
Abstract
Infertility and its treatment are associated with a host of negative emotions, including perceived injustice. However, no quantitative study has examined the link between perceived injustice and psychological difficulties in couples seeking fertility treatment. This study examined the associations between perceived injustice and both partners’ psychological well-being and investigated possible differences in perceived injustice based on sex or cause of infertility. Both partners of 103 couples seeking fertility treatment completed the Injustice Experience Questionnaire—Infertility, the Hospital Anxiety and Depression Scale, and the Fertility Quality of Life Tool. Perceived injustice was associated with one’s own and one’s partner’s higher depressive symptoms and lower infertility-related quality of life, as well as one’s own higher anxiety symptoms. Women also perceived more injustice than men. The cause of infertility was unrelated to perceived injustice. Findings suggest that perceived injustice could represent an intervention target to reduce psychological distress in infertile couples.
Keywords
Infertility and assisted reproduction technology are known to disrupt individuals’ relational functioning, psychological well-being, and overall quality of life (for a review, see Luk & Loke, 2015). Indeed, numerous studies have reported high rates of both anxiety and depressive symptoms as well as lower relationship and life satisfaction in men and women seeking fertility treatment (Galhardo, Cunha, Pinto-Gouveia, & Matos, 2013; Greil et al., 2018; Luk & Loke, 2015; McQuillan, Torres Stone, & Greil, 2007; Péloquin & Lafontaine, 2010; Verhaak, Lintsen, Evers, & Braat, 2010). The psychological distress experienced by infertile couples can be attributed to several factors, including being deprived of the normative experience of becoming a parent as well as the stress associated with the treatment itself—that is, treatments tend to be intrusive on many aspects of couples’ lives, and are often accompanied with multiple losses and treatment failures (Maroufizadeh, Karimi, Vesali, & Omani Samani, 2015). Some studies, however, have reported no significant differences in terms of psychological well-being in infertile couples compared to fertile couples (for reviews, see Péloquin & Lafontaine, 2010 and Verhaak et al., 2007), suggesting that there is considerable variability in the experience of infertility. In order to address the specific needs of infertile couples, it is crucial to better understand the factors that may contribute to these differences in partners’ emotional adjustment in the context of infertility.
Infertility has often been described as an emotional roller coaster (Boden, 2007; Hanna & Gough, 2016; Jacobs & O’Donohue, 2007), involving feelings of isolation, stigma, anger, loss, as well as blame and perceived injustice (Borghi et al., 2018; Hjelmstedt et al., 1999; Péloquin, Brassard, Arpin, Sabourin, & Wright, 2018; Raque-Bogdan & Hoffman, 2015; Steuber & Solomon, 2011). Perceived injustice is defined as a set of cognitions comprising elements of irreparability of loss, attributions of blame, severity of loss consequent to a negative experience, and a sense of unfairness (Sullivan, 2008). It has been associated with poorer physical and psychological health, including higher levels of anxiety and depression, anger, hostility, and guilt among community samples (Bezrukova, Spell, & Perry, 2010; Doosje, Branscombe, Spears, & Manstead, 1998; Smith, Parrott, Ozer, & Moniz, 1994). In clinical samples of patients with chronic pain (Sullivan et al., 2008), fibromyalgia (Rodero et al., 2012) and genito-pelvic pain (Pâquet et al., 2016), perceived injustice has also been associated with depressive symptoms and pain, as well as significant impairments in daily functioning.
The clinical literature and qualitative studies have suggested that perceived injustice is a common experience among couples faced with fertility issues (Genesse, Bécotte, Brassard, Purcell-Lévesque, & Péloquin, 2019; Hjelmstedt et al., 1999; Ohl et al., 2009; Williams, 1997). Experiencing infertility could indeed be considered unfair given that most couples are able to achieve a pregnancy without significant difficulties or having to go through the ordeal of assisted reproduction. However, to our knowledge, no quantitative studies have examined the perception of injustice and its association with psychological well-being in couples undergoing fertility treatment. Given that perceived injustice has been associated with worse psychological and physical outcomes in other health populations, understanding its role in the psychological well-being of infertile couples and the factors that may contribute to perceiving injustice seems highly justified.
Perceived injustice may be experienced differently by men and women in the context of infertility. In the context of infertility, women have been found to react more negatively, and to experience more depression, anxiety, and stress than men (for reviews, see Luk & Loke, 2015 and Ying, Wu, & Loke, 2015), suggesting that women may be more likely to perceive injustice. Nonetheless, most studies examining psychological well-being in the context of infertility have focused solely on women’s perspective, limiting our understanding of the emotional experiences of men (Wischmann & Thorn, 2013). Among the few qualitative studies examining perceived injustice in this context, Hjelmstedt et al. (1999) found that both men and women described experiencing injustice with regards to their infertility. However, Genesse et al. (2019) found that this perception was only reported by women. These conflicting findings suggest that examining the extent to which men and women may differ with respect to perceived injustice is warranted.
