
Abstract
Since the fall of communism, approximately 10%–15% of the Romanian population are estimated to have left the country in search of economic opportunities, resulting in a high number of children being left behind (i.e., children of migrant parent; CMP) in Romania.
This study explored patterns of parental migration and frequency and correlates of mental health problems among CMP. A total of 889 adolescents, aged 13–18 years, with migrant parent(s) participated in the present study. Results showed a high prevalence of mental health problems, with dysthymia (51%) being the most common. As for parenting styles, “inconsistency” was found to increase the risk for depression and dysthymia. “Higher involvement” from parents significantly decreased the risk for attention deficit hyperactivity disorder, panic, and substance abuse. The findings were discussed in terms of their clinical, training, and political implications.
Introduction
The fall of communism in Romania in 1989 has been associated with a high level of migration. It is estimated that 10%–15% of the Romanian population have left the country in search of economic opportunities (Sandu, 2006). The accession of Romania to the European Union and the lifting of the Schengen visa restriction have further increased the number of economic migrations, with Romanians representing up to 40% of all economic migrants in some European countries (International Fund for Agricultural Development [IFAD], 2017; Sandu, 2006). Not surprisingly, economic migration has made a significant contribution to Romanian economic development. In 2016, Romanian migrants sent US$3.5 billion remittances to their families in Romania (IFAD, 2017). This figure shows a 10-year (2007–2016) growth rate of 116.3%.
Because the average age of economic migrants is in the early 40s, which coincide with the start of the family formation, many children are being left behind in Romania. According to the Romanian National Authority for the Protection of the Rights of the Child and Adoption, the institution responsible by law for monitoring the children left at home as a result of the parents’ emigration, 82,464 children are left in Romania by their parents who migrated for work abroad in 2007 (http://www.copii.ro). This figure is likely to be underestimated as few parents are willing to inform the authorities of their intention to work abroad and leave their children in Romania. As reported by the United Nations Children’s Emergency Fund (UNICEF)/Alternative Social Association, 350,000 children are estimated to have been left by one or both parents due to economic migration (Soros Foundation, 2007); half of these children were under the age of 10 years who were left behind in the care of their grandparents, extended family members, and neighbors. Approximately 4% of these children were placed in the care of public authorities.
The impact of parental migration is complex and could bring advantages and disadvantages to the children of migrant parents (CMPs). One of the main advantages include the remittances sent by the migrant parents to the left-behind family members, which could enhance their socioeconomic status and quality of life; this in turn helps to enhance positive developmental outcomes of the CMP’s education, nutrition, and physical health (Andrioni, 2011; Botezat & Pfeiffer, 2014; Cortes, 2011; Gassmann et al., 2013; Hu, 2012; Macours & Vakis, 2010).
Other studies have, however, reported the negative impact of parental migrant on CMP’s educational and psychological outcomes (Mazzucato, 2014). Specifically, studies conducted in China (Chang et al., 2011; Fan et al., 2010; He, 2008; Wen & Lin, 2012), in the Philippines (Cortes, 2011), and in the Caribbean (Smith et al., 2004) have reported high levels of behavioral and emotional problems, low self-esteem, low school engagement, and poor health (Wen & Lin, 2012) among CMP; these children were also at a high risk of dropping out of school (UNICEF, 2008). Similarly, according to a handful of reports and small-scale studies in Romania, CMPs frequently suffered from physical sickness (Botezat & Pfeiffer, 2014) and had low educational and psychological well-being (i.e., aggressive and delinquent behavior; feeling of abandonment, anxiety, and depressive moods) (Andrioni, 2011; Luca et al., 2007). CMPs who infrequently communicated with their parents tended to encounter severe loneliness and low levels of life satisfaction (Jia & Tian, 2010). Research has also shown a lack of adolescent–parent bonding (Moretti & Peled, 2004) and lack of parental support and monitoring to be associated with emotional and behavioral problems in adolescents (Matjasko et al., 2007). However, the impact of parental migration on children’s well-being and other outcomes (e.g., academic) seemed to differ across gender. For example, in a recent study in China (Wu et al., 2015), girls who were left by their migrant parents, compared to boys, had poorer mental health. In another study (Leng & Park, 2010), fathers’ migration reduced enrolment among sons, but it had a significant positive effect on the academic outcomes of daughters.
Despite the high number of CMP in Romania, little is known about the characteristics of parental migration, living arrangement, and its impact on CMP’s psychological well-being. Therefore, to make up this gap, the aims of the present study were to explore the (a) patterns of parental migration (i.e., gender of migrating parents, length of migration, frequency, and type of contact with CMP) and CMP’s living arrangements; (b) frequency of mental health problems among the CMP; and (c) factors that are associated with mental health problems among the CMP. The factors under investigation include social support, parenting styles, parental bonding, and factors that are specific to parental migrant such as type and frequency of contact.
Methods
Participants
The data were obtained from a large study on the psychological well-being of adolescents in Romania in which a total of 1,764 adolescents participated. In the present study, data of 889 adolescents, aged 13–18 years, with migrant parent(s) were used. One hundred and forty-seven participants with some missing values in at least one of the study’s variables were excluded, thus resulting in a final sample of 741. There were no significant differences between those who were included and excluded in terms of sociodemographic and clinical characteristics, except for age and substance abuse. Adolescents who were excluded in the analyses were significantly younger (mean = 15.63 years, SD = 1.41) than those who were included in the analyses (mean = 15.89 years, SD = 1.32, p < 0.05); they also reported higher rates of substance abuse (22.3% vs. 15.5%, p < 0.05).
