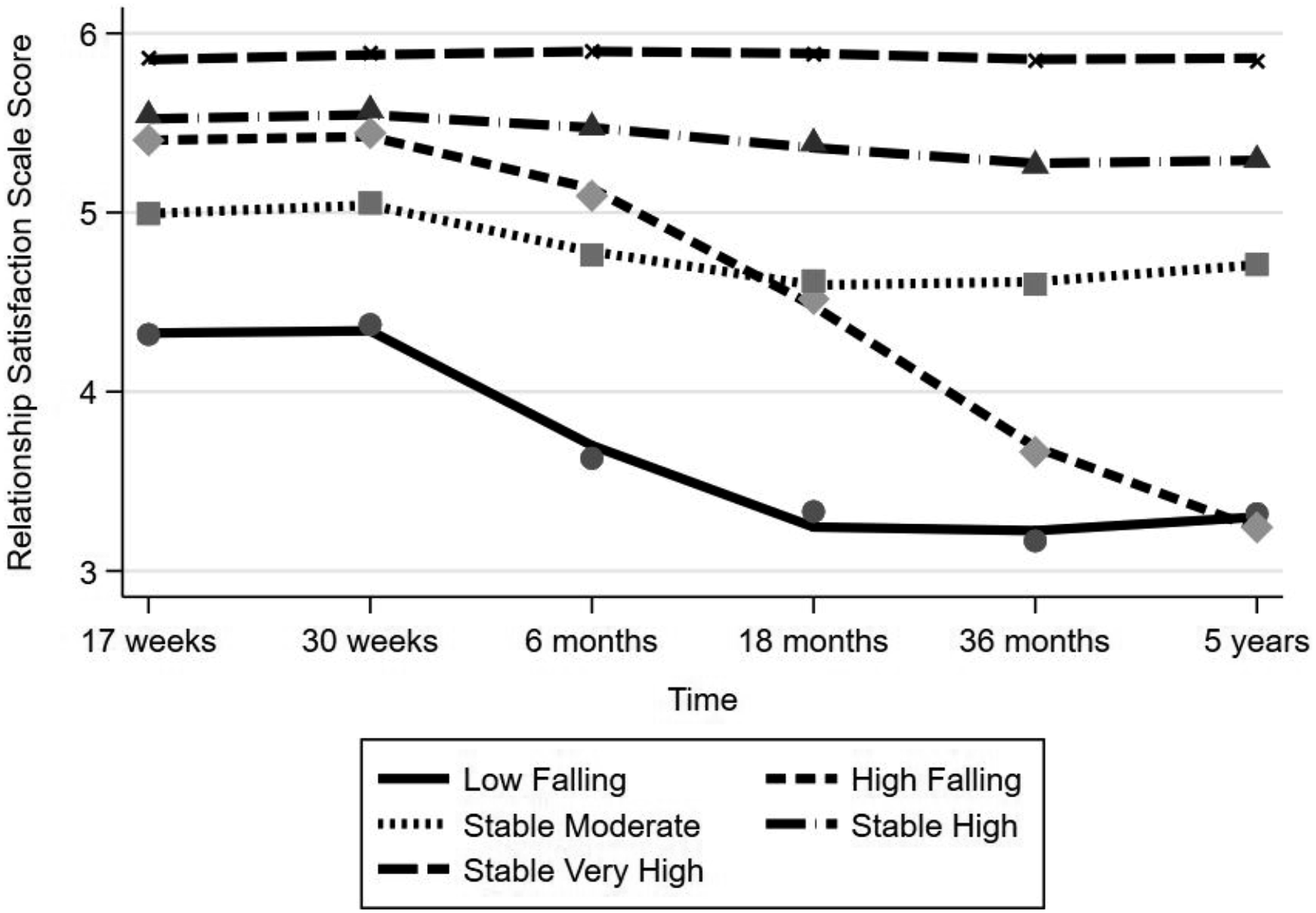
Predictors and Correlates of Trajectory Membership
Summary of Hierarchical Multinomial Regression Analyses with Relative Risk Ratio Estimates (Stable High as Reference Group).