The cause of infertility is another factor that may affect the extent to which partners perceive injustice. Infertility can be attributed to female factors (e.g., anovulation), male factors (e.g., low sperm count), a combination of factors in both partners, or it can be unexplained. It could be postulated that an individual would perceive higher injustice when their partner is diagnosed with the fertility problem, compared to when he or she is responsible for the couple’s inability to conceive. Indeed, men and women can blame their partner for the fertility problem (Abbey, Andrews, & Halman, 1991; Péloquin et al., 2018). Alternatively, not knowing the cause of the infertility may also increase one’s sense of unfairness regarding the situation compared to when there is an identifiable cause. Research examining the cause of infertility and psychological well-being has yielded inconsistent results. Whereas some studies have found that the cause of infertility was not associated with the intensity of the emotional responses to infertility (Hjelmstedt et al., 1999; Holter, Anderheim, Bergh, & Möller, 2007; Peronace, Boivin, & Schmidt, 2007; Souter, Hopton, Penney, & Templeton, 2002), others have found that male-factor and unexplained infertility were associated with psychological distress and quality of life (Chan, Chan, Chan, Ng, & Ho, 2015; Connolly, Edelmann, & Cooke, 1987; Nachtigall, Becker, & Wozny, 1992; Newton, Sherrard, & Glavac, 1999; Smith et al., 2009; Zurlo, Cattaneo Della Volta, & Vallone, 2018). To our knowledge however, no study has looked at the association between the cause of infertility and perceived injustice.
Goals of the Study
The primary aim of this study was to examine the association between perceived injustice and both partners’ psychological well-being in the context of assisted reproduction. We used a dyadic design, allowing us to investigate the effects of both partners’ perceived injustice on each other’s psychological well-being. Whereas the majority of studies on infertility has focused solely on women’s experiences, previous research has underscored the importance of studying infertility from a dyadic perspective (Donarelli, Kivlighan Jr, Allegra, & Lo Coco, 2016; Péloquin et al., 2018; Peterson, Pirritano, Christensen, & Schmidt, 2008). Our main hypothesis was that one’s perceived injustice would be associated with one’s own higher levels of anxiety and depression and lower infertility-related quality of life. The association between one’s perception of injustice and their partner’s psychological well-being was also explored. The secondary objectives of this study were to examine possible differences based on sex or cause of infertility with respect to perceived injustice.
Materials and Methods
Study Design
The couples were recruited in four Canadian fertility clinics and through social media. A research assistant planned a phone meeting with interested couples to provide them with information about the study and verify their eligibility. Partners were informed that their data would be published in a journal article and were free to consent to the study. Both partners of eligible couples received an email including an individualized link to sign the online consent form and complete the questionnaires independently through a secure online research platform. Each couple received a compensation of $20 CAN for their participation in the study.
Participants
The sample consisted of 103 mixed-sex couples who were seeking fertility treatment. The inclusion criteria were: (a) at least 18 years of age, (b) good understanding of French or English, and (c) both members of the couple willing to participate and complete the questionnaires. Single mothers and same-sex couples were not eligible to participate. While we recognize that these individuals may also experience fertility-related difficulties, their experiences, including the additional barriers they may face (e.g., stigma, injustice unrelated to infertility, and non-medical reasons for infertility) could significantly differ from those of mixed-sex infertile couples. Moreover, the measures used in this study may not be appropriate for all couples of sexual minorities or single mothers, given that they imply medical infertility.
