
Abstract
This article considers interactional trouble that arises when the social distribution of knowledge and interpersonal relationships come together in the delivery and reception of good news in pediatric neurology visits for video-electroencephalography testing. Contrary to common perceptions of good news as easy to deliver and receive, I find that it is occasionally fraught with hesitancy in this context. Using conversation analysis, I explore what drives this trouble and argue that some of the difficulty associated with good news in this context arises from its structure: Physicians prioritize conveying “the facts” of the news over characterizing its valence. However, parents treat physicians’ assessments of the news as critical for the news delivery. When physicians fail to evaluate the information they present, parents tend to treat news deliveries as incomplete, which not only causes difficulties in their reception of the news but also leads to protracted news deliveries.
The social distribution of knowledge and interpersonal relationships come together in our everyday lives when we deliver and receive news (Maynard 1997, 2003; Raymond and Heritage 2006; Sacks 1967; Terasaki 2004). If a friend tells you that she is pregnant, it may seem easy to determine what kind of response would be prosocial—a positive assessment or congratulations, for example. These reactions do two important things: they treat the informing as news and assess the news as positive. Assessments in this context can be either affiliative if they match or disaffiliative if they conflict with the teller’s position. Thus, when you respond to your friend’s pregnancy announcement with a positive assessment, you respond as someone who is close enough to her to know that this news is good. However, responding to good news is not always as straightforward as one might expect. Indeed, you would likely have more trouble formulating a prosocial response to your friend’s pregnancy announcement if you knew that her husband had undergone a vasectomy in the past (cf. Maynard 2003:19–20).
Popular belief tends to regard good news as easy to deliver and receive, but systematic research on news deliveries shows that participants engage in complex interactional work to collaboratively achieve the status of an announcement as news and, moreover, as news of a particular type, such as good, bad, funny, or sad (Maynard 1997, 2003; Terasaki 1976, 2004). For instance, whereas “good” news is typically delivered and responded to in an exposed fashion without mitigation or delay, “bad” news is commonly shrouded by delay and stoicism in its delivery and reception (Maynard 2003). From this perspective, the valence of news is jointly negotiated through its delivery and reception rather than inherent in its content. This also applies to institutional contexts such as medicine, where doctors and patients can find themselves at odds over the valence of medical facts. For instance, physicians routinely present the exclusion of serious diagnoses as patently good news, but patients treat these exclusions as a failure to adequately explain their presenting complaints (Maynard and Frankel 2006). Alternatively, patients may orient to undesirable implications of ostensibly good news—for example, when patients feel too ill to work but medical evaluations indicate that they are too well to qualify for disability assistance (Maynard 1997). Consequently, each news delivery represents a site of social influence where social solidarity hangs in the balance.
In this article, I consider how knowledge and interpersonal relationships play out in news delivery sequences where physicians deliver good news to families in pediatric neurology visits for video-electroencephalography (vEEG) testing. I find that these sequences are occasionally fraught with hesitancy and become protracted as a result. This initial observation poses a puzzle: Why is good news sometimes challenging to deliver in pediatric neurology? To approach this puzzle, I ask what drives this interactional trouble and argue that some of the difficulty associated with good news arises from its structure. I argue that in these encounters, physicians prioritize the informing component of the news over their evaluation of it, but parents treat both components as necessary before being willing to take up the news. When physicians fail to provide either the informing or their assessment of it, parents orient to news deliveries as incomplete, which not only causes difficulties in their reception of the news but also leads to protracted news deliveries.
Background
The knowledge and relational dimensions of news are shaped by the extent to which it informs the recipient and whether the recipient takes it up in a way that is affiliative. Existing research provides empirical support for these dimensions by reference to the complementary conduct of the teller and recipient (Maynard 1997, 2003; Terasaki 1976, 2004). Specifically, news delivery sequences represent courses of action where one participant proposes that some piece of information is news to a recipient and the recipient then confirms (or not) the newsworthiness of this information. If the recipient rejects the newsworthiness of the informing, then the sequence is usually aborted. However, if the recipient confirms the newsworthiness of the informing, then the teller typically develops it further, and the recipient should ultimately display their stance toward the news with an assessment. If the recipient’s assessment supports the teller’s stance vis-à-vis the valence of the news, then it will serve to generate affiliation.
The Knowledge Dimension of News Deliveries
Support for the idea that news should be informative comes from prior research that has shown speakers consistently work to avoid telling recipients things that they already know, which would erroneously cast them as uninformed. Before presenting information as news, speakers routinely implement preliminary sequences (Holt 1993; Schegloff 1988; Terasaki 2004) and prefaces (Sacks 1974; Sacks and Schegloff 1979). These are at least partially dedicated to establishing whether the recipient of a prospective news delivery will hear the information as news (e.g., “Did Joey tell you the news?”) while also allowing for the possibility that the recipient is already informed and providing an opportunity for this to be conveyed in advance (Terasaki 1976, 2004).
The Relational Dimension of News Deliveries
The relational dimension of news deliveries is primarily driven by the extent to which interlocutors agree on news valence. Goffman (1955:213) synthesized the social norms of interpersonal relationships in the concept of face—the sense of self that manifests publicly through social interaction as dimensions of participants’ identities are claimed or imposed and affirmed or undermined. Brown and Levinson (1987) extended this framework by differentiating between negative face, the human desire to be unimpeded in one’s actions, and positive face, or the desire to be understood and affirmed in social interaction. This is what is at stake in news deliveries: If the recipient does not have access to the teller’s stance regarding the valence of the news, then the recipient will likely encounter difficulty in formulating an affiliative response, and a failure to affiliate in this context is face threatening (Goffman 1955). Specifically, it jeopardizes the teller’s positive face (Brown and Levinson 1987). Consequently, when the teller’s stance is unclear, ambiguity can create an “affiliation problem” for the recipient (Stivers, Rossi, and Chalfoun 2022:1558).
To mitigate this threat, speakers may embed evidence of their stance toward the news in their delivery of it. While speakers may use pre-announcements as a means of gauging whether recipients already know the news, these preliminary utterances can also indicate the speaker’s stance vis-à-vis its valence (e.g., “Did Joey tell you the good news?”). Moreover, whereas presequences are designed so that deliveries can be aborted if a speaker has heard the news, the practice of prefacing news in a multiunit turn is largely oriented to conveying the speaker’s stance toward it (e.g., “The funniest thing happened on the way here” vs. “I had the worst drive here”). When speakers build characterizations of the news into their pre-announcements and prefaces of it, they aid in the relational dimension of news deliveries by projecting what kind of response would be affiliative (Terasaki 1976, 2004). However, the relational dimension of news deliveries is complicated by the fact that news deliverers do not always have primary rights to ascribe valence to the news they convey.
Relative Rights to Ascribe Valence to News
Although valence is best understood as a negotiated product of collaborative social interaction, participants nevertheless have asymmetrical roles in establishing it (Heritage and Raymond 2005; Maynard 2003; Raymond and Heritage 2006). Maynard (2003:89) shows that participants engaged in the delivery and reception of news orient to the consequences it has for specific individuals or the “consequential figures” of the news. He argues that the relative rights to ascribe valence to news are directly associated with the degree to which the respective participants will be affected by it. There are three basic permutations of news deliveries in this regard: the teller announces news that is primarily consequential for (1) themselves, (2) the recipient, or (3) a third party. The relative rights associated with each of these are summarized in Table 1.