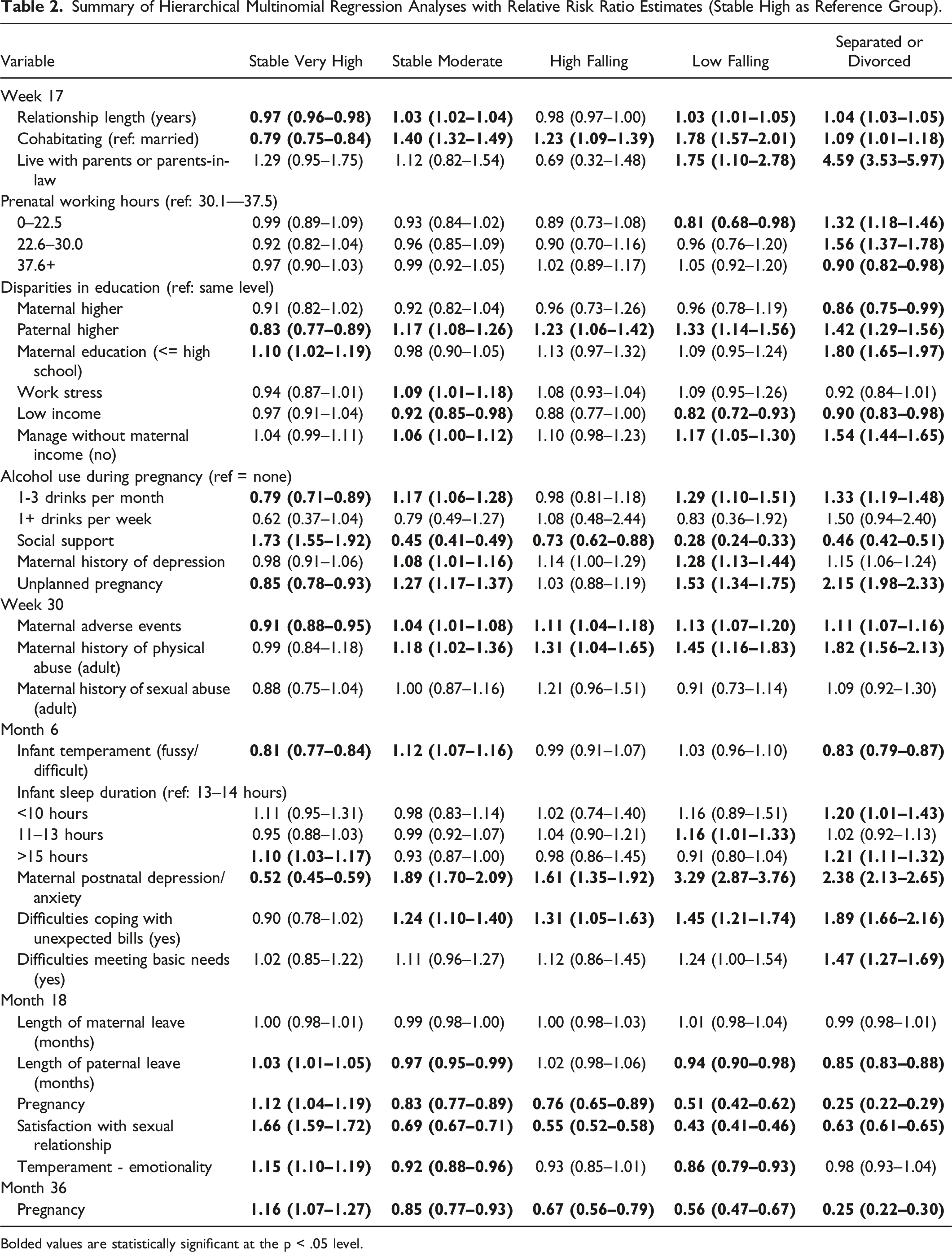
Bolded values are statistically significant at the p < .05 level.