Procedure
Adolescents were randomly recruited from 17 schools from the city of Iasi (urban area) and from five villages (rural area) near the city of Iasi in Romania. These samples approximate national geographics, and thus, could be regarded as representative of the population in question.
An ethical approval to conduct this study was obtained from the University of Roehampton Ethics Board, the Ministry of Education and Culture represented by School Inspectorate and the relevant local authorities in Iasi. Only adolescents who had given their written consent to participate in this study and the written consent form of their parents or guardians prior to completion of the questionnaire were allowed to participate.
About 70% of the adolescents who were invited to participate in the study took part and had the written consent from their parents or guardians prior to the study. The main reason for the adolescents not wanting to participate in the study was lack of interest or being too busy; the main reason for not having a written consent from the parents or guardians was because they had forgotten to give their parents/guardians the form to sign.
The questionnaires were administered by the researcher (AD) in a designated room within the schools to ensure independent answering and allowing the adolescents to ask any questions that they may have.
Instruments
Perceived Social Support scales (PSS; Zimet & Farley, 1988) was used to measure the extent to which the adolescents perceived their friends, family, and a significant other as providing their needs for support. Each item was rated on a 7-point rating scale, ranging from “very strongly disagree” (1) to “very strongly agree” (7). The total PSS has good internal reliability with a Cronbach’s α of 0.88 (Zimet & Farley, 1988). In the present study, the Cronbach’s α for the total PSS scores was 0.76.
The Parental Bonding Instrument (PBI; Parker et al., 1979) was used to measure perceived parental bonding. It contains 25 items that can be used to measure “care” and “overprotection.” The items are scored on a 4-point Likert scale ranging from “very likely” (1) to “very unlikely” (4), indicating the degree of the participant’s agreement with each statement. The split-half reliability of the PBI was 0.88 for the care scale and 0.74 for the protection scale (Parker et al., 1979). In the present study, the Cronbach’s α for care and protection scales were 0.86 and 0.70, respectively.
The Social and Health Assessment (SAHA; Schwab-Stone et al., 1995) parent–adolescent interaction subscale was used to assess the four aspects of parenting styles, namely parental warmth, parental control, parental involvement, and inconsistent parenting. Participants had to evaluate their parents’ behavior on a 4-point scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often). In the present study, the Cronbach’s α for the total SAHA scores was 0.78.
Youth Inventory-4R (YI-4R; Gadow & Sprafkin, 1997) was used to assess DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th Edition; American Psychiatric Association, 1994) symptom categories of attention deficit hyperactivity disorder (ADHD), conduct disorder, anxiety disorders, depression, and substance use. The YI-4R can be scored to derive symptom count scores (diagnostic model) or symptom severity scores (dimensional model). In the present study, the Cronbach’s α for each of the symptom severity scales ranged from 0.89 to 0.91.
Translation of Questionnaires
All the questionnaires except for the SDQ were translated and adapted from English to Romanian according to the back-translation guidelines that are widely accepted for the successful translation of instruments in cross-cultural research (Brislin, 1970). The SDQ has been translated previously and was downloaded from the SDQ website (http://www.sdqinfo.com/a0.html).
Statistical Analysis
Frequencies, proportions, and means were used for descriptive analyses. The prevalence of DSM-IV symptom categories and the mean and standard deviation for the SDQ scores were obtained for boys and girls, and they were compared using chi-square tests and the Wilcoxon–Mann–Whitney test, respectively.
Adjusted logistic regression models and linear models were run to determine the association between covariates with DSM-IV symptom categories and SDQ scores, respectively. Models calculated for each diagnosis or SDQ subscale included age, gender, and urbanity. Other covariates (number of people living in the house, time parents were abroad, frequency of contact with parents, who was working abroad, parenting styles, support perceived, and parenting bounding) were also included in these models only if they appeared as significantly associated (p-values < 0.05) with the diagnosis or the SDQ subscales in bivariate analyses. This was done to avoid overfitting. Bivariate analyses to determine the differences between CMPs with and without DSM-IV symptom categories included chi-squared test for categorical variables, and t-test for continuous variables. SDQ scores were not normally distributed. Thus, median and interquartile were calculated in each sociodemographic and family covariates and compared with nonparametric tests (Wilcoxon–Mann–Whitney test for binary variables and Kruskal–Wallis test for categorical variables) (results of the bivariate analysis not shown but available under request). Thus, each model for each clinical outcome (clinical diagnosis or SDQ subscale) could include different covariates at the same time, depending on the results of the bivariate analyses.
All the analyses were performed using Stata version 13 for Windows (SE version 13, College Station, TX), and statistical significance was set at a p < 0.05.
Results
The sociodemographic, clinical, and family characteristic of the sample (N = 714), which are used in the present analyses, are presented in Table 1. The mean age was 15.9 years (SD = 1.3), and 50.5% of the sample were females. The majority of the sample was living in urban areas with at least one parent (68.8%). Of the two parents, it was the father who was most frequently working abroad; the majority of parents had been away for more than one year (59.2%). Approximately half of the CMPs were in daily contact with their migrant parent.
Sociodemographic and Family Characteristics of Left Behind Children (N = 741).