Measures
Demographic Characteristics and Clinical Information
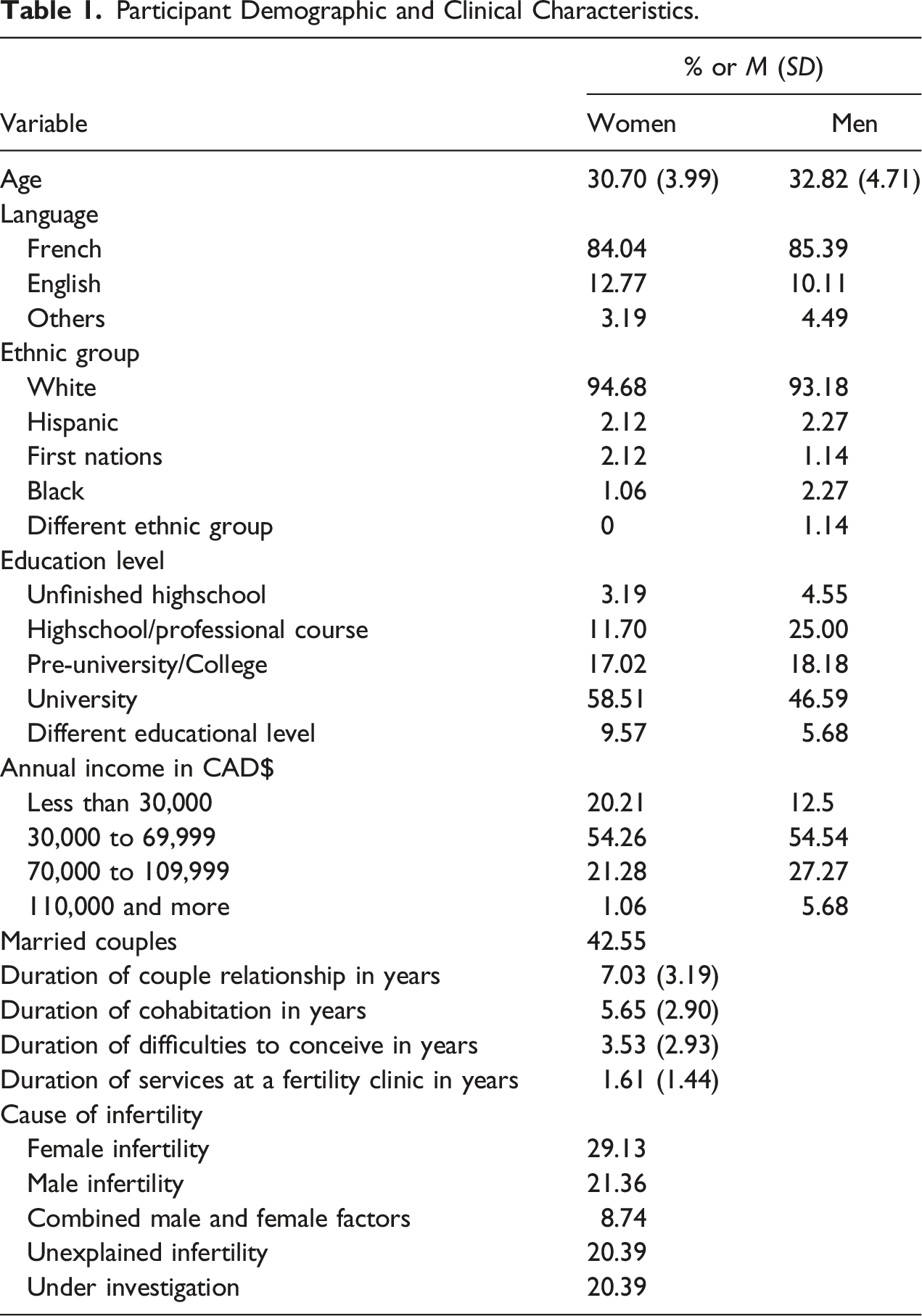
Participants’ sex, age, ethnic group, level of education, employment, income, relationship status, and duration were collected. Data on the cause and duration of infertility, diagnosis, duration of treatments, use of medication, previous pregnancies, and history of psychological treatment was also obtained.
Perceived Injustice
Perceived injustice was measured using the Injustice Experience Questionnaire–Infertility (IEQ-I), which we adapted from the Injustice Experience Questionnaire (IEQ; Sullivan, 2008) originally developed in the context of musculoskeletal injuries. The IEQ-I comprised six items assessing the severity of the loss, the sense of unfairness, and the experience of an irreparable loss (e.g., “I feel as if I have been robbed of something very precious”). Items were rated on a 5-point scale (i.e., from “0 = Not at all” to “4 = All the time”). An exploratory factor analyses with the maximum likelihood method yielded a one-factor solution, explaining 60.43% of the variance. The KMO index (0.880) and Bartlett’s Test of sphericity (χ2 [15] = 644.76, p < .001) supported the sampling adequacy of the data. Factor loadings ranged from 0.61 to 0.87. A total score was created using the sum of all items (range: 0–24), with higher scores indicating higher perceived injustice. The original IEQ has excellent internal consistency (α = 0.92) and good construct validity (Sullivan et al., 2008). The internal consistency for the IEQ-I in our sample was high (α = 0.87 for women, α = 0.88 for men).
Anxiety and Depression Symptoms
The Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983; French translation by Savard, Laberge, Gauthier, Ivers, & Bergeron, 1998) was used to measure anxiety and depressive symptoms. The HADS was designed for use in medical populations. It comprised 14 items that were rated on a 4-point scale (from 0 to 3). A score for each subscale was calculated by summing the items. Subscale scores ranged from 0 to 21, with higher scores reflecting higher depression and anxiety. Both the English and French versions have good psychometric properties (internal consistency varying from 0.67 to 0.93; Bjelland, Dahl, Haug, Neckelmann, 2002; Roberge et al., 2013). In this study, the internal consistency was also good (Depression: α = 0.84 for women, α = 0.80 for men and Anxiety: α = 0.83 for women, α = 0.78 for men).