In the postnatal period, postnatal depression/anxiety, financial stress, shorter infant sleep duration and toddler negative emotionality were associated with membership in trajectories characterized by lower or declining relationship satisfaction, and negatively associated with membership in the “very high” satisfaction trajectory. Satisfaction with the sexual relationship and subsequent pregnancy at 18 months were predictive of membership in the “very high” satisfaction trajectory, and protective against lower or declining relationship satisfaction; longer paternal leave was protective against lower relationship satisfaction and divorce.
Discussion
Using data from 43,517 mothers in a large, prospective birth-cohort study, we identified five distinct trajectories of relationship satisfaction across the transition to parenthood. We identified several predictors of these trajectories, which may be amenable to intervention.
Results suggested that Norwegian mothers are, overall, happy with their relationships. Importantly, most mothers in the sample appeared to experience stable relationship satisfaction across the transition to parenthood. This runs contrary to what was expected based on cross-sectional studies comparing parents to nonparents (Twenge et al., 2003), and on longitudinal studies using US data (Umberson et al., 2005). This somewhat surprising result may be due in part to the Norwegian context: Scandinavian countries, and Norway in particular, are known for relatively generous family leave policies when compared with the US and other Western countries (Perez, 2019). In fact, enhancing women’s labor force participation while increasing men’s family involvement has been cited as a central goal of Norwegian work-family policies (Kitterød & Lappegård, 2012). More generous parental leave policies, in turn, tend to be associated with smaller differences in happiness between parents and nonparents (Glass, Simon, & Andersson, 2016; Pollmann-Schult, 2018). However, overall declines in satisfaction post birth have been found for couples in the US, the UK, the Netherlands, and Germany, despite differing family leave policies between these countries (Kluwer, 2010). As compared to other Western countries, (e.g., U.S., Canada, and the U.K.), Norway and other Scandinavian countries have notably more egalitarian division of unpaid work between spouses, a factor that has been associated with female partners’ relationship satisfaction at the couple level (Greenstein, 2009; Miranda, 2011). Relative equality between partners in the Norwegian national context may partly explain the high, stable levels of relationship satisfaction reported by most mothers in the present study.
We noted that in our sample, longer parental leave among fathers was negatively associated with membership in trajectories characterized by lower levels of satisfaction, as well as with divorce. Norman at al. (2018) reported that fathers’ caring for infants in the first year, without the mother present, was protective against later relationship breakdown. Fathers who take longer parental leave are also more likely to be involved in childcare later on (Adema, Clarke, & Frey, 2015). Length of paternity leave may, therefore, have served as a proxy measure of fathers’ overall engagement in childrearing—and, consequently, a reduction in mothers’ overall unpaid labor burden (a factor related to mothers’ relationship satisfaction; Greenstein, 2009; Oshio, Nozaki, & Kobayashi, 2013). Though the Norwegian national context is characterized by relative equity between partners, relative deprivation theory (Crosby, 1976) suggests that inter-household differences in division of unpaid labor may nonetheless explain differences in relationship satisfaction, as individuals judge the relative fairness of their own situations as compared to national norms (Greenstein, 2009). In light of these findings, encouraging fathers to make use of paternity leave may have long lasting impacts on families. Data from the Swedish Institute of Labor Market Policy Evaluation suggests that each additional month of paternity leave is associated with a 7% increase in future earnings for mothers (Perez, 2019). In terms of encouraging uptake, “use it or lose it” paternity leave policies (i.e., those with portions of parental leave reserved exclusively for the father, non-transferrable to the mother) are linked to greater use of paternity leave by fathers (Adema et al., 2015).
The level of social support available to mothers (outside of the couple relationship) was found to be robustly protective against poor and declining relationship quality. This finding is in keeping with previous research indicating that social support outside of the marital relationship is associated with greater relationship satisfaction (Kurdek, 2005; Scheidler, 2008). According to the vulnerability-stress-adaptation model, partners’ external social support represents an adaptive process that may buffer against the negative effects of stress on the relationship—a hypothesis that has been substantiated through research in populations experiencing significant stress due to health problems (Steiner, Bigatti, Hernandez, Lydon-Lam, & Johnston, 2010; Unger et al., 1996), or demanding work schedules (Scheidler, 2008). However, it is also plausible that mothers’ social support is a marker of their ability to form and maintain close relationships.