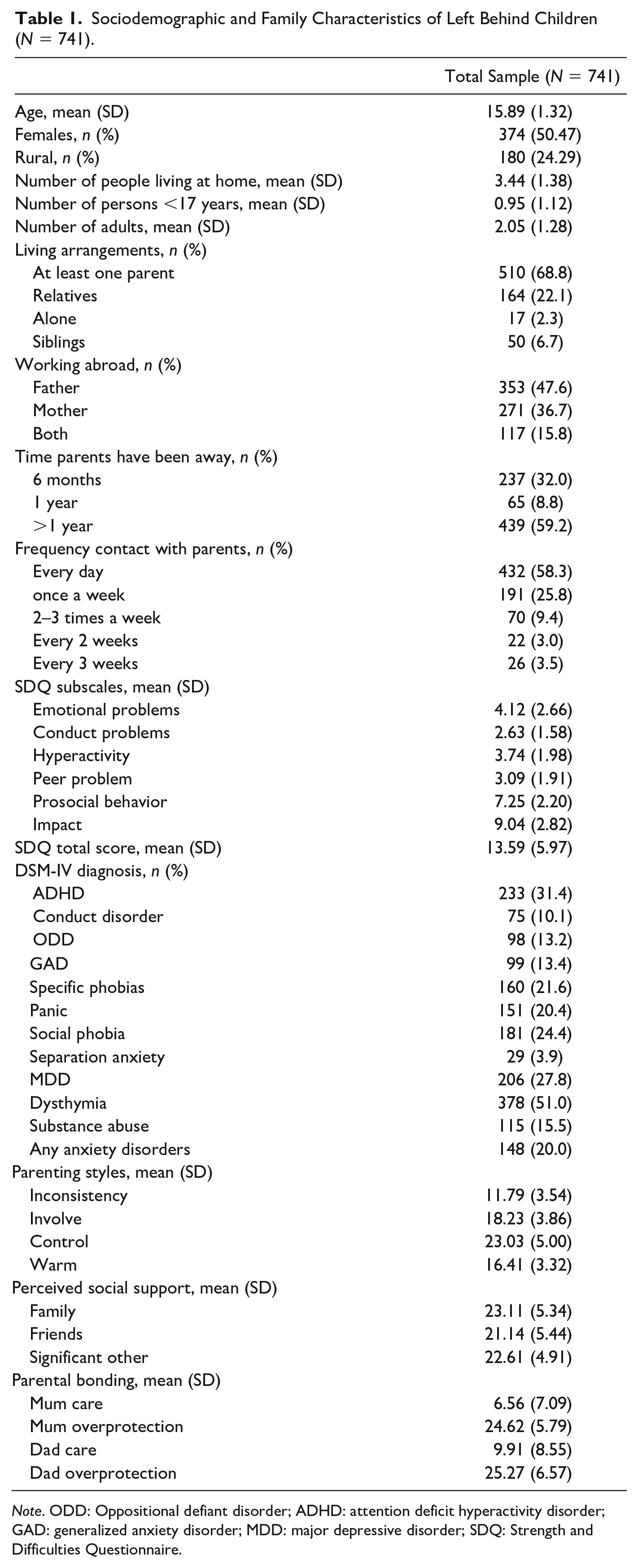
Note. ODD: Oppositional defiant disorder; ADHD: attention deficit hyperactivity disorder; GAD: generalized anxiety disorder; MDD: major depressive disorder; SDQ: Strength and Difficulties Questionnaire.
The most prevalent symptom categories were dysthymia (51%), followed by ADHD (31.4%). The least frequent was DSM-IV symptom category of separation anxiety disorder, affecting only 3.9% of the sample. In terms of gender, girls were more likely than boys to have the symptom categories of ODD (p < 0.01), major depression (p < 0.01), dysthymia (p < 0.001), anxiety disorders (p < 0.001), and various subtypes of anxiety disorders, including GAD (p < 0.001), specific phobia (p < 0.001), panic (p < 0.001), social phobia (p < 0.001), and separation anxiety disorder (p < 0.05). Boys, on the other hand, were more likely to suffer from symptom categories of conduct disorder (p < 0.01) and substance abuse (p < 0.001) (Figure 1) than girls. As for the SDQ, girls reported significantly higher scores than boys on emotional symptoms, hyperactivity, peer problems, social behavior, and on total scores and impact scores (p < 0.001) (Figure 2).
