
Abstract
The impact of grandparenting on the grandparents’ health has been relatively under-studied. This study examined country differences in the effects of grandchild care provision on the grandparents’ depression in Italy, Spain, China, Denmark and Sweden using the longitudinal Harmonised CHARLS and SHARE data collected between 2010–2015. Controlling for the grandparents’ depression in 2011, grandmothers providing non-intensive grandparental care in Sweden in 2013 reported lower depression score in 2015 compared to those who did not provide any care in 2013. Chinese grandfathers, Italian and Swedish grandmothers who provided intensive grandchild care reported lower depression score compared to their counterparts who did not provide any grandchild care. This study indicates that the Structural Ambivalence Theory can only partially explain the findings, suggesting further theoretical development in this area. Future research can focus on identifying the causal pathways between grandparenting and wellbeing, and the implications of such pathways for older persons’ wellbeing worldwide.
Introduction
The global population of older people is growing rapidly. The increasing life expectancy has resulted in more common grandparental childcare, but also in a higher likelihood of individuals to experience certain physical and mental health conditions in later life (Arpino & Gomex-Leon, 2020; Di Gessa, Glaser & Tinker, 2016; Hank & Buber, 2009). Depression is the leading cause of disability among older people (Ferrari et al., 2013), and the provision of grandchild care has complex associations with grandparents’ depressive symptoms, which is yet to be thoroughly examined (Arpino & Gomez-Leon, 2020). Specifically, the direction and strength of such associations differ across countries and individuals, and are influenced by the cultural and policy context, the characteristics of grandparents such as ethnicity, gender, age, marital status and whether they co-reside with their adult children and their grandchildren (Bordone & Arpino, 2019; Kim, Kang, & Johnson-Motoyama, 2017; Schwarz, Trommsdorff, Zheng, & Shi, 2010; Silverstein & Zuo, 2020). According to existing research, Southern European countries are permeated by strong filial norms, while Nordic countries tend to have relatively loose family ties and strong welfare states (Di Gessa, Glaser & Tinker, 2016; Hank & Buber, 2009). Previous studies have shown that such differences contribute to different levels of grandchild care provision in these countries, as the level of filial expectations or formal support provided by the welfare state interacts with the level of informal support provided by individuals (Di Gessa, Glaser, Price, et al., 2016; Neuberger & Haberkern, 2014). A recent piece of research found significant variance in the effects of grandchild caring on grandparents’ depressive symptoms in 16 European countries which may be related to different cultural contexts, whilst suggesting a need for further research to understand such differences (Bordone & Arpino, 2019).
The impact of grandchild caring on the depressive symptoms of grandparents may also differ in Eastern and Western societies as cultural context and social policies matter. Existing research showed that providing grandchild care is associated with fewer depressive symptoms in Asian countries (Chung & Park, 2018; Tsai, Motamed, & Rougemont, 2013; Xu, 2019), while the relationship between grandchild care provision and grandparents’ health is not positively/negatively linear in Western societies (Bordone & Arpino, 2019; Hughes, Waite, LaPierre, & Luo, 2007; Neuberger & Haberkern, 2014). However, no research has directly compared the effect of grandchild caring on grandparents’ depressive symptoms across Eastern and Western cultures. Conducting comparative research on such topics involving diverse populations may help produce useful lessons for policymakers. For instance, one recent study examining the relationship between older people’s living arrangement and their depressive symptoms in China and England found that the mechanisms of the relationship differed by the role of socioeconomic position (Hu, Ruiz, Bobak, & Martikainen, 2020). In order to address the research gap, this study aims to compare grandchild care provision and its impact on grandparents’ depression within a context defined by the Confucian culture, in the People’s Republic of China, and a Western context, including Northern and Southern European countries. Only a limited number of European countries are examined in the current study so as to illustrate a clear pattern. Referring to existing studies, Sweden and Denmark are selected as representative of Northern European countries, whilst Italy and Spain are chosen as representative of Southern European countries (Di Gessa, Glaser & Tinker, 2016; Hank & Buber, 2009; Neuberger & Haberkern, 2014).
The study is based on the longitudinal Harmonised Survey of Health, Ageing and Retirement in Europe (SHARE) and the China Health and Retirement Longitudinal Study (CHARLS) data collected between 2010–2015. This study addresses the following research questions: (1) What were the patterns of grandchild care provision and depression in China and Northern and Southern Europe between 2010–2015? (2) How does providing grandchild care impact on the depression among grandparents in China, Northern and Southern Europe?
Literature Review
Grandchild Caring in China and Europe
Researchers have used the frequency of grandchild caring or the number of hours of care to measure the intensity of grandchild care (Bordone & Arpino, 2019; Di Gessa, Glaser & Tinker, 2016; Hank & Buber, 2009; Liao, Qi, Xiong, Yan, & Wang, 2021). Recent evidence suggests that the prevalence, amount and frequency of grandchild caring vary across countries (Kim et al., 2017). In countries with strong filial culture such as China, over 60% of people aged over 45 provide grandchild care (Xu, 2019). A recent study shows that more than half of grandmothers (52%) and almost half of grandfathers (49%) aged between 50 and 84 provide care for their grandchildren in Europe (Bordone & Arpino, 2019). Research based on the SHARE data suggests that the provision of grandchild care is most prevalent in Nordic countries such as Denmark and Sweden, and least prevalent in Southern European countries such as Spain and Italy (Hank & Buber, 2009; Igel & Szydlik, 2011). By contrast, grandparents in Spain and Italy are most likely to provide frequent grandchild care (weekly or more often), and their counterparts in Denmark and Sweden are least likely to do so (ibid). Such pattern can be explained by the national differences in the contextual-structural factors including formal childcare provision and female labour force participation (Di Gessa, Glaser, Price, et al., 2016; Igel & Szydlik, 2011). Specifically, in Southern European countries with relatively low formal childcare coverage and low female employment rate, mothers are the main carers of their children; however, grandparents are likely to provide intensive grandchild care if the mother is working with little formal childcare available (Bordone & Arpino, 2019; Di Gessa, Glaser, Price, et al., 2016; Hank & Buber, 2009). By contrast, in Nordic countries with relatively high coverage of formal childcare and high female labour force participation rate, grandparents are not likely to provide intensive grandchild care due to the availability of formal childcare, however, they are likely to provide supplementary grandchild care occasionally (e.g. to drive grandchildren to nurseries or to provide care when the mother works extra time) (ibid).
Based on the literature review, it can be hypothesised that grandparents in China, Denmark and Sweden are more likely to provide grandchild care compared to their counterparts in Italy and Spain (H1), and grandparents in China, Italy and Spain are more likely to provide intensive grandchild care compared to their counterparts in Denmark and Sweden (H2).
Grandchild Caring and Late-Life Depression
Previous research on the relationship between grandchild care provision and the depression status of older people has presented mixed findings (Bordone & Arpino, 2019; Kim et al., 2017; Silverstein & Zuo, 2020). Most of existing studies used cross-sectional data which limited causal inference, and a few longitudinal studies reached contradictory findings (Kim et al., 2017). For example, some longitudinal studies show that caring for grandchildren contributes to fewer depressive symptoms among older people in Asian regions such as China, Korea and Taiwan (Chung & Park, 2018; Tsai et al., 2013; Xu, 2019). However, a more recent study focussing on complex intergenerational support patterns suggests that providing intensive grandchild care does not have a clear effect on the depressive symptoms among Chinese grandparents in the rural Anhui province, however, it is harmful for grandparents’ depression when they receive less economic support from their adult children (Silverstein & Zuo, 2020). Another longitudinal study based on the SHARE data shows that both intensive and non-intensive grandchild care provision bring benefits for grandparents’ self-rated health, whilst no significant associations are found between grandchild care provision and grandparents’ depressive symptoms (Di Gessa, Glaser & Tinker, 2016). Other researchers using the SHARE dataset found that the influence of grandchild care provision on grandparents’ depressive symptoms varied according to country, however, the differences did not have a clear pattern (Bordone & Arpino, 2019). The authors argued that culture can be an important factor moderating the association between grandchild care provision and the health of grandparents (ibid). Using the same dataset, Brunello and Rocco (2019) found that 10 additional hours of childcare per month increased depression among grandmothers by 1.1 percentage point and among grandfathers by 0.7 percentage point, respectively. Some researchers argued that the influence of grandchild care provision on the health of grandparents was due to between-individual differences only, thus within-individual analysis with fixed effects estimations did not yield significant results (Danielsbacka et al., 2019).