Relative Rights to Ascribe Valence
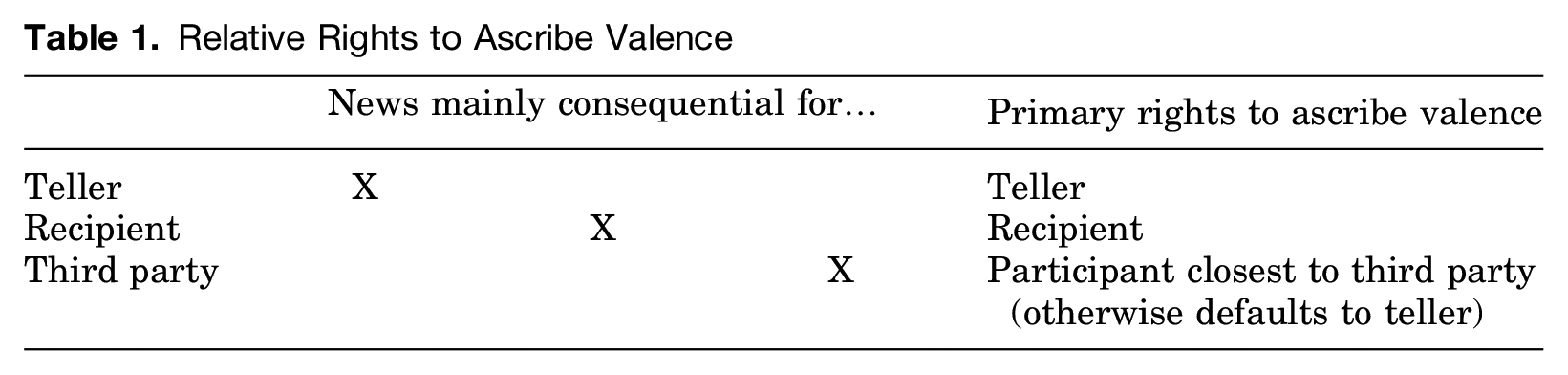
In each version outlined in Table 1, rights to ascribe valence are shaped by the consequences of the news, or more specifically, who must ultimately bear them and to what extent. If the news is consequential for the recipient rather than the teller, then the recipient has a more pronounced role in shaping its valence. When the news is about a third party, the participant closest to the third party has primary rights to ascribe valence. That is, through their social relationship to the third party, the teller or recipient (or both) will also be affected by the news, albeit to a lesser extent. If the news affects neither teller nor recipient, then by virtue of going first, the teller has primary rights and opportunity to ascribe valence, and by virtue of going second, the recipient is generally in a position to affiliate with the teller’s stance on the matter (Heritage and Raymond 2005). This holds for news that is similarly consequential for both teller and recipient—for example, when a father tells his son that his mother has cancer (Beach 2002).
News Deliveries in Medical Contexts
Managing the knowledge and relational dimensions of news deliveries can be challenging, especially in medical interactions, where physicians deliver news that they have primary rights to know about but that primarily concerns patients and their families. This can make the relational dimension of news deliveries challenging for three main reasons. First, patients and their families may not be able to appreciate the full range of implications that the news will have for them and may struggle to determine whether the news is good or bad. Second, parents may understand how the news will affect them but may be hesitant to encroach on physicians’ epistemic rights to medical knowledge. Third, physicians and families occasionally orient to the news differently. Perhaps nowhere is this more evident than in the pediatric context, where parental authority and medical authority sometimes collide. For instance, when physicians present the exclusion of diagnoses (e.g., “Your son’s episodes aren’t seizures”) as good news, parents sometimes orient to this as problematic because it fails to address their presenting complaint, and they may design their responses to expose this “symptom residue” rather than to affiliate with physicians (Maynard and Frankel 2006). In these cases, physicians engage in what Maynard (1997:119) calls “problematic presumptiveness,” where their presumptive orientation toward the valence of the news does not jibe with parents’ treatment of the news upon its delivery. Occasionally, this can be exploited to temper undesirable news: by foregrounding good elements of bad news, physicians and families can make news “bivalent” (Stivers and Timmermans 2017).
Researchers have examined the delivery of diagnostic news after autism evaluations (Gill and Maynard 1995; Maynard 2003), pediatric primary care visits (Stivers 2007), and genetic screenings (Stivers and Timmermans 2017), among others. What is clear from these studies is that parents evaluate the news for what it means for them and their children. However, less is known about the extent to which physicians and parents orient to the relative rights and obligations associated with news deliveries in these highly specialized contexts. This leaves open the question of how the knowledge and relational dimensions of news deliveries get managed when issues associated with who has primary rights to evaluate the news and what constitutes affiliative uptake become more complicated.
In this research, I target news deliveries in pediatric neurology visits for vEEG monitoring. Here, news deliveries normally involve an informing about the presence or absence of seizure activity. However, while physicians have primary rights to interpret the vEEG data and deliver the news, parents have primary rights to assess the news in terms of what it means for their family. As tellers, physicians are well positioned for the knowledge dimension of news deliveries, but how do they manage the relational dimension in light of the complications outlined previously? I explore whether and how physicians and parents orient to the knowledge and relational dimensions of news deliveries in the pediatric neurology context.
Data and Methods
Data for this study consist of video-recorded pediatric neurology visits for overnight vEEG testing collected in a teaching hospital in Southern California in 2018. The corpus contains recordings from three phases of the visit: (1) admission interviews, (2) the neurology team reviewing the vEEG data in the lab, and (3) the rounds phase, where the neurology team reports their findings to the families. The present study focuses on the rounds phase, which consists of 38 discrete encounters. All participants provided informed consent, Institutional Review Board approval was obtained in advance, and identifying references to persons and places have been pseudonymized.
During these visits, patients are fitted with electrodes that measure the electrical activity in their brains throughout the night while an in-room camera provides a concurrent visual record of their body. This assists the neurology team in differentiating between electrical activity associated with muscle activation during normal bodily movements and that indicative of seizures. However, reading vEEGs is not like reading pregnancy tests; there is subjective interpretation involved, and research suggests that interrater reliability among EEG readers is lacking (e.g., Hussain et al. 2015). Yet the interpretive nature of vEEG testing might be lost on parents who see high-tech medicine as all science and no art.
When the neurology team sets out on rounds the morning after vEEG monitoring, they stop at each patient’s room to report preliminary findings. In most cases, but not all, this entails delivering (un)desirable news of some kind. In building a collection for analysis, I excluded cases that did not involve any presentation of vEEG findings because there was no orientation to valence, good or bad, by any parties to the encounter. This happened when, for instance, the neurology team requested that the patient stay for a second night of observation, and thus testing remained “in progress.” After excluding such cases, 25 encounters remained.
For the purposes of this study, valence statements are operationalized as utterances that display an evaluative stance vis-à-vis the news to which they refer. Consistent with prior research, preliminary review of the initial collection confirmed that participants orient to bad news in ways that diverge from cases where the news was treated as good. For instance, explicit characterizations of the news as bad are virtually nonexistent in the corpus (Freese and Maynard 1998). Yet valence is typically conveyed overtly when news is good (Maynard 2003). This “on record” treatment of valence offers greater analytical leverage and clarity. For this reason, I excluded eight cases where news was delivered but parents and physicians either offered an overall negative evaluation of the child’s test results or did not indicate their orientation to its valence at all.
Thus, in the remaining cases, physicians and parents ultimately arrive at a mutual orientation toward the news as positive overall, a total of 17 good news delivery sequences. As I show, there can be potential ambiguity at the outset of the news delivery sequences in some cases, but in all cases, physicians and parents ultimately orient to the news as good.
