
Abstract
Supporting an adolescent who has an emotional or behavioural disorder is challenging for parents. This article reports the findings of a qualitative study of parents’ perceptions of stigma associated with parenting an adolescent with a diagnosis of ADHD or depression. 40 parents (28 mothers and 12 fathers) took part in semi-structured interviews. The interview guide focussed on their parenting experience in social contexts such as interactions with friends, family and the wider community, and perceptions of their own parenting abilities and experiences. Thematic analysis was used to code and interpret the data. Parents felt that other people held ill-informed or dismissive views of what their child’s disorder entailed; they experienced parental self-blame; they engaged in efforts to normalize their child’s experiences and they reported being selective in deciding whether to talk to others about their child’s diagnosis. The implications of the findings for addressing stigma are discussed.
Introduction
Parents play an important role in their child’s pathway to mental health care, often acting as gatekeepers to accessing professional services (Reardon, Harvey, Young, O’Brien, & Creswell, 2018). In addition to dealing with a child’s symptoms and associated difficulties in academic and interpersonal functioning (Theule, Wiener, Tannock, & Jenkins, 2013), parents face the pressures of coping with or avoiding stigmatizing reactions from others (McIntyre & Hennessy, 2012). It is possible that for these parents, dealing with stigma may be even more onerous than dealing with difficulties that are inherent to the disorder itself. In Ireland, one-in-six 11–13 year olds has a current mental disorder (Cannon, Coughlan, Clarke, Harley, & Kelleher, 2013). The most common mood disorder experienced by these young adolescents is depression and the most common behavioural disorder is attention deficit hyperactivity disorder (ADHD; Cannon et al., 2013).
Globally, ADHD affects 63 million children and adolescents, with lower estimates for depression at 47 million (Polanczyk, Salum, Sugaya, Caye, & Rohde, 2015). The age of onset for ADHD is 7–9 years (Kessler et al., 2007), whereas mood disorders have low prevalence until early adolescence (Kessler et al., 2007), with the first episode of major depression typically occurring at around the age of 14 years (Lewinsohn, Clarke, Seeley, & Rohde, 1994). For young people with ADHD, approximately 15% will continue to meet the full diagnostic criteria by age 25 years (Faraone et al., 2006) and persistence into adulthood is associated with higher ADHD symptom severity and the presence of comorbid disorders including conduct disorder and depression (Caye et al., 2016). In the case of depression, of those who attend Child and Adolescent Mental Health Services (CAMHS) in childhood or adolescence, over 50% have recurrent depressive episodes or persistent depression that continues into adulthood (Dunn & Goodyer, 2006). In terms of the co-occurrence of these disorders, approximately 1-in-10 children with ADHD is experiencing comorbid depression (Blackman, Ostrander, & Herman, 2005) and this has been linked to higher ADHD symptom severity (Connor et al., 2003).
Stigma is a multifaceted construct and is commonly described in terms of stereotypes, prejudice and discrimination (Corrigan, Kerr, & Knudsen, 2005; Hinshaw, 2005). In childhood and adolescence, stigma often plays out in the peer domain (O’Driscoll, Heary, Hennessy, & McKeague, 2012), and experiences of discrimination in the form of bullying or peer exclusion are not uncommon for young people with a diagnosed mental health problem (Moses, 2010). These stigma experiences not only impact the adolescent but also their parents. Given their role in helping the young person to navigate social and interpersonal difficulties, parents may experience ‘vicarious stigma’, a tendency to worry about the impact of stigma on their child (Corrigan & Miller, 2004). In addition, parents themselves may experience courtesy stigma (stigma by association), where they feel devalued because of their association with the individual who has a mental health issue (Goffman, 1963; Heflinger & Hinshaw, 2010). This form of stigma has been reported in the wider literature on the experience of caring for a family member with an illness, for example, Alzheimer’s disease (Werner, Goldstein, & Buchbinder, 2010) and in relation to parenting a teen with ADHD (Koro-Ljungberg & Bussing, 2009). A further, distinct aspect of the stigma experience for these parents occurs when they experience blame and judgement on the basis of their own parenting abilities, rather than merely due to their association with their child, whereby prejudice, stereotyping and discrimination is directed towards the parent themselves (Eaton, Ohan, Stritzke, & Corrigan, 2016; Francis, 2012). Parenting efforts may be judged publicly, by other people who encounter the adolescent, and privately, by the parent themselves (Harden, 2005). As the focus of stigma in this case is on the parent, not the young person, this form of stigma has been called ‘parent blaming’ or ‘bad parent stigma’ in the literature (Eaton et al., 2016; Francis, 2012). There is evidence that this form of stigmatization comes both from family members and the wider community (Mofokeng & van der Wath, 2017). For example, parents of children with ADHD often report that other people do not take the diagnosis seriously (McIntyre & Hennessy, 2012) or that they are using the diagnostic label as an ‘excuse’ for the child’s behaviour (Peters and Jackson, 2008). Investigating stigma in relation to both depression and ADHD is important because there is evidence that stigma varies depending on the type of mental disorder in question (Walker, Coleman, Lee, Squire, & Friesen, 2008).
