
Abstract
Islamophobia is a global problem that has reached epidemic proportions according to recent government reports and international research. In this preregistered, randomized control study, conducted in a field setting in Australia (N = 227), we investigated whether Islamophobia—negative and hostile attitudes toward Islam and Muslim people—was reduced by a short door-to-door canvassing intervention. Our study involved participants who had expressed negative or ambivalent attitudes toward Muslim residents in a previous survey. These participants were randomly assigned to receive either no treatment or a 15-minute door-knocking conversation that encouraged empathy building through (1) active processing of new information and (2) perspective taking through personal reflections on past experiences of exclusion. Follow-up surveys suggest that, compared with a baseline survey completed before the intervention, prejudice was significantly reduced in the treatment group 6 and 12 weeks later.
Xenophobia is a complex, socially constructed phenomenon that varies by context. Evidence suggests that positive interaction between ingroups and outgroups can improve relations, although such contact does not often happen organically in social situations due to homophily (Ladegaard 2018), race- and class-based segregation patterns (Allport 1954; Pettigrew 1998), and intergroup anxiety (Islam and Hewstone 1993; Stephan and Stephan 1985). Some scholars suggest that xenophobia will naturally decrease over time, even without intervention, as immigration streams and urban population concentration increase acceptance by bringing people together (Jolly and DiGiusto 2014) through settings such as diverse workplaces (Lamont and Aksartova 2002) and schools (Bekhuis, Ruiter, and Coenders 2013). However, the prominence of anti-immigrant rhetoric in contemporary politics in places like Germany, France, and the United Kingdom suggests that increases in immigration and the visible presence of minorities will continue to be framed as threatening (Golder 2003; Inglehart and Norris 2016; Thränhardt 1995). This is also the case in Australia, where this research is situated.
Reducing xenophobia is a task at the center of the social science literature on multiculturalism in majority-Christian countries such as the United States, United Kingdom, and Australia. Research interest has burgeoned in response to the global resurgence of populist politics (Berman 2021; Inglehart and Norris 2016; Urbinati 2019) and growing anti-immigrant sentiment (Ceobanu and Escandell 2010). Further, empowered far-right movements (Muis and Immerzeel 2017), hate crime and extremist violence (Klein, Gruenewald, and Smith 2017), and political events such as the United Kingdom’s exit from the European Union and the presidential election of Donald J. Trump, which were widely interpreted as electoral backlashes against globalization (Bhambra 2017; Inglehart and Norris 2016), have also played a role. This scholarship suggests that to prevent such divisions, it is critical to generate social cohesion among those who are racially or ethnically different from each other. Yet, countries that aspire to build diverse societies ascribe a minority status to migrants (Benier et al. 2018; Benier and Wickes 2016; Marshall 1997). Whether migrants can then successfully integrate depends in large part on the majority’s beliefs, attitudes, and opinions and the social and political forces that shape them.
The Harms of Islamophobia
One of the most frequent expressions of xenophobia are anti-Muslim sentiments, with Islamophobic incidents becoming more violent and bold in recent years (Iner 2019; Poynting and Mason 2007; Zempi and Awan 2016). While there is some debate around the scope of incidents included in definitions, Islamophobia can be broadly defined as the unfavorable treatment of Muslim people through negative and hostile attitudes as well as verbal and physical abuse that denigrates the Muslim identity (Abdel-Fattah 2017; Aslan 2009; Hassan and Martin 2015; Iner 2019). Islamophobia is not a new concept, but Islamophobic incidents significantly increased after September 11, 2001, with empirical evidence suggesting an 82 percent increase in implicit and indirect bias and a 75 percent increase in overt discrimination toward those of Muslim appearance/background in the aftermath of that date (Sheridan 2006). Furthermore, mosques were subjected to vandalism, graffiti, arson, and bomb attacks (Abu-Raiya, Pargament, and Mahoney 2011; Al Atom 2014; Barkdull et al. 2011). Since then, the social and economic exclusion of Muslim citizens has remained high in many countries—in part due to the continuing stereotyping between Islam and terrorism. At the national level, Islamophobia is evidenced in the speeches of political leaders who routinely make statements about cultural, religious and terroristic “threats” posed by “all Muslims” with disregard for the heterogeneity of individuals within this label (Chalmers and Robertson 2021; Jamal 2017; Murphy 2017; Pettersson 2019). Globally, the media represents the Muslim faith negatively and portrays Islam as a violent religion (Ahmed and Matthes 2017). This has led to endemic marginalization of Muslims (United Nations Secretary General 2021).