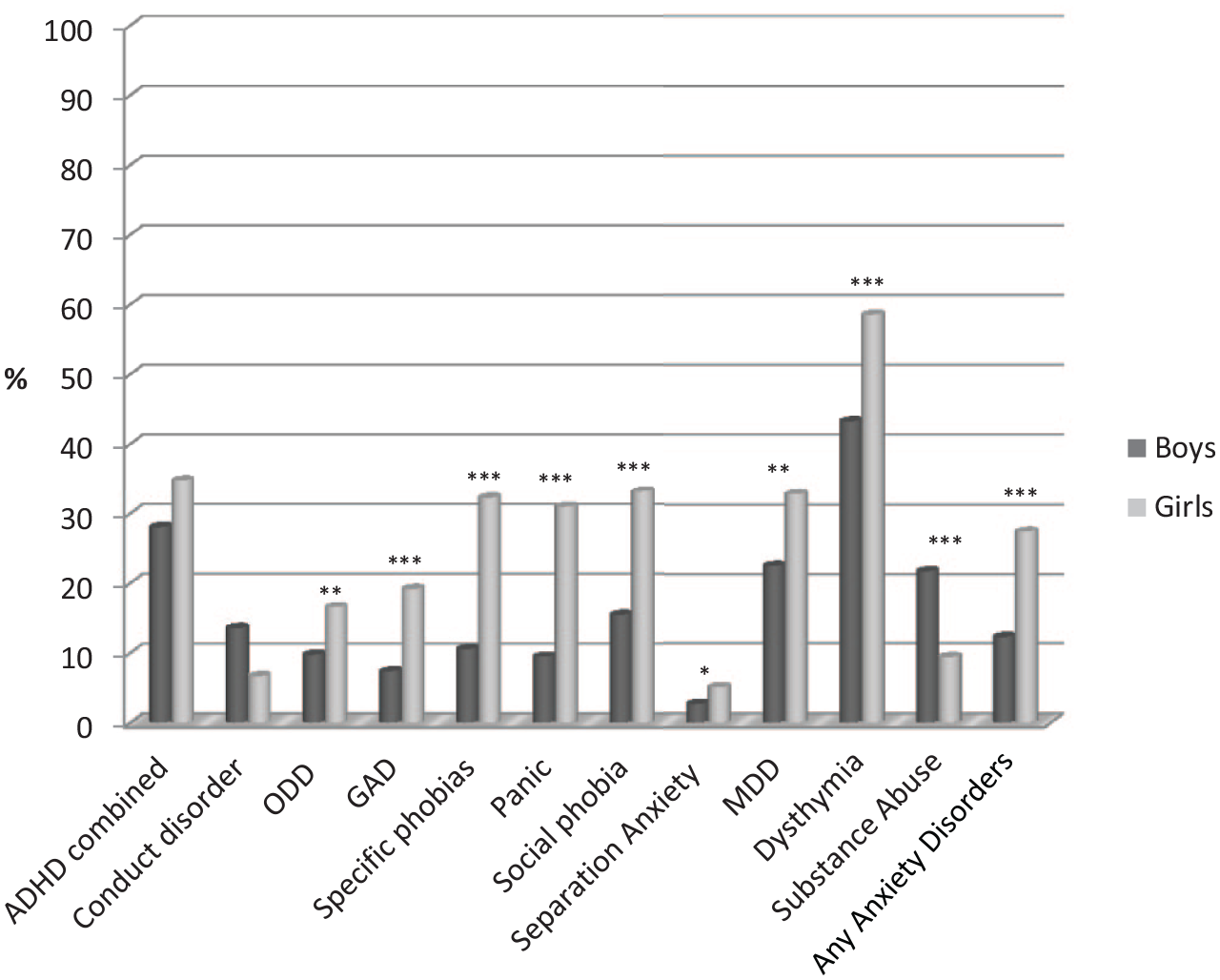
Proportion of DSM-IV diagnoses among the CMPs by gender.
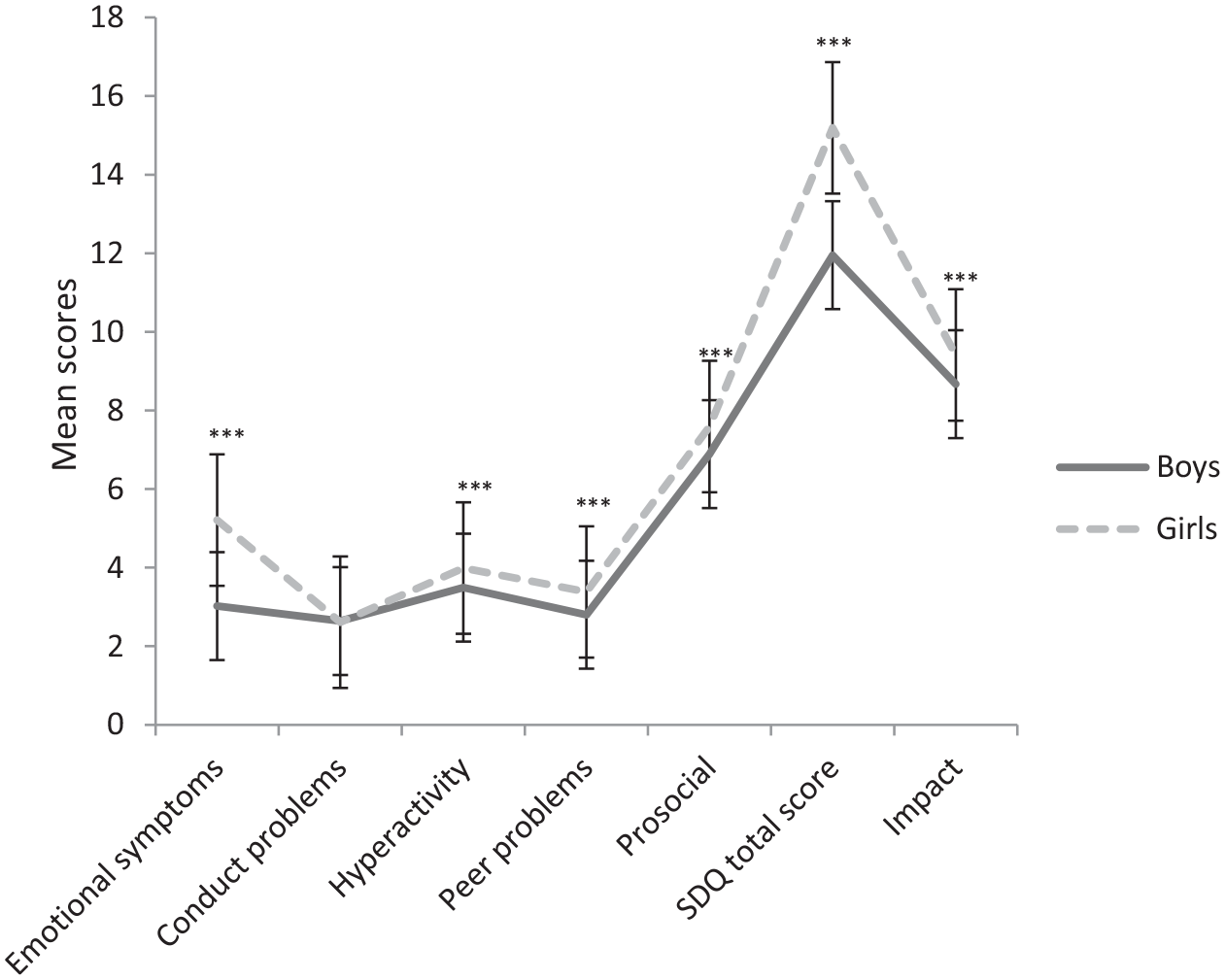
Mean scores of the SDQ subscales among the CMPs by gender.