As a consequence of parent blame, parents may come to feel that their parenting efforts are inadequate and endorse the idea that they are personally responsible for their child’s problems (Eaton et al., 2016; Singh, 2004). The experience of being judged by others can, in turn, contribute to feelings of self-blame and distress for the parents (Eaton et al., 2016; Harborne, Wolpert, & Clare, 2004). Eaton et al. (2016) suggest that to fully understand how parents of children with mental health problems experience self-stigma, we must go beyond merely focussing on courtesy stigma. They propose that self-stigma arises when a parent becomes aware of the judgements and blaming reactions by others towards them, leading to self-doubt and social avoidance, followed by a belief that they are an inadequate parent and to blame for their child’s problems. This conceptualization shows similarities to the ‘three As’ model which describes self-stigma as the awareness, agreement and application of stigma to the self by persons who have a mental health problem (Corrigan & Watson, 2002). In the case of self-stigma experiences for parents of children with mental health problems, the key difference is that stigma arises in response to their perceived failure to meet a ‘good parent’ ideal, rather than due to any inherent characteristic of the parent themselves or their association with the child (Eaton et al., 2016).
Living with a concealable stigmatized identity, such as a mental health diagnosis, involves making decisions about whether to hide the diagnosis or disclose it to other people. Disclosure decisions are relevant to a range of stigmatized health problems, such as HIV-positive diagnosis (Varga & Brookes, 2008) and exploring how people open up to others can reveal a lot about how they anticipate and cope with stigma. Issues surrounding concealment and disclosure apply to parents of young people with diagnosed mental health problems (Eaton, Ohan, Stritzke, Courtauld, & Corrigan, 2017). Parents of children/adolescents with ‘invisible’ mental health problems have some degree of choice as to whether or not they disclose their child’s mental health problem in social encounters with others (Koro-Ljungberg & Bussing, 2009). Moen, Hall-Lord, and Hedelin (2011) found that parents of children with ADHD controlled the amount and type of information relating to their child’s diagnosis that they shared with others. Similarly, McIntyre and Hennessy (2012) reported that some parents decided to hide the fact that their child had ADHD due to a fear of their child being labelled. Concerns around labelling have also been reported by parents of children with emotional disorders. Parents in one qualitative study expressed fear that the diagnostic label of an anxiety disorder would lead to negative social consequences, such as teasing, by the child’s peers (Chavira et al., 2017).
Although labelling and disclosing their child’s mental health problem may be necessary and perhaps beneficial in some contexts (e.g. school), making other people aware of the issue poses a threat to the image of ‘normality’ that many parents wish to maintain (Koro-Ljungberg & Bussing, 2009). This fear of labelling is in line with Modified Labelling Theory (MLT; Link, Cullen, Struening, Shrout, & Dohrenwend, 1989) which suggests that labelling people as ‘mentally ill’ contributes to stigmatization (see Hinshaw, 2007). Recent findings suggest that children and adolescents stigmatize peers in response to direct observation of behaviours as opposed to labels; however, for adults, the addition of a label triggers a stigmatizing response (Kaushik, Kostaki, & Kyriakopoulos, 2016). Despite this, diagnostic labels may have positive connotations for parents in so far as they can be used as a tool for explaining the young person’s behaviours and attributing the difficulties to factors beyond the parent’s control. For example, previous research suggests that receiving a diagnosis of ADHD is associated with diminished parental self-blame and feelings of relief (Larson, Yoon, Stewart, & DosReis, 2011; Moen et al., 2011).
An important narrative running through previous research findings is parents’ quest to manage an identity that is known to be stigmatized. There is a sense of striving to achieve and maintain ‘normality’ despite difficulties presented by the young person’s experience of mental health problems (Frigerio & Montali, 2016; Koro-Ljungberg & Bussing, 2009). To avoid prejudice or discrimination by others, parents often work to portray themselves and their child as ‘normal’ (Koro-Ljungberg & Bussing, 2009). Some parents who took part in Koro-Ljungberg and Bussing’s qualitative study ‘minimised’ or downplayed the impact that ADHD had on their lives. Interpreting the behaviour of a young person diagnosed with ADHD as ‘normal’ was used as a stigma management technique achieved by rationalizing behaviour as age-typical and/or by interacting with other families with an adolescent with the same mental health problem.
The present study was conducted in Ireland, where mental health stigma is currently considered a prevailing societal issue (See Change, 2017). There is evidence that Irish children and adolescents report stigma towards peers who display deviant behaviours (O'Driscoll, Heary, Hennessy, & McKeague, 2015). Findings from one qualitative study conducted in Ireland suggest that young people with ADHD or depression experience peer stigmatization and self-blame and that they sometimes hide their mental health problem in order to avoid stigma (McKeague, Hennessy, O’Driscoll, & Heary, 2015). Despite this evidence, and although stigma prevention campaigns have been developed in Ireland (e.g. the See Change Green Ribbon campaign), at the time of writing there were no published intervention studies that focussed specifically on addressing the issue of mental health stigma experienced by Irish children, adolescents or their parents. As a precursor to developing such interventions, we need to find out more about how these individuals experience stigma. The views of parents will be explored in this article.
Research on stigma experienced by parents of children/adolescents with emotional and behavioural disorders has increased considerably in the past two decades, yet most of this research has concentrated on the mothers of adolescents diagnosed with behavioural disorders such as ADHD. ADHD and depression are both common child/adolescent disorders, but with very different symptoms (predominately behavioural vs. predominantly emotional). Parents of children/adolescents with ADHD tend to cite over-activity or impulsivity as contributing to judgemental responses by others, but less is known about whether parents of adolescents with depression face similar stigmatizing responses, and if so, what the nature and basis of these reactions might be. One area of interest is whether perceptions of stigma are similar or different for parents with experience of different types of disorder, and whether certain types of stigma-related perceptions might be more salient for one group than the other, or if stigma-related concepts (e.g. anticipated stigma) might be equally applicable to both groups.