The consequences of Islamophobia are dire. Prejudice, bias, and discrimination create an array of negative outcomes for society. In extreme forms, hate has resulted in mass shooting events, such as the terror incidents in Christchurch, Quebec City, and Marseilles mosques, and the Finsbury Park van attack in the United Kingdom (Besley and Peters 2020; Macklin 2019; Mahrouse 2018; Roy 2013). Social exclusion arguably has the most sustained impact on daily lives (Jenkins 2018). At the localized level, Islamophobia manifests as a form of hate crime that targets individuals and communities through verbal and physical abuse and intimidation. Emerging research into the experiences of Muslim Australians from the Australian Human Rights Commission (2021) details that almost 80 percent of participants have faced unfavorable treatment and discrimination within society. These statistics highlight the prevalence of negative attitudes, which have detrimental consequences for belonging and social inclusion in the community (Benier 2019). They also curtail the right to freedom of religion for Muslim people (Australian Human Rights Commission 2021), which has severe consequences for democratic societies.
Shifting Islamophobic Attitudes
It is notoriously difficult to change attitudes toward stigmatized groups (Batson et al. 1997). Efforts to reduce prejudice with diversity training and media campaigns have thus far yielded inconclusive results, and it remains unclear how, exactly, prejudice against Muslims and other ethnic minorities can be reduced (Hsieh, Faulkner, and Wickes 2022; Paluck et al. 2021; Paluck and Green 2009). Outside of psychology labs, few prejudice-reduction studies have involved randomized control groups. A notable exception is a field trial study by Broockman and Kalla (2016), which found that canvassing can change transphobic attitudes. The authors used techniques of active processing (“active consideration of counter-prejudicial thoughts”, Broockman and Kalla (2016: 220)) and perspective taking (“imagining the world from another’s vantage point”, Broockman and Kalla (2016: 220)) in their conversations to increase acceptance of transgender people. Yet their study notes that their participants may have been unfamiliar with definitions of transgender and therefore may not have had strong opinions on the issue.
We specifically targeted older people with negative or ambivalent feelings of warmth toward Muslim residents. Older populations have established opinions that are deeply ingrained and resistant to change (Paluck and Green 2009; Scacco and Warren 2018). We conducted a randomized control field trial to establish whether a one-off, scripted door-to-door visit can produce lasting empathy and therefore reduce prejudice against a highly targeted ethnoracial group. Central to the study was whether canvassing could be a useful approach for those members of the community who may be less inclined to change their perspective. Scalability and reliability were key goals of our study as prejudice-reduction interventions often do not consider scalability (Hsieh et al. 2022), despite it being critical to in turn deliver the intervention to large populations.
Our intervention took place in Melbourne, Australia, where Islamophobia is a growing concern (Abdel-Fattah 2017; Aslan 2009). Melbourne was selected as a research site for studying prejudice reduction in multicultural societies as its foreign-born population is among the largest in the world and is in proportion to other global cities, such as London, Vancouver, and New York (Price and Benton-Short 2007). Moreover, Australia is considered an immigration destination—similar to countries such as the United States, Canada, and New Zealand—with the integration of foreigners being central to its social and economic policy goals (Koopmans 2013).
Cognitive and Emotional Empathy
We examine participants’ levels of cognitive and emotional empathy toward Muslim Australians before and after a home visit. Empathic concern has a well-documented role in eliciting prosocial behavior (Batson 2012; Forgiarini, Gallucci, and Maravita 2011), and it has been researched in the psychological literature for decades (Decety and Yoder 2016). Empathy, defined as a sensitivity to, and understanding of, the mental states of others, is vital for humans to navigate their social environment and to understand others’ intentions, actions, and behaviors (Forgiarini et al. 2011). It has been categorized into two constructs: cognitive empathy and emotional empathy (Smith 2006).
Emotional empathy refers to the ability to respond with an appropriate emotion to another’s mental state (Khanjani et al. 2015), or the vicarious sharing of emotion (Smith 2006). Research demonstrates that emotional empathy is impacted by implicit racial biases. For example, evidence from Forgiarini et al. (2011) documents that their white participants recorded a stronger empathetic physical reaction to a white individual experiencing pain than to an Asian or African individual. Similarly, Brown, Bradley, and Lang (2006) found increased empathetic reactions toward ethnic ingroup members compared with outgroups, proposed to be a result of group identification and personal relevance. We contacted participants who had previously recorded low feelings of warmth toward Muslim Australians in a prior survey and, therefore, likely had low emotional empathy toward the group.