Gender differences permeate patterns of grandchild care provision. Although in recent decades both women and men are increasingly involved in many activities to an equal extent, childcare provision is still viewed as primarily women’s responsibility, particularly among older people (Wang & Mutchler, 2020). Many existing studies on grandparenting and its psychological effects on older people have focused only on female respondents (Chung & Park, 2018; Kim et al., 2017). However, evidence from previous research shows that the effect of grandparents’ childcare provision on their depression can vary by gender (Arpino & Gomez-Leon, 2020; Hughes et al., 2007). For example, Arpino and Gomez-Leon (2020) highlight that providing grandchild care only reduces the risk of having depression among European grandmothers, but not their male counterparts. Therefore, it is essential to analyse grandchild care provision and its effect on grandparents’ depression from a gender perspective.
Overall, the research on grandchild caring and its effects on the grandparents’ depressive symptoms remains at a preliminary stage and there is a need for theoretical and empirical development. Previous research on grandchild caring and late-life depression has mostly focused on a single country. In addition, most research in this area has focused on grandparents in western societies while relatively little research examined Asian grandparents (Kim et al., 2017). It is important to longitudinally examine the relationship between grandchild care provision and grandparents’ depression by gender, with a comparative perspective in both Asian and Western countries.
Theoretical Framework
The structured ambivalence theory has guided research investigating different impacts of grandchild care provision on depression or other psychological health among grandparents in different contexts (Bordone & Arpino, 2019; Connidis & McMullin, 2002; Kim et al., 2017; Neuberger & Haberkern, 2014). The concept of structured ambivalence refers to the conflict between individual behaviours and the individuals’ social context (Connidis & McMullin, 2002), and researchers have used the concept to explain how social or cultural expectations for grandchild care provision can influence the psychological health among grandparents (Bordone & Arpino, 2019; Neuberger & Haberkern, 2014).
In countries with a traditional familistic culture, grandparents are more likely to be the main source of childcare (Jappens & Van Bavel, 2012). Previous research has shown that in European countries with a stronger societal expectation towards grandparental childcare such as Italy, grandparents who do not provide grandchild care report a lower quality of life compared to their counterparts who provide such support (Neuberger & Haberkern, 2014), and the provision of grandchild care can have a protective effect against depression among grandparents due to the fulfilment of filial expectation (Xu, 2019). Hence, in the current study, it is hypothesised that intensive care for grandchildren fulfils cultural expectation and therefore has a protective effect against depression among grandparents in China, Italy and Spain (H3) (Neuberger & Haberkern, 2014; Silverstein & Zuo, 2020). By contrast, it is hypothesised that providing non-intensive grandchild care reduces depressive symptoms among grandparents in countries where norms of filial piety are comparatively less embedded such as Denmark and Sweden (H4) (Neuberger & Haberkern, 2014).
Methods
Data
The current study is based on the quantitative analysis of the Health and Retirement Study (HRS)-sister surveys, including the SHARE and the CHARLS. The first wave of the SHARE and the CHARLS data was firstly collected in 2004 and 2010, respectively, and the respondents have been followed up biennially (Beaumaster et al., 2018; Munich Center for the Economics of Aging (MEA), 2020). The harmonised versions of the datasets have recently been developed to encourage cross-national comparative studies, and the release of the Harmonised CHARLS version in 2018 has made it possible to conduct cross-country comparisons including China (Program on Global Aging, 2018). In order to compare information about grandparents in the same periods, the Harmonised SHARE Waves 4–6 and CHARLS Waves 1, 2 and 4 collected in 2010/1, 2012/3 and 2014/5 are used in their long form (observations are nested within individuals).
The longitudinal dataset represents some major advantages for researching this topic. First, it is appropriate for conducting international comparisons as multidisciplinary variables are defined consistently across the Harmonised SHARE and CHARLS (Beaumaster et al., 2018; Lee et al., 2018). Second, the use of the dataset provides a timely and necessary study of the research topics in the context of rapid global ageing and great sociodemographic changes. For example, researchers have used the HRS-sister surveys to examine mortality prediction in the USA, UK and Europe (Jing et al., 2018) and depression in the US, Europe, Korea and China (Jadhav & Weir, 2018). The current study is the first using the longitudinal dataset to investigate grandchild caring and depression across Asian and European countries, which exploits the nature of the surveys, informs learning between countries and can discuss the policy implications for a broader population. Nevertheless, using secondary data has some unavoidable limitations, which are discussed later.
Measures
Grandchild care provision
Both the SHARE and the CHARLS provide information on the provision of grandchild care by asking whether the respondents or their spouse spent any time taking care of their grandchildren during the previous year (1= yes, 0= no) (Beaumaster et al., 2018; MEA, 2020). Notably, in the CHARLS, the respondents who provided grandchild care were asked which of their children’s child(ren) they cared for, and how many weeks and hours per week during the previous year they spent taking care of their grandchildren. By contrast, in Waves 4–6 of the SHARE, the respondents were asked about the frequency of providing grandchild care (1= about daily, 2= about every week, 3= about every month and 4= less often). In order to obtain a comparable measure for intensive grandchild care provision among these countries, two dimensions are combined to define the intensity of care: the number of hours of care for the CHARLS data and the frequency of grandchild care provision for the SHARE data. Intensive grandchild care provision refers to care provided by respondents on a daily or weekly basis in the SHARE (see Hank & Buber, 2009), and those who provided grandchild care more than 40 hours per week (HPW) in the CHARLS (see Liao et al., 2021). Previous research has used either 30 or 40 HPW as a threshold for intensive grandchild care provision as they are (roughly) comparable to holding a full-time job (Di Gessa, Glaser, Price, et al., 2016; Liao et al., 2021; Thomson & Minkler, 2001).This study uses 40 HPW as the threshold because of two reasons. First, by referring to previous literature, providing grandchild care more than 30 HPW has been treated as providing intensive care in the Western context (Di Gessa, Glaser, Price, et al., 2016; Thomson & Minkler, 2001), whilst an alternative of 40 HPW as a threshold has been validated in the Chinese context (Liao et al., 2021). Second, based on the descriptive analysis not provided in this paper, using 40 HPW as the threshold is more appropriate following the principle of averaging the sample size of each category (i.e. 21% and 25% of Chinese respondents provided non-intensive grandchild care and intensive grandchild care, respectively, at baseline). As a result, and in line with previous research, a three-category variable capturing whether grandparents provided intensive grandchild care in the previous week was created: 1= No care, 2= Non-intensive care and 3= Intensive care (Bordone & Arpino, 2019; Liao et al., 2021).
Depression
Depression (Centre for Epidemiologic Studies Depression Scale (CES-D)) is measured by the summative score of 10 items (coded 0= rarely or none of the time, 1= some or a little of the time, 2= occasionally or a moderate amount of time, 3= all of the time) in the CHARLS, leading to a variable with range of 0–30 where higher values indicate more depressive symptoms (Beaumaster et al., 2018). The SHARE collects information about the respondents’ depressive symptoms using the 12-item EURO-D (1= yes, 0= no), and the total score ranges between 0–12 (MEA, 2020). The differences in measuring depression in these countries should not be a concern as previous research has validated them in different settings and showed that they are valid comparable measures (Chin, Choi, Chan, & Wong, 2015; Crimmins, Kim, & Solé-Auró, 2011; Jadhav & Weir, 2018).
Two forms of the depression variables are used in the current study: the normalised depression score (ranging between 0–12 for both the CHARLS and the SHARE), and a binary variable reflecting the self-reported depression status of respondents (1= yes, 0= no). As has been done in existing studies, the cut-off point for the category of being depressed is 4 for the SHARE (Arpino & Gomez-Leon, 2020; Dewey & Prince, 2005), and 12 for the CHARLS (Cheng & Chan, 2006; Cheng, Chen, Phillips, & McBride, 2016; Ni, Tein, Zhang, Yang, & Wu, 2017; Xu et al., 2016).