This study utilizes conversation analytic methods to identify patterned usage of interactional practices in news deliveries (Sacks, Schegloff, and Jefferson 1974; Sidnell and Stivers 2013). Consistent with the principles of conversation analysis (CA), data were transcribed in detail to capture various features of voice quality, such as amplitude, stress, and tempo (Hepburn and Bolden 2013). I then built a collection including all news delivery sequences in my data and refined this collection based on the operationalization discussed previously. Analysis of the core collection proceeded in two phases. First, I identified the primary components of news delivery sequences in these data. Second, I looked for patterns relevant to these components. My analysis focuses on participants’ orientations as they are delivering or receiving news, parent uptake of the news, and whether and how these news delivery sequences are expanded. In line with CA methods, I also considered the relative frequencies of particular elements of news deliveries, their uptake, and their expansions. Accordingly, I analyzed each case separately and worked to identify regularities across the collection (Schegloff 1997). In what follows, I detail this analysis further.
Analysis
The knowledge and relational dimensions of news are embodied by what I call the dual imperatives of news deliveries: (1) the news should inform the recipient, and (2) the participants should affiliate. In these data, informings typically involve the selective presentation of vEEG findings, such as the presence or absence of specific epileptiform activity, and evaluations involve explicit characterizations of the news as good. Although both components are generally present, their relative ordering varies, and this shapes how parents respond. We begin by exploring parents’ uptake of news as it is most frequently delivered, with the informing first.
Foregrounding the Informing
As Table 1 indicates, when news is chiefly consequential for recipients in everyday life, they have primary rights to ascribe valence to it. Thus, in the context of vEEG news deliveries, we might expect parents to readily evaluate the news first. However, in this section, I provide evidence that parents treat news deliveries as incomplete if the physician’s evaluation is missing. Here, I focus on cases where physicians announce news without characterizing its valence. Drawing on responses to these informings as my primary evidence, I argue that parent conduct embodies a reluctance to assess the news ahead of the physician.
When physicians announce news without displaying a stance vis-à-vis its valence, parents generally fail to assess the news and, moreover, treat it as insufficient for them to assess until the physician offers an evaluation. These account for 71 percent (n = 12) of cases. Although an informing without an evaluation can stand as a complete provision of news in some contexts (e.g., “I got an A on my history test”), parents tend to treat the physician’s evaluation as a normatively required component of news deliveries in this context. This is evidenced by various features of parents’ situated conduct, including, for instance, their pursuit of clinicians’ evaluations. This is readily apparent in Extract 1.
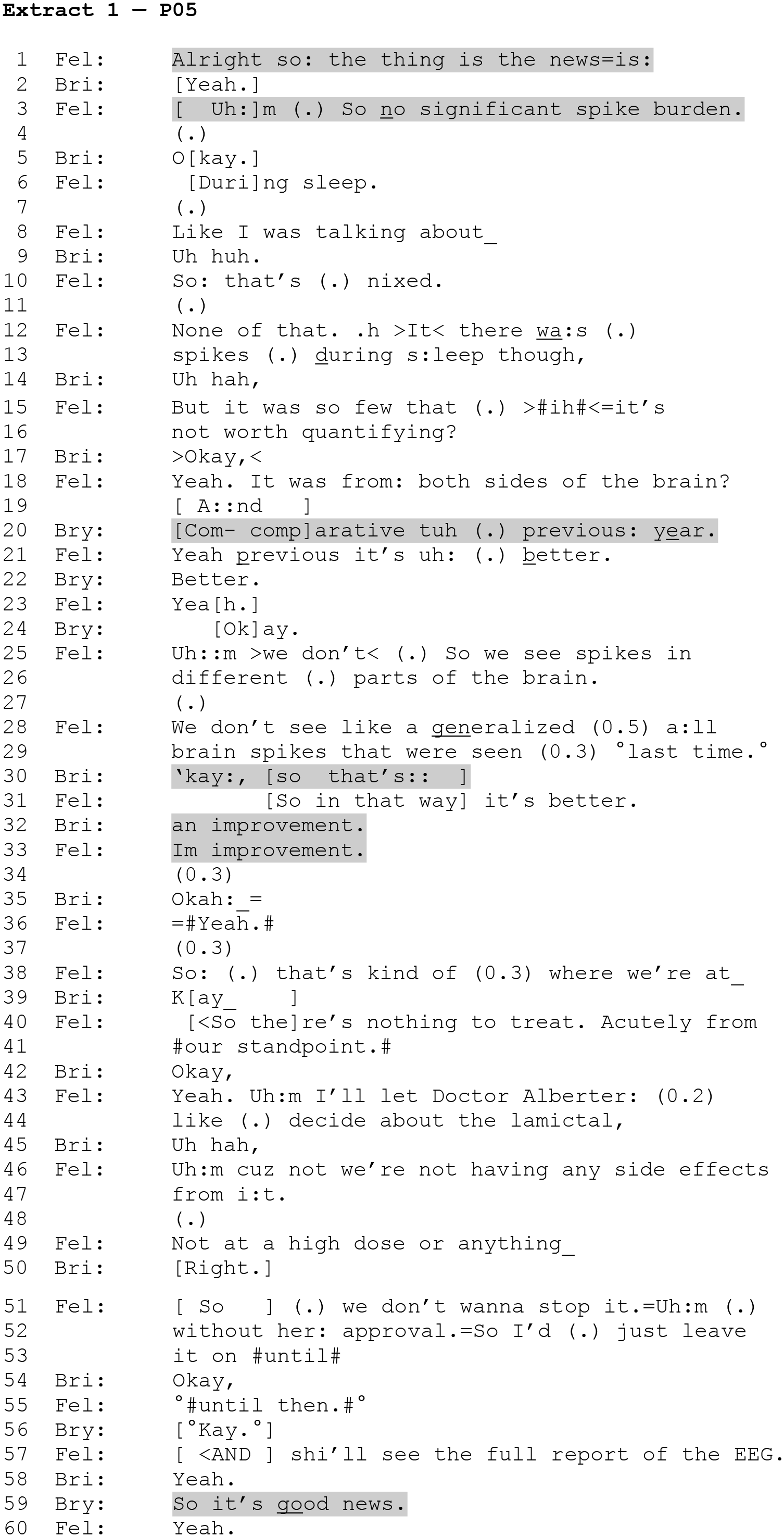
Ben is an eight-year-old in the clinic for routine monitoring. He is accompanied by his parents, Brittany and Bryan. As is typical in teaching hospitals, physicians in training (residents and fellows) are often tasked with conveying the news to families. In this case, the fellow begins his news delivery with a pre-announcement that stops short of evaluating the news (line 1) in favor of foregrounding the informing (line 3).
Brittany receipts the informing with an acknowledgment token (line 5), which she produces in overlap with the fellow as he expands his turn with more contextual detail (line 6). At this point, the valence of the news remains unstated. The fellow’s language is technical and vague insofar as “no significant spike burden” on the one hand sounds positive, but on the other hand, it implies at least some degree of “spike burden,” and neither “spike” nor “burden” sound promising on their own, let alone when combined (line 3). As is typical of these data, the parents treat this as an incomplete provision of the news. Brittany offers acknowledgments and continuers that reveal neither her understanding of the information nor her stance vis-à-vis its valence (lines 5, 9). Rather, they treat the news delivery as ongoing (Heritage and McArthur 2019; Jefferson 1981; Schegloff 1982).