Cognitive empathy is the ability to identify another’s mental state (Khanjani et al. 2015), and thus, perspective taking increases cognitive empathy. Perspective taking is the ability to consciously put oneself into the mind of another person to understand their thoughts or feelings (Decety and Yoder 2016; Lamm, Batson, and Decety 2007; Vescio, Sechrist, and Paolucci 2003). Indeed, perspective taking has been shown to reduce bias toward a range of stigmatized groups and to inhibit the activation of subconscious prejudices (Van Ryn et al. 2011). Batson et al. (1997) propose this shift to be the result of a three-step process. First, perspective taking of a member of a stigmatized group leads to increased empathy toward that person. Second, this empathy leads to an increased perceived value of their welfare. Third, the value should, by association, supersede barriers and increase positive feelings toward the whole group. We determined that it was essential to include perspective taking in our intervention strategy, as evidence suggests that cognitive empathy is reduced in older adults (Bailey, Henry, and Von Hippel 2008; Khanjani et al. 2015), such as our participants. Next, we detail our research methods and then discuss our findings.
Method
Study Design
We used a two-arm randomized controlled trial design to test the effect of a door-to-door canvassing intervention on prejudice against Muslims, cognitive perspective taking (i.e., the extent to which people think about what it is like for Muslims), and emotional empathy (i.e., the extent to which people feel compassionate and empathic emotions toward Muslims). 1
We first contacted people who had reported low or ambivalent feelings of warmth toward Muslim residents in an earlier study on community perceptions and safety in Melbourne, Australia, and invited them to partake in further research. 2 Those who agreed were first asked about their attitudes and sentiments regarding Muslim immigrants in a baseline survey. Respondents were randomly assigned to either an intervention condition or a no-treatment control condition. Respondents in the intervention group were visited, in their homes, by a pair of canvassers who were trained to hold a short, structured discussion about Muslim people in Australia. The goal was to get participants to think about the issue (active processing) and use their personal experiences to imagine what it is like for Muslim people in Australia (analogic perspective taking; Broockman and Kalla 2016). These mediators are known to stimulate cognitive and emotional engagement with the issue at hand, which can in turn build empathy and reduce prejudice (Gardiner 1972; Schaller et al. 1996; Vescio et al. 2003). Participants assigned to the control condition received no intervention and had no social interaction at all; they were only asked to complete the surveys used to measure the outcomes just noted. Measures were collected on three occasions: a baseline before intervention delivery (Time 1 [T1]), 6 weeks postintervention (Time 2 [T2]), and 12 weeks postintervention (Time 3 [T3]).
Surveys
We sent an introductory letter and then the baseline survey to 694 participants from an earlier study (Wickes et al. 2020) who reported that they had negative or ambivalent feelings toward Muslim residents. We explained that our new study would include surveys about social inclusion in their community and possibly a home visit. A total of 327 participants completed and returned the baseline survey (see Figure 1 for a flowchart). These were randomly allocated into two groups: one that received no treatment and one that received home visits. In total, 74 homes received the intervention. A further 68 residents were not home on either of our two attempts, 5 residents were home but refused participation, 18 were not visited in time for our study’s completion, and a further 2 withdrew from the study altogether. Six weeks after the intervention period, we sent the first follow-up survey to 339 participants who had returned the baseline survey, of which 209 were completed. Another 6 weeks later—12 weeks after the intervention period— we sent a second follow-up survey to all participants who received the baseline survey and had not since opted out. At this stage, we received 218 completed surveys. The three surveys included measures of prejudice, cognitive empathy, emotional empathy, and filler questions.