Covariates
A number of covariates related to depression were controlled in the analyses based on existing literature (e.g. Bordone & Arpino, 2019; Silverstein & Zuo, 2020; Wang & Mutchler, 2020). Four baseline health indicators, namely the respondents’ depression status (1= yes, 0= no), Activities of Daily Living (ADL) functional status (1= severe functional impairment, 2= moderate functional impairment, 3= full functional status), Instrumental Activities of Daily Living (IADL) functional status (the same categories as ADLs) and self-reported health (1= poor, 2= fair, 3= good) were included in the models. Sociodemographic variables including age (centred at 60), age squared, marital status (1= married or partnered, 0= others), educational attainment (1= less than lower secondary, 2= upper secondary & vocational training, and 3= tertiary), the employment status (1= working, 0= not working) and the logarithms of the individual income of respondents (in Euros) were controlled in the multivariate models (Bordone & Arpino, 2019; Di Gessa, Glaser & Tinker, 2016). The annual individual income for the Chinese sample was calculated based on the exchange rate in 2015 (€1Euro = 7 Yuan). The number of grandchildren under age 16 respondents had were also included (ibid). Intergenerational support including bi-directional economic transfers and weekly contact were also considered, however, these indicators were removed from the multivariate models in order to improve the model fit (Silverstein & Zuo, 2020; Wang & Mutchler, 2020).
Sample
The original Harmonised SHARE contains an initial sample of 58,129 individuals in 2010/1, 66,188 individuals 2012/3 and 68,188 individuals in 2014/5, and the original Harmonised CHARLS contains an initial sample of 17,500, 18,612 and 21,097 individuals in 2010/1, 2012/3 and 2014/5, respectively. Respondents who were aged between 50 and 90, had at least one grandchild under 16 years, and who had valid answers in questions related to grandchild care provision and depression at all three waves were kept, leading to the analytical sample of 4020 male respondents and 4621 female respondents. When comparing the effect of providing intensive grandchild care against providing non-intensive grandchild care, only respondents who provided grandchild care between 2010–15 were included, resulting in the sample size of 2296 grandfathers and 2468 grandmothers in the analysis as presented by Figures 1 and 2. The possible influence of the sample selection is discussed later. Four European countries including Denmark, Sweden, Italy and Spain were selected in order to reflect a clear Southern-Northern European trend. This is because Denmark and Sweden have been treated in previous research as representative of Nordic Countries with relatively loose family ties, and Italy and Spain have been shown to represent Southern European countries where filial norms are highly embedded (Neuberger & Haberkern, 2014). The Proportion of Grandparents Providing Intensive Grandchild Care in Italy, Spain, China, Sweden and Denmark, 2010–2015. Note: Providing intensive grandchild care refers to providing grandchild care on a daily and weekly basis in the SHARE, and for at least 40 HPW in the CHARLS. The sample includes respondents who had the experience of providing grandchild care between 2010–2015 (N = 2296 for grandfathers and N= 2468 for grandmothers). Error bars show 95% confidence interval; data weighted at the household level for each survey. Source: Author’s analysis of the Harmonised CHARLS and SHARE 2010–2015. Marginal Effects for Providing Intensive Grandchild Care Compared to Providing Non-Intensive Grandchild Care on Grandparents’ Depression, By Gender and Country. Note: Controlling for depressive symptoms, age, age squared, marital status, education, employment status, income, number of grandchildren, living arrangements, SRH, ADL disability and IADL disability at baseline. Providing intensive grandchild care refers to providing grandchild care on a daily and weekly basis in the SHARE, and for at least 40 hours per week in the CHARLS, and providing non-intensive grandchild care refers to providing grandchild care on a less than weekly basis in the SHARE, and for less than 40 HPW in the CHARLS. Number of observations (N): N = 4020 for grandfathers and N = 4621 for grandmothers. Source: Author’s analysis of the Harmonised CHARLS and SHARE 2010–15.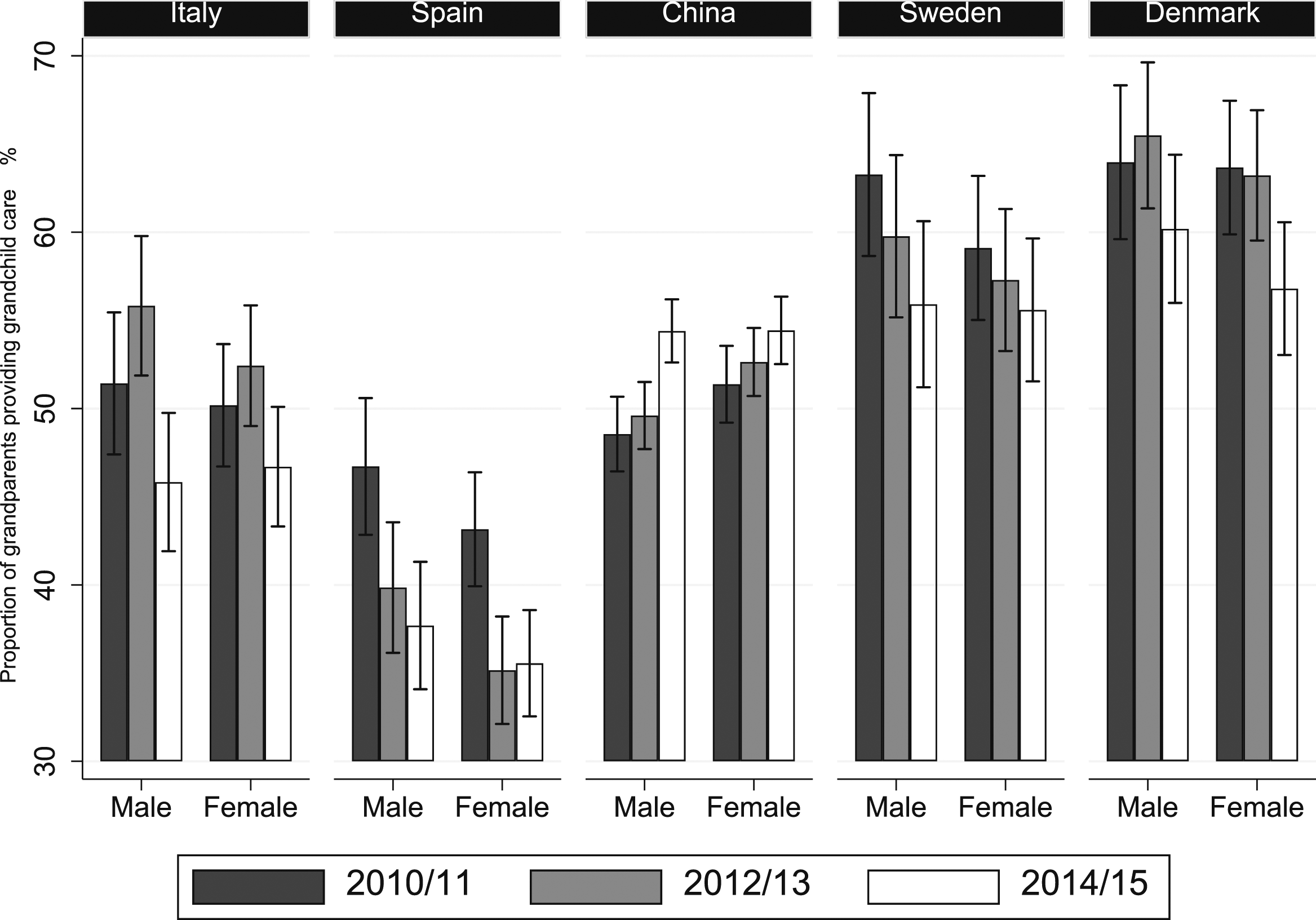
Descriptive Sample Statistics Based on the Baseline Sample.