Infertility-Related Quality of Life
The Fertility Quality of Life Tool (FertiQol; Boivin, Takefman, & Braverman, 2011) is a measure of quality of life in individuals experiencing fertility problems. The instrument comprised 36 items (24 core items measuring emotional, relational, social, cognitive, and physical quality of life, 10 items assessing treatment environment and tolerability, and 2 items measuring overall and physical health). This study focused only on the 24 core items measuring the impact of fertility problems on quality of life. Items are rated on a 5-point scale (from 0 to 4) and transformed into scaled scores, ranging from 0 to 100. Higher scores indicated a higher quality of life related to infertility. The FertiQoL has excellent internal consistency for the core items (α = 0.92; Boivin et al., 2011). In our sample, the internal consistency for the core items (infertility-related quality of life) was also excellent (α = 0.91 for women, α = 0.89 for men).
Statistical Analyses
Preliminary analyses were performed with SPSS 25. Variables were normally distributed, with the exception of women’s quality of life and men’s anxiety and depressive symptoms. Nonparametric bootstrapping was used in the main analyses to account for the non-normality of these variables. Missing data were replaced by simple imputation using the expectation-maximization algorithm (EM) in SPSS. Potential covariates among demographic and medical variables were examined using correlations and repeated measures Analysis of Variance (ANOVA).
To examine the association between perceived injustice and both partners’ anxiety and depressive symptoms, as well as their infertility-related quality of life, path analyses based on the actor-partner interdependence model (APIM; Kenny, Kashy, & Cook, 2006) were conducted (with maximum-likelihood estimation and nonparametric bootstrapping) using IBM SPSS Amos software (version 25). APIM analyses are used to test actor (e.g., the effect of one’s own perceived injustice on one’s own anxiety symptoms) and partner effects (e.g., the effect of one’s own perceived injustice on one’s partner’s anxiety symptoms), while controlling for the statistical non-independence of dyadic data (Kenny et al., 2006). To examine whether the theoretical model was a good fit for the data, three fit indices were considered: a non-significant chi-square, a value of CFI greater than 0.90, and a value of RMSEA below 0.08 (Kline, 2015). In order to verify whether there were sex differences in the actor and partner effects, we conducted an omnibus within-dyad test of distinguishability (Kenny et al., 2006). That is, a fully constrained model in which both actor and partner effects were constrained to be equal between men and women was compared to a model in which the actor and partner effects were freely estimated using a chi-square difference test. Nonparametric bootstrapping allowed us to obtain 90% confidence intervals around standardized regression coefficients.
To examine possible differences based on sex or cause of infertility with respect to perceived injustice, repeated measures ANOVA were used with sex as a repeated factor for the dyad and infertility cause as the between-subject factor. Possible differences based on cause of infertility were tested using four analyses. We compared differences in perceived injustice based on (a) the five cause categories (i.e., female factors, male factors, combined factors, unexplained, and diagnosis under investigation), (b) whether the cause was due to a female factor alone or not (dichotomous variable), (c) whether the cause was due to a male factor alone or not (dichotomous variable), and (d) whether the cause was known to couples (i.e., unexplained or under investigation) or not (dichotomous variable). All significance tests were performed at p < .05.
Results
Participant Demographic and Clinical Characteristics.
Descriptive Statistics and Correlations for Perceived Injustice, Anxiety and Depressive Symptoms, and Infertility-Related Quality of Life.
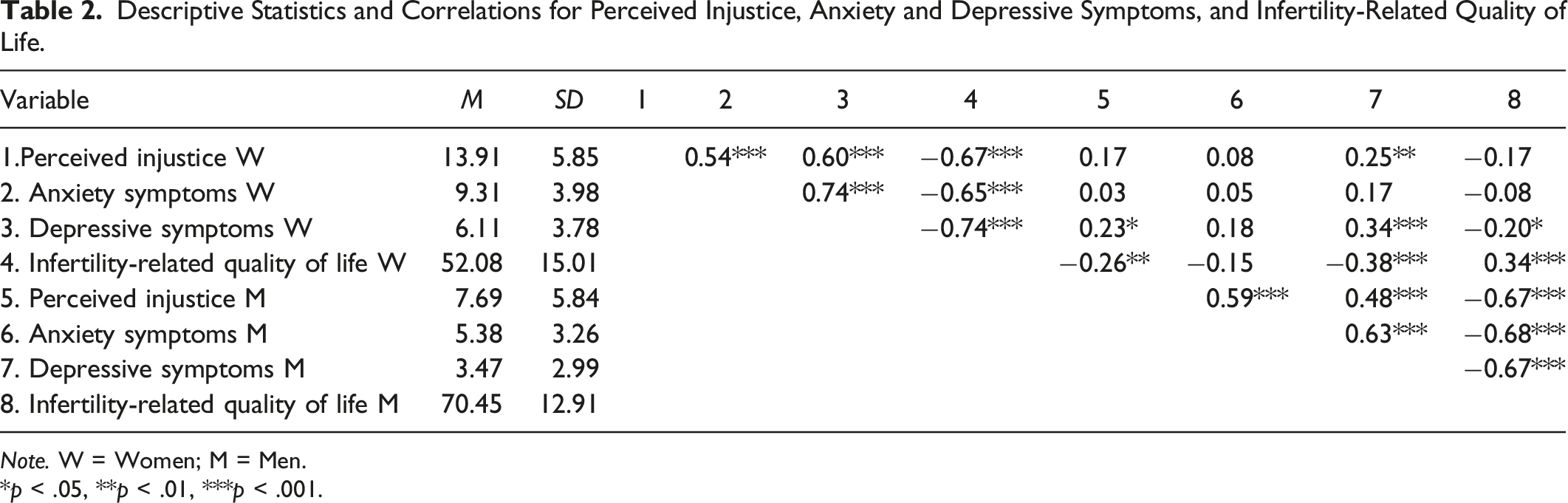
Note. W = Women; M = Men.