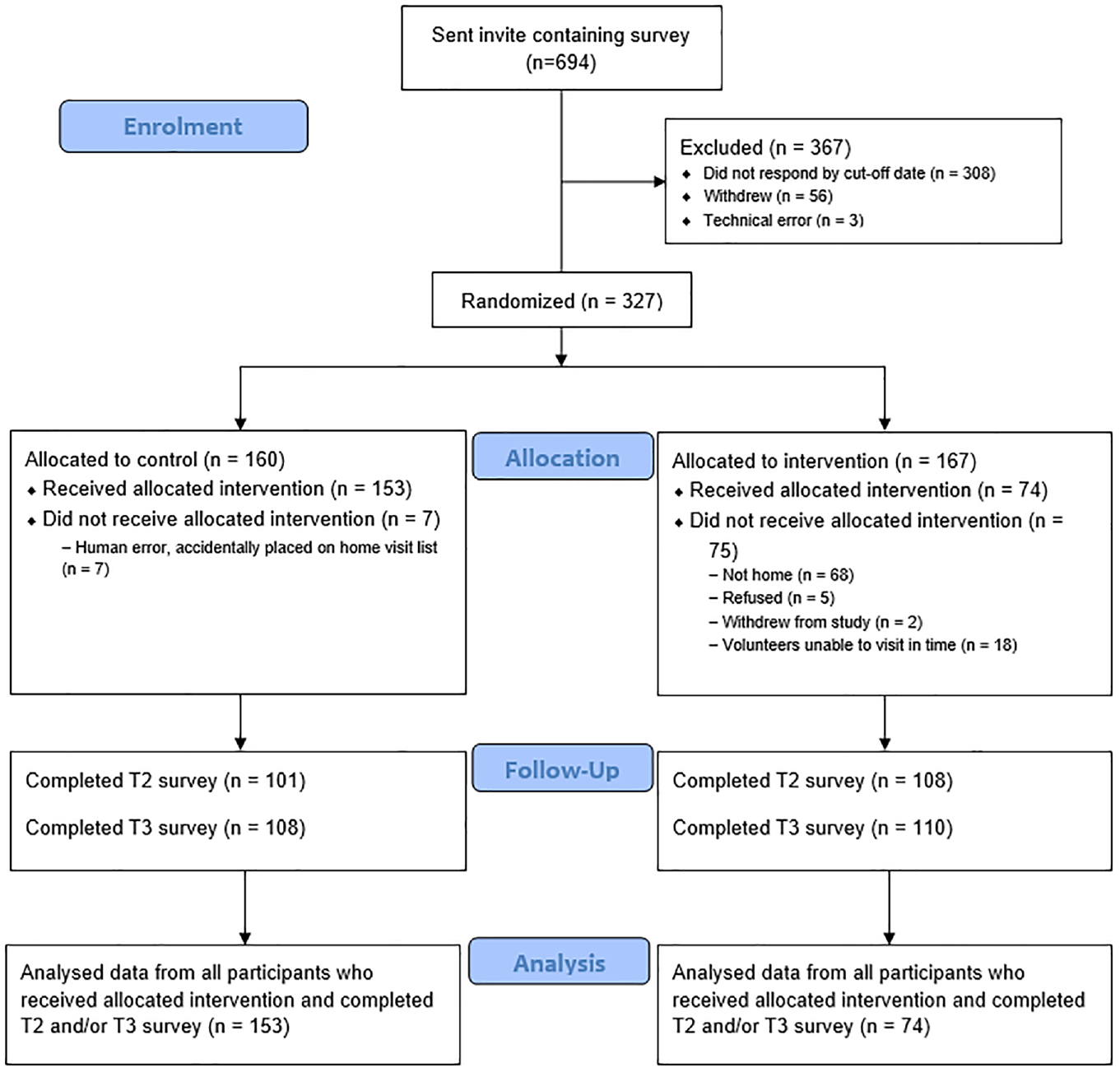
Participant Flow Diagram
Measures of Prejudice, Cognitive Empathy, and Emotional Empathy
We measured prejudice against Muslim residents using seven items from the Blatant and Subtle Prejudice Scale (Pettigrew and Meertens 1995). Example items included “Non-Muslims and Muslims can never really be comfortable with each other, even if they are close friends” and “I would not mind if a suitably qualified Muslim person was appointed as my boss.” We collected responses on a 5-point scale ranging from 1 = strongly disagree to 5 = strongly agree. Items were also reversed where appropriate and averaged to form a reliable composite scale, αT1 = .86.
Cognitive perspective taking was measured using the Intergroup Perspective-Taking Scale (Hodson, Choma, and Costello 2009; e.g., “I can easily imagine a day in the life of a Muslim person”). Responses to each item were collected on a 5-point scale ranging from 1 = strongly disagree to 5 = strongly agree. We collected five items but dropped two of these items due to low reliability. The remaining three items were averaged to form a reliable composite scale, αT1 = .75.
Emotional empathy was measured using Batson et al.’s (1997) Empathy Scale. This scale asks participants to report the extent to which they feel a series of emotions toward Muslims (from 1 = not at all to 7 = extremely). Responses to the following six items were averaged to form a composite measure of emotional empathy: sympathetic, compassionate, soft-hearted, warm, tender, and moved, αT1 = .86.
Analysis
We prospectively registered the trial before data collection began (see https://osf.io/n6tp8). This preregistration detailed the method and analytic approach prior to completing data collection. Using GLIMMPSE software (Kreidler et al. 2013), we initially estimated that a sample size of 266 would provide 80 percent power to detect a 0.3 mean difference between the intervention and control conditions in one-month outcomes, controlling for baseline outcomes (on a scale with a standard deviation equal to 1 and assuming equal sample sizes in the treatment and control groups, an r = .6 correlation between T1 and T2 responses, and a two-sided p < .05 significance level). Our data collection was halted by the COVID-19 pandemic, yet as indicated in the results, we identified significant change with the final sample (n = 227).