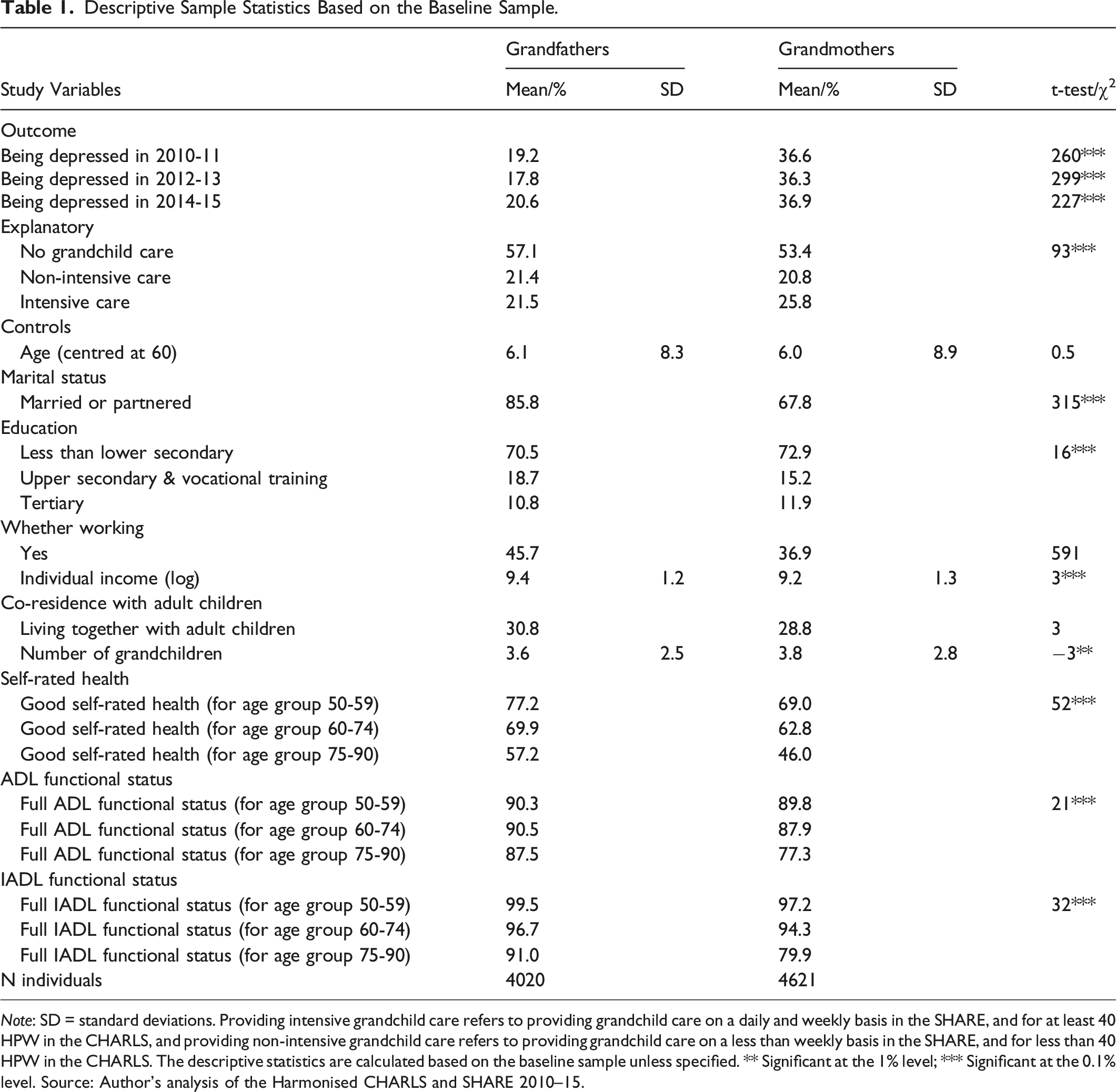
Note: SD = standard deviations. Providing intensive grandchild care refers to providing grandchild care on a daily and weekly basis in the SHARE, and for at least 40 HPW in the CHARLS, and providing non-intensive grandchild care refers to providing grandchild care on a less than weekly basis in the SHARE, and for less than 40 HPW in the CHARLS. The descriptive statistics are calculated based on the baseline sample unless specified. ** Significant at the 1% level; *** Significant at the 0.1% level. Source: Author’s analysis of the Harmonised CHARLS and SHARE 2010–15.
The average age of grandfathers and grandmothers were about 66, respectively, at baseline. Almost 86% of grandfathers were married or partnered at baseline, while the proportion was significantly lower among grandmothers (68%). The majority of respondents reported that they had received less than lower secondary education, and this proportion was higher among grandmothers (73%) compared to grandfathers (71%) at baseline. About 46% of grandfathers and 37% of grandmothers were working at baseline. The average annual individual income for grandfathers was significantly higher than grandmothers at baseline. Less than one third of grandfathers and grandmothers co-resided with their adult children at baseline. Grandparents had almost 4 grandchildren on average. In addition, a higher proportion of grandfathers reported good health and full (I)ADL functional status compared to grandmothers in all three age groups.
Analytical Strategy
Using the software of Stata V.16 (StataCorp, 2019), three steps of analyses were conducted. First, the provision of grandchild care, intensive grandchild care and depressive symptoms among grandparents between 2010 and 2015 were compared by country and gender. Second, lagged outcome models were used to examine the effects of grandchild caring on the grandparents’ depression score 2 years later, as has been done in previous research (Di Gessa, Glaser & Tinker, 2016). Specifically, the lagged outcome models provide estimates of the effects of grandchild care provision in 2013 on the normalised depression score of grandparents in 2015, controlling for the respondents’ depression and a number of covariates at baseline as discussed earlier. Controlling for the baseline health of respondents and using lagged outcome models to examine the effects help to reduce reverse causality in the estimation, as the predictor is measured preceding the outcome measure (Arpino & Gomez-Leon, 2020; Silverstein & Zuo, 2020). Thirdly, the marginal effects of providing non-intensive grandchild care and intensive grandchild care on grandparents’ depression score, compared to not providing grandchild care, and the marginal effects of providing intensive grandchild care on grandparents’ depression score, compared to providing non-intensive grandchild care, are plotted by country and gender. As shown in previous research, plotting the impact of grandchild caring on the predicted changes in the depression score eases the interpretation of the complex effects (Bordone & Arpino, 2019).