Instead of evaluating the news at this point, the fellow expands his informing at lines 12 and 13 with another layer of factual detail that explicates his prior “no significant” formulation (line 3). Yet again, Brittany treats the news delivery as incomplete, receipting this information only with an acknowledgment (line 14). And the cycle repeats once more as the fellow expands his informing (lines 15–16), and Brittany receipts it with a continuative “Okay,” (line 17) that registers but does not evaluate the information (Guthrie 1997). With each increment of the informing, the fellow generates structural opportunities for Ben’s parents to display how they have understood the news, thereby treating an indication of understanding, such as an assessment, as relevant and invited. Yet in withholding an assessment of the news thus far produced, Brittany and Bryan treat the informing as insufficient for them to evaluate on its own.
The fact that Ben’s EEG revealed spike-wave discharges originating from both hemispheres of his brain may be viewed as self-evidently good or bad by members of the neurology team. Yet this valence is embedded in medical knowledge to which the parents have limited access and reduced rights. This epistemic asymmetry may help explain parents’ reluctance to assess findings ahead of the physician, especially because first-position assessments, by virtue of coming first, “carry an implied claim that the speaker has primary rights to evaluate the matter assessed” (Heritage and Raymond 2005:16). Moreover, first assessments have a binding quality insofar as evaluating the news first implies that the speaker independently holds the stance embodied by their evaluation, which entails a degree of commitment to it and accountability for it. As I show, parents routinely withhold assessments until clinicians evaluate the news. In this way, parents orient not only to valence as a key component of news deliveries but also to physicians as having primary rights to ascribe valence to news in this context.
We gain further support for the claim that the parents are “withholding” assessment as part of orienting to the news as incomplete in what comes next. In a context where the physician has expanded his informing with additional details but has refrained from evaluating them, Bryan explicitly seeks to draw out the clinician’s stance by broaching a contrast with Ben’s prior vEEG (line 20). Through inviting the fellow to compare the present vEEG with the previous one, Bryan generates the relevance of an assessment on the fellow’s part. However, this establishes the relevance of an evaluation in relative, rather than absolute, terms. In response, the fellow marks the relative valence of the present vEEG results as better than before (line 21), but this creates problems for affiliation (Stivers et al. 2022).
Typically, after one person provides a clear assessment of something, coparticipants will also provide an assessment (e.g., Pomerantz 1984). Here, the physician complied with Bryan’s comparative language, assessing the vEEG as better, but his stance regarding the present news remains ambiguous overall—it is unclear whether this news is to be taken as good or if it is still bad despite being better. This ambiguity appears to be at issue in what follows, where even after the fellow specifies how the current vEEG results are better (lines 25–29), neither Brittany nor Bryan readily treat the news delivery as sufficiently complete. Rather, Brittany issues a B-event question (Labov and Fanshel 1977:100) at lines 30 and 32 that displays her orientation to the fellow as having primary rights to assess the information he has presented. In an environment where the parents have yet to receipt the informing as good, this question format creates an opportunity for the physician and parents to satisfy the affiliation imperative of news deliveries by converging on a mutual orientation toward the valence of the news.
Further evidence for this can be found at line 59, which comes after the fellow has indicated that he plans to defer to Ben’s primary neurologist on all treatment decisions (not shown). Here, Bryan reaches back to the news delivery and revives the relevance of agreement on its valence with a so-prefaced assertion that invites the fellow’s confirmation—“So it’s
Extract 1 represents a pattern in these data: parents treat physicians as having primary rights to characterize the valence of the news they deliver and tend to withhold uptake of the news until the physician has evaluated it. 1 When parents do assess the news first, they may nevertheless orient to the physician as having primary rights to evaluate it (Antaki 2012; Sidnell 2012; Stivers 2002).
We see this in Extract 2, with Walter, who brought his 11-month-old son, Wyatt, in for vEEG testing. Nearly two weeks prior to the present visit, Wyatt presented with seizure symptoms indicative of infantile spasms. At that time, he was prescribed a short-term course of a steroid called prednisolone to curtail his episodes. The present visit is to evaluate the effects of the drug and if it is not working, to pursue an alternative course of action to quell his seizure activity.
As with Brittany and Bryan, when the physician foregrounds the informing (lines 1–7, 9–10) Walter responds with continuers and minimal acknowledgments (lines 8, 11), treating the news as incomplete (Heritage and McArthur 2019; Jefferson 1981; Schegloff 1982). The resident then provides a plan of action that entails discharging Wyatt and tapering his prednisolone (lines 12–14). After a brief discussion of the titration schedule (not shown), the resident signals completion of her extended telling by reinvoking the plan to discharge Wyatt (lines 58–59).
Walter accepts the treatment plan, thereby providing for closure of the treatment recommendation sequence (line 60), but unlike Brittany and Bryan, he does not go further to elicit the physician’s evaluation of the news here. However, when the resident subsequently projects that she is ready and willing to close the news delivery sequence—“Any questions for us?” (line 61)—Walter orients to the valence of the news as missing (lines 62–63).
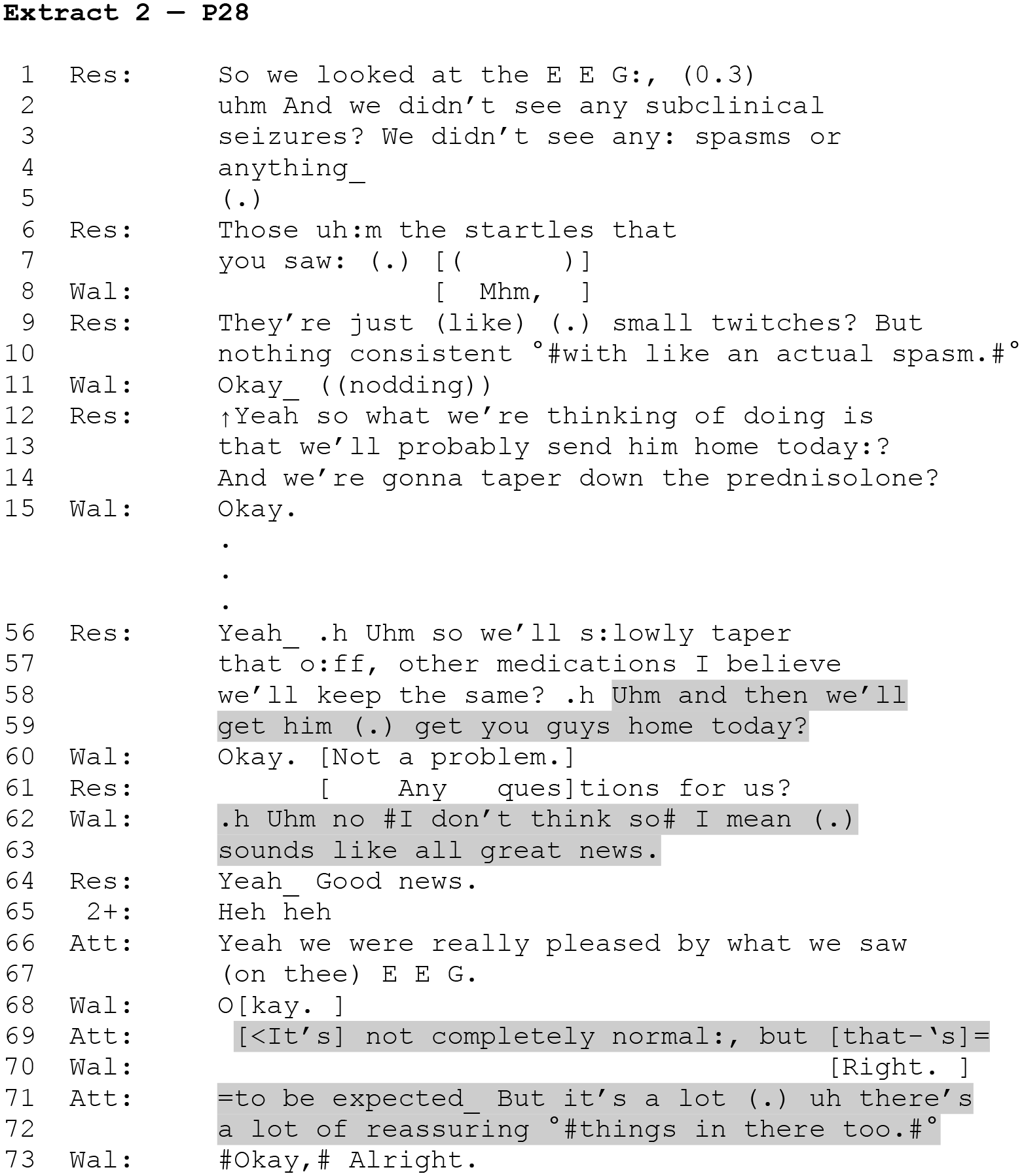
First hesitatingly (“Uhm”) and with mitigation (“think”), Walter declines to ask questions (line 62). He then self-repairs (“I mean”) before producing an assessment, but even here, at the end of the news delivery, he downgrades his assessment with the evidentially marked “sounds like” at line 63 (Raymond and Heritage 2006). Thus, his valence is presented for the physicians’ confirmation rather than spoken as a declaration on his own behalf (Sidnell 2012). Through inviting confirmation, Walter orients to the physicians in the room as having primary rights to know and to evaluate the news, and the resident aligns with this epistemic positioning when she designs her response as a confirmation followed by an assertion that the news is in fact good (line 64). Note also that here the resident responds with an interjection followed by a downgraded repetition (Stivers 2022) “Yeah_ Good news.”; and this might speak to her reluctance to be overly optimistic in conveying complex news. Indeed, the attending subsequently concedes that the news is not exclusively good (lines 69, 71–72).