We assessed the direct effects of the intervention at 6 (T2) and 12 (T3) weeks postintervention using a series of linear regression models. To assess the effects at 6 weeks, we computed models for each outcome that used the outcome at 6 weeks as the dependent variable and used baseline outcome score and experimental condition (0 = no intervention, 1 = intervention) as the independent variables. The coefficient for condition indicated the effect of the intervention. To assess the effects at 12 weeks, we employed the same approach but used the 12-week outcomes instead of the 6-week outcomes as the dependent variable. For example, the effect of the intervention on prejudice at 12 weeks postintervention was assessed using prejudice at 12 weeks as the dependent variable and baseline prejudice and experimental condition as the independent variables. Cohen’s d effect size measures were calculated using techniques appropriate for trials using a two-independent-groups pretest and posttest design (Feingold 2013). To examine whether the effects of the intervention on prejudice were mediated by cognitive perspective taking or emotional empathy, we used path analysis. The results of these analyses are presented in the following sections.
Volunteer Training
Door-to-door canvassing was conducted by volunteer graduate students. We recruited 15 volunteers by circulating advertisements for the study on university newsletters and social media channels. Volunteers worked in pairs and covered 10 to 18 houses each, depending on their proximity. All volunteers were paid an AUD$150 honorarium at the end of the project to cover travel expenses and incidentals. While we did not record the religion of the volunteers (and note this as a limitation in the discussion that follows), students were primarily recruited through the Monash Migration and Inclusion Centre, and most were of an Asian or Middle Eastern background. There were 11 female and 4 male recruits, and the majority were between 25 and 35 years old.
Volunteer training had three steps. First, we discussed the project’s intellectual and social merits and our individual responsibility for its integrity and value. Second, we detailed why it was important to facilitate a conversation with participants that was friendly, nonjudgmental, engaging, and organized without seeming inauthentic. We accomplished this by writing a script based on the script used in Broockman and Kalla (2016). Third, we conducted several canvassing role-play exercises in order to train participants to be friendly and respectful while sticking to the script and also to probe participants for their own reflections, all while sticking to the allotted time of 15 minutes per visit. We also prepared and distributed training material: a videotaped role-play; a volunteer handbook detailing all steps, including safety precautions; and an overview of the study’s conceptual framework.
Intervention
Participants in the intervention group engaged with canvassers on their doorsteps and in their homes in a semistructured 15-minute conversation about Muslim immigration. First, volunteers told residents that politicians have talked about reducing Muslim immigration and that they might be asked to vote on this issue in a potential referendum. Canvassers probed for participants’ stance on a hypothetical ban on Muslim immigration and inquired about their concerns and existing views on Muslim immigration. This approach is believed to encourage active processing of information about the topic (Petty, Cacioppo, and Schumann 1983). Second, participants were shown a video clip from a debate between a white Australian woman and a Muslim Australian woman who discussed issues of terrorism and fears of their families’ safety in an attack and, in the case of the Muslim Australian woman, a backlash against minorities. Participants were asked to share their reactions to the video and reflect on any resulting uncertainties. We determined that using a video was effective for our study purposes because showing an image of an outgroup member is an entry point for perspective taking (Todd and Galinsky 2014). Third, participants were asked to describe if they had ever felt the kind of negative judgment or stigma that the Muslim woman in the video felt. At this point, canvassers would often, in accordance with their training, tell a personal story of facing judgment and discrimination to make participants feel comfortable sharing a story of their own. The purpose of this step was to prompt analogic perspective-taking (Gehlbach and Brinkworth 2012). The intervention ended by encouraging reflections (active processing) on the value of taking Muslim Australians’ perspective and if and why the conversation had changed their attitudes toward the group. This final step was included because rehearsal of opinion change can facilitate active processing and increase the persistence of attitude changes (Petty and Cacioppo 1986), if any. We note that there is a selection effect present, as not everyone who was allocated to the door-knocking condition answered the door.
Six and 12 weeks after the intervention period, we sent two additional surveys to the control and treatment groups. Next, we compared differences in prejudice between the control and intervention groups in the completed surveys at both time points, controlling for baseline scores.
Transparency and Openness
The study design and analysis were preregistered. We report how we determined our sample size, all manipulations, and all measures in the study. While the final sample size was slightly smaller than the preregistered figures, calculations show that there were no issues with statistical power. We also specified data exclusions. Data analyses were performed using the lm and lavaan packages (version 0.7) in R Studio (version 1.3.1093). All code and research materials are available for purposes of verification or reanalysis upon request.
Results