Results
Grandchild Care Provision in China and Europe
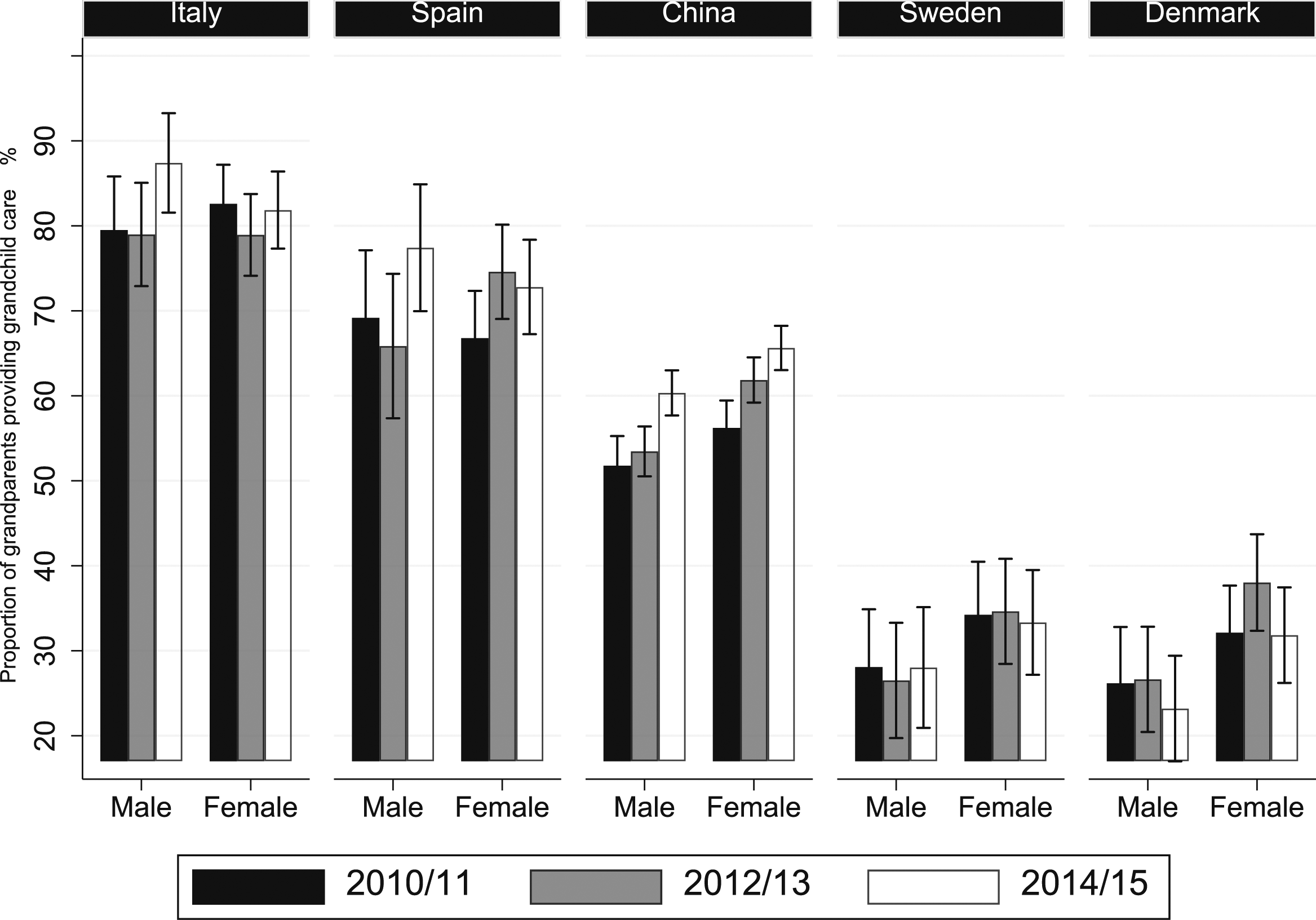
The proportions of grandparents looking after grandchildren in the five countries are provided by gender in Figure 3. Consistent with previous research findings (Hank & Buber, 2009; Igel & Szydlik, 2011), a North-South gradient in terms of the grandchild care provision is observed in Europe. The Proportion of Grandparents Providing Grandchild Care in Italy, Spain, China, Sweden and Denmark, 2010–2015. Note: error bars show 95% confidence interval; data weighted at the household level for each survey. Number of observations (N): N = 4020 for grandfathers and N = 4621 for grandmothers. Source: Author’s analysis of the Harmonised CHARLS and SHARE 2010–2015.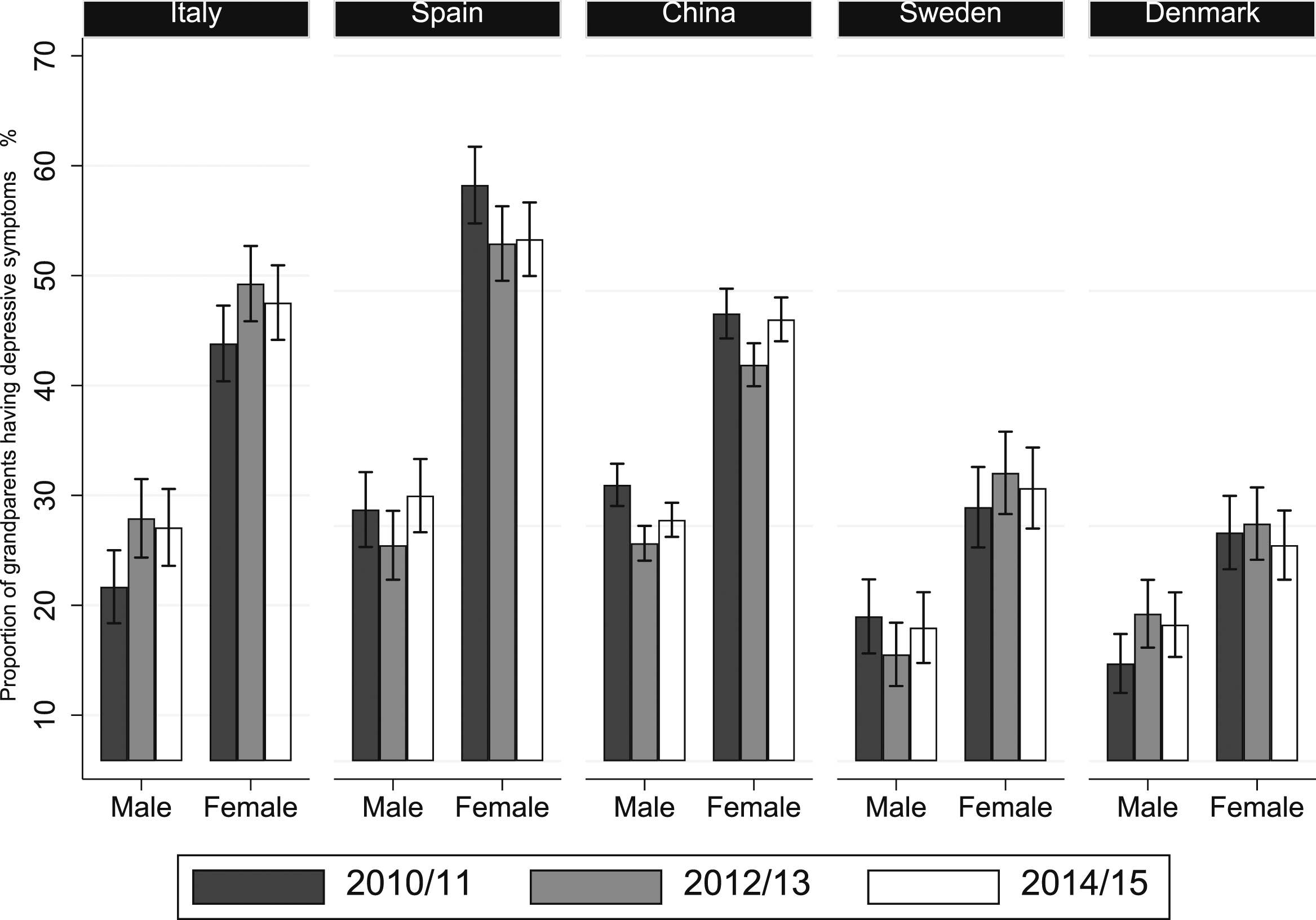
Specifically, Spain and Italy had the lowest proportion of grandchild care provision among people aged 50–90 (35–55%). A much higher proportion of grandparents in Denmark and Sweden (about 55–65%) provided grandchild care compared to their counterparts in Spain and Italy. The proportion of respondents providing grandchild care in China (about 50–55%) was higher compared to Spain, and lower compared to Denmark and Sweden. In terms of gender difference, the proportions of grandmothers providing grandchild care were lower compared to grandfathers in Spain, while such proportions were similar for grandfathers and grandmothers in Italy, China, Sweden and Denmark.
The patterns between the countries changed significantly when the intensity of grandchild caring was examined in the same five countries (Figure 1). The sample included respondents who had the experience of providing grandchild care between 2010–2015. Denmark and Sweden exhibited the lowest proportions of intensive grandchild care provision (20–40%), followed by China (about 50–65%). The respective proportions of Italy and Spain were about three times as high as in Denmark and Sweden.