*p < .05, **p < .01, ***p < .001.
Perceived Injustice and Psychological Well-Being
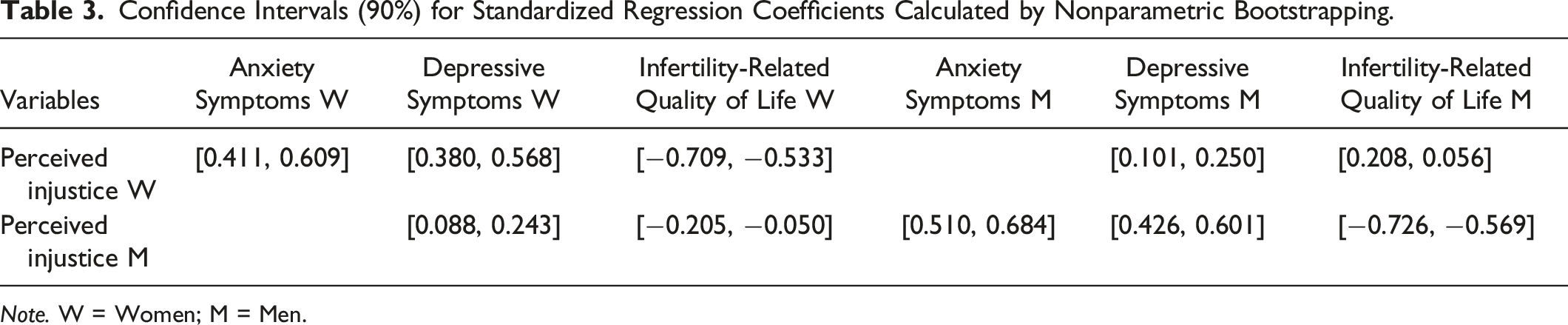
The final path model testing the associations between both partners’ perceived injustice and their psychological well-being is displayed in Figure 1. Although women’s income was initially included as a covariate, it was no longer significantly associated with the study variables and was thus removed in the final model. Since partner effects were examined on an exploratory basis only, two models were tested. The first model included all possible partner effects, whereas the non-significant partner effects were removed in the second model. This later model yielded superior fit indices and thus was kept as the final model. We found no statistical difference between the fully constrained model and the freely estimated model (Δχ2 (5) = 8.02, p = .155), suggesting that there were no significant sex differences in the actor and partner effects. The final model was a good fit to the data (χ2 (13, N = 103) = 10.03, p = .981; CFI = 1.00; RMSEA = 0.000, 90% CI [0.000; 0.078]). Table 3, available in online supplementary material, presents the 90% confidence intervals for the standardized regression coefficients calculated by nonparametric bootstrapping. Results indicated that for men and women, higher levels of perceived injustice were associated with their own higher anxiety and depressive symptoms, as well as their own lower infertility-related quality of life. Moreover, for both members of the couple, higher levels of perceived injustice were also associated with their partners’ higher depressive symptoms and lower infertility-related quality of life. Path analyses based on the actor-partner interdependence model between perceived injustice and anxious and depressive symptoms and infertility-related quality of life. Note. W = Women; M = Men. Dashed lines represent non-significant paths. **p < .01. ***p < .001. Confidence Intervals (90%) for Standardized Regression Coefficients Calculated by Nonparametric Bootstrapping. Note. W = Women; M = Men.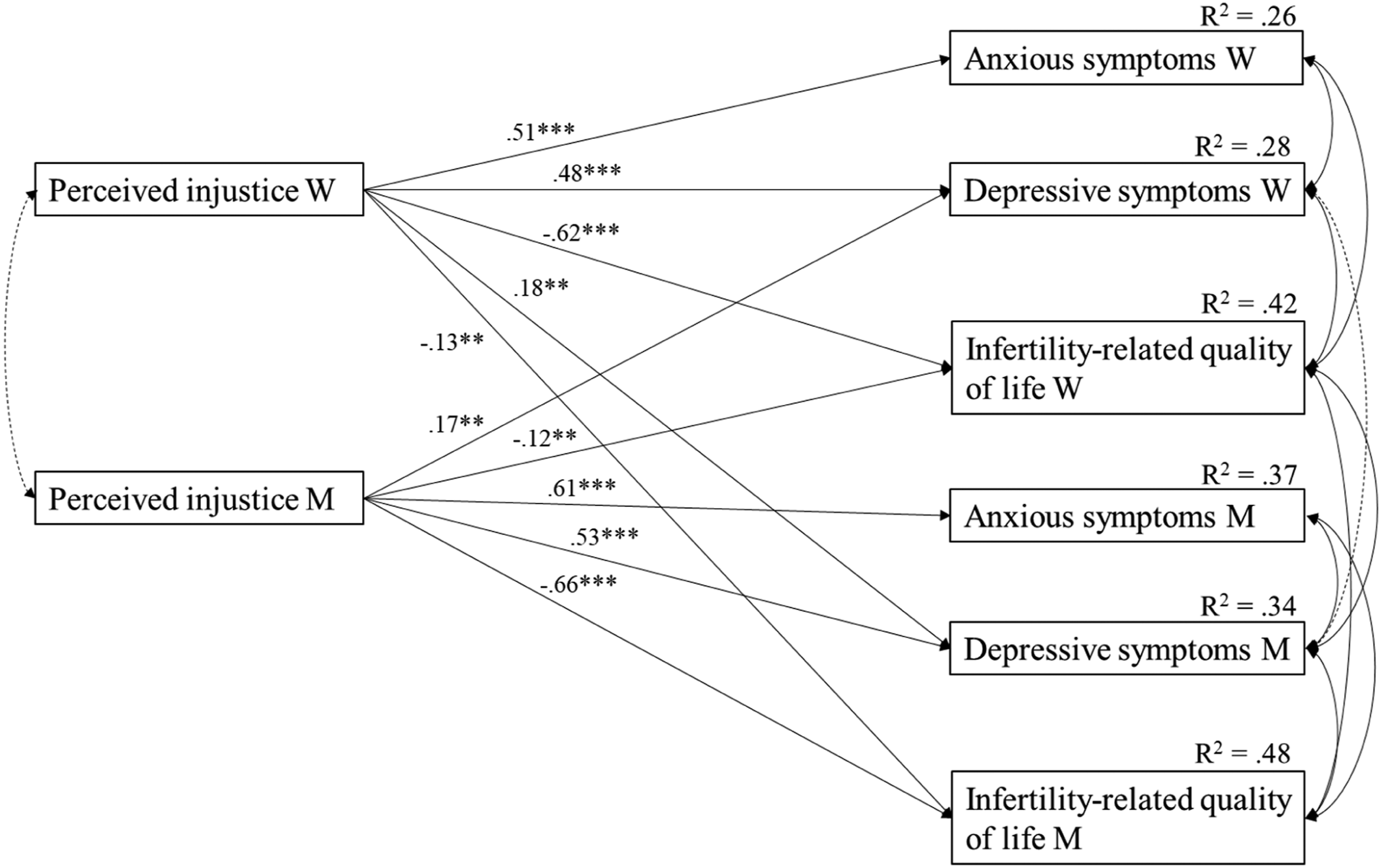
Cause of Infertility and Sex Differences in Perceived Injustice