Like Extract 1, the clinician in Extract 2 does not evaluate the news at her own initiative. Rather, she presents an informing through a series of facts delivered without evaluative terms that would reveal her stance vis-à-vis the valence of the news. Consistent with Extract 1, the parent in Extract 2 orients to the valence of the news as relevant but absent. These cases illustrate the variation between parents and clinicians with respect to how they approach news deliveries in this context. When physicians provide only the informing, parents consistently treat the news as incomplete by producing continuers but withholding more substantive uptake. If withholding uptake does not lead the physician to characterize the valence of the news, parents have other practices for securing an evaluation, including, as shown in Extracts 1 and 2, proffering a candidate one for the clinician’s confirmation. In the next section, I show what happens when physicians lead their news deliveries with an evaluation of the news rather than the informing.
Foregrounding the Evaluation
In a minority of cases (29 percent, n = 5), physicians present their evaluation of the news as the “headline” of it (Button and Casey 1985)—for example, “So we have good news on her EEG.” Although a report of good news can be sufficient to engender rapid affiliative uptake before the news is unpacked in some contexts (e.g., when telling your family that you have good news upon returning home from a job interview), I offer evidence that parents routinely treat such evaluations as prefatory in the context of vEEG news delivery and as insufficient for uptake on their own.
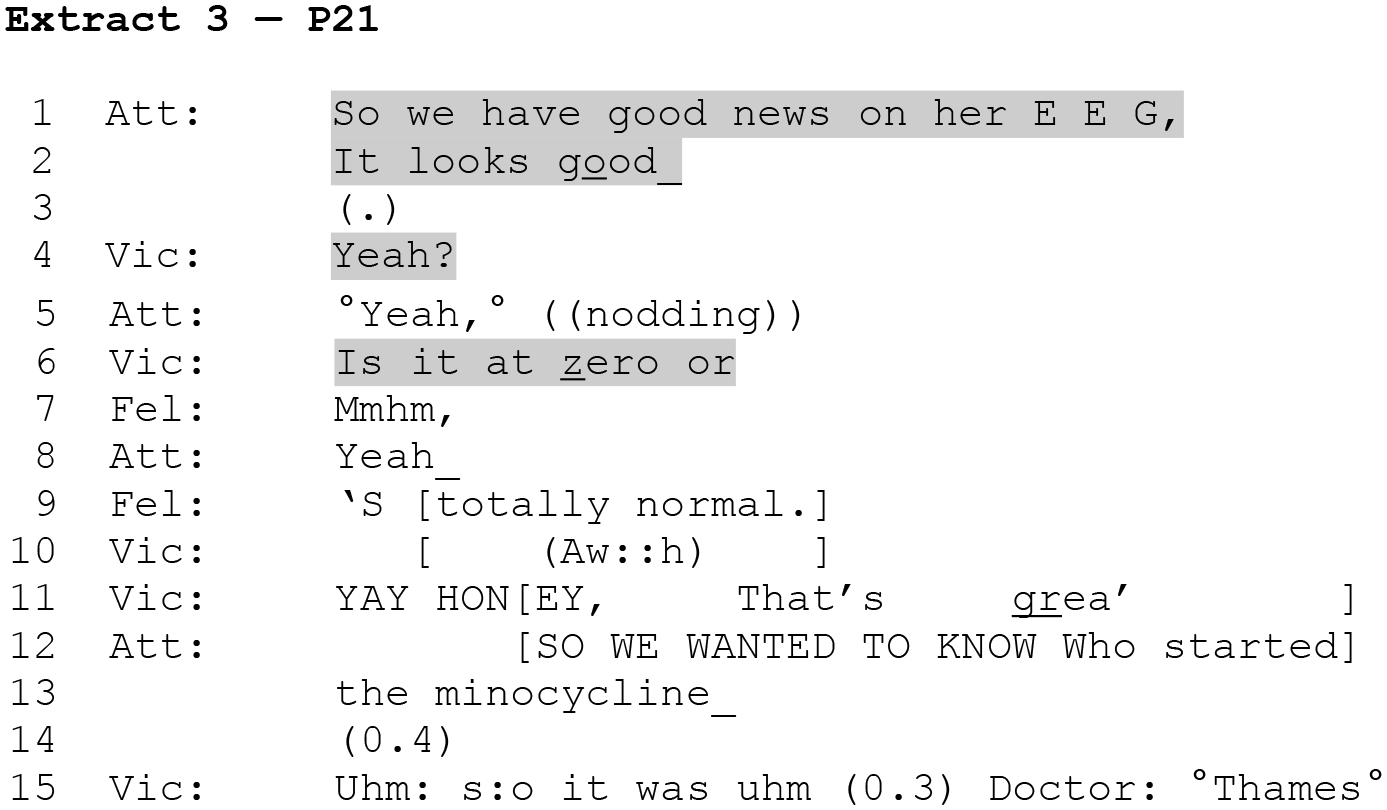
The patient in Extract 3 is Veronica, a developmentally disabled 16-year-old previously diagnosed with electrical status epilepticus in sleep (ESES). Her condition is characterized by near-continuous spike-wave discharges during sleep. Although this electrical activity is subclinical (meaning it cannot be observed in daily life as it happens), it interferes with normal cognitive development and can lead to cognitive decline when left untreated. Veronica’s psychiatrist prescribed an antibiotic (minocycline) in an attempt to reduce brain swelling, which could be provoking her ESES, but the effects of the drug on her brain cannot be assessed without a vEEG. For this reason, Veronica’s mother, Vickie, brought her in for testing.