Late-Life Depression in China and Europe
Figure 4 shows the proportion of grandparents reporting depressive symptoms over the five countries by gender. A North-South gradient was observed among these countries. Denmark and Sweden had the lowest proportions of reporting depression among grandparents between 2010 and 2015, and grandparents in Spain and Italy were the most likely to report depression, almost at double the rate compared to Denmark and Sweden. The pattern is consistent with the findings from previous research (Bordone & Arpino, 2019; Missinne, Vandeviver, Van de Velde, & Bracke, 2014). About one-quarter of grandfathers and almost half of grandmothers reported depressive symptoms in China, which was similar to Italy. In all five countries, a significantly higher proportion of female respondents reported depressive symptoms compared to their male counterparts. The Proportion of Respondents Reporting Depression in Italy, Spain, China, Sweden and Denmark, 2010–2015. Note: Respondents who had a depression score higher than 4 in the SHARE and respondents who had a depression score higher than 12 in the CHARLS are considered being depressed. Error bars show 95% confidence interval; data weighted at the household level for each survey. Number of observations (N): N = 4020 for grandfathers and N = 4621 for grandmothers. Source: Author’s analysis of the Harmonised CHARLS and SHARE 2010–15.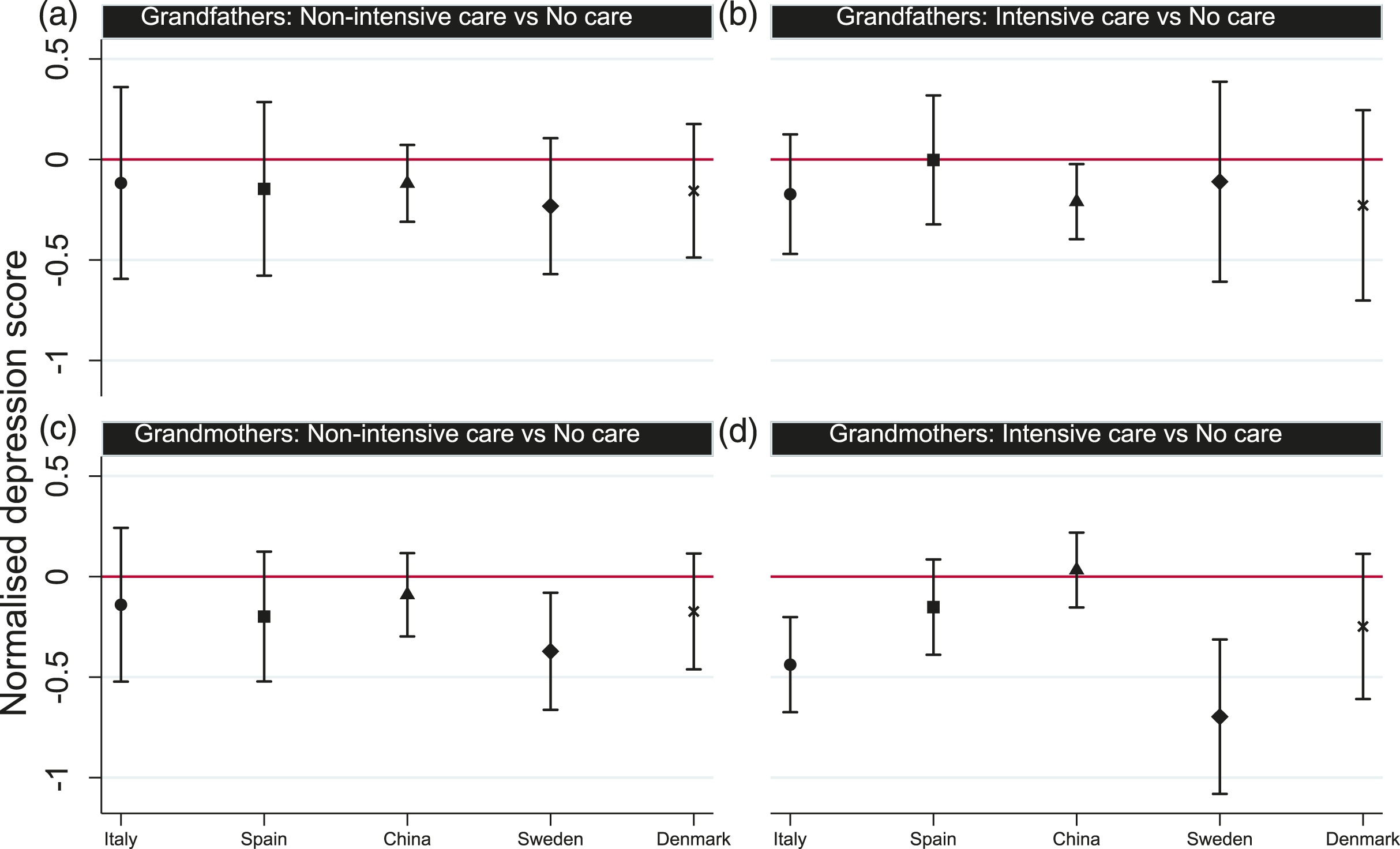
Grandchild Caring and Depression in China and Europe
Lagged Effect of Providing Grandchild Care on Grandparents’ Depression Score, Controlling for Baseline Depression, Socioeconomic and Demographic Characteristics.
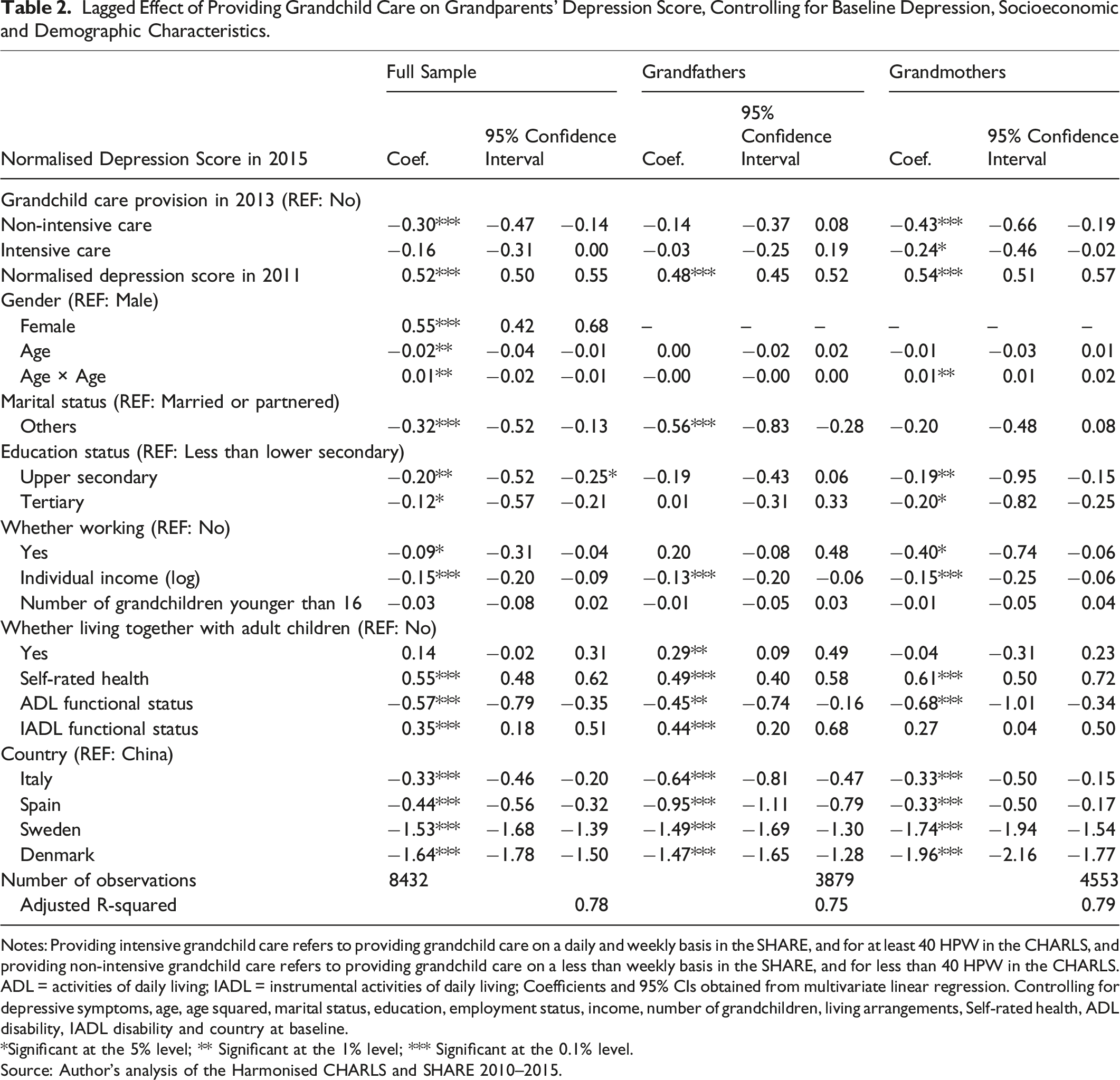
Notes: Providing intensive grandchild care refers to providing grandchild care on a daily and weekly basis in the SHARE, and for at least 40 HPW in the CHARLS, and providing non-intensive grandchild care refers to providing grandchild care on a less than weekly basis in the SHARE, and for less than 40 HPW in the CHARLS.
