
Abstract
Previous research has shown that women providing family care tend to decrease paid work. We take the opposite perspective and examine how current and previous family care tasks influence women’s likelihood to (re-)enter employment or to increase working hours. Family care is defined as caring for an ill, disabled or frail elderly partner, parent, or other family member. Using German Socio-Economic Panel data, we apply Cox shared frailty regression modeling to analyze transitions (1) into paid work and (2) from part-time to full-time work among women aged 25–59. The results indicate that in the German policy context, part-time working women providing extensive family care have a lower propensity to increase working hours. When family care ends, the likelihood that part-time working women change to full-time does not increase. Homemaking women’s likelihood of entering the workforce is not influenced by either current or previous family care tasks.
Introduction
Women’s employment careers in contemporary Western societies continue to be characterized by prolonged withdrawals from the workforce or a reduction in working hours due to their frequently assumed role as primary caregiver within the family (Carmichael & Ercolani, 2016; Killewald & Zhou, 2019; McMunn et al., 2015; Simonson, Romeu Gordo, & Titova, 2011). Besides childcare, as women age, they increasingly engage in care of a partner, parents, parents-in-law, or other family members in regular need of care due to poor health, disability, or age-related frailty (‘family care’ in the following) (Bianchi, Folbre, & Wolf, 2012; Geyer & Schulz, 2014). Care-related interruptions of or reductions in labor market activity can have adverse long-term consequences for individuals and societies as they can lead to cumulative disadvantage over the life course implying economic dependency, reduced old-age pension entitlements, and thus increased risk of old-age poverty (Fasang, Aisenbrey, & Schömann, 2013; Möhring, 2015, 2018). In fact, women as family caregivers are central in maintaining the health, well-being, and quality of life of individuals in need of care (Blome, Keck, & Alber, 2009; Leitner, 2013).
Most research on women’s careers and consequences of labor market withdrawal has focused on young mothers, that is, women in the years shortly after childbearing. Unpaid care responsibilities related to child-rearing clearly represent a major constraint on women’s labor market participation (e.g., Anxo, Fagan, Cebrian, & Moreno, 2006; Dotti Sani & Scherer, 2018; Drobnič, 2000; Gash, 2008). However, after the period in which women typically care for their young children, new demands arise if parents(-in-law) or older spouses become in need of care due to frailty or deteriorating health conditions. Compared to childcare, family care needs are generally less predictable in terms of timing, duration, intensity, and type of care. Moreover, demands on family caregivers that accompany what are often chronic health conditions associated with aging usually increase rather than decrease over time (Kröger & Yeandle, 2014; Moen, Robison, & Fields, 1994; Roundtree & Lynch, 2006; Stewart, 2013; Stewart, Stutz, & Lile, 2018).
Previous research on family care has focused on selection into care provision, either with respect to the sociodemographic characteristics of family caregivers and their position in the family (e.g., Chesley & Poppie, 2009; Dwyer & Seccombe, 1991; Henz, 2006; Leopold, Raab, & Engelhardt, 2014); the psychological consequences of family caregiving (e.g., Choi & Marks, 2006; Cullen, Hammer, Neal, & Sinclair, 2009; Gordon, Pruchno, Wilson-Genderson, Murphy, & Rose, 2011); or whether providing family care is associated with working hour reductions or labor market withdrawals (e.g., Carr et al., 2016; Henz, 2006; Kelle, 2018; van Houtven, Coe, & Skira, 2013). However, our understanding of family caregivers’ ability to increase working hours or to return to the labor market during or after a family care period is very limited. Hence, this study examines the impact of family care on chances to (re-)enter employment or to increase working hours. We focus on women in Germany and use data provided by the German Socio-Economic Panel (SOEP). Event history modeling is applied to study the impact of family care and the termination of family care, respectively, on two transitions: (a) entering employment from homemaking and (b) changing from part-time to full-time work for a sample of 7,911 women.
Background
The Concept of Family Care
Besides childcare and housework, family care is an important aspect of unpaid work (Bianchi et al., 2012; ILO, 2018; Kröger & Yeandle, 2014). Throughout this article, the term ‘family care’ refers to the activities of individuals who care for a family member in regular need of care due to poor health, disability, or age-related frailty (Kröger & Yeandle, 2014; Moen & DePasquale, 2017). Typical childcare is not subsumed under the concept of family care used in this article, while exceptional childcare is (Daly, 2001; Kröger & Yeandle, 2014; Stewart, 2013). In contrast to typical childcare, exceptional childcare refers to caring tasks that are experienced by parents of children with nontypical development or serious illness (Roundtree & Lynch, 2006; Stewart, 2013).
In contrast to typical childcare, family care dynamics are less predictable in terms of timing, duration, kind, and intensity of care. The need for family caregiving can occur at any point throughout the life course of an individual (Bianchi et al., 2012; Moen et al., 1994): many family care needs arise suddenly when a child, partner, or parent either suffers diverse impairments following an accident or is diagnosed with a life-threatening disease like cancer. Other family members need support and care from time to time, for example, elderly, frail parents who more frequently experience illness and injury. Still other family care needs persist over the long term, for instance when parents have to care for their disabled child from birth onwards or when individuals have to care for family members with chronic and deteriorating health conditions like Alzheimer’s, or requiring constant care as a result of a stroke (Moen et al., 1994; Roundtree & Lynch, 2006; Stewart, 2013; Stewart et al., 2018; Yeandle, Bennett, Buckner, Fry, & Price, 2017).
Depending on the care needs, family care provision can span a wide spectrum of tasks, which in turn are very heterogeneous with respect to time sensitivity and time commitment (Hassink & van den Berg, 2011; Hielscher, Kirchen-Peters, Nock, & Ischebeck, 2017; Keck, 2012; Stewart et al., 2018; Yeandle, Bennett, et al., 2017). Family care may encompass help with instrumental activities of daily living (iADLs), that is, cooking or cleaning (Lawton & Brody, 1969); or family care may contain tasks that refer to support with activities of daily living (ADLs), such as getting in and out of bed, toileting, bathing, dressing, or feeding (Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963). Another aspect of family care may be supervising or looking after the person in need of care if individuals in need of care cannot be left alone for long periods without involving safety risks. This could be the case if a person suffering from dementia is at risk of wandering off; if a person is in permanent danger of falling; or if a person displays self-damaging, auto-aggressive behavior (e.g., Bianchi et al., 2012). Finally, family caregivers not only ‘care for’ the person in need of care, but often they also ‘care about’ the cared-for person (e.g., Folbre & Wright, 2012; Traustadottir, 1991; Tronto, 1993). Accordingly, family caregivers provide emotional and psychological support by being approachable and being present as well as by interacting and talking to the cared-for person.
Depending on the family care tasks provided, the necessity to be available and approachable during the day varies substantially. Some activities are time-sensitive, that is, they need to be performed at fixed points in time during the day (and probably on a daily basis). Other tasks are shiftable and can be provided flexibly at any time of the day. For example, household chores or organizational work (iADLs) are shiftable tasks, whereas personal care activities (ADLs), like washing, bathing or toileting, are non-shiftable tasks (Hassink & van den Berg, 2011). In terms of time commitment, the different family care tasks are heterogeneous, too. Supervisory care tasks are the most time-consuming, whereas basic care tasks such as personal care and feeding require less time commitment. As individuals needing care are often no longer able to run a household, providing help with household chores is the second most time-consuming task. Moreover, the worse the health status of the person in need of care, the more time-consuming the family care tasks. Thus, time committed to every care task increases with the cared-for person’s increasing care needs (Hielscher et al., 2017).