Extract 3 begins as the attending physician characterizes the vEEG findings (lines 1–2). In this case, she immediately issues an evaluation of the news, “So we have good news on her E E G,” (line 1), and follows it with a valence-based gloss of the vEEG (line 2). Importantly, however, neither the pre-announcement nor the announcement proper articulates the basis for the valence they advance—that is, the actual informing about the vEEG findings. In other words, the attending conveys that the news is good but not what the news is.
As a first form of support for the claim that physicians’ evaluations of the news are treated as insufficient for meaningful uptake on their own, we can observe that Vickie, like the parents in Extracts 1 and 2, treats the news as incomplete (line 4). Initially, Vickie does not respond at all (at line 3), and when she does respond, it is with a request for confirmation (line 4). Such known-answer requests for confirmation are routinely used and oriented to as account solicitations (Raymond and Stivers 2016). Here, we see that Vickie is orienting to an account for the positive evaluation of the news as not only relevant but as absent (and therefore as expected in this context). When the attending provides only a minimal confirmation (line 5), Vickie pursues a basis for the valence of the news directly—“Is it at
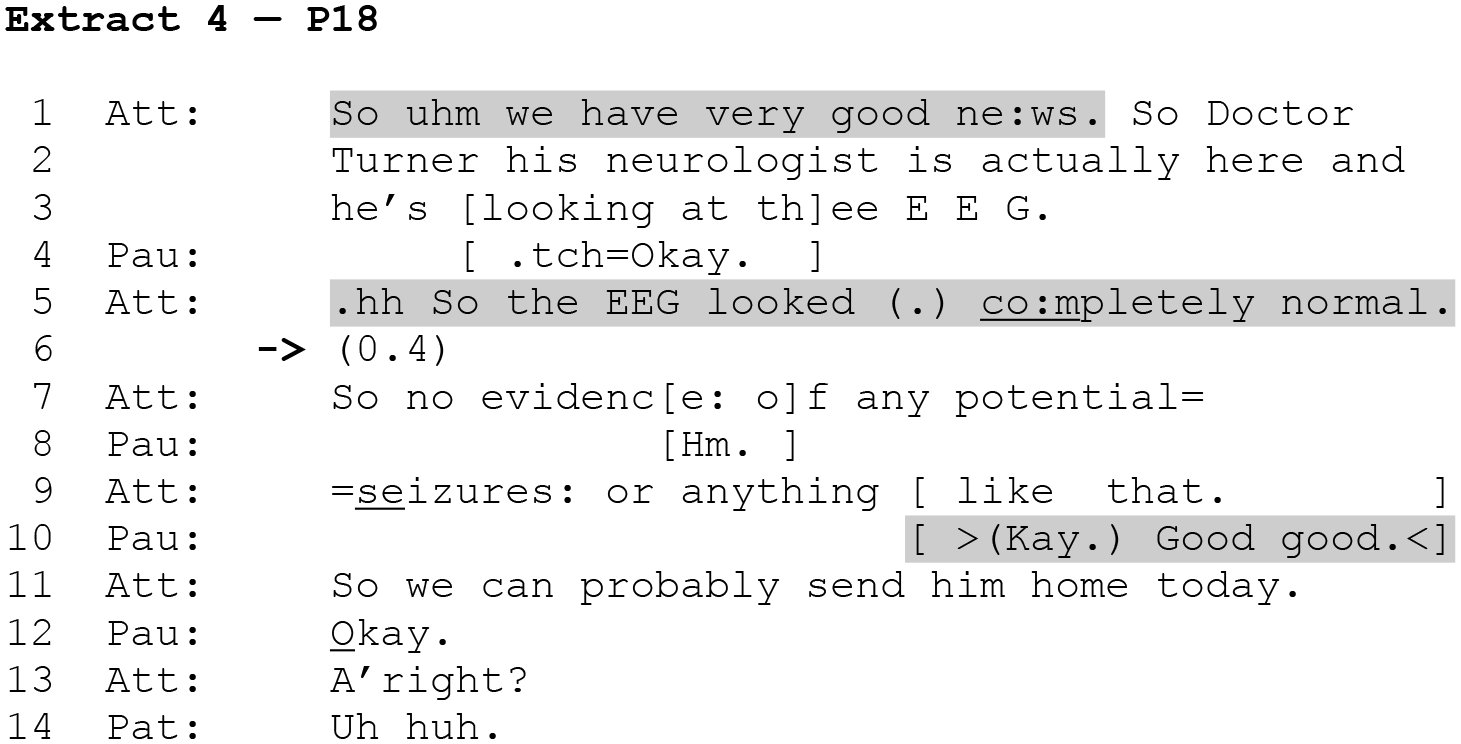
We see a similar pattern in Extract 4. Here, the patient is 17-year-old Parker. He has had two lifetime seizures, neither of which occurred recently. However, his parents noticed that his legs jerk occasionally when he sleeps, so they brought him in for testing to determine the cause. Only Parker and his father, Paul, are present during rounds. Here, the attending begins her news delivery with a valence characterization that serves as a headline for the news—“So uhm we have very good ne:ws.” (line 1). She then goes on to produce an announcement at line 5 that utilizes an extreme-case formulation of a positively valenced gloss of the EEG as “
However, as with Extract 3, Paul treats neither the valence-based preface (line 1) nor the valence-based gloss (line 5) of the findings as a complete provision of the news. An assessment from Paul is most clearly relevant at line 6, just after the attending’s gloss of the EEG as “
Prioritization
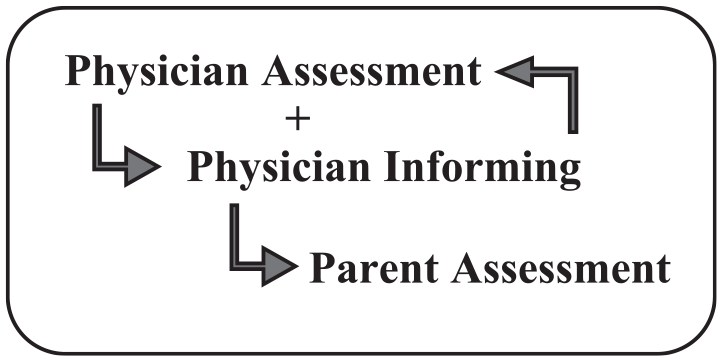
In this section, I show that physicians prioritize the informing component of the news over their evaluation, but parents treat both components as necessary before they are willing to take up the news. Extracts 1 and 2 showed that when physicians present only an informing, parents pursue the physician’s evaluation. This led me to consider whether parents primarily sought valence. If this were the case, we would expect parents to readily provide assessments in cases where the physician foregrounds an evaluation of the news. Yet, Extracts 3 and 4 suggest that parents do not have an exclusive interest in securing the physician’s evaluation. Parents tend to wait when presented with an evaluation of the news and continue to withhold affiliation until a basis for the evaluation is provided, thus treating both components as required before they are willing to take up the news. This claim is supported by three key forms of evidence. (1) Parents tend to readily assess the news once both the informing and the physician’s evaluation have been provided, but (2) they tend to withhold uptake when only one component has been provided, and (3) if either component is absent, parents will solicit it. This model of news delivery is depicted in Figure 1.