All analyses involving the cause of infertility yielded no significant effect on men’s and women’s levels of perceived injustice (i.e., no significant main effect of cause, nor Sex X Cause interaction). Analyses showed that women (M = 13.91, SD = 5.85) reported higher perceived injustice than their male partners (M = 7.69, SD = 5.84), F (1, 102) = 69.88, p < .001; ηp2 = 0.41, with a large effect size.
Discussion
This study examined the association between perceived injustice and psychological well-being in both members of couples seeking fertility treatment. The findings showed that perceived injustice was associated with lower psychological well-being in both men and women. Supporting the use of a dyadic approach, we found that perceived injustice was also associated with the partner’s higher depressive symptoms and lower infertility-related quality of life. Women also reported higher levels of perceived injustice than their male partners.
Perceived Injustice and Psychological Well-being
Supporting our hypothesis, in both men and women, perceived injustice was associated with higher anxiety and depression symptoms as well as lower infertility-related quality of life. These findings are consistent with the results of previous studies conducted in community and medical samples (Bezrukova et al., 2010; Doosje et al., 1998; McParland & Knussen, 2010; Pâquet et al., 2016; Rodero et al., 2012; Sullivan et al., 2008; Sullivan, Scott, & Trost, 2012), supporting the notion that perceived injustice may compromise individuals’ psychological well-being. Perceived injustice has been conceptualized as cognitions comprising elements of irreparability and magnitude of loss. Given that the experience of any loss (e.g., of health, of self-esteem, of status, of hope of fulfilling a goal, or of a loved one) may precipitate a depressive reaction (Keyes et al., 2014; Wallach & Mahlstedt, 1985), it is not surprising that infertile men and women, whose experience may involve multiple losses (Fisher & Hammarberg, 2012; McBain & Reeves, 2019; Wallach & Mahlstedt, 1985), would develop higher anxiety and depressive symptoms. Moreover, for couples who remain childless, the grieving process related to infertility may remain unresolved for numerous years (Volgsten, Svanberg, & Olsson, 2010), fueling an enduring sense of unfairness and thereby, significantly deteriorating their psychological well-being.