The Gendered Nature of Family Caregiving
There is ample evidence that the provision of family care is unequally divided between women and men. Throughout the working life, women perform most of family care (Arber & Ginn, 1990; Carr et al., 2016; Ehrlich, 2019; Geyer & Schulz, 2014; ILO, 2018). For example, children with a serious health condition, health risk, or disability almost always live within the family household, and almost always their mother is the primary caregiver—regardless of whether children’s care needs exist from birth onwards or become apparent later in a family’s life course (Büker, 2008; Hunt, 2012; Kofahl & Lüdecke, 2014; Rothgang, Müller, Runte, & Unger, 2017; Traustadottir, 1991). If an adult develops care needs, the first source of help and support is, if available, a healthy (marital) partner living within the same household. Even though serious health conditions or health risks may occur regardless of gender, most often the typical situation is that a wife takes over care for her elderly husband, because women are typically younger in the couple, have a higher life expectancy, and become disabled later in the life course (Bianchi et al., 2012; Norton, 2000; van Houtven, 2015). When a parent develops care needs and no healthy partner is available to meet these needs, adult children become an important source of care. In general, children want to fulfill this role. They feel a sense of filial responsibility and obligation, driven by norms of reciprocity (e.g., Finch & Mason, 1990, 1993; Klaus, 2009; Silverstein, Conroy, & Gans, 2008), to take care of their parents. However, it is a well-established finding in the literature that it is usually the daughters who assumes the parent caregiver role (Leopold et al., 2014; Scheekloth, Geiss, & Pupeter, 2016). Research by Matthews (2002) suggests that daughters are more likely to provide parent care than sons because they feel a stronger obligation to meet parents’ care needs and are more likely to experience feelings of guilt if they do not adequately fulfill the caregiver role. Furthermore, the provision of care by (female) family members rather than professional care services is a consequence of the specific institutional setting in Germany as we explain below.
Family Care in Germany
Germany represents a ‘conservative’ welfare state, characterized by the dominance of the male breadwinner model and a highly coordinated labor market (Buchholz et al., 2009; Esping-Andersen, 1990; Möhring, 2016). In 1995, the public long-term care insurance was introduced to cover the costs of those in need of long-term care. It is funded through social security contributions paid typically in equal shares by employers and employees, and benefits are typically provided as individual cash benefits, benefits-in-kind, or care home benefits for those who are in need of care according to an official classification scheme (Boeckh, Huster, & Benz, 2011; Rothgang, 2010). Compared with other European countries, Germany is on a mid-level with respect to the generosity of the public long-term care system (Schulz, 2012). Cash benefits for home-based care are lower in amount than benefits-in-kind or benefits-for-care provision in care homes. However, benefits-in-kind or benefits-for-care homes are only partially comprehensive and care-dependent individuals or their family members have to make high top-up payments (Hielscher et al., 2017; Rothgang et al., 2017). As a result, the most cost-effective arrangement for care-dependent individuals and their families is to opt for cash benefits and to be cared for at home by family members. Therefore, Germany is described as an ‘explicit familialistic’ care regime which actively shifts the care responsibility to the family by giving home-based care by family members priority over professional care services or full-time institutional care settings (Leitner, 2013; Rothgang, 2010). This also translates into numbers: in 2015, 2.9 million persons in Germany were eligible to receive benefits from the long-term care insurance, and therefore had substantial care needs. Of those, 2.1 million (73%) were cared for in their own home by family members or friends (Federal Statistical Office, 2017). However, the number of persons in need of regular help, support, or care is considerably higher because eligibility for benefits under the long-term care insurance is restricted to those with the greatest care needs. According to Geyer and Schulz (2014), the number of persons who are severely impaired in performing everyday tasks and do not receive any support from long-term care insurance is estimated to be 5.4 million (6.7% of the German population). Thus, a total of approximately 7.5 million persons (9.3% of the German population) are in need of regular help, support, or care by family members or friends.
Welfare state policies that actively support family members to provide care for the ill, disabled, or elderly are likely to have a greater impact on women “because care work traditionally falls within their area of responsibility” (Schmid, Brandt, & Haberkern, 2012, p. 41). Moreover, given the prevailing gender differences in labor market participation and earnings as well as persistent welfare state policies promoting a male breadwinner family (e.g., Aisenbrey & Fasang, 2017), the German care regime clearly provides incentives for women to take over family care tasks. Therefore, the German care regime is classified as a “gender-specific discriminatory variant of familialism” that reproduces the gendered division of labor (Leitner, 2013).
Figure 1 depicts the share of women and men providing care for the ill, disabled, or elderly according to age as well as the employment rate of women according to age and family caregiver status.
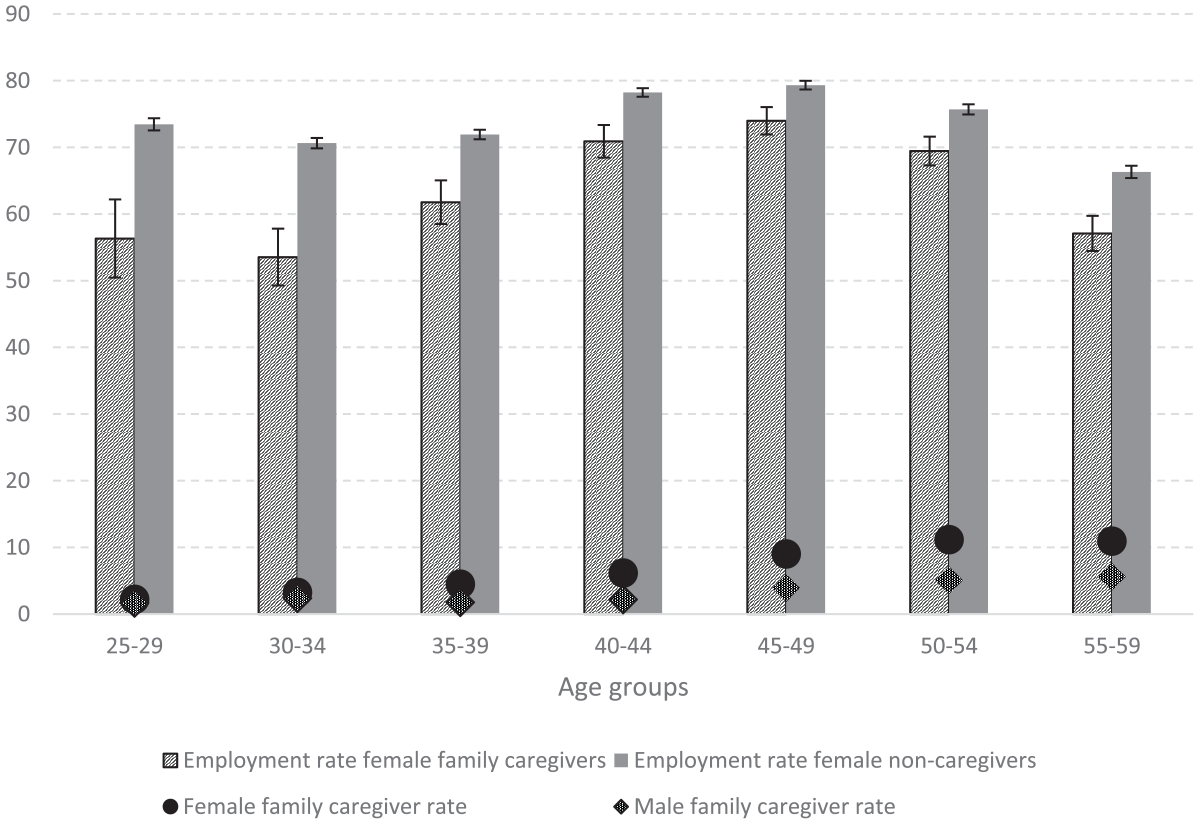
Female Employment Rate According to Age and Family Caregiver Status and the Share of Female and Male Family Caregivers According to Age, in %, 2001–2014.