Table 2 shows the adjusted odds ratios (aORs) and 95% confidence intervals (95% CI) for the association between DSM-IV symptom categories and covariates. Each logistic regression model included age, gender, and urbanity, and those covariates which appeared as significantly related to that particular diagnosis in the bivariate analyses, with all of them introduced simultaneously in the regression model. For example, for ADHD, the bivariate analysis showed that parenting styles, PSS scores, and parenting bounding were significantly related to ADHD. Therefore, they were included simultaneously in the logistic model for ADHD, along with age, gender, and urbanity (Table 2).
Multivariate Logistic Regression Models for the DSM-IV Diagnoses.
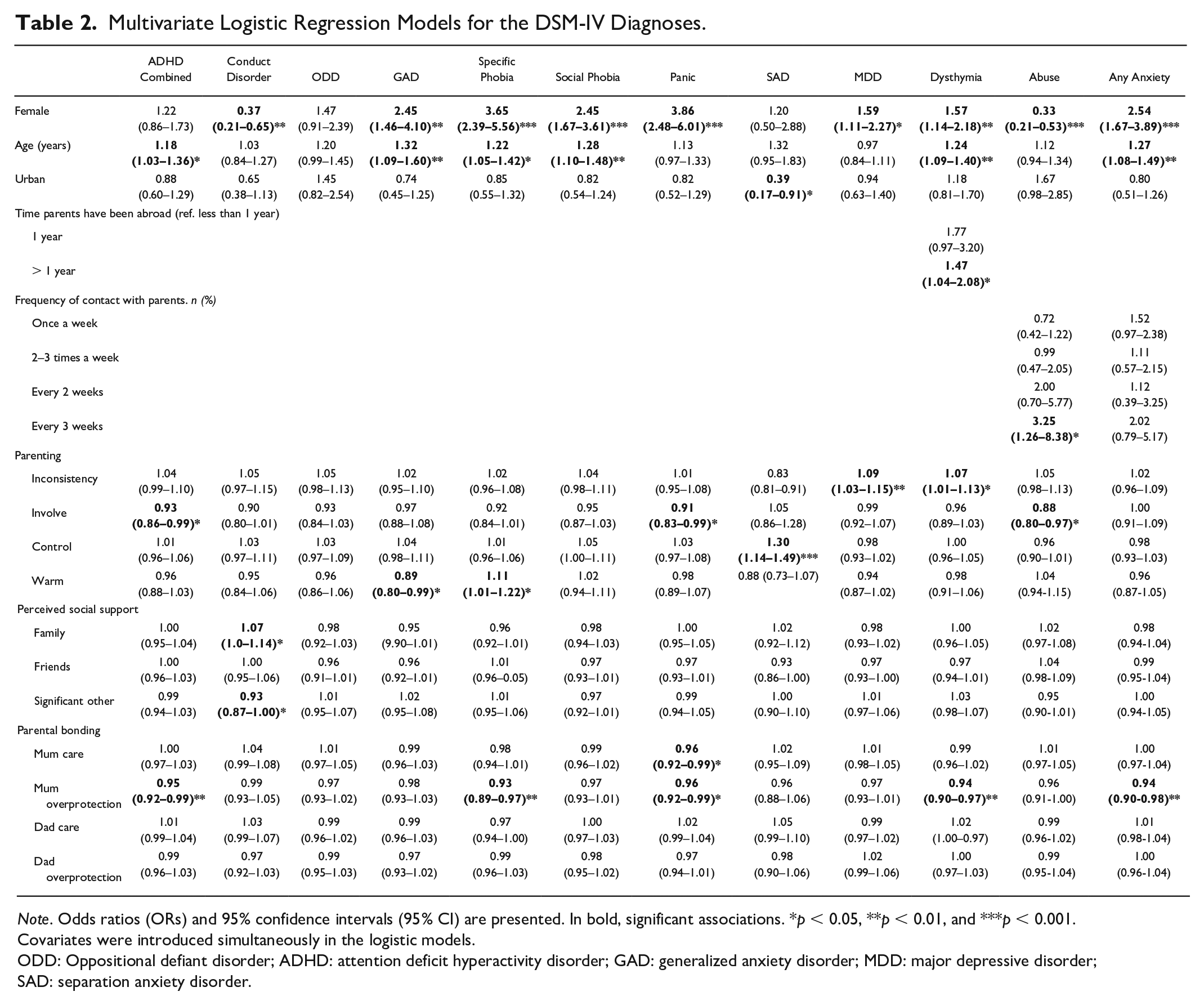
Note. Odds ratios (ORs) and 95% confidence intervals (95% CI) are presented. In bold, significant associations. *p < 0.05, **p < 0.01, and ***p < 0.001.