Based on the literature, it is assumed that reacting to stigmatizing responses from others would be a personal and emotive experience. This study did not ask parents questions that use the term ‘stigma’ explicitly. This has not been the case in previous research (e.g. Eaton et al., 2016), where interview questions have typically referred extensively to ‘stigma’, regardless of whether parents spontaneously mention this as something that is relevant to them. The rationale behind our approach was to allow parents to mention stigma only if perceptions of stigma were central to their experience of parenting. In addition, a noted limitation of previous research, the exclusion of fathers, has been addressed in this study. The aims of this study are to explore parents’ perceptions of stigma and to examine the applicability of the stigma construct to parents of young people diagnosed with two common emotional and behavioural disorders, through qualitative accounts of the parenting experience.
Method
Design
The study used a qualitative design. Parents’ personal experiences were explored using semi-structured interviews with open-ended questions. The interview guide focussed on their parenting experience in social contexts such as interactions with friends, family and the wider community, and perceptions of their own parenting abilities and experiences (see Supplementary Material). Questions focussed on both positive and negative aspects of parents’ experiences. Probes were used where necessary to elicit further discussion.
Data Collection
Ethical approval was sought and granted by the Ethics Boards of the relevant CAMHS and university ethical approval was granted by University College Dublin. Participants provided written informed consent.
Three CAMHS services were involved in participant recruitment. Clinicians identified children/adolescents who were eligible to take part and a letter was sent to the parent(s)/primary caregivers of these young people. Leaflets and information sheets on the study were also made available to parents/primary caregivers when they visited CAMHS for their child’s appointment. Participant recruitment continued until uptake from suitable families ceased, as opposed to being based on data saturation.
Sample
Characteristics of Child/Adolescent Participants.
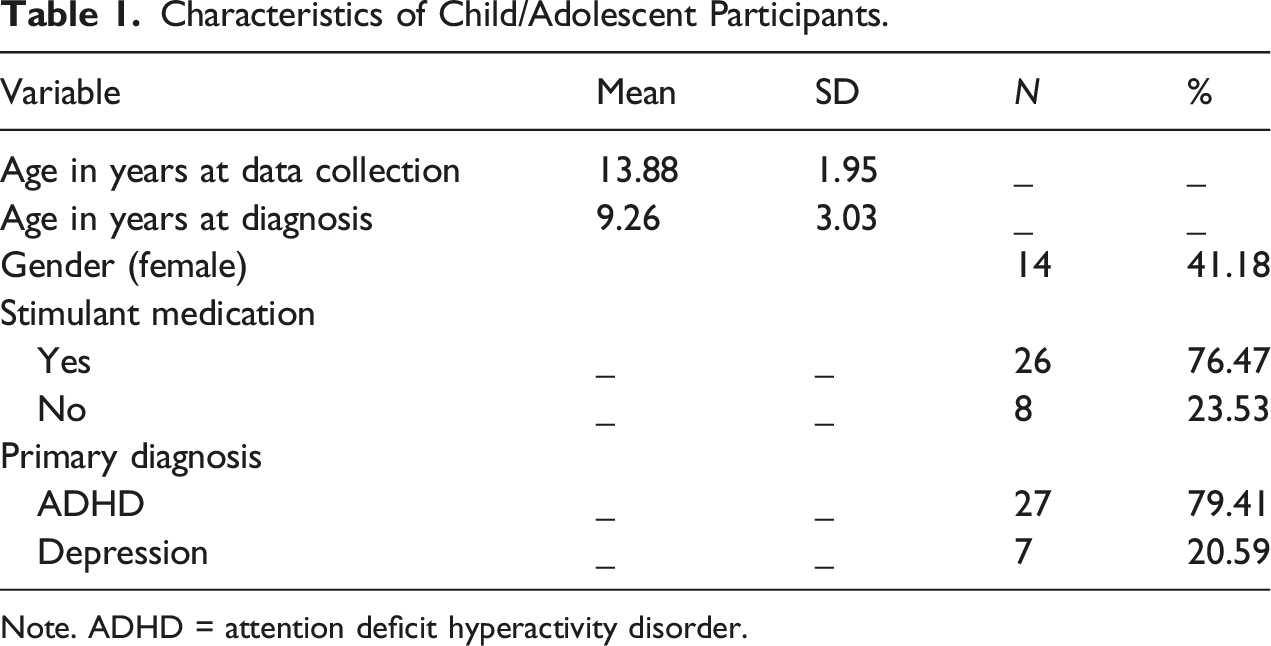
Note. ADHD = attention deficit hyperactivity disorder.
Characteristics of Parent Participants.