ADL = activities of daily living; IADL = instrumental activities of daily living; Coefficients and 95% CIs obtained from multivariate linear regression. Controlling for depressive symptoms, age, age squared, marital status, education, employment status, income, number of grandchildren, living arrangements, Self-rated health, ADL disability, IADL disability and country at baseline.
*Significant at the 5% level; ** Significant at the 1% level; *** Significant at the 0.1% level.
Source: Author’s analysis of the Harmonised CHARLS and SHARE 2010–2015.
Table 2 shows that overall, the provision of non-intensive grandchild care in 2013 was associated with lower depression score among grandparents 2 years later, even taking into account of the baseline depression status. Such positive effect was found among grandmothers, but not among grandfathers. Specifically, compared to grandmothers who did not provide grandchild care, those who provided non-intensive grandchild care and intensive grandchild care in 2013 reported lower depression score 2 years later. In addition, having higher depression score, being female, receiving less than lower secondary education, having lower income, having poorer self-rated health and (I)ADL health at baseline were significantly associated with higher depression score in 2015. Both grandfathers and grandmothers in Italy, Spain, Sweden and Denmark reported lower depression scores than those in China.
The effects of grandparents providing grandchild care on the depression score 2 years later were further investigated over the five countries by country and gender. The marginal effects shown in Figure 5a refer to the effect on the depression score in 2015 of providing non-intensive grandchild care (left panels, Figure 5a) and intensive grandchild care (right panels, Figure 5b), compared to not providing grandchild care in 2013 among grandfathers. Similar marginal effects for grandmothers are shown in Figure 5c (the effect of providing non-intensive grandchild care in 2013 on the depression score in 2015 among grandmothers, compared to not providing grandchild care) and 4d (the effect of providing intensive grandchild care in 2013 on the depression score in 2015 among grandmothers, compared to not providing grandchild care). Marginal Effects for Providing Grandchild Care Compared to Not Providing Grandchild Care on Grandparents’ Depression, By Gender and Country. Note: Controlling for depressive symptoms, age, age squared, marital status, education, employment status, income, number of grandchildren, living arrangements, SRH, ADL disability and IADL disability at baseline. Providing intensive grandchild care refers to providing grandchild care on a daily and weekly basis in the SHARE, and for at least 40 hours per week in the CHARLS, and providing non-intensive grandchild care refers to providing grandchild care on a less than weekly basis in the SHARE, and for less than 40 HPW in the CHARLS. Number of observations (N): N = 4020 for grandfathers and N = 4621 for grandmothers. Source: Author’s analysis of the Harmonised CHARLS and SHARE 2010–15.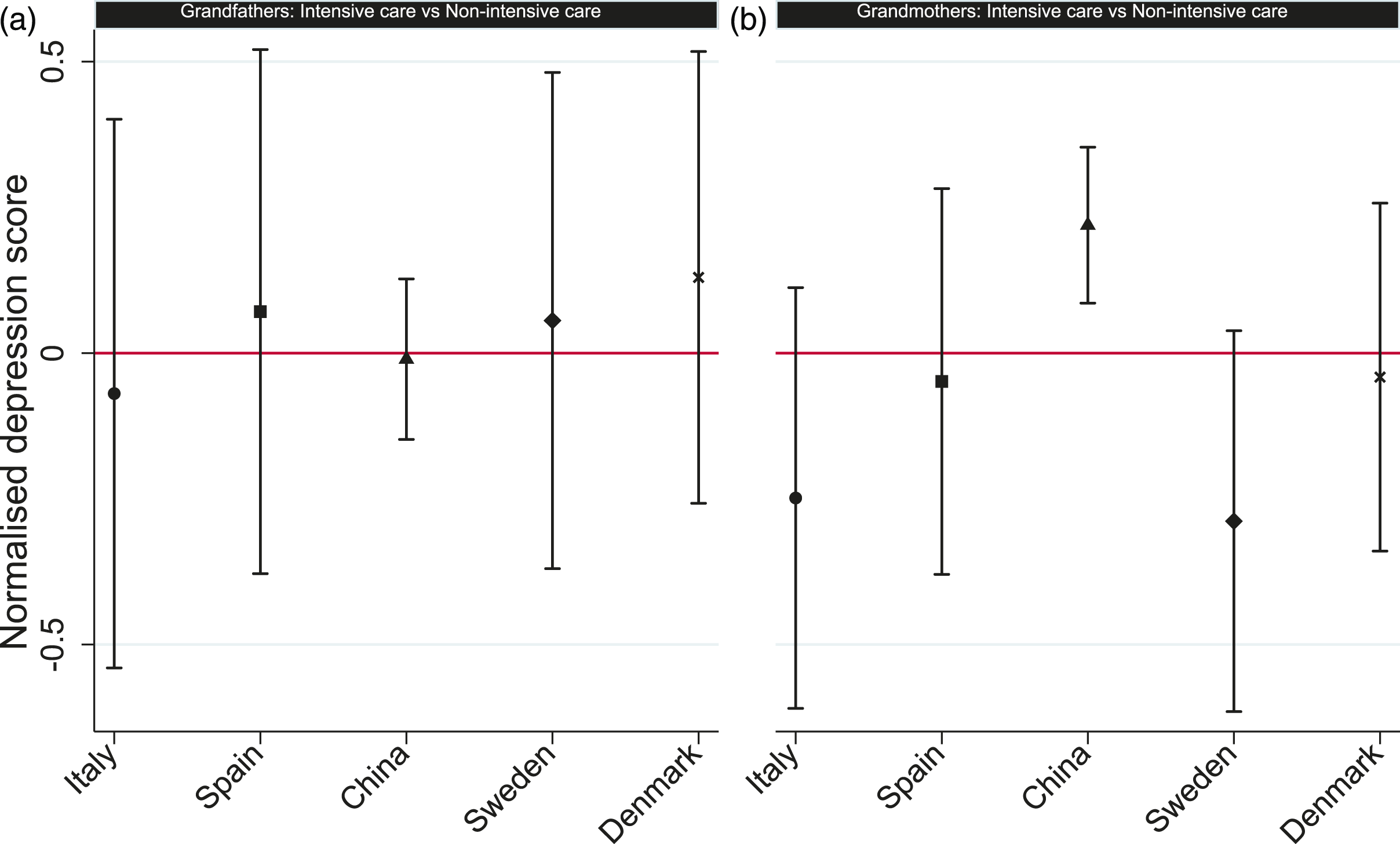
Figure 4a shows that compared to grandfathers who did not provide any grandchild care, grandfathers who provided non-intensive care did not report statistically different depression score in all five countries. However, compared to grandmothers who did not provide any grandchild care, grandmothers who provided non-intensive care in Sweden reported lower depression score 2 years later (Figure 5c). Furthermore, Figure 5b shows that compared to grandfathers who did not provide any grandchild care, grandfathers who provided intensive care in China reported lower depression score 2 years later. Similar relationship was found among grandmothers in Italy and Sweden (Figure 5d). Overall, compared to grandfathers, the same models for grandmothers produced more pronounced results.
In order to disentangle the effect of providing grandchild care and the effect of its intensity, a comparison of the effect of providing intensive and non-intensive grandchild care on the respondents’ depression score is provided in Figure 2. The estimated marginal effect shows that compared to providing non-intensive grandchild care, grandmothers providing intensive care had a statistically significant higher depression score in China. Such effect was not found in the four European countries.
Discussion
With the global trend of population ageing and the increasingly significant role of grandparents in grandchild care provision, it is crucial to understand the complex impact of grandchild caring on the grandparents’ psychological health. Little is known about whether such impact varies across country and culture (Bordone & Arpino, 2019; Kim et al., 2017), particularly across Eastern and Western cultures. To our knowledge, this study is the first to examine the level of grandchild care provision and depression among grandparents in China and European countries over time, and assess cross-country difference in the impact of grandchild care provision on the grandparents’ depressive symptoms using the longitudinal dataset harmonising the CHARLS and the SHARE. Findings from this study contribute to the literature on the implications of grandchild caring for grandparents, and demonstrate the cross-national differences in the impact of grandchild caring on the depression among grandparents across China and Europe.