In addition to support within and outside of the couple, unplanned pregnancy was predictive of membership in trajectories characterized by poorer relationship adjustment, as has been shown in previous literature (Cox, Paley, Burchinal, & Payne, 1999). Events, even joyful ones, that occur “off-time” (i.e., out of synch with one’s expectations or plans) are thought to be stressful (Neugarten, 1979)—unplanned pregnancy may therefore represent an additional stressor for couples who did not consider themselves “ready” for parenthood. Alternately, unplanned pregnancy may be an indicator of a less stable or serious relationship at baseline, as couples facing a planned pregnancy tend to express more commitment to the relationship (Schwerdtfeger, Todd, Oliver, & Hubler, 2013). In the same vein, cohabiting (versus being married) was associated with poorer and declining relationship satisfaction in our sample. Previous research has suggested that married couples report higher levels of relationship satisfaction than cohabiting couples, but that this difference is attenuated when couples’ future marital intentions are taken into account (Tai, Baxter., & Hewitt, 2014). Public health programs targeted to couples facing unplanned pregnancies may help bolster relationship quality during this transitional period.
Maternal depression in the perinatal period is a known risk factor for offspring mental health and behavior problems (Stein et al., 2014), and may also impinge on family functioning (Tammentie, Tarkka, Åstedt-Kurki, Paavilainen, & Laippala, 2004). In the present study, maternal postnatal depression predicted membership in the moderate satisfaction, high falling, low falling, and divorced groups, compared to the stable high group, over and above mothers’ history of depression prior to pregnancy. Bidirectional associations have been noted between postnatal depression and relationship satisfaction: a new mother’s depression can take a toll on her ability to engage with her partner as usual, but inter-partner dynamics, including the level of perceived partner support during the transition to parenthood, can also impact the development and severity of postpartum depression (Barnes, 2006).
One of the many challenges faced by new parents is the reorganization of family structures around the introduction of a new member (LeMasters, 1957). As children grow, they become important contributors to family dynamics (Crouter & Booth, 2003), including their parents’ relationship dynamics. In support of this notion, we found that child temperament at 18 months was robustly associated with trajectories of relationship satisfaction: mothers of children lower in negative emotionality were more likely to be characterized by “very high” relationship satisfaction, and less likely to follow moderate or falling trajectories. Infant fussy temperament was similarly associated with these trajectories in the crude model, but these associations were attenuated once later temperament was included in the adjusted model. Child temperaments characterized by negative affect may be a significant source of stress to parents, which may spill over into the couple relationship (Mehall, Spinrad, Eisenberg, & Gaertner, 2009). In a similar vein, infants sleep duration was a robust predictor of trajectory membership in unadjusted models: having an infant who slept less than 12–13 hours per 24 was associated with membership in trajectories characterized by lower relationship satisfaction, as well as with divorce/separation. These relationships were attenuated in the adjusted model, but having an infant who slept less than 10 hour per 24 was significantly associated with membership in the divorced/separated group. Paradoxically, mothers of infants who slept more than 14 hours a day were overrepresented in both the “stable very high” and “divorced/separated” groups. Infant sleep quality has been found to impact parents’ sleep quality and mood (Meltzer & Mindell, 2007), and some studies have shown associations between poor infant sleep quality and diminished quality of co-parenting (McDaniel & Teti, 2012) and lower relationship satisfaction (Ricci, Parra-Robledo, Rothernbacher, Diaz-Morales, & Genuneit, 2020). However, as evidence comes mostly from small samples (i.e., < 200 participants), more investigation in population-based samples is needed to clarify associations and mechanisms, particularly longitudinally.