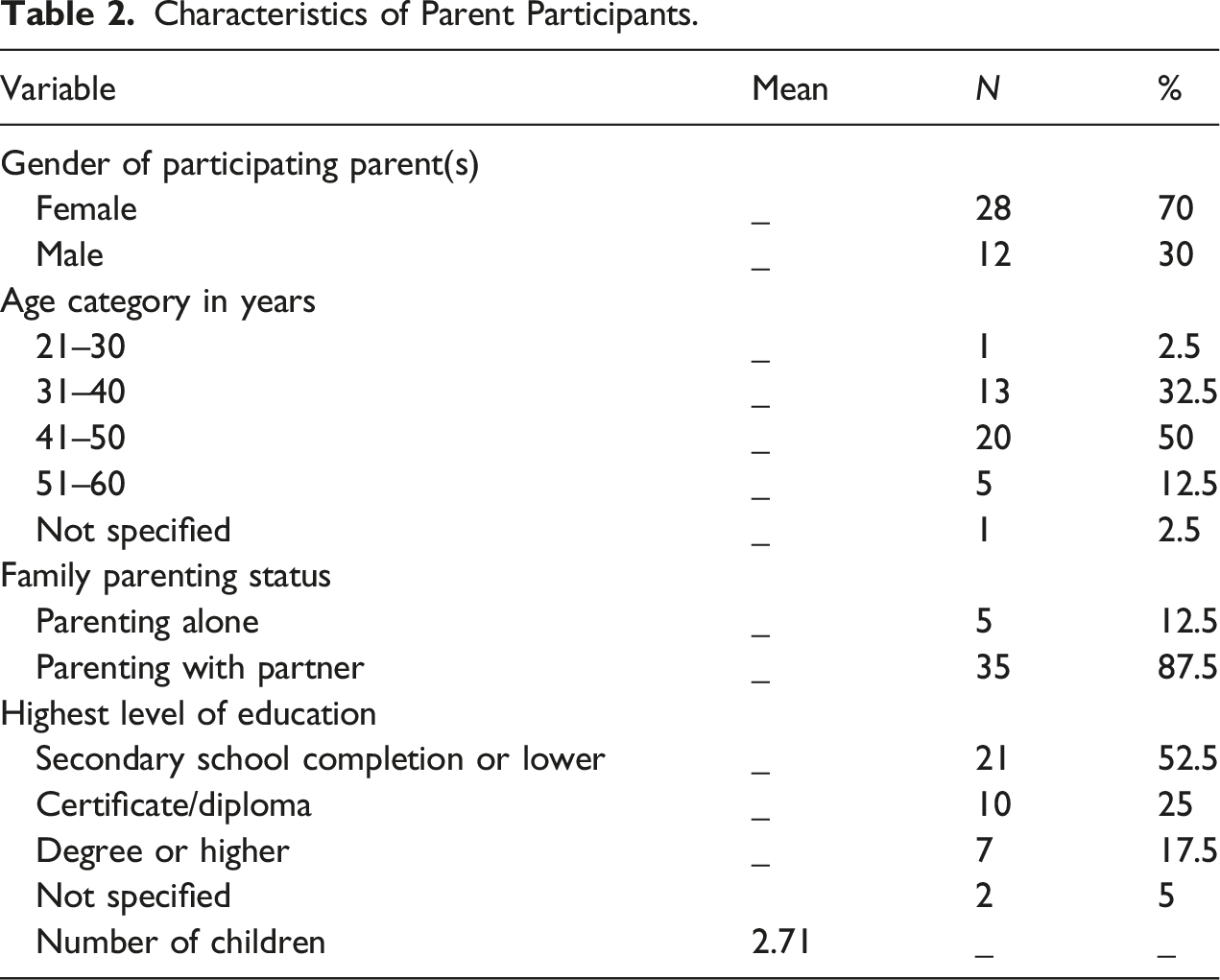
In some cases, both of the child’s parents took part in the study (n = 9); however, in the majority of cases, only one parent was interviewed (n = 22; three fathers). Therefore, in total, 31 interviews were conducted and 40 parents took part (12 fathers). Whether one or two parents/caregivers took part was at the discretion of the parent to whom the participant recruitment letter was addressed. Parents were given the option to take part either at home or in an office space in the CAMHS setting. The majority of families (74%) chose to take part in the family home. The average interview length was 46 minutes. In total, transcripts amounted to 277, 000 words of text. In order to allow readers to ‘situate the sample’ (Elliott, Fischer, & Rennie, 1999), demographic details for participants are provided.
Data Analysis
All interviews were conducted and transcribed verbatim by the first author. The names of these individuals and their children have been changed to ensure anonymity. Pseudonyms were selected using an online name generator.
A hybrid approach of inductive and deductive coding (Fereday & Muir-Cochrane, 2006) was used in the development of a coding frame. Codes were developed from the parent interview transcripts (inductive), consideration of study research questions (deductive) and the researchers’ awareness of the literature and research findings on this topic (deductive).
Interviews were analyzed using thematic analysis (Braun & Clarke, 2006, 2013). Following initial reading and rereading of the interview transcripts, codes were developed and refined by merging codes until all available codes represented a conceptually distinct aspect of stigmatization. At this point, the interview transcripts were saved to QSR NVivo.10 and codes were applied to each transcript. Data that were deemed unrelated to the issue of stigma were not coded. As each interview was analyzed, the researchers remained open to the possibility of making further revisions to the codes. Similar codes were often collapsed or divided into separate codes.
The codes were sorted into themes and subthemes and these were subsequently reviewed and refined (Braun & Clarke, 2006). The final stage of data analysis involved naming the themes and subthemes (Braun & Clarke, 2006) and careful selection of extracts from the data to illustrate each one (Elliott et al., 1999).
Inter-rater reliability analysis was conducted on a sample of the data (10%), with the second author acting as second rater (kappa = 0.75), 95% CI (0.705, 0.799).
Results
Four key themes were identified: (1) Parenting an adolescent with a diagnosed emotional or behavioural disorder in an ill-informed and dismissive society; (2) the experience of parental self-blame; (3) normalizing the young person’s disorder and (4) to disclose or not disclose. The relevance of these themes to parents’ perceptions of stigma and potential experience of self-stigma will be discussed.