The Parent Model
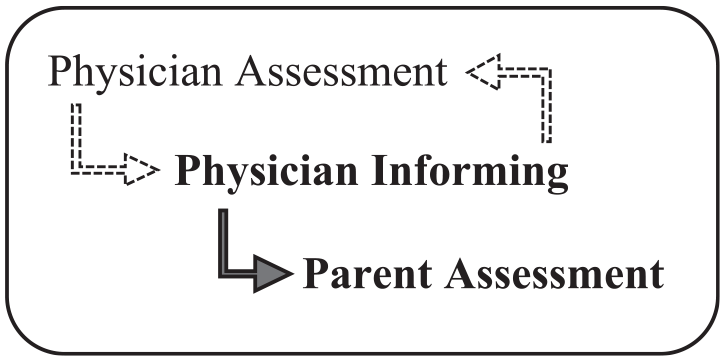
By contrast, physicians lead with informings most of the time (71 percent, n = 12). In some cases, they work to delay (or avoid) expressing their evaluation of the news (n = 5), and occasionally, they indicate a readiness to close the news delivery activity before they have characterized the valence of the news (e.g., Extract 2). Thus, as Figure 2 illustrates, the physicians’ model of news delivery varies from the parents’ model in that priority is given to the informing.
The Physician Model
Because physicians deliver informings first most of the time, they may find themselves working to elicit parent uptake at a point that parents treat as “too early” because physicians have not yet provided their own evaluation. The result is, as shown in Extracts 1 and 2, protracted news deliveries where physicians are searching for a parent evaluation while parents are searching for a physician evaluation. When clinicians include both components of the news, parents tend to respond with assessments, leading to relatively short, unproblematic news deliveries. However, parents occasionally withhold uptake despite the presence of an informing and an evaluation (e.g., Extract 5, discussed in the following section).
Negotiating the Adequacy of Informings
Thus far, I have shown that parents tend to withhold uptake of the news until both the informing and the physician’s evaluation of it have been provided. However, much remains to be understood about how these components shape parent uptake. What exactly is it about an informing and an evaluation that makes the difference for parents? In this section, I argue that not just any informing will suffice but rather, an informing that addresses parents’ primary concerns (e.g., their motivation for the present visit) paired with an evaluation that they can endorse. Thus, although a sufficient news delivery minimally contains an informing and an evaluation, the adequacy of each is jointly negotiated.
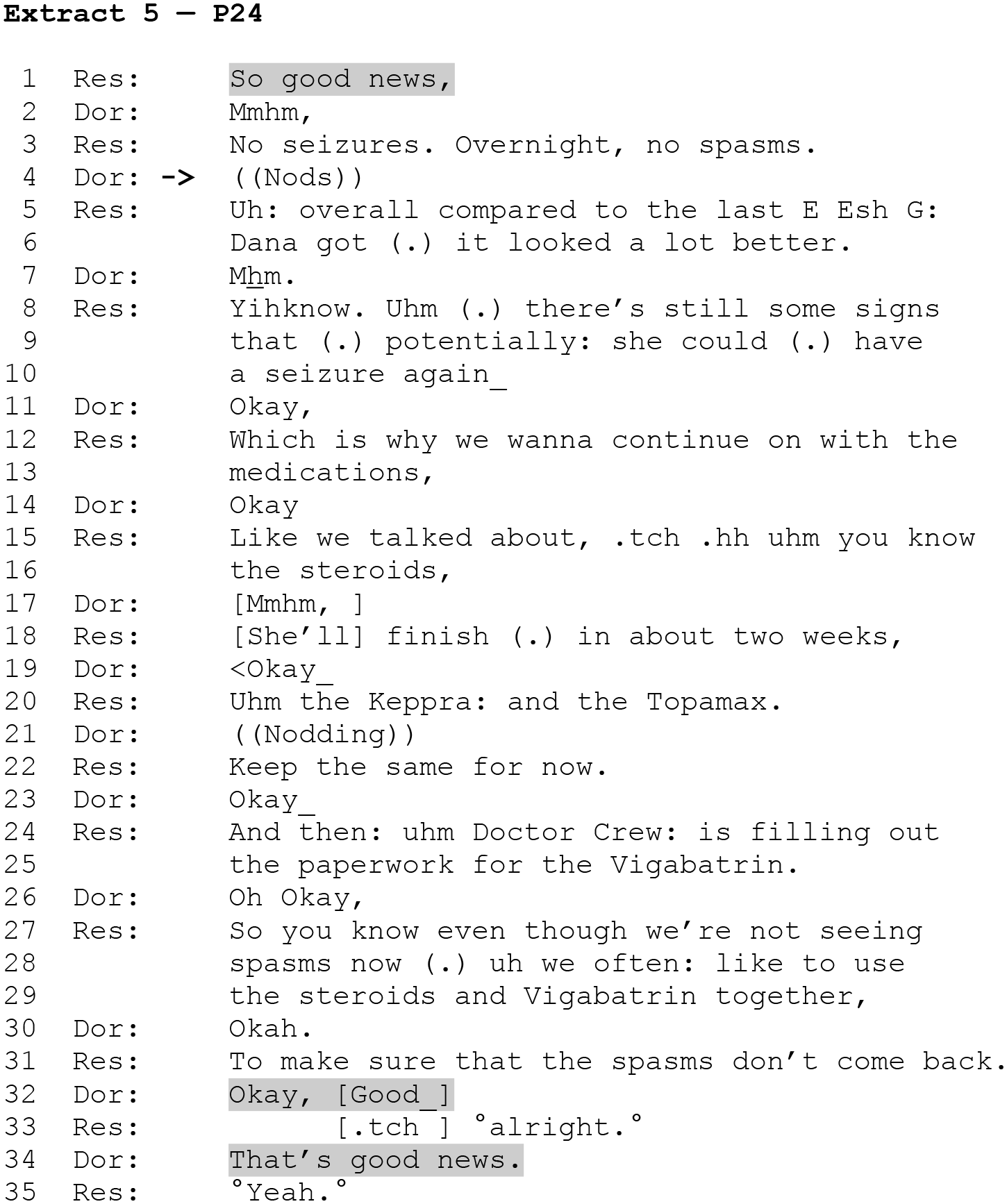
Extract 5 illustrates this. The patient is Dana, a six-month-old with a history of infantile spasms. Her grandmother, Doris, brought her in for this visit to assess the effects of a shunt that was surgically implanted to relieve pressure on her brain. During the admission interview, Dana’s mother was also present, and she conveyed concern about the medication regimen the neurology team implemented following Dana’s procedure. As I show, this turns out to have implications for the adequacy of the informing. Here, as with Extracts 3 and 4, the clinician begins with an evaluation of the news (line 1). And again, the recipient does not readily affiliate with the clinician’s stance. Rather, Doris responds with a “go-ahead” (Schegloff 2007:30) in the form of a continuer, “Mmhm,” (line 2), thereby treating the news delivery as incomplete (Heritage and McArthur 2019; Jefferson 1981; Schegloff 1982). The resident subsequently presents an informing—“No seizures. Overnight, no spasms.” (line 3). At this point, the resident has produced both components of the news delivery, yet Doris provides only minimal acknowledgement (line 4). In the absence of uptake from Doris, the resident renews the relevance of an assessment by invoking Dana’s prior EEG as a baseline for comparison with the present EEG, which he characterizes as “a lot better.” (line 6). Based on Extracts 3 and 4, we would expect affiliation to be forthcoming once the resident has characterized the news as good and has made the basis for his stance both available to Doris, in the first instance (line 3), and relative to Dana’s medical history subsequently (lines 5–6). Yet in producing a continuer and nothing more, Doris continues to treat the news delivery as incomplete (line 7).