Covariates were introduced simultaneously in the logistic models.
ODD: Oppositional defiant disorder; ADHD: attention deficit hyperactivity disorder; GAD: generalized anxiety disorder; MDD: major depressive disorder; SAD: separation anxiety disorder.
Overall, girls presented higher risk than boys for having internalizing symptom categories: major depression, dysthymia, and any anxiety disorders and their subtypes (i.e., GAD, specific phobia, social phobia, panic disorder). For example, girls were 3.65 times more likely than boys to have specific phobia (95% CI = 2.39; 5.56, p < 0.001) and 2.54 times more risk for any anxiety disorders (95% CI = 1.67; 3.89, p < 0.001). Older adolescents were more likely to have a diagnosis of ADHD, dysthymia, as well as any anxiety disorders and their subtypes (i.e., GAD, specific, social phobia) than younger participants. Those children living in urban areas were less likely to have separation anxiety disorder (aOR = 0.39, 95% CI = 0.17; 0.91, p < 0.05). The amount of time parents have been living abroad was only significantly associated with dysthymia in the bivariate analysis, and in the adjusted logistic regression model for dysthymia, we found that children whose parents have been living abroad for more than one year were 1.5 times more likely to have dysthymia than those whose parents were abroad less than one year. The frequency of contact with parents was significantly associated with substance abuse and anxiety disorder in the bivariate analysis. However only having contacts each three weeks, compared with every day, increased the risk of having a substance abuse diagnosis (aOR = 3.25, 95% CI = 1.26; 8.38, p < 0.05).
Parenting styles, perceived social support, and parental bonding were all significantly associated with all the DSM-IV categories in the bivariate analysis. In the adjusted models, as for parenting styles, “inconsistency” was found to increase the risk for depression (aOR = 1.09, 95% CI = 1.03; 1.15, p < 0.01) and dysthymia (aOR = 1.07, 95% CI = 1.01; 1.13, p < 0.05). “Higher involvement” from parents significantly decreased the risk for ADHD, panic, and substance abuse. Higher scores on “parental control” were related to higher risk for separation anxiety disorder, and “warmth” was protective against GAD and was a risk factor for specific phobia.
Perceived social support was significantly associated with conduct disorder; higher scores on family support were related to higher risk for conduct disorder (aOR = 1.07, 95% CI = 1.0; 1.14, p < 0.05), whereas higher support from significant ones was related to lower risk (aOR = 0.93, 95% CI = 0.87–1.00, p < 0.05). In terms of parental bonding, our findings showed mother’s care was associated with lower risk for panic, and mother’s overprotection was related with lower risk for symptom categories of ADHD, dysthymia, and any anxiety disorders and their subtypes (i.e., specific phobia, panic).
The adjusted beta coefficients and the 95% CI for the SDQ scores are presented in Table 3. Linear regression models for the SDQ subscales also included, simultaneously, gender, age, and urbanity, and those covariates which appeared as significantly associated with the SDQ scores in the bivariate analyses. Compared with boys, girls showed significantly higher scores on emotional symptoms, peer problems, prosocial behavior, total SDQ, and impact scores. For example, girls scored 2.51 points higher on the total SDQ scores (95% CI = 1.82; 3.21, p < 0.001) than boys. Older participants had higher scores on emotional symptoms, prosocial behavior, total SDQ, and impact scores, whereas children living in urban areas presented lower scores on emotional subscale, hyperactivity subscale, prosocial subscale, and total SDQ score, compared with those children from rural areas. There were significant associations between high parental “inconsistency” with more emotional behavior, hyperactivity, peer problems, and total SDQ scores. High involvement from parents was related to low scores of emotional symptoms, peer problems, and total SDQ scores (β = −0.24, 95% CI = −0.40; −0.09, p < 0.01). Parental “control” was related to higher prosocial behavior, and parental “warmth” was associated with more peer problems and low prosocial behavior. While perceived support from family was related to lower scores on prosocial behavior, support from friend was related to lower emotional symptoms, lower peer problems, and lower total SDQ scores and higher prosocial behavior; on the other hand, support from significant persons was linked to higher emotional symptoms and impact. As for parental bonding, high scores on mother’s care were found to be related to more emotional problems, hyperactivity, peer problems, lower prosocial behavior, and higher scores on the total SDQ (β = 0.16, 95% CI = 0.10; 0.23, p < 0.01). Mother’s overprotection was linked to lower scores on the emotional, hyperactivity, and impact scales and with lower total SDQ scores (β = −0.13; 95% CI = −0.21; −0.06, p < 0.01). Only father’s care was significantly associated with more peer problems.
Multivariate Linear Regression Models for the SDQ Scores.