Figure 1 shows that the prevalence of family caregiving increases with age and differs between genders. The share of family caregivers in the population is low and equally distributed among both genders when women and men are in their 20s and early 30s. Starting from the mid-30s until retirement, women are involved in family care to greater extent than men. Family care is particularly relevant in women’s late career phase. Eleven% of women aged 50–54 provide family care compared to only 6% of men of this age group.
Figure 1 also shows that working-age women often reconcile family care with paid work, but the employment rate of female family caregivers is significantly lower compared to women without family care responsibilities. However, even though the share of family caregivers is substantial and many are employed, the ‘explicit familialistic’ German care regime (Leitner, 2013) provides only limited access to professional and affordable care services which could facilitate the reconciliation of family care and employment. Thus, working family caregivers are confronted with reconciling family care and paid work with little state support, resulting in difficulties to combine both tasks. In this policy context, part-time or full-time exits from the labor market are very likely when family care tasks become too time-consuming.
Family Care and Women’s (Re-)Employment
Due to their frequently assumed role as primary caregivers, career choices and decisions of women are linked to intra- and intergenerational family care responsibilities (Elder & O’Rand, 1995; Heinz & Krüger, 2001; Moen, 2003). Changes in these responsibilities may constitute obstacles but also incentives to (re-)starting or increasing labor market activity. Some studies found that the provision of family care corresponds with slight reductions in working hours (Leigh, 2010; Meng, 2013; Pavalko & Artis, 1997; van Houtven et al., 2013), others showed that providing family care can increase the likelihood to stop working—for both full-time and part-time working women (Colombo, Llena-Nozal, Mercier, & Tjadens, 2011; Henz, 2006; Schneider, Drobnič, & Blossfeld, 2001). Previous research underlines the importance of family care intensity: women’s likelihood of reducing employment hours increases with more hours of family care (Berecki-Gisolf, Lucke, Hockey, & Dobson, 2008; Heitmueller, 2007; Keck, 2012; Kelle, 2018; van Houtven et al., 2013). However, Kröger and Yeandle (2014) argue that the family care relationship, that is, the relationship between family caregiver and care recipient, has important implications for the reconciliation of family care and paid work. They justify this, among other things, with the assumption that “different configurations of love, concern, obligation, intimacy, responsibility and reciprocity” (ebd., p. 13) might play a role that make caring for an (adult) child, partner, or parent different. Carr et al. (2016) adopted this line of argumentation in their analysis of Britons aged 50–75 years and concluded that only full-time working women who provided family care for a partner/spouse were more likely to exit the labor market, while caring for parents/grandparents or others had no impact on their employment. Using the same sample, they also found that only caring for someone within their own household instead of caring for someone in another household had negative consequences on paid work. This is in line with previous studies differentiating between co- and extra-residential family care when analyzing the family care–employment relationship (Heitmueller, 2007; Michaud, Heitmueller, & Nazarov, 2010). However, Ehrlich (2018) showed that the influence of the family care location does not persist when family care intensity is controlled for: women providing care for a household member and women providing care for a non-household member are likely to experience equally harmful labor market consequences when controlling for the amount of time devoted to family care. The importance of family care intensity has also been confirmed for the United States in a study by van Houtven et al. (2013). The authors found that labor market outcomes do not vary by the type of care provided. Family caregivers providing non-shiftable personal care, that is, help and support with ADLs, and those providing shiftable chore care, that is, help and support with iADLs, reduce their working hours to the same extent. What counts is rather the time devoted to family care. Family caregivers providing a high amount of care hours are the ones with the highest working time reductions. Taken together, all these studies point in the same direction: the reconciliation of family care and employment is difficult, and its success depends, above all, on the time devoted to family care.
But what happens after family care has ended? According to the time availability approach, time spent on family care limits the time available for paid work. The end or an ease of family care—for example when the cared-for person recovers, moves to an institutional care home, or passes away—may provide an opportunity to (re-)enter the labor market or to increase working hours. However, previous research on the employment behavior of women providing family care rather points in the opposite direction. In a cross-national comparative study of 12 European countries, Spieß and Schneider (2003) showed that women in the 1990s do not increase working hours after family care hours decrease or family care episodes end. For Great Britain, Henz (2004) found that re-employment chances diminish with the duration of family care episodes. For the United States, Pavalko and Artis (1997) as well as Wakabayashi and Donato (2005) employed data for the 1980s and 1990s and found that terminating family caregiving has no impact on women’s hours worked.
From a theoretical perspective, the economic theory of the family with intra-household specialization (Becker, 1993; Himmelweit, Santos, Sevilla, & Sofer, 2013) is congruent with these findings. As partners are assumed to have a joint utility function with a stable specialization in either paid work or unpaid care work, the person with the higher earnings potential specializes in paid work and provides the household’s income, whereas the person with the lower earnings potential specializes in care and household obligations and is only—if at all—marginally employed (Becker, 1993). Since women’s wages are, on average, lower than men’s (Minkus & Busch-Heizmann, 2018), it is usually the women who invest less in their occupational career and specialize in household production and unpaid caregiving tasks (Aisenbrey & Fasang, 2017). However, it might not only be specialization why women ‘opt’ to work reduced hours or to stay out of work after family care has terminated, but also other factors related to labor market and health consequences of caregiving. Thus, from the labor demand point of view, another line of argumentation is possible. Human capital (Mincer & Ofek, 1982) and signaling theory arguments (Albrecht, Edin, Sundström, & Vroman, 1999) assume that homemaking and part-time working women in general face institutional barriers to (re-)entering employment or expanding their working hours from part-time to full-time. Full-time or part-time absences from the labor market lead to a loss of work potential because new human capital is not accumulated or existing human capital is depreciated (Mincer & Ofek, 1982). As a consequence, employers rate homemaking and part-time working individuals’ labor potential worse than that of continuously (full-time) employed workers. Moreover, full-time or part-time labor market exits signal to the (potential) employer a lower future career commitment (Albrecht et al., 1999). As a consequence, an employer is not willing to (further) invest in the human capital of homemakers or part-time workers. Moreover, former family caregivers might face specific barriers related to their previous caregiver role similar to those of mothers of small children (Budig & England, 2001; Correll, Benard, & Paik, 2007; Gangl & Ziefle, 2009). Employers might avoid hiring and investing in women who were previously family caregivers assuming that they could take up family care responsibilities again and be (partially) absent from the workplace.