At lines 8–10, the resident expands his informing to include a different dimension of the news, and as Doris acknowledges this (line 11), he goes on to recommend that Dana continue treatment (lines 12–13). Through his turn-initial “Which” (line 12), the resident designs this turn as an increment (Ford, Fox, and Thompson 2002; Schegloff 2016), thus “skip-tying” back to his prior utterance (see Sacks 1995:734) and leveraging it as an account for his recommendation.
Finally, having reviewed the treatment plan, the resident orients to uptake from Doris as still relevant yet absent, joining an item of news “So you know even though we’re not seeing spasms now” with the treatment plan “we often: like to use the steroids and Vigabatrin together,” (lines 27–29). In this context, “you know” serves to reinvoke the recipient’s support and thereby renews the relevance of affiliation (Clayman and Raymond 2021). When Doris offers only acknowledgment (line 30), the resident treats this as insufficient. By designing his next utterance as an increment (Ford et al. 2002; Schegloff 2016) of his prior turn (line 31), the resident sequentially deletes Doris’s acknowledgment (Jefferson 1978) and thereby renews the relevance of a response to his informing. Finally, after accepting the treatment recommendation (line 32), Doris produces an assessment—“That’s good news.” (line 34).
Thus far, I have shown that incremental elaboration of the news can engender uptake, but I have not yet considered how this works or why it was necessary in the first place. Based on my claim that parents withhold uptake of the news, usually in the form of an assessment, until the physician has presented both an informing and an evaluation, we would expect Doris to produce an assessment as early as line 4. Yet Doris continues to withhold uptake long after both components have been presented; and although we might have expected this to be a harbinger of disagreement, Doris ultimately does affiliate with the resident (line 34). What can account for her apparent reluctance to treat the news delivery as sufficient after the resident’s initial informing and evaluation? Recall that during the admission phase of the visit, Dana’s mother and grandmother were both present. At that time, Dana’s mother indicated that she was unhappy with the medication regimen implemented by the neurology team. In her view, the prescribed drug cocktail was excessive for a baby. Thus, here a key part of the news is that Dana will be able to stop taking some of the prescribed medications soon. This serves as the basis for a positive characterization of the news that Doris can endorse, and once the resident makes it available, she affiliates with him explicitly (line 34).
Extract 5 shows that the adequacy of the informing that underlies an evaluation is subject to negotiation and can be contingent on parents’ concerns about the child, which suggests that valence is morally accountable (Garfinkel 1967). This adds an additional analytic layer to my previous claim that for parents, both components of the news delivery are relevant, and they treat either component as absent until both are provided. Specifically, it shows us that parents do not treat just any informing as sufficient when paired with an evaluation but, rather, one that addresses their primary concerns (in this case, the treatment implications of the news). Thus, incremental elaborations of the news are successful insofar as they allow physicians and parents to jointly negotiate the adequacy of the informing and evaluation components underlying the dual imperatives of the news deliveries in this context. Parents can withhold uptake until the informing addresses their primary concern(s), and physicians can elaborate incrementally until parents orient to the news delivery as sufficiently complete.
Discussion
The present study contributes to the literature on news deliveries in the following ways: I showed that the knowledge and relational dimensions of news are embodied by dual imperatives—news should inform recipients, and the participants should affiliate. Moreover, I demonstrated that the affiliation imperative can become complicated in medical contexts, where relative rights to ascribe valence to news diverge from those observed in everyday life. Many everyday news deliveries are either “third-party” deliveries, where news is about a nonpresent party, or “first-party” deliveries, where deliverers offer news about themselves. Although “second-party” deliveries (i.e., when the deliverer informs a recipient of news that is consequential for the recipient) do happen in everyday life, they are comparatively infrequent (Maynard and Frankel 2006:251). Yet this is the primary form of news delivery in medical visits. This is significant because when the recipient of some news is its main consequential figure, then the recipient generally has more control over its negotiated valence (Maynard 2003:96, 113) and can claim primary rights to characterize the news by virtue of evaluating it first (Heritage and Raymond 2005). However, physicians have epistemic primacy over medical science (Heritage 2021). Consequently, if parents assess news first, they risk being heard as claiming epistemic primacy over matters that fall within the physician’s domain; and if physicians evaluate news first, they run the risk of engaging in “problematic presumptiveness” (Maynard 1997:119). Insofar as these could be face threatening for physicians and parents alike, both may be reluctant to assess news first. Yet when physicians delay or equivocate their evaluations, the resulting ambiguity may create a face-threatening “affiliation problem” (Stivers et al. 2022:1558) of its own, and efforts to resolve it can result in protracted news deliveries.
What, then, explains parents’ reluctance to receive news as good once physicians indicate that it is good but before they have produced an informing? Without a clear basis for their assessment, parents’ evaluations risk being heard as affiliating for the sake of affiliation rather than as affiliation resulting from the congruence of independently held positions (i.e., “genuine” affiliation). Although parents may lack the epistemic basis to agree with physicians on the nature of the news being delivered, they can affiliate with the news independently if and only if they have sufficient access to the information underlying the physician’s evaluation.
Although the informing and evaluation components can be delivered in either order, their relative positioning clearly has implications for parent uptake. In this regard, there are advantages to valence-first news deliveries. First, because bad news is typically delivered without explicit orientation to the news as bad, good news runs the risk of being heard as bad when it is delivered without valence. Although there are interactional resources, such as prosody, that participants can deploy to display an orientation toward the news without characterizing its valence explicitly (Freese and Maynard 1998), these may not be sufficient for parents to risk encroaching on medical authority with a first assessment. Valence headlines, in contrast, appear to facilitate the smooth delivery and reception of news as they make it easier for parents to mitigate face-threatening actions, such as explicit disagreement, while also cashing in on the affiliation potential that assessments offer.
However, if early evaluations have these apparent advantages, then what accounts for delayed good news evaluations, or those that are cautious in general? I have shown that physicians tend to mitigate and/or delay (but still provide) positive evaluations of news that is not exclusively good (e.g., Extracts 1–2) or when an early unmitigated positive evaluation of the news might conflict with recommendations to maintain medications that parents are opposed to (i.e., the news is good from a clinical perspective but not necessarily in line with parents’ hopes, as in Extract 5). Together, these observations suggest that the position of clinicians’ evaluations may be “strategic” in light of their overall sense of the case as a whole.
Contrary to common perceptions of good news as unproblematic, I have shown that trouble can arise while negotiating what the news is and how it should be taken. Of course, some of this difficulty can be attributed to clinical uncertainty—unlike HIV tests, which are typically reduced to either HIV positive or HIV negative outcomes, vEEG results are complex and somewhat subjective (Hussain et al. 2015). However, I have argued that in addition to this, there are structural features of news that make it difficult in pediatric neurology.
Limitations
This study is based on a limited collection of news deliveries in one specialty clinic, so results may not generalize to other clinics. Moreover, this study deals exclusively with the delivery and reception of good news and thus provides only a partial picture of news deliveries in this context. Future research on a larger and more diverse corpus of data will be necessary to assess the robustness of these findings.
Footnotes
Acknowledgements
I would like to thank John Heritage, Giovanni Rossi, Stefan Timmermans, and Andrew Chalfoun for comments throughout the development of this article. I am particularly indebted to Tanya Stivers for her guidance and support throughout this project.
1
Parents were first to characterize the valence of the news in just 24 percent of cases (n = 4).