The physical changes of pregnancy and the postpartum period, as well as psychosocial changes associated with the transition to parenthood, often bring changes to the couple’s sexual relationship (Abdool, Thakar, & Sultan, 2009; Hipp, Kane Low, & Van Anders, 2012). In this study, we found that mothers’ satisfaction with their sexual relationship at 18 months postpartum was robustly protective against low and declining relationship satisfaction. Previous longitudinal research has suggested that greater sexual satisfaction may attenuate declines in marital satisfaction over time (McNulty, Wenner, & Fisher, 2016). Notably, this relationship is likely to be bidirectional, as higher levels of relationship satisfaction also lead to greater sexual satisfaction over time (McNulty et al., 2016). Contextual factors specific to the postpartum period, including the birth experience, breastfeeding, and sleep disturbance may impinge on sexual functioning (Abdool et al., 2009; Hipp et al., 2012), and in turn, on relationship satisfaction during the transition to parenthood.
Strengths and Limitations
The present study has considerable strengths, including the large sample size, use of latent class trajectory modeling, and inclusion of a wide variety of pre-and postnatal correlates of relationship trajectories. Nevertheless, the following limitations must be considered. First, we examined mothers’ reports of relationship satisfaction; it is possible that fathers’ relationship satisfaction may be differently associated with the transition to parenthood (see Keizer & Schenk). However, Kurdek (2005) found that the processes affecting marital satisfaction were largely the same for male and female partners. Second, our sample consisted of heterosexual couples and their biological children; future work examining these processes should ideally include other family types. Third, relationship satisfaction and predictors were assessed during the same time frame. Therefore, the direction of the effects cannot be determined. For many of the constructs assessed, such as sexual satisfaction, associations with relationship satisfaction are likely to be bidirectional. Fourth, most covariates were assessed at a single time point, but are likely to have themselves varied over the course of follow-up. For example, mothers’ social support was assessed during pregnancy, but not after birth. Though we assume some level of stability in social support over time, it is possible that women’s relationships may change significantly after the birth of their first child, and that the support these relationships provide may also change. Other constructs, for example, work stress, are also likely to have varied over the time frame of the study—a factor we were not able to assess in the present study. Finally, the mothers reported on their own relationship satisfaction as well as on key predictors, including mental health. This may result in confounding due to shared method variance or reporting bias (Kolstad et al., 2011). For example, women who were experiencing symptoms of depression may have been more likely to report poor relationship quality.
Implications and Conclusions
Interventions to bolster relationship functioning during the transition to parenthood have proven protective against declines in relationship satisfaction post-birth (Doss, Cicila, Hsueh, Morrison, & Carhart, 2014), and have shown secondary benefits for offspring mental health, including reduced externalizing symptomatology in toddlerhood (Tomfohr-Madsen et al., 2020). The present study has identified particular characteristics which may put couples at risk for declining trajectories of relationship satisfaction, as well as plausibly modifiable factors that may buffer against such risk. These factors may represent additional targets for intervention aimed at improving family dynamics during this vulnerable period.
Supplemental Material
Supplemental Material—Predictors of Relationship Satisfaction Across the Transition to Parenthood: Results from the Norwegian Mother, Father, and Child Cohort Study (MoBa)
Supplemental Material for Predictors of Relationship Satisfaction Across the Transition to Parenthood: Results from the Norwegian Mother, Father, and Child Cohort Study (MoBa) by Mila Kingsbury, Zahra Clayborne, Wendy Nilsen, Fartein Ask Torvik, Kristin Gustavson, and Ian Colman in Journal of Family Issues
Footnotes
Acknowledgments
The Norwegian Mother, Father and Child Cohort Study is supported by the Norwegian Ministry of Health and Care Services and the Ministry of Education and Research. We are grateful to all the participating families in Norway who take part in this on-going cohort study. The present study was partially supported by the Research Council of Norway (RCN; project # 218373) and through RCN’s Centres of Excellence funding scheme, project # 262700, RCN’s guest research program, and the Canada Research Chairs program for IC. WN was funded by RCN (project # 296770). The consent given by the participants does not allow for storage of data on an individual level in repositories or journals. Researchers who want access to data sets for replication should submit an application to ![]() . Access to data sets requires approval from The Regional Committee for Medical and Health Research Ethics in Norway and an agreement with MoBa.
. Access to data sets requires approval from The Regional Committee for Medical and Health Research Ethics in Norway and an agreement with MoBa.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canada Research Chairs and Norges Forskningsråd (218373, 262700, 296770).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.