Parenting an Adolescent With a Diagnosed Emotional or Behavioural Disorder in an Ill-Informed and Dismissive Society
When talking about people’s reactions to their child’s diagnosis, parents said that other people did not understand the diagnosed disorder or had prejudiced views of what it entailed. This lack of understanding manifested in different ways. For example, some parents said that other people did not always take the diagnosis seriously. Parents expressed concern that people do not consider ADHD to be a ‘real’ disorder. This appeared to be associated with prejudiced views, including the perception that their child was ‘wild’ or that the diagnosis is merely an excuse for inappropriate behaviour. Meredith (daughter, 16, ADHD) felt that: ‘A lot of people’s attitude is it’s just a makey-uppy thing, you know, for wild kids’. Parents of adolescents with depression also felt that other people held inaccurate or unfair views. The possibility that other adults view adolescents diagnosed with depression as being spoiled was described by Georgina (daughter, 14, depression): ‘Most of them would think in general that the child is spoiled and being over-indulged’.
Participants also said that other adults could not tolerate the young person’s behaviour. This issue was particularly salient for parents of teenagers with ADHD. One consequence of this intolerance was that it impacted other people’s willingness to look after the child. Harriet (twin sons, 14, ADHD) commented that family members were unwilling to look after the boys: ‘Nobody would offer to take them! Who in their right minds would offer to take two ADHD kids!’ Parents of young people with depression also perceived other adults as intolerant. Pearl (son, 15, depression) said: ‘...people wouldn’t be tolerant of it like, so people would, friends would say to me “Jesus I don’t know how you’re living with someone like that”’.
The Experience of Parental Self-Blame
A number of parents specifically mentioned how other adults made judgements about their parenting abilities, and some parents felt that they were viewed as responsible for the difficulties that their child was facing. This form of stigma was experienced irrespective of the type of diagnosis. Daphne (daughter, 13, depression) described how some people attributed her daughter’s difficulties to the fact that she was: ‘...minding them [her children] at home all the time, and babying her’. Rosie (daughter, 15, depression) considered that people were judging her family: ‘They’d say, “Well obviously there’s something going on in that house” and “why should a child from a normal background suffer with depression and anxiety and things like that?”’
Despite their perception that they were being blamed and judged in this way, the majority of parents were also able to reflect on experiences of support and acceptance by others. Most parents had at least some experience of other people reacting in a positive manner upon finding out that the child had a diagnosis. For example, Lindsey (daughter, 14, depression) recalled receiving support from friends and family whom she confided in: ‘I suppose it makes them sad to think that, that she would be experiencing it [depression], but [they were] very supportive; [...] they’d do anything that they could’. Similarly, Liliana (son, 11, ADHD) pointed out that: ‘Everybody’s been very open, and you know, accepting and that’.
Parents reported experiencing self-stigma, whereby they doubted their own ability as parents and believed the stigmatizing views of others to be true. Bree (son, 11, ADHD) said that: ‘I thought it was kinda my fault. I blamed myself first, you know, because I’m not setting enough rules and boundaries and things’. Pearl (son, 15, depression) said that: ‘...you get upset with yourself because you say, we weren’t listening to him. He must have been trying to tell us something. We missed this, and we missed that’. Many of the parents’ comments about self-blame referred to a previous time in their child’s life. Greg (son, 16, ADHD) pointed out that when his son received a diagnosis this removed some of the blame: ‘I suppose there was a little bit of relief that there wasn’t something wrong with us, as parents’. Similarly, Lindsey (daughter, 14, depression) said that: ‘[Psychologist] told me one time that it was nature not nurture, and I suppose I grasped onto that, and it just, it made it a little bit easier [...] that this is bigger than anything that I have control over’.
Some participants felt that parenting a teen with a diagnosed emotional or behavioural disorder had enhanced their parenting skills or expressed a sense of empowerment and confidence in their parenting abilities and in this way were able to refute stigma. For example, Eithne (son, 10, ADHD) pointed out that her son’s well-being was her main concern and what anyone else thought of her parenting abilities was inconsequential: ‘What anyone else thinks of me, the way I’m doing things, I don’t care. […] I want what’s best for him, and I will fight tooth and nail for him. And if people don’t like that, then that’s their problem’.
Normalizing the Young Person’s Disorder
Parents’ normalization of their child’s diagnosis and/or behaviours was evident in these interviews. This may be indicative of attempts to manage other people’s perception of the young person or their own parenting efforts. Although they were not asked any questions about perceptions of ‘normality’, a recurring theme was seen in parents’ spontaneous descriptions of their child’s diagnosis as ‘quite common’ or ‘the norm’. Speaking about ADHD, Orla (son, 15, ADHD) pointed out that: ‘I think now it’s the norm. Nearly every second or third child, especially boys, have it’. One parent (Pearl; son, 15, depression) recalled explaining her son’s low mood to friends in the following way: He’s still Jacob, and he just has down time, you know and we’re trying to sort it out, trying to get him to manage it so he can live a normal life. I said, ‘Everybody has down time’. I said, ‘His just are a little bit worse at the minute than yours or mine. Everybody has bad days like’.
Many parents said that they did not treat their child differently just because he/she had an emotional or behavioural disorder. For example, Graham (son, 13, ADHD) said that: ‘I don’t treat Oliver as having ADHD, I treat him just as a normal son’. The majority of parents (e.g. Theresa, daughter, 14, ADHD) said that they were accepting of their child, despite the difficulties that they presented with: ‘Yes, she has ADHD. Yes, it’s incredibly frustrating. [But] she’s my daughter, I gave birth to her, she’s mine and I still love her and accept her for how she is’. However, in contrast to this, Clarissa (daughter, 13, ADHD) spoke of the emotional impact of having a daughter diagnosed with ADHD: ‘I just sat in the bath crying last night, wishing I had a normal daughter’.