No sex differences were observed in the association between perceived injustice and psychological well-being, suggesting that injustice may have a similar impact for both partners of infertile couples. This finding supports the fact that infertility can also be distressing for men, who have been shown to experience stress, anxiety, depression, lower quality of life, and self-esteem issues due to difficulties conceiving a child (Cousineau & Domar, 2007; Wischmann & Thorn, 2013; Ying et al., 2015). Our results extend these findings and suggest that men who perceive more injustice show lower psychological well-being, just as their female partners do.
Moreover, our finding that perceived injustice in men and women was also associated with their partners’ higher depressive symptoms and lower infertility-quality of life emphasizes that infertility is a shared experience within the couple. Infertility impacts many spheres of a couple’s life, represents an obstacle to a common goal of the couple, and requires a significant involvement from both partners. It is therefore possible that injustice experienced by an individual would be associated with depressive symptoms and a more negative impact of infertility on several life domains in their partner. The individual may feel powerless in helping alleviate their partner’s perceived injustice, distress, and sense of deep loss with respect to infertility. The anger and blame attributions that often result from perceived injustice may also be especially difficult for partners to deal with, further exacerbating their depressive symptoms and their perception that infertility has negatively permeated all aspects of their life. Indeed, previous studies have reported that male partners in particular tend to assume the role of supporters and often feel helpless when faced with their partner’s infertility-related distress (Genesse et al., 2019; Herrera, 2013; Koert et al., 2019). It should be noted, however, that the cross-sectional nature of our data prevents establishing causality between the variables. Therefore, it is also possible that a partner’s depressive symptoms may render the situation more difficult for the other partner, magnifying his or her perception that the situation is unfair due to having to deal with the burden of fertility problems and his or her partner’s high levels of distress. Future studies will be needed to examine the factors that may mediate the links between individuals’ perceived injustice and their partners’ well-being.
Sex Differences in Perceived Injustice
Our finding that women reported higher levels of perceived injustice than men is in concordance with what was observed in a qualitative study on individuals undergoing fertility treatment in which almost all women (7 out of 8) reported experiencing injustice, whereas none of the men did (Genesse et al., 2019). Sex differences in perceived injustice could be explained by the fact that infertility appears to be experienced as more difficult for women, who report higher levels of guilt, blame, and distress related to self-esteem (Lee, Sun, & Chao, 2001; Péloquin et al., 2018), as well as more depression, anxiety, and stress than men in the context of infertility (Luk & Loke, 2015; Ying et al., 2015). It has been suggested that women tend to be more loss-oriented following bereavement, whereas men tend to be more solution-oriented (Stroebe & Schut, 2010), which seems coherent with women perceiving greater injustice in the context of infertility. The higher levels of perceived injustice in women may also be associated with socialization processes and societal expectations related to sexual roles and maternity (Greil, McQuillan, & Slauson-Blevins, 2011; Péloquin & Lafontaine, 2010). Women generally are more likely to report a strong desire to have a child (Hjelmstedt et al., 1999) and to have more pressure placed on them to have children (A. Greil et al., 2011), which could exacerbate their perceived injustice when they are unable to conceive a child. The differential experiences of men and women in the context of assisted reproduction also need to be acknowledged. Women undergo the majority of invasive and time-consuming treatments, which involve physical discomfort and hormonal medication that could interfere with mood (Cousineau & Domar, 2007; Peterson et al., 2012). This could accentuate women’s perception of injustice.
However, this sex difference could also reflect the fact that men may be less inclined to reveal experiencing a sense of injustice. In their review of the literature on men’s experience of infertility, Wischmann and Thorn (2013) concluded that gender differences in the context of infertility should be interpreted in light of the general gender differences observed in stress reactions, coping, and grief. Indeed, due to socialization, men may be less inclined to express and reveal certain feelings and emotions (Niedenthal, Krauth-Gruber, & Ric, 2009), and this has been observed in the context of infertility as well (Wischmann & Thorn, 2013), with men being more likely to suppress their emotions “to be strong” and to support their partner (Hudson & Culley, 2013).