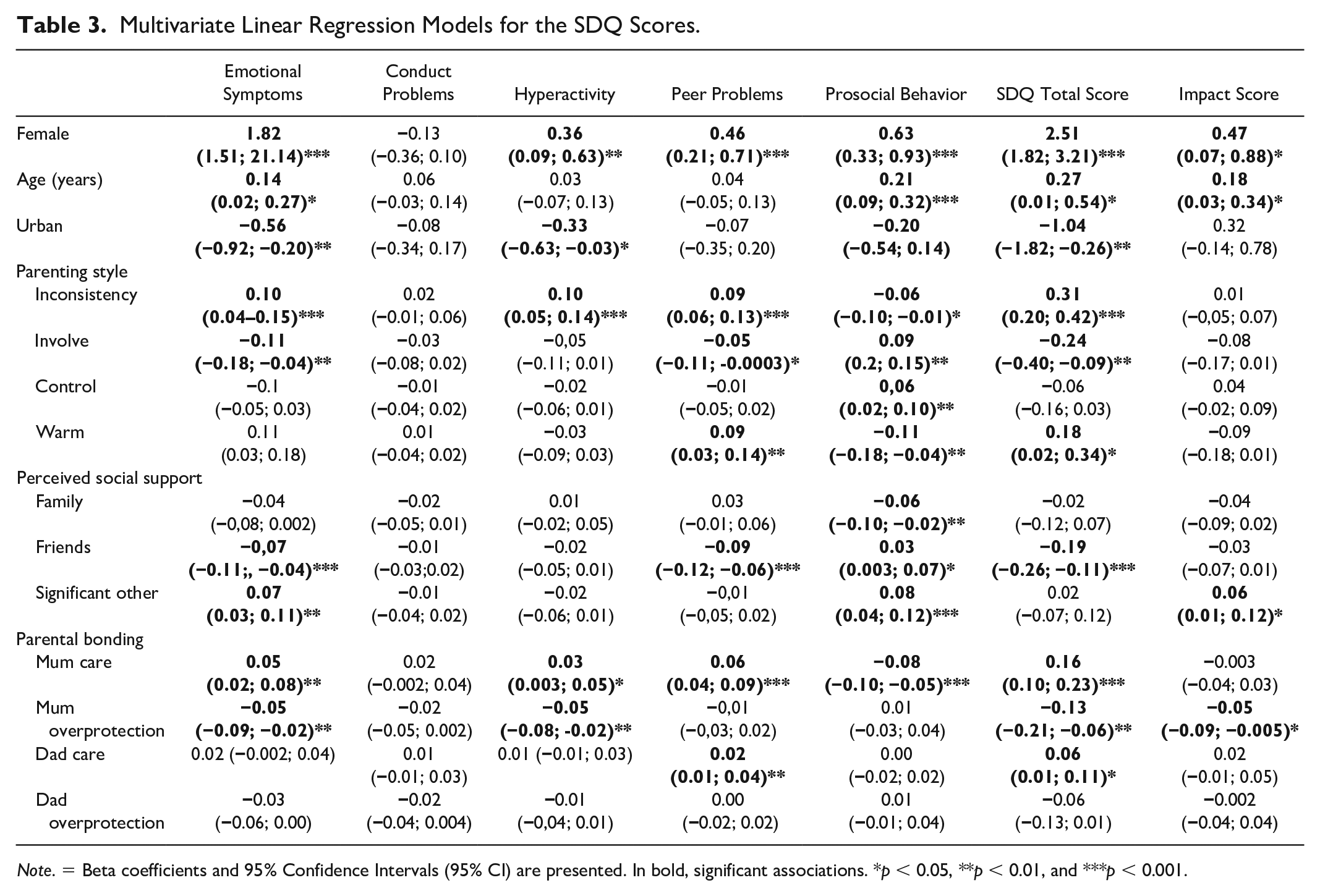
Note. = Beta coefficients and 95% Confidence Intervals (95% CI) are presented. In bold, significant associations. *p < 0.05, **p < 0.01, and ***p < 0.001.
Discussion
The present study examined the patterns of parental migration and CMPs’ living arrangement; frequency of mental health problems among CMPs; and factors that are associated with mental health problems among CMPs. To our knowledge, this study was among the first to have examined the specific features of parental migrant (e.g., living arrangement, frequency of contact) and psychological well-being of a large sample of CMPs in Romania. The main findings can be described as follows. In line with previous studies, the percentage of CMPs with both parents working overseas was lower compared to those who have only one migrant parent (Toth et al., 2007). Most (68.8%) adolescents with migrant parent(s) lived with one parent, while others lived either with their relatives or other siblings; only a small percentage of them lived alone (17%).
In agreement with previous findings, the present study suggested that CMPs have high levels of DSM-IV symptom categories (Jia & Tian, 2010; Pottinger, 2005), the most common being dysthymia (51%), followed by ADHD (31.4%). NGO reports and small-scale studies have similarly reported that CMPs felt being abandoned and rejected by their parents, and they exhibited a high level of depressive and anxiety symptoms (Soros Foundation, 2007). Parents who worked abroad and left their children in Romania were perceived negatively and were regarded as neglectful of their children, leading CMPs to be stigmatized by their peers and by the society at large (Robila, 2011). Other common problems reported among CMPs included behavioral problems, drug and alcohol abuse, and numerous other deviant behaviors (Salah, 2008). It has been argued that the high prevalence of behavioral problems among CMPs is related to a lack of parental monitoring and supervision (Demuth & Brown, 2004). This finding provided further support that parental monitoring is negatively associated with externalizing problems among adolescents (Van Loon et al., 2014). Thus, our present findings are expected to generalize to other countries and/or cultures that have experienced similar situations, or among careers that remove parents/caregivers for extended periods of time.