Some parents did not want their child to be labelled as different. For example, Yasmin (parent of one son and two daughters with ADHD, aged 12–15 years) said that: ‘I don’t want them to be labelled, and I don’t want them to be tagged for the rest of their lives’. Similarly, Lindsey (14, depression, female) did not want her daughter to be: ‘...labelled as being any way out of, you know, out of the norm’. However, negativity in relation to ‘labelling’ was not unanimous for this sample. Some parents spoke of the benefits of having a diagnosis for their child, specifically referring to the importance of being able to put ‘a name on it’.
To Disclose or Not Disclose
Examination of parents’ accounts of their disclosure decisions provides an important insight on stigma because individuals tend to be secretive about attributes that they consider a source of shame, and conceal this information to avoid experiencing prejudice and discrimination. In this sample, a range of patterns of disclosure were evident: reluctance to disclose to anyone, limited disclosure and complete openness about the diagnosis. Parents gave a variety of reasons for being selective in deciding who to tell about their child’s diagnosis. Anticipation of negative reactions was one of main reasons against disclosure. As Finbar (son, 11, ADHD) put it: ‘I wouldn’t tell somebody that I thought would have a problem with it’. Rosie’s (daughter, 15, depression) concealment was also related to her anticipation of stigma: ‘I don’t want a stigma over her […] I just don’t want it always hanging over Leah’s head. If she makes a mistake, “Oh that’s cause she suffers with depression”, or things like that’.
Another reason for being cautious about disclosure was the perception that discussion of mental health problems is not the norm in Irish society: ‘I think mental health in this country has a bad stigma to it anyway. And I don’t think people really understand mental illness, even though there’s so much of it in the country – I think there’s very poor understanding. And it’s something that’s kinda, it’s not talked about, and it’s kept hush hush’. (Lindsey; daughter, 14, depression). Other parents decided against telling others because they did not want to worry them. Fathers, in particular, often did not see the necessity in telling people about what their child was going through. Greg (son, 16, ADHD) said that he did not discuss the matter with his friends because: ‘...you go to friends, you go out for a drink, you want to get away from your family really. So that’s probably the only reason, you know’.
Reluctance to disclose was not ubiquitous, with some parents stating that they did not care what other people thought or said that they had ‘nothing to hide’, that they ‘wouldn’t hide it’ or that they ‘don’t make a secret of it’. For example, Bree (son, 11, ADHD) said that she was open to telling others about their son’s diagnosis: I don’t care. […] the stigma around it doesn’t bother me’. Despite having described her concerns in relation to disclosure, Yasmin (son, daughter, daughter, 15, 15, 12, ADHD) also said that: ‘...at the end of the day, […] you don’t give a rat’s arse at times who knows and who doesn’t know, you just have to get on with it’.
A number of parents mentioned disclosure as a means to foster a support network, including reaching out to other parents whose children were facing similar issues. For example, Orla (son, 15, ADHD) said that: ‘I went to [support group], and I found it very good, just that other parents were going through the same, and that you weren’t going mad’. Some parents said that they had disclosed their child’s diagnosis to others in order to explain or justify his/her behaviour and described telling other parents about the diagnosis in scenarios where they were likely to witness the child’s behaviour first-hand. For example, Jimmy (son, 11, ADHD) said that: If the kids are acting the maggot [being foolish/annoying], and they’re wrecking the place […] at least you can say ‘Look, he has a condition, and that’s part of it, like, so I’m not a bad parent, and he’s not a bad child’.
Parents of children with depression also spoke about justifying their child’s behaviour. For example, Breda (son, 12, depression) described telling her son’s football coach about his low mood because: ‘He could have just walked off [the pitch]’. Her rationale for telling was that: You can’t expect people to be supportive of a child if their actions on the face of it are just like maybe being bold [naughty] or something like that, or just you know ‘God that child is strange!’ But if you’ve explained why they’re doing that...
Discussion
The aims of this study were to explore perceptions of stigma and the applicability of the stigma construct to parents of young people diagnosed with two common emotional and behavioural disorders, through qualitative accounts of the parenting experience. Respondents provided unique insights into their perceptions of stigma experienced in their role as a parent. Following thematic analysis, there were four themes showing how parents experience stigma: (1) Parenting an adolescent with a diagnosed emotional or behavioural disorder in an ill-informed and dismissive society; (2) the experience of parental self-blame; (3) normalizing the young person’s disorder and (4) to disclose or not disclose. Although parents described the many challenges in having a child/adolescent with a diagnosed emotional or behavioural disorder, distinct coping mechanisms and personal triumphs were also evident. Stigma, in the form of perceived prejudice, courtesy stigma, self-blame, anticipated stigma and selective disclosure, was apparent throughout these parents’ narratives. The study highlights the relevance of these constructs not only to the experience of parenting and childhood ADHD but also to those parents who have children with depression.
One of the goals of this study was to explore potential differences in views expressed by mothers and fathers, and by parents of young people with behavioural disorders compared to those with emotional disorders. Our analyses show that there are more similarities than differences in perceptions of stigma across these participant groups. This may mean that current conceptualizations of stigma (including constructs such as anticipated stigma and selective disclosure) are equally applicable to parents of children with emotional disorders as they are those with behavioural disorders. However, the potential for differences between groups should be further explored in samples involving larger numbers of fathers and parents in ‘non-traditional’ family structures. Research focussing solely on the experience of parents of children with emotional disorders may be particularly helpful to advancing this area of research.