Cause of infertility and Perceived Injustice
Corroborating previous studies examining women’s emotional reactions to infertility (Hjelmstedt et al., 1999; Nachtigall et al., 1992; Souter et al., 2002), the cause of infertility had no effect on women’s level of perceived injustice. Unlike previous studies showing that men had more negative emotional responses when infertility was caused by a male factor (Connolly et al., 1987; Nachtigall et al., 1992; Newton et al., 1999; Smith et al., 2009), we found that men’s perceived injustice was unrelated to the cause of infertility. Our results, as well as previous inconsistent findings about the association between the cause of infertility and psychological well-being, suggest that for women and men, the experience of infertility and treatment may not strongly dependent on the specific diagnosis or on who has been diagnosed with the fertility problem. When it comes to the perception of injustice, the inability to have a child when one desires to have one, treatment failures, and pregnancy losses may all be highly distressing experiences, irrespective of the cause of infertility (Gameiro, Boivin, Peronace, & Verhaak, 2012; Koert et al., 2019; McQuillan, Greil, White, & Jacob, 2003; Newton, Hearn, & Yuzpe, 1990).
Limitations
This study presents some limitations. First, the data were obtained through self-reported questionnaires only. Therefore, our results could be influenced by social desirability and shared-method variance. These biases, however, would not explain the observed partner effects. Second, the cross-sectional nature of the data precludes making any assumptions about causality between the variables. For instance, it is possible that depression could cause this perception of injustice in infertility patients. Longitudinal designs will be needed to expand our knowledge of the developmental course of perceived injustice and its potential predictors over time. Third, the sample was heterogenous in that couples were surveyed at different time points in their fertility journey. Although no treatment or medical history variables were associated with perceived injustice in our analyses, the mechanisms that may drive men’s and women’s perceived injustice could change over time. For instance, anger and a sense of unfairness may characterize the emotional experience of women in the early stages when noticing an inability to conceive naturally compared to other women. The severity of the loss and the experience of an irreparable loss may become apparent only later in the treatment process, as couples experience repeated treatment failures. Hence, although we made several hypotheses that could explain why men and women may be more or less likely to perceive injustice, the measure we used to assess perceived injustice and the design of the study do not allow us to pinpoint the precise mechanisms underlying this perception. The circumstances that generate perceived injustice and the mediating processes involved require further investigation. Fourth, the results cannot be generalized to all infertile couples because the sample predominantly included French-Canadian and White individuals with a high level of education and high socio-economic status. Levels of perceived injustice might be higher in couples who cannot afford treatment and in marginalized groups, such as LGBTQ+ individuals who use assisted reproduction technology.
Clinical Implications
Examining perceived injustice in the context of infertility, which has not been studied quantitatively to date, has allowed us to better understand the experiences of couples followed in fertility clinics. From a clinical perspective, our findings support the importance of a focus on perceived injustice as an intervention target to reduce psychological distress and increase the quality of life of couples seeking fertility treatment. Indeed, counseling could help normalize and validate the experience of injustice in the context of infertility. Psychoeducation about the long-term negative effects of ruminating over perceptions of injustice and associated anger and blame on both partners’ well-being could also be beneficial. Counselors could then assist couples in developing alternative coping strategies for managing this sense of injustice and the inevitable stress associated with fertility treatments. Perceived injustice could also be an important factor to take in consideration during screening to assess the psychological well-being of individuals seeking fertility services. Indeed, since perceptions of injustice appear to be associated with anxiety and depressive symptoms, as well as lower infertility-related quality of life, the assessment of such perceptions could represent an indicator of potential psychological distress. In addition, if one partner reports experiencing a sense of injustice, health care professionals could be prompted to also explore psychological well-being in the other partner. This exploration could allow health care professionals to provide comprehensive clinical care and appropriate resources applicable to both partners, not solely women, who are generally the patients when it comes to fertility treatments.
Conclusion
“Why has this happened?” “Why me?” “It all seems so unfair!”
These expressions translate a perception of injustice that is a reality of infertile couples’ lives and that, as the present study suggests, could significantly impair couples’ psychological well-being. Several directions for future studies could be considered to further develop our understanding of the association between perceived injustice and psychological adjustment to fertility issues. First, it would be important to conduct a similar study with couples whose members self-identify as LGBTQ+ to verify whether the results would be comparable to those found in the present study. In order to understand couples’ experiences more fully, a mixed-methods design involving qualitative methods that would allow participants to further elaborate on their perceived injustice would warrant consideration. The us of daily diaries would also allow us to pinpoint specific moments when perceptions of injustice are being triggered (e.g., when the nurse calls to inform them about treatment failure) and if daily changes in these perceptions explain variations in psychological distress. Finally, future studies should assess whether interventions targeting perceived injustice would be effective in improving the psychological well-being of infertile couples.
Footnotes
Acknowledgments
We would like to acknowledge the contributions of the following fertility clinics to our research project: Fertilys, Procréa Fertility, CIUSS-CHUS de l’Estrie, and CHU de Quebec, as well as thank Virginie Arpin and all other students who have participated in the data collection for the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Fonds de recherche du Québec – Société et Culture (Grant #2014-NP-172420) and the Fonds de recherche du Québec – Santé (Grant #30628).