Perceived family support was associated with high risk for conduct disorder; however, previous findings on the association between parental support and externalizing problems have been inconsistent, with some studies showing parental support to be related to few externalizing problems (Wills & Cleary, 1996), whereas some other studies failed to find this association (e.g., Van Loon et al., 2015). Our findings could be explained by the severity of the problems, in that CMPs with emotional or behavioral problems might represent severe cases, which cause family members to offer much higher support. Conversely, CMPs who did not present mental problems were in less need of support from their relatives, or their relatives did not consider it necessary to give them support. Further research is needed to support this explanation.
Perceived support from peers appeared to be important for preventing mental health problems among CMPs. As argued by numerous authors, during adolescence, friendships become increasingly important for adolescent’s social and psychological development. which may increase resilience in vulnerable adolescents (Brent et al., 2014; Goodyer et al., 1990). Several studies have, indeed, shown the positive impact of peer support among adolescents who have been exposed to negative events (e.g., van Harmelen et al., 2016). The mechanism for this association is not well understood. It has been suggested that perceived peer support may have a positive effect on coping skills and self-esteem (Cohen & Wills, 1985). Other authors have suggested that peer support increased adolescents’ perceived friendship self-efficacy and increased their beliefs on their ability to communicate and engage with their friends (Fitzpatrick & Bussey, 2014). Examining the mechanisms through which peers’ support protects adolescents from developing a mental health problem is an important avenue for future research.
As reported in previous studies, CMPs who reported emotional and behavioral problems were more likely to report parental styles, which involved inconsistency (Frick et al., 1992) and overprotection (Waite & Creswell, 2015). Indeed, a series of studies by Patterson and his colleagues (Capaldi & Patterson, 1994; Patterson et al., 1992) have, for example, shown that inconsistent parenting practices accounted for 30–52% of the variance in the development of antisocial behavior. Other studies have also shown inconsistent parenting to be a powerful predictor of juvenile delinquent behavior (e.g., Wasserman et al., 1996).
Our findings showed “parental control” to be related to a high risk for separation anxiety disorder. Overcontrol is characterized by parental over-involvement and excessive regulation of the children’s behavior, which several authors believed had an impact on the children’s sense of self-efficacy, and limits their experience of novel situations (Waite & Creswell, 2015). The finding that parental “control” was related to higher prosocial behavior and the finding that parental “warmth” was associated with more peer problems and low prosocial behavior were not clear.
Similar to previous studies among adolescents in community settings (e.g., Essau et al., 2010), significantly more girls than boys had emotional problems such as anxiety and depression, whereas significantly more boys than girls had substance abuse. Among studies of home-alone children, findings of mental health problems across gender have been inconsistent, with some studies reporting no significant difference between boys and girls (Leng & Park, 2010), while in some other studies, girls reported poorer mental health than boys (Wu et al., 2015). While it is beyond the scope of this study to examine the reasons for this gender difference, gender socialization, and social and hormonal mechanisms have been put forward as explanations for this difference (Cyranowski et al., 2000).
In interpreting the present findings, some limitations should be discussed. For example, the findings on the association between parenting styles and mental health problems should be taken into consideration because both variables are self-reported by the adolescents. Thus, underreporting of problems could be possible. It could also be possible that they can more likely underreport or overreport extreme parenting styles, especially because they have been “left behind” by their parent(s) and might be living in exceptional circumstances within their families, or they might distort the parenting styles of their parents who have been living abroad. Furthermore, in terms of adolescent’s self-report, some authors argued that teachers or parents should be included as informants. However, other informants may not be the best informants as they are less aware of the internalizing problems of adolescents compared to externalizing problems (Hu et al., 2014). For confidentiality reasons, we did not have information on the schools that children were attending. Therefore, we did not account for potential clustering effect (i.e., children from the same school might be expected to be more homogeneous). When clustering effect is present, standard errors might be misestimated (Hox, 1998). Finally, the data do not allow us to disentangle mental health problems that are not analogous to the non-left-behind adolescents because we did not collect any information on the participant’s mental health issues prior to parental migration. Thus, it is unclear if the mental health problems necessarily constitute the impact of parental migration. The finding that parental migration had negative impact on CMP’s psychological well-being has important political implication for social and health service providers, as well as for policymakers who provide funding for developing and implementing intervention programs to promote emotional well-being in young people in general, and for CMP in particular. Our findings could also inform curriculum development in clinical child and adolescent psychology. The faculties of psychology were closed during the communist regime, and it was only after the Revolution in 1989 that the faculties were reopened (Smith, 2002). Consequently, there is a shortage of trainers for psychology and psychotherapy, especially in youth mental health. In order to overcome this shortage, one way forward is to provide school-based psycho-educational program to CMPs to enhance their skills to cope with situations that are related to parental migration or at-risk children and families. Equally important is to provide psycho-educational programs to parents who intend to migrate to help them reduce the challenges and maximize the experience of economic migration both for themselves and for their children. To conclude, our findings provided implications on enhancing psychological well-being of CMPs through clinical, training, and political reform.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: B.O. is supported by the Miguel Servet program (CP20/00040), funded by the Instituto de Salud Carlos III and co-funded by the European Union (ERDF/ESF, “Investing in your future”).