Parents felt that other people were dismissive, did not understand what their child’s disorder entailed or had negative attitudes. In addition, parents felt that their child’s emotional or behavioural symptoms were viewed with disfavour by other adults. Similar findings have been observed in previous studies involving parents of children with ADHD (e.g. McIntyre & Hennessy, 2012; Moen et al., 2011). Parents in this study appear to be picking up on stigmatizing views held by the public, including, in some cases, members of their own social network, their families and people in their local communities. In the present study, the perception that other people are ill-informed and dismissive was one issue that transcended type of diagnosis. This consistency in how people reportedly respond to children and adolescents with very different (emotional vs. behavioural) diagnoses is noteworthy and is an area worthy of further investigation. These findings highlight the need for continued efforts to develop and implement mental health stigma reduction campaigns focussing on the needs of children, adolescents and their carers.
This study confirms that courtesy stigma and parent self-blame were experienced by parents of children/adolescents with both ADHD and depression. This was evident in parents’ accounts of being judged by others on the basis of their child’s behaviours (courtesy stigma) and their approach to parenting (parent blame). Parents’ views of themselves were explored to examine the possibility that they had internalized these negative views. A number of parents described blaming themselves for the difficulties that their child was facing, potentially experiencing self-stigma. Self-stigma arises where negative societal responses towards are internalized, often leading to diminished self-esteem or self-efficacy (Corrigan & Watson, 2002). The idea that parents believe they are blamed for their child’s disorder has been highlighted in previous research (McIntyre & Hennessy, 2012) and this can cause the parent to experience self-scrutiny, guilt and shame (Harden, 2005).
Although the concept of self-stigma is well established in the literature on adults with first-hand experiences of mental health issues, little is known about how it is experienced by parents such as those in the present study (Eaton et al., 2016). Our findings support Eaton et al.’s (2016) suggestion that the self-stigma experience for parents is different to that experienced by those who have emotional or behavioural disorders themselves because the concept must be broadened to include elements such as self-doubt, self-blame and social avoidance (in the form of selective disclosure or turning to families who are going through something similar). This study also supports the idea that parents may transition from viewing themselves as a ‘bad parent’ to considering themselves a ‘good enough’ parent (see Eaton et al., 2016). Parents in the current study found ways to resist stigma and spoke of putting their child first while ignoring the responses of others. This ability to resist and rise above stigma has been reported in the wider literature on the stigmatization of health conditions (Cuca & Rose, 2016) and by parents of children with emotional and behavioural problems specifically (Eaton et al., 2016). The findings support recent calls for interventions that tackle stigmatizing attitudes and blame directed towards these parents (Reardon et al., 2017). Clinicians should acknowledge the possibility that parents will experience self-blame and work on finding ways to help them to tackle any related feelings of self-deprecation.
Parents’ efforts to maintain a sense of normality in the face of their child’s emotional or behavioural disorder is consistent with previous findings on managing stigma (Frigerio & Montali, 2016; Koro-Ljungberg and Bussing, 2009). This has been described as a form of coping for parents who have a child with a diagnosed mental health problem (Harden, 2005). Perceiving the child/adolescent as ‘normal’ may serve a protective function for parents in terms of reducing the likelihood that they experience self-blame. Diminishing the extent to which their child is portrayed or perceived as ‘different’ may act as an important coping mechanism for parents who wish to avoid stigmatizing experiences. These findings suggest that promoting continuum-based conceptualizations of mental health problems (Corrigan et al., 2017) in public anti-stigma campaigns may be a useful approach. The current study also shows that opportunities to share and compare experiences with other parents in similar circumstances (e.g. through support groups) may be a constructive coping resource for parents. Parental support groups have been advocated as a place where parents can escape public scrutiny and create a discourse that helps to diminish feelings of self-blame and self-stigma (Frigerio & Montali, 2016; Perlick et al., 2011).
In line with previous research (Chavira et al., 2017) some parents viewed ‘labelling’ their child as something to be avoided because they felt that a label would mark their child as ‘different’. For others, however, use of a label was welcomed, by giving a ‘name’ and explanation to disruptive behaviours. This adds to the debate on the role of labelling and the applicability of Modified Labelling Theory (Link et al., 1989) to understanding stigma experienced by parents of children/adolescents (10–16 years) with diagnosed ADHD and depression. The present study suggests that stigma arises not only in response to awareness of the label but also upon observing behavioural manifestations of both of these disorders.
Parents varied in the extent to which they were willing to disclose their child’s diagnosis to others. Many parents told people on a need to know basis, in cases where they felt the disclosure was relevant, or where disclosure served a particular purpose. Some outlined reasons for being cautious in terms of discussing their child’s mental health issues, referring to mental health as a topic that is not openly discussed in Irish society. Such findings are in line with the literature on adult mental illness. Corrigan and Matthews (2003) refer to the use of ‘selective disclosure’ as an approach that is used when stigmatizing reactions are anticipated and it has been described as an adaptive approach to identity management (Ilic et al., 2014), with non-disclosure serving a self-protective function (Murphy, Hevey, O’Dea, Ní Rathaille, & Mulcahy, 2016). For parents in the present study, selective disclosure to close friends and family was generally seen as beneficial, in terms of facilitating feelings of acceptance and support. The experience of gaining support following disclosure is in line with previous qualitative findings on mothers’ decisions to disclose their child’s mental health disorder (Eaton et al., 2017).