This study shows that grandparents in Denmark, Sweden and China are most likely to provide grandchild care, followed by Italy and Spain, which supports H1. The Southern-Northern Europe gradient in the provision of grandchild care is consistent with previous research findings (Di Gessa, Glaser, Price, et al., 2016; Hank & Buber, 2009; Igel & Szydlik, 2011). As evidenced earlier, grandparents in China have a high likelihood of providing grandchild care due to their high sense of traditional family values (Silverstein & Zuo, 2020; Xu, 2019). The current study adds to the literature by showing that the prevalence of grandchild care provision in China is a little lower compared to Denmark and Sweden, and significantly higher than Spain.
In addition, grandparents in Italy, Spain and China are more likely to provide intensive grandchild care compared to their counterparts in Denmark and Sweden, which supports H2. The results in European countries are consistent with existing evidence (Hank & Buber, 2009). The higher prevalence of intensive grandchild care in Italy and Spain compared to Denmark and Sweden is explained by the stronger family ties, and the lower levels of formal childcare provision and female labour force participation in Southern European countries compared to Nordic countries (Di Gessa, Glaser, Price, et al., 2016; Igel & Szydlik, 2011). In particular, about 25% of grandfathers and 30% of grandmothers provide intensive grandchild care in China between 2010–2015, which is consistent with recent research findings (Liao et al., 2021). The relatively high proportion of intensive grandchild care provision in China may be due to the fact that the younger generation is increasingly involved in paid work and by the low coverage of formal child care in China (Silverstein & Zuo, 2020; Zhao & Zhang, 2019).
The results based on the multivariate linear models partly support H3 and H4: providing intensive care for grandchildren reduces the depression score for grandmothers in Italy (H3) (the same effect has been found in Sweden, but not in Spain), and providing non-intensive grandchild care reduces depressive symptoms among grandmothers in Sweden (H4) (but not in Denmark). The same models for grandfathers show different results. Specifically, compared to grandfathers who do not provide any grandchild care in 2013, grandfathers who provide intensive grandchild care in China report lower depression score 2 years later. The results highlight the importance of using gender role perspectives to understand grandchild caring, and further suggest a possibility of interactions between grandparents’ gender and country level factors (Bordone & Arpino, 2019; Wang & Mutchler, 2020).
The findings in European countries are partly explained by the Structural Ambivalence Theory (Bordone & Arpino, 2019; Neuberger & Haberkern, 2014). Specifically, in Italy where the norms of providing grandchild care are widely accepted, providing intensive grandchild care fulfils cultural expectations and favours positive feelings, and therefore reduces the grandparents’ depressive symptoms; whilst in countries with low expectations for grandchild care provision such as Sweden, providing non-intensive grandchild care has a protective effect against the grandparents’ depressive symptoms. This is because providing non-intensive grandchild care enhances self-esteem and contributes positively to the psychological health of respondents, especially in countries with low expectations towards grandparenting (Di Gessa, Glaser, Price, et al., 2016; Kim et al., 2017). However, further investigation is needed to understand the findings which are not consistent with the hypotheses. For example, the positive effect of providing intensive grandchild care on grandparents’ depression was found among Swedish grandmothers, but not among Spanish grandmothers. In addition, the effect of grandchild care provision on grandparents’ depression was not consistent in European countries with similar characteristics, that is, different results were found among grandparents in Sweden or Denmark. This suggests the need of incorporating specific country level factors in future research to better understand the complex pattern.
The results for Chinese grandparents partly support hypothesis H3, that is, the provision of intensive grandchild care has a beneficial effect on the depressive symptoms of Chinese fathers, compared to grandfathers who do not provide grandchild care. Interestingly, the findings also suggest that in China, compared to grandmothers who provide non-intensive grandchild care, grandmothers who provide intensive grandchild care have more depressive symptoms. The Structural Ambivalence Theory on its own cannot explain such complex findings in China, suggesting a need for further methodological and theoretical development in this area.
Strengths and Limitations
This study utilises the CHARLS and the SHARE datasets in order to compare the relationship between grandchild caring and depressive symptoms among grandparents in China and Europe, contributing to a comparative understanding of the research topic based on more diverse populations.
Theoretically, this study shows that the Structural Ambivalence Theory explains the different relationship between grandchild caring and depressive symptoms in Italy and Sweden, which provides further evidence to previous research (Bordone & Arpino, 2019; Neuberger & Haberkern, 2014). However, the results suggest that the theory may not apply to China, Spain and Denmark, which is an important added contribution of this study, as the theory has not been applied previously to study this topic in an Asian context. This shows a need for theoretical development to better understand the cross-national differences in the effect of grandchild care provision on grandparents’ depression.
Methodologically, this longitudinal study innovatively uses the three-wave Harmonised CHARLS and SHARE data to investigate the effects of grandchild care provision on the depressive symptoms of grandfathers and grandmothers 2 years later. On the one hand, the use of the internationally harmonised data contributes to understanding the homogeneity and heterogeneity in ageing processes across cultures (Lee et al., 2018). On the other hand, the lagged effects used in the longitudinal models help to reduce reverse causality, which strengthens our confidence in interpreting the causal relationship (Silverstein & Zuo, 2020).
However, the current study has some limitations. First, the measures of grandchild care provision and depressive symptoms in the surveys are self-reported. Hence, parts of the differences in the two variables may be due to reporting differences (Di Gessa, Glaser & Tinker, 2016; Hank & Buber, 2009). Previous research has validated the measures of grandchild caring and depression in the CHARLS and SHARE (Chin et al., 2015; Crimmins et al., 2011; Jadhav & Weir, 2018). In addition, the results from the models in Table 2 show that the major part of the differences in the variables are true underlying differences rather than reporting differences.
Second, only respondents who participated in all three waves of the surveys were included in the analytical sample. As respondents who drop out of the studies are more likely to have poor health (Di Gessa, Glaser & Tinker, 2016), the possible patterns of attrition may bias results (i.e. respondents included in the analytical sample have a low likelihood of reporting depressive symptoms). In the current study, comparisons between the characteristics of respondents in the analytical sample and the full sample were conducted, and analysis not shown here indicates that no significant differences were found in the depressive symptoms between the two groups (29.3% for the analytical sample and 28.9% for the full sample, with Chi-squared tests not statistically significant).
Finally, this study found cross-national differences in the effects of grandchild care provision on the grandparents’ depressive symptoms. However, due to the limited availability of information from the CHARLS and SHARE datasets, specific cultural effects (i.e. country-specific cultural norms, welfare policies and family closeness at a household level) and children/grandchildren characteristics could not be investigated. An important area for future studies on grandchild caring and depression is to examine how specific cultural factors or children/grandchildren characteristics may moderate the causal effects of grandparental provision of childcare on their depression status, which may help to understand the complex effect found in this study.
Future work can also contribute to identifying the causal pathways between grandchild care provision and depression in different countries. For example, the CES-D and EURO-D scales can be distinguished into somatic and mood effects in order to develop a nuanced understanding of the depression pathways (Jadhav & Weir, 2018), taking into account the cultural differences. Including more diverse populations in future research can enrich our understanding of grandchild caring and its effect on late-life depression from a comparative perspective.
In summary, the current study demonstrates the complex relationship between grandchild caring and depression among grandparents, and how such relationship varies across country. The mechanisms of the relationship also differ across culture (i.e. the Structural Ambivalence Theory applies to Italy and Sweden but is not appropriate for Asian settings such as China). The findings from this study call for attention from both researchers and policymakers, as it is crucial to identify the causal pathways and to improve health and wellbeing among the older population worldwide.
Footnotes
Acknowledgments
This study used Gateway to Global Aging Data, produced by the Program on Global Aging, Health & Policy, University of Southern California. This study was approved by the University of Southampton’s Ethics Committee. The author thanks Maria Evandrou and Athina Vlachantoni for their helpful comments that improved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Economic and Social Research Council Post-Doctoral Fellowship under Grant number ES/V011456/1 and Economic and Social Research Council Doctoral Training Centre under Grant number ES/J500161/1.