Furthermore, women’s health status after caregiving could be a barrier for re-employment after family care has stopped. Several studies show that providing family care has negative consequences for women’s physical and mental health (Coe & van Houtven, 2009; Hiel et al., 2015; Kaschowitz & Brandt, 2017; Schmitz & Westphal, 2015). Consequently, due to poor health, women may not be able to increase working hours or to (re-)enter the labor market after family care has stopped. In this regard, possible health consequences also depend on who was cared for and how the family care episode ended. Psychological strain arising from the loss of a partner or close relative may impair women’s (re-)employment chances more strongly than if, for example, the care-dependent person recovers.
Thus, in contrast to the time availability approach which postulates that individuals may increase labor market activity when family care terminates, the economic theory of the family, labor demand side approaches, and research on the family care–health nexus rather support the assumption that former family caregivers may not adapt to changing time availability.
Household and Individual-Level Characteristics
Apart from current or completed family care demands, other factors may influence women’s labor supply, such as child-rearing activities, the household’s socioeconomic situation, or partner’s characteristics. Previous studies have shown that homemaking women with school-aged children are more likely to enter part-time or full-time employment than those with preschool children (Drobnič, 2000; Drobnič, Blossfeld, & Rohwer, 1999), whereas the transition from part-time to full-time work is not dependent on the age of children, indicating that part-time work is a rather robust work–family reconciliation strategy (Kitterød, Rønsen, & Seierstad, 2013; O’Reilly & Bothfeld, 2002).
The household’s financial situation is also expected to shape women’s employment transitions. Even though the economic theory of the family argues that a specialized household maximizes the joint household utility function (Becker, 1993), the feasibility of upholding a specialized household depends on its overall financial resources. Accordingly, O’Reilly and Bothfeld (2002) found that West German women from high income households were less likely to move from part-time to full-time work than those from low-income households. Specialization can become particularly problematic when the main earner is no longer capable of guaranteeing the economic security of the household (Oppenheimer, 1997). In such a case, the coupled career perspective, which takes life-course dynamics into account (Blossfeld & Drobnič, 2001; Moen, 2003) as well as the ‘added worker effect’ (Lundberg, 1985; Smith, 2010) suggest that a decrease in the household’s financial resources, which may arise from a reduction in earnings, a partnership dissolution or the partner becoming unemployed, leads women to enter the labor market or to increase their work hours.
Human capital resources are expected to play an important role in women’s (re-)employment chances (Mincer & Ofek, 1982). Educational qualifications and job experience may be beneficial not only in terms of skill enhancement, but also due to contacts to potential employers and as an indicator for productivity. Within the group of homemaking or part-time working women, inequalities will emerge from differences in educational investments and labor market experience prior to interrupting employment or reducing working hours. Higher education and previous labor market experience may increase women’s chances to find employment and put them in a better bargaining position to obtain a full-time job (Drobnič et al., 1999; Gash, 2008; Kitterød et al., 2013; O’Reilly & Bothfeld, 2002). In addition to human capital resources, a stronger career orientation can lead to higher propensity for employment and longer working hours (Gangl & Ziefle, 2015; Stam, Verbakel, & de Graaf, 2014; Vlasblom & Schippers, 2006). Finally, women’s labor market behavior is likely to be influenced by their age. Older workers in the German labor market face far less job opportunities and show lower job mobility compared to younger workers based on age-related discrimination by employers (Heywood & Jirjahn, 2016). Also, as retirement age approaches, many may feel less attached to the labor market and may be reluctant to (re-)start or increase labor market activity (Hess, 2018; Hess, Bauknecht, & Pink, 2018).
Hypotheses
Based on theoretical considerations and the results of previous studies, we derive the following hypotheses on the relationship between family care and employment transitions: we assume that family caregiving lowers women’s propensity to enter employment or to change from part-time to full-time employment (Hypothesis 1a). This effect will be stronger for women who provide more hours of family care (Hypothesis 1b).
Concerning women’s employment behavior after family care has terminated, previous research did not provide a conclusive evidence. Research for typical childcare has shown that women have been increasing their labor market engagement when care intensities ease (Dotti Sani & Scherer, 2018; Drobnič, 2000; Drobnič et al., 1999). Along the same lines, we assume that when a family care episode ends, the likelihood to take up employment or to change from part-time to full-time employment increases (Hypothesis 2a). However, based on the household specialization argument, women’s commitment to family care may reflect a long-term decision to focus on the family sphere instead of employment (Becker, 1993). Thus, women with low engagement in paid work may select into family care rather than pursue a career. Besides, employers might be reluctant to hire or increase working hours of previous family caregivers due to assumed human capital loss or lower (future) productivity. Also the health status of former family caregivers can be an obstacle to employment or increasing working hours. Therefore, we formulate the alternative hypothesis that the end of a family care period has no impact on women’s likelihood to take up employment or to change from part-time to full-time employment (Hypothesis 2b). Previous research on family care seems to support this argument (Pavalko & Artis, 1997; Spieß & Schneider, 2003; Wakabayashi & Donato, 2005).
Apart from family care, women’s employment behavior is likely to be influenced by several additional factors related to the household situation as well as women’s individual characteristics. Therefore, we control for the presence and age of children, the household’s socioeconomic situation and the partner’s employment situation as well as for women’s level of education, labor market experience, career orientation, and age.
Data and Method
Data and Operationalization
For the empirical analysis, 14 annual waves of the German Socio-Economic Panel (SOEP) were employed. The SOEP is a representative household panel study that started in 1984 in West Germany and was extended in 1990 to also include former East Germany (Goebel et al., 2018). As a panel study, the SOEP follows the same individuals over time, hence allowing the study of transition processes within individuals’ life courses. The SOEP provides longitudinal data on the respondents’ and their partners’ labor market and caregiving activities, as well as the household’s socioeconomic situation. Altogether 30,000 individuals residing in nearly 15,000 households participated at least once in the SOEP. For our analyses, data come from 7,911 female respondents that had at least one homemaker or one part-time employment episode.
The observation window for our analysis starts in January 2001 and ends in December 2013 as information on family care is only available from 2001 onward. The sample is restricted to women in prime working age of 25–59 years. Since the SOEP interviewees report their employment status on a monthly basis, precise information on the start and end month of each employment spell is available. The analysis focuses on employment episodes consisting of the homemaker status, defined as being a homemaker and not simultaneously employed, unemployed, retired, or on parental leave; part-time employment; and full-time employment. The employment measures are based on respondents’ self-assessment. Since SOEP only started differentiating between marginal employment (“Mini-Jobs”) and regular part-time employment in 2005, marginal employment and regular part-time employment are summarized in one category even though both differ with respect to social security contributions and entitlements. The dependent variables are transition rates between the following states: (a) from homemaker status to either part-time or full-time employment and (b) from part-time to full-time employment. The final sample consists of 4,296 homemaker episodes of which 1,969 end with labor market entry, and 10,173 part-time employment episodes of which 2,213 terminate with moves into full-time employment.
The main independent variable is providing family care. The information on family care is based on the SOEP time use module and captures regular family care involvement between Monday and Friday. The question is: What is a typical day for you? How many hours do you spend on the following activities on a typical week day—care and support for persons in need of care? Typical childcare is not included in the family care variable since both activities are captured separately in the same SOEP time use module with typical childcare put first. It is thus unlikely that respondents mix up typical childcare and family care responsibilities. Consistent with previous research (Carmichael & Charles, 2003; Carr et al., 2016; Kelle, 2018; King & Pickard, 2013), we distinguish different intensities of family caregiving in three categories: high-intense family caregiving of more than ten hours per working week; up to ten hours caregiving; and ‘no family care’ as reference category. Furthermore, a time-varying covariate denoting the end of family care is created; this binary variable has a value one if a person previously provided family care during the employment episode, but stopped to do so.
Typical child-rearing activities are assessed by including the information on the age of the youngest child in the household, distinguishing between school-aged children (7–15 years) and older or no children (reference category: youngest child is preschooler). Three indicators examine the influence of the household’s financial situation on women’s labor-market activity: First, last year’s household income, distinguishing between low-income (lowest quartile), high-income (highest quartile), and middle-income households. Second, a binary variable indicates a decrease in household income of 10% or more compared to the previous year. For missing income information, the imputed values provided by the SOEP are applied (Frick & Grabka, 2014). Third, partner’s employment status in the previous year: partner was ‘employed,’ ‘retired,’ ‘non-/unemployed,’ and ‘no partner in the household’ as reference category. Variables on educational level and prior work experience measure women’s human capital endowments. We also include a subjective measure of general career orientation on which all respondents provide information regardless of their current employment status; this binary variable has a value of 1 if a woman reported that to have success in a job is important or very important to her. Respondents’ ‘age’ is measured in years.
Further control variables are: respondent’s subjectively rated health in the previous year, migration background, and homeownership. We also take into account three macrostructural indicators that may affect women’s (re-)employment chances: living in eastern/western part of Germany, annual unemployment rate, and a period effect to indicate the paradigm shift in childcare policy in 2007. The new parental leave scheme introduced nation-wide in 2007 provides strong incentives for mothers to return to the labor market more quickly after the birth of a child (Ziefle & Gangl, 2014). As our samples consist of women aged 25 to 59 years, that is, including women who are in their childbearing years, it is essential that we control for this significant policy change, even if the focus of our study is on family care rather than typical childcare. Finally, as employment episodes can be left-censored, we control for the employment episode length before entering the sample. For further operationalization details as well as information on time-varying covariates, see Table A1 in the Appendix.
Method
Employment transitions are analyzed by means of event history analysis. Event history modeling estimates transition rates from the initial status (homemaking or part-time employed) to the destination state (employment or full-time employment, respectively). For analyzing transition rates, we employ Cox shared frailty regression modeling for two main reasons. First, Cox semiparametric modeling leaves the baseline hazard rate unspecified (Cox, 1972), which is suitable for our purposes. We are interested in estimating how the hazard changes with covariates, and not in the baseline rate itself. Second, by using Cox shared frailty regression modeling we take into account that family care and employment behavior might be driven by unobserved heterogeneity. One respondent can generate several employment episodes which are likely not independent of each other on some unobserved characteristics. This method controls for unobserved factors, such as personality or preferences that are unique to each individual (Box-Steffensmeier & Jones, 2007, pp. 141–154; Hougaard, 2000, pp. 215–262). Further, we use episode splitting to incorporate time-varying covariates in the analysis (Blossfeld, Golsch, & Rohwer, 2009). Cox shared frailty regressions are run in R using the coxph function.
Results
Descriptive Results
Table 1 presents the description of the sample at the beginning of the episodes or when the episodes enter the observation window, respectively. Women in 8% of the homemaker episodes (n = 331) and 6% in the part-time episodes (n = 661) provide family care. The share of women involved in time-consuming family care of more than 10 hours per week is significantly greater in the homemaker than in the part-timer sample.
Sample Description at the Beginning of the Episode or When an Episode Enters the Observation Window. Means and Standard Deviations.
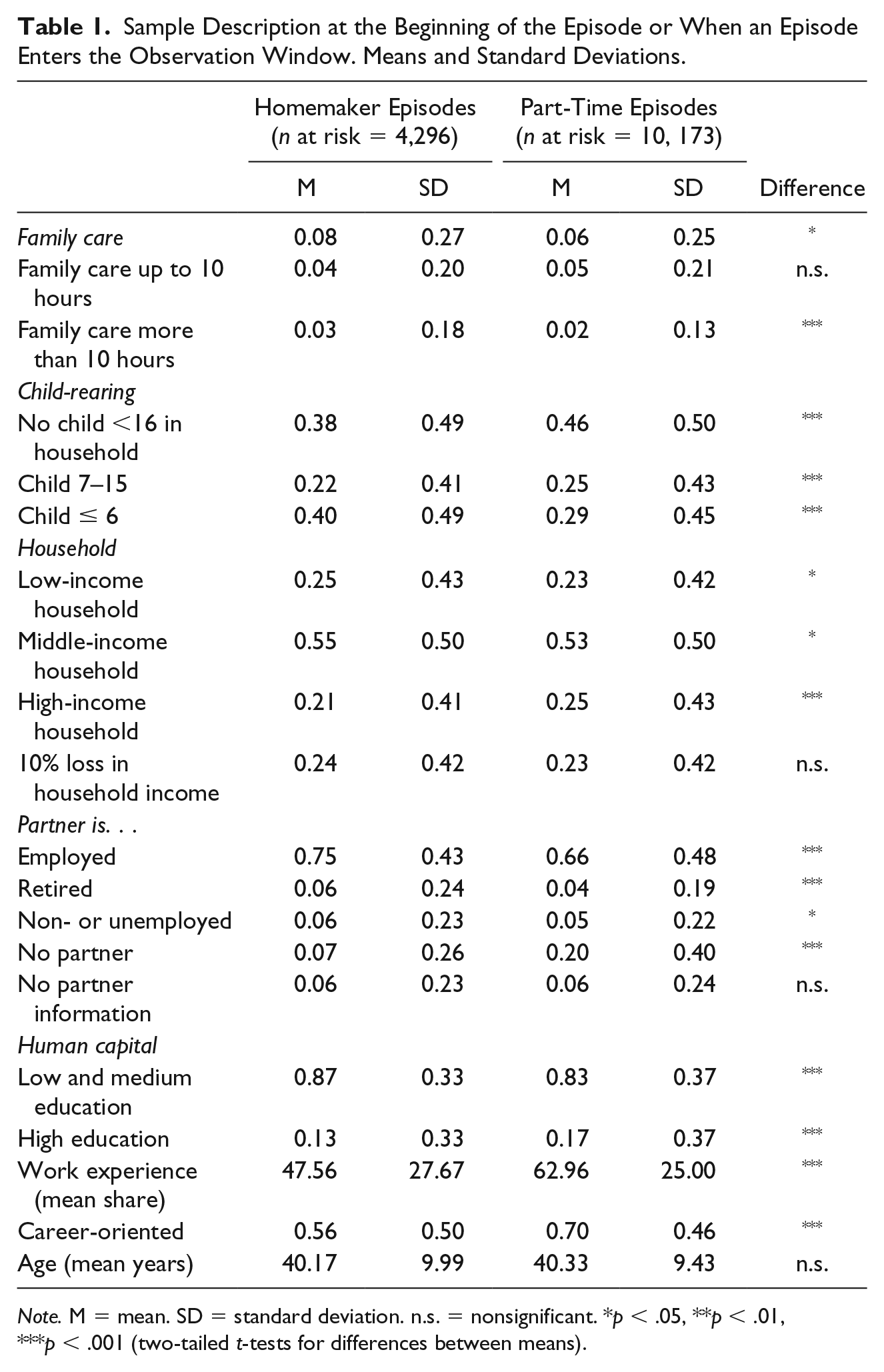
Note. M = mean. SD = standard deviation. n.s. = nonsignificant. *p < .05, **p < .01, ***p < .001 (two-tailed t-tests for differences between means).
Sixty-two% of women in the homemaker sample and 54% of part-time workers are living with a child/children younger than 16 years old in the household. Both groups differ with respect to income; a significantly larger proportion of women in the part-timer sample live in high-income households. Income drops of more than 10% occur in roughly one quarter of households in both samples. Consequently, women in both samples are vulnerable to income losses. With regard to partner’s characteristics, homemaking women significantly more often report to have an employed partner, while part-time working women significantly more often report to have no partner.
There are notable differences regarding women’s education, work experience, and career orientation. Women in the part-timer sample are more highly educated, more career-oriented, and have more work experience. Since entering the labor market, they have spent on average 63% of the time in employment, in contrast to only 48% among homemakers. Also, they more often state that having success in a job is (very) important to them. Thus, homemakers and part-time working women represent two distinct groups that differ slightly in the extent of family caregiving and more substantially with regard to typical child-rearing responsibilities, household situation, partner’s labor market participation, education, work experience, and career orientation.
Multivariate Results
The estimated rates of entering the workforce or changing from part-time to full-time work are reported in Table 2 as hazard ratios. Hazard ratios greater (less) than 1 indicate that the covariate is associated with an increased (decreased) probability of experiencing the respective employment transition. If the hazard ratio is 1, there is no association between a covariate and the transition probability. Estimated rate of change can be transformed to percentage change in the hazard for a one-unit increase in the predictor by the formula (Hazard Ratio – 1)*100. For each transition, model specifications include family care intensity as well as the end of family care. To account for unobserved heterogeneity, an individual-specific “random effect” is included. In all model estimates, the variance of this parameter θ (theta) is greater than 0 and statistically significant, indicating the importance of controlling for unobserved individual factors.
Estimated Transition Rates, Cox Shared Frailty Regression Models.
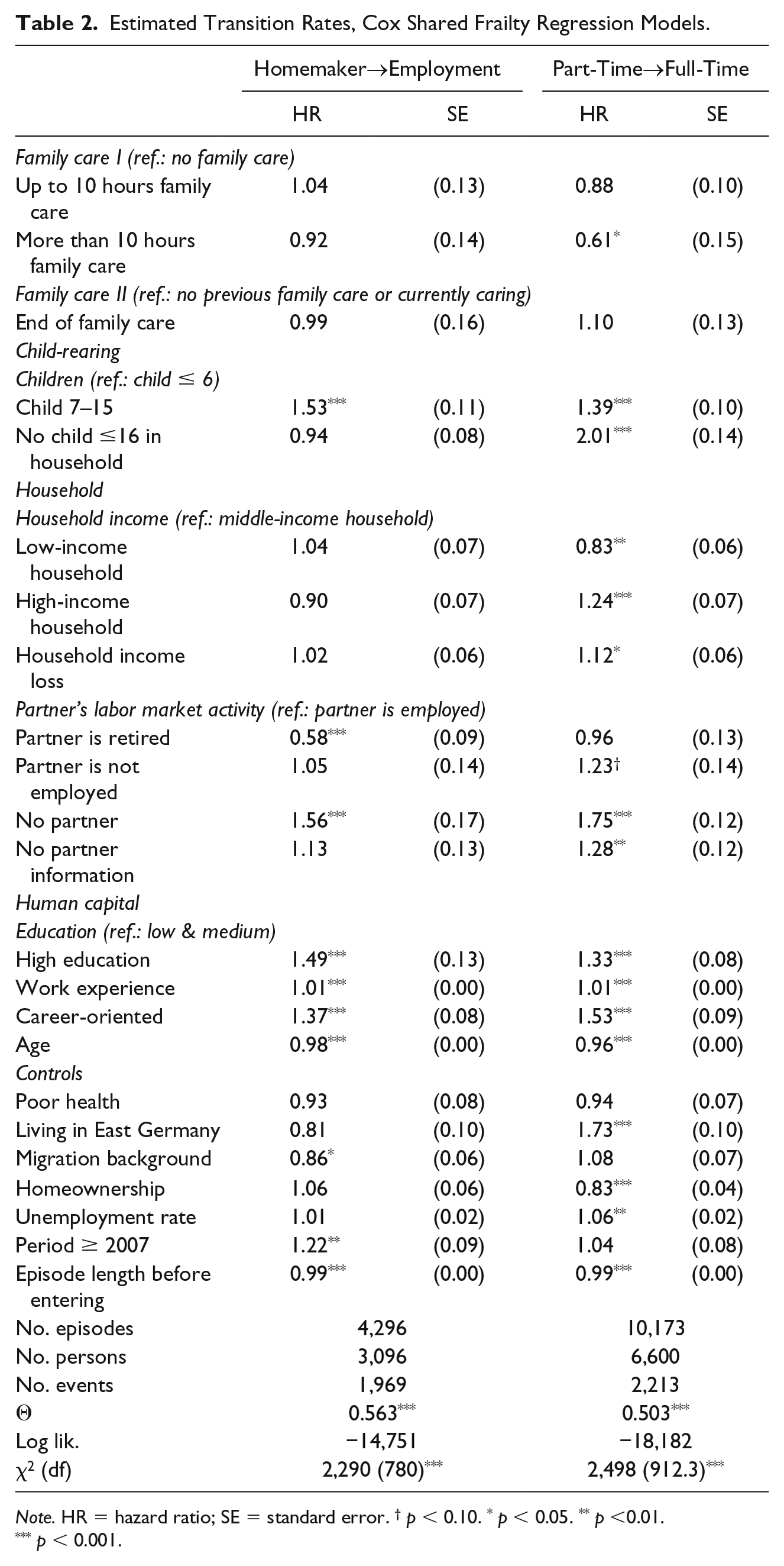
Note. HR = hazard ratio; SE = standard error. † p < 0.10. * p < 0.05. ** p <0.01. *** p < 0.001.
Table 2 shows the results of event history models for homemaking and part-time working women’s labor market transitions. We started by analyzing whether current family care has an impact on women’s (re-)employment entries (Hypothesis 1a), and whether this effect is stronger for women who provide more hours of family care (Hypothesis 1b). We find confirmation for Hypotheses 1a and 1b only for the part-timer sample. Homemaking family caregivers have no reduced hazard to enter employment. In contrast, for part-time working women who provide more than 10 hours of family care during the workweek, family caring reduces women’s propensity to switch from part-time to full-time work by about 39%. Fewer than 10 hours of family care have no significant effect.
Next, we tested alternative hypotheses predicting that the end of a family care episode either increases the likelihood to enter employment or increase working hours (Hypothesis 2a), or has no effect (Hypothesis 2b). The results support Hypothesis 2b. When family care comes to an end, homemakers with previous family care tasks do not significantly differ from homemakers with(out) family care commitments. The same applies to part-time working women: the end of family care does not significantly increase their tendency to change to full-time employment.
Furthermore, our analyses reveal additional interesting results. Among homemakers only those with school-aged children have a significantly higher propensity to enter employment, while those with preschool children as well as those without (co-residing) children rather remain nonemployed. In contrast, part-time working women have a significantly increased propensity to change to full-time when their children reach school-age and their propensity increases further if they have no (co-residing) children. With regard to household financial resources, we do not find any significant associations for the homemakers, while part-time working women’s labor market behavior is significantly influenced by both, the overall household income as well as income losses. Part-timers from low-income households have a significantly decreased propensity and part-timers from high-income households have a significantly increased propensity to change to full-time work as compared to medium-income households. This pattern might reflect the limited opportunities of low-paid part-time workers to increase working hours due to working in specific labor market segments which mainly offer atypical work arrangements. Furthermore, part-time working women having to deal with a loss of household income also have a significantly increased propensity of switching to full-time employment, possibly as a compensation for decreased financial resources. Partner’s characteristics are very important for women’s employment transitions. Homemakers living with a retired partner have a reduced propensity of taking up employment and those living without a partner an increased propensity, while no significant differences are observed between homemakers with an employed partner and those with a non- or unemployed partner. The hazards of changing from part-time to full-time employment are significantly increased for women with a non- or unemployed partner and those without a partner. For both transitions, highly educated women, those with more work experience and those who are more career-oriented have a significantly higher propensity to enter the labor market or to increase working hours. Finally, our results show that higher age is associated with lower chances of entering employment or increasing working hours despite controlling for other relevant labor market characteristics. However, based on our data we cannot determine whether this effect stems from age-discrimination by employers or older women’s preferences.
Discussion and Conclusion
While previous studies showed that women involved in family care, that is, caring for a partner, parents(-in-law), (adult) child, or other family members in need of regular care due to severe illness, disability, or old age, are more likely to reduce working hours or to drop out of the labor market (e.g., Heitmueller, 2007; Henz, 2006; van Houtven et al., 2013), our study also demonstrates that part-time working women providing extensive family care have a significantly reduced likelihood to increase their working hours from part-time to full-time over the course of family caregiving. In contrast, homemaking women providing family care did not behave differently than homemaking women without family care tasks. In terms of post-care behavior, previous studies suggest that after family care ends, women do not increase their labor market activity (e.g., Spieß & Schneider, 2003; Wakabayashi & Donato, 2005). This finding has been confirmed for part-time working women as well as homemaking women in our study. However, the results obtained from this study refer to the particular national case of Germany. Therefore, one should be careful when generalizing results to other country contexts with different levels of female employment, prevalence of part-time work, and different policy frameworks. Consequently, it would be worth testing whether and to what extent family caregivers’ ability to return to the labor market or to increase working hours during or after a family care period varies across different welfare state contexts.
Overall, our study strengthens the idea that homemakers in Germany are a highly selective group with low labor market attachment. They might perceive the family caregiver role as a long-term commitment and may systematically select into providing family care. Accordingly, irrespective of current or previous family care activities, homemaking women in general have a lower labor market attachment and low rates of entering or re-entering employment. The German tax system further supports women’s low labor market attachment with a “marriage premium for couples with unequal earnings, while the premium is zero for couples with similar earnings” (Aisenbrey, Evertsson, & Grunow, 2009, p. 578). This creates strong disincentives for nonemployed married women to increase their labor market activity. Furthermore, nonemployed or marginally employed wives profit from a free coverage in their spouses’ health insurance.
In contrast, part-time working women providing extensive family care have a lower propensity to enter full-time work than their noncaregiving counterparts; however, after family care ends, part-time working women do not increase their working hours either. Therefore, it might be possible that part-time working women already worked reduced hours before assuming family care and they selected into the family caregiver role due to available time resources. In this case, part-time working women’s reduced propensity to enter full-time work over the course of family caregiving is not a result of family care, but rather shows a generally lower labor market attachment. Accordingly, it would be unlikely for them to increase their workload when family care terminated. However, previous studies addressing this particular selection problem found that current working hours were not related to subsequent family caregiving, whereas family caregiving was related to working hour reductions or labor market dropouts (e.g., Berecki-Gisolf et al., 2008; Lee, Tang, Kim, & Albert, 2015; Pavalko & Artis, 1997). This indicates two things. First, female family caregivers are not a selective group of women with low labor market attachment even before caregiving. Second, family care provision competes directly with working time. Along this line of argument, the results obtained in this study can also be interpreted as follows: family caregivers in part-time employment have a reduced propensity to change to full-time work as family care leaves them less time available to engage in paid work to a greater extent. Upon the termination of family care, part-time working women may experience diverse constraints that prevent them from taking up a full-time position.
Within our analytic strategy, we were not able to explore factors that could facilitate family caregivers’ chances to increase their labor market activity. For example, scrutinizing the role of support networks in the family care–employment relationship could be an avenue of future research. A recent study showed that two thirds of all family caregivers receive care support from other family members, friends, or neighbors, but also from professional care services (Ehrlich & Kelle, 2019). However, our data does not allow to investigate the role of informal and formal support networks on female family caregivers’ chances to enter employment or to increase working hours. Moreover, we were not able to explore which constraints exactly prevent women from increasing their labor market activity after family care has stopped. The relevance of different factors could be addressed in further research using a qualitative or experimental research design (for experimental research designs on investigating individual’s job opportunities, see for example Hipp, 2018; Weisshaar, 2018). It is possible that former family caregivers ‘opt’ to work reduced hours or to stay out of work (argument derived from the economic theory of the family) or they are rather ‘blocked’ out by (potential) employers (arguments derived from labor demand side approaches). In addition, the rather inflexible and highly segmented German labor market provides few opportunities for employees to increase working hours in accordance to their life circumstances. If women opt to work part-time hours once in their career, this decision is often hardly reversible. The government has addressed this issue and implemented a new law providing a right to return to full-time hours in 2018 (BMAS, 2018). Moreover, it is also possible that women’s post-care employment behavior is determined by their health. Although we controlled for women’s overall health status, future research should investigate patterns of health trajectories over the course of family caregiving and how they relate to women’s (re-)employment chances after family care has terminated. Also, due to data limitations we were not able to parse out whether women’s (re-)employment chances depend on who was cared for and how the family care episode ended. For example, if a care-dependent partner recovers, this may, from a psychological point of view, represent a different starting point for a woman’s future employment than if the care-dependent partner has died.
Notwithstanding these limitations and the need for further research as well as data improvements, this article makes important contributions to the literature. Little research has examined the career paths of women providing family care, which plays an increasingly important role in aging societies. This study contributes to the literature by analyzing whether and to what extent women with current and previous family care tasks (re-)enter the labor market or increase working hours from part-time to full-time. Moreover, our results yield implications for policies addressing family care and employment. The increasing demands of employers for a skilled labor force in times of decreasing unemployment rates are potentially in conflict with the increasing demand for care provision in an aging society that relies on care provided by the family. On the one hand, the labor market in Germany increasingly relies on prolonged employment careers and the mobilization of nonemployed and part-time employed women in order to counteract the emerging shortage of skilled labor, potentially minimizing the supply of family care provided by female family members. Furthermore, the social security system in Germany and similarly in other European countries punishes career interruptions as these lead to fragmented contribution records, and consequently, lower public pension benefits. On the other hand, the German care system depends strongly on home-based care provided by (very often female) family members to ensure that the care needs of the ill, disabled, and elderly are met. These family care demands are expected to increase in view of demographic aging. However, while policies encouraging maternal employment after childbirth have been considerably developed over recent years, policies supporting the reconciliation of family care and paid work have been largely ignored. Policymakers intending to increase women’s labor market integration and to uphold home-based care by family members should seek to minimize the negative consequences on employment chances of women who care for family members, for example, through expanding the infrastructure of professional care services and making them more accessible and affordable for the families. Labor market reintegration programs that not only address young mothers but also family caregivers could be another angle of support for former family caregivers.
Footnotes
Appendix
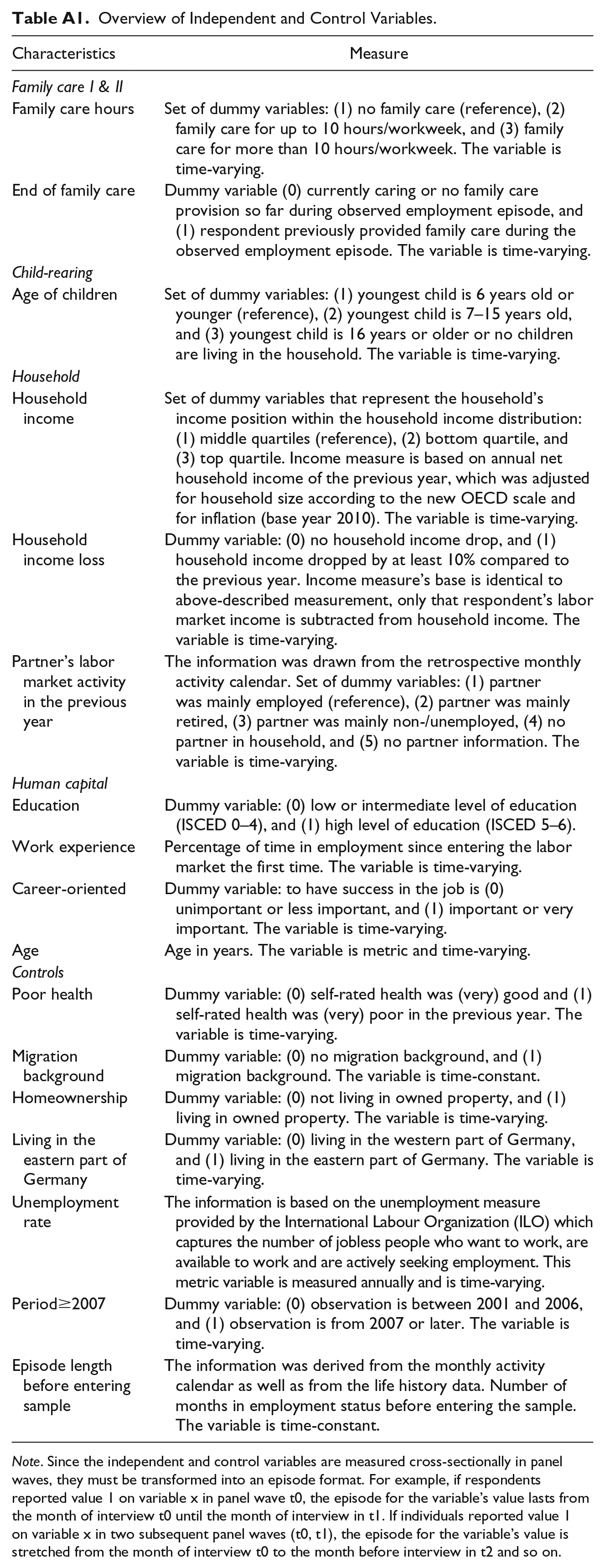
Overview of Independent and Control Variables.
| Characteristics | Measure |
|---|---|
| Family care I & II | |
| Family care hours | Set of dummy variables: (1) no family care (reference), (2) family care for up to 10 hours/workweek, and (3) family care for more than 10 hours/workweek. The variable is time-varying. |
| End of family care | Dummy variable (0) currently caring or no family care provision so far during observed employment episode, and (1) respondent previously provided family care during the observed employment episode. The variable is time-varying. |
| Child-rearing | |
| Age of children | Set of dummy variables: (1) youngest child is 6 years old or younger (reference), (2) youngest child is 7–15 years old, and (3) youngest child is 16 years or older or no children are living in the household. The variable is time-varying. |
| Household | |
| Household income | Set of dummy variables that represent the household’s income position within the household income distribution: (1) middle quartiles (reference), (2) bottom quartile, and (3) top quartile. Income measure is based on annual net household income of the previous year, which was adjusted for household size according to the new OECD scale and for inflation (base year 2010). The variable is time-varying. |
| Household income loss | Dummy variable: (0) no household income drop, and (1) household income dropped by at least 10% compared to the previous year. Income measure’s base is identical to above-described measurement, only that respondent’s labor market income is subtracted from household income. The variable is time-varying. |
| Partner’s labor market activity in the previous year | The information was drawn from the retrospective monthly activity calendar. Set of dummy variables: (1) partner was mainly employed (reference), (2) partner was mainly retired, (3) partner was mainly non-/unemployed, (4) no partner in household, and (5) no partner information. The variable is time-varying. |
| Human capital | |
| Education | Dummy variable: (0) low or intermediate level of education (ISCED 0–4), and (1) high level of education (ISCED 5–6). |
| Work experience | Percentage of time in employment since entering the labor market the first time. The variable is time-varying. |
| Career-oriented | Dummy variable: to have success in the job is (0) unimportant or less important, and (1) important or very important. The variable is time-varying. |
| Age | Age in years. The variable is metric and time-varying. |
| Controls | |
| Poor health | Dummy variable: (0) self-rated health was (very) good and (1) self-rated health was (very) poor in the previous year. The variable is time-varying. |
| Migration background | Dummy variable: (0) no migration background, and (1) migration background. The variable is time-constant. |
| Homeownership | Dummy variable: (0) not living in owned property, and (1) living in owned property. The variable is time-varying. |
| Living in the eastern part of Germany | Dummy variable: (0) living in the western part of Germany, and (1) living in the eastern part of Germany. The variable is time-varying. |
| Unemployment rate | The information is based on the unemployment measure provided by the International Labour Organization (ILO) which captures the number of jobless people who want to work, are available to work and are actively seeking employment. This metric variable is measured annually and is time-varying. |
| Period≥2007 | Dummy variable: (0) observation is between 2001 and 2006, and (1) observation is from 2007 or later. The variable is time-varying. |
| Episode length before entering sample | The information was derived from the monthly activity calendar as well as from the life history data. Number of months in employment status before entering the sample. The variable is time-constant. |
Note. Since the independent and control variables are measured cross-sectionally in panel waves, they must be transformed into an episode format. For example, if respondents reported value 1 on variable x in panel wave t0, the episode for the variable’s value lasts from the month of interview t0 until the month of interview in t1. If individuals reported value 1 on variable x in two subsequent panel waves (t0, t1), the episode for the variable’s value is stretched from the month of interview t0 to the month before interview in t2 and so on.
Acknowledgements
We are grateful for the useful comments and valuable suggestions by Sonja Bastin, the participants of the BIGSSS Field B colloquium (Bremen University), the participants at the ESPAnet Conference, Rotterdam, September 1–3, 2016 and the anonymous reviewers. The SOEP data were kindly provided by the SOEP Group at the German Institute for Economic Research (DIW), Berlin.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author’s contribution was funded by grants from the German Research Foundation (DFG) to the Bremen International Graduate School of Social Sciences (BIGSSS) [grant number: GSC 263/1] and from the Research Network on Pensions (FNA).