Despite the appeal of selective disclosure, not all parents who took part relied on this stigma management technique. Some parents described their willingness to let everyone know about what their child was going through. This is similar to the idea of ‘indiscriminate disclosure’, where individuals disregard the potential negative consequences of telling others about the mental health problem and do not restrict the information that they share or the people to whom they disclose (Corrigan & Matthews, 2003).
Further research is needed to explore the implications of disclosure for parents of a young person with a mental health diagnosis. There has been a call for the development of grassroots interventions to promote disclosure, using a combination of contact and education as approaches to reduce stigma (Corrigan, 2017; Corrigan and Fong, 2014), empower and support parents (Mofokeng & van der Wath, 2017). It is likely that different approaches to disclosure are used by the same individuals over time (McKeague et al., 2015), although this is an area that warrants future longitudinal research. Research on other stigmatized health conditions suggests that stigma management strategies will vary depending on the context (Olsson, Lyon, Hornell, Ivarsson & Sydner, 2009), as will the implications of disclosure (Corrigan, 2017). The findings of the present study indicate that some parents believe that their willingness to disclose their child’s diagnosis to others has contributed to enhanced social support. However, negative experiences may arise when disclosure is met with a lack of understanding. This may contribute to a reluctance to discuss mental health for some, and the decision to disclose is one fraught with uncertainty. Research exploring effective disclosure strategies and ways to deal with the reactions of others, perhaps involving focus groups, will move this area of research forward. The aim of such research should be to inform the development of programmes to help parents and their children to consider the costs and benefits of disclosure. The Honest, Open, Proud programme (Rüsch et al., 2014) was designed to help people to consider the implications of disclosure. Adaptation of this approach for parents of children and adolescents with diagnosed emotional and behavioural disorders would be a useful next step.
In several respects, the sample included in this study is more diverse than those described in previous literature on this topic. Similar to recent research (Eaton et al., 2016), this study focuses on more than one type of diagnosed mental health disorder, whereas most previous studies included parents of ADHD only. The sample in the present study included fathers as well as mothers. Difficulty in recruiting fathers despite extensive effort to do so has been noted in similar research projects (Eaton et al., 2016). Future research focussing on how fathers perceive and deal with stigma is encouraged. Another important strength of this study was that parents were given the opportunity to focus on both positive as well as negative aspects of their experiences, for example, some parents described how parenting a child/adolescent with an emotional or behavioural disorder enhanced their parenting skills. While it was important that the interview guide allowed parents to voice any stigmatizing experiences, it was equally important that their responses were not biased towards focussing on negative experiences and omitting positive ones.
The findings of this study should be interpreted in light of some limitations. In terms of the study sample, there was a gender bias, whereby more parents of males than females took part. In addition, the sample includes more parents of children/adolescents with ADHD than depression and more mothers than fathers. However, this pattern reflects the epidemiology of mental health diagnoses in Ireland, where ADHD is the most common reason for attending CAMHS (Health Service Executive, 2014) and it is well established that more boys than girls present with this disorder. Recruitment of fathers was higher than what has been reported in other recent studies in this area, but efforts to encourage their participation should continue in future research. Perceptions of stigma may be more or less pertinent for parents of youth with diagnoses that were not examined in this study (e.g. psychosis). It is also possible that parents of youth who have comorbid emotional and behavioural disorders have different perceptions of stigma experiences than participants in this sample, who did not have comorbid difficulties of that nature. Future research in this area should collect additional background information on children’s use of different types of medication (e.g. antidepressants) and whether they are receiving psychotherapy at the time of the study. Treatment may impact stigma-related experiences, given its role in reducing behavioural manifestations of these disorders.
Conclusion
This study provides valuable insights into how parents of children and adolescents with diagnosed emotional and behavioural disorders perceive and contend with potential stigma in their everyday lives. One of the main areas of stigma reported by these parents is the dismissive attitudes and inaccurate perceptions that other adults hold in relation to the young person’s emotional or behavioural symptoms. Some parents also reported challenges associated with their own experiences of self-blame. Efforts to deal with stigma were apparent in parents’ attempts to frame their child’s experiences as normal and their use of selective disclosure. These findings highlight the additional challenges faced by parents of children with emotional or behavioural disorders, challenges that go beyond their child’s condition and influence how they relate to their extended family and the wider community. In particular, public health campaigns for stigma reduction should take a family perspective and consider how stigma affects parents of children and adolescents attending CAMHS.
Supplemental Material
sj-pdf-1-jfi-10.1177_0192513X211030924 – Supplemental Material for Parenting an Adolescent Who is Using a Mental Health Service: A Qualitative Study on Perceptions and Management of Stigma
Supplemental Material, sj-pdf-1-jfi-10.1177_0192513X211030924 for Parenting an Adolescent Who is Using a Mental Health Service: A Qualitative Study on Perceptions and Management of Stigma by Lynn McKeague, Eilis Hennessy, Claire O’Driscoll-Lawrie and Caroline Heary in Journal of Family Issues
Footnotes
Acknowledgements
The authors would like to thank the parents who contributed to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by the Health Research Board, Ireland. This publication is independent research funded by the Health Research Board in Ireland under Grant no: HRA/2009/269. Any opinions, findings, conclusions or recommendations expressed are those of the author(s) and not necessarily those of the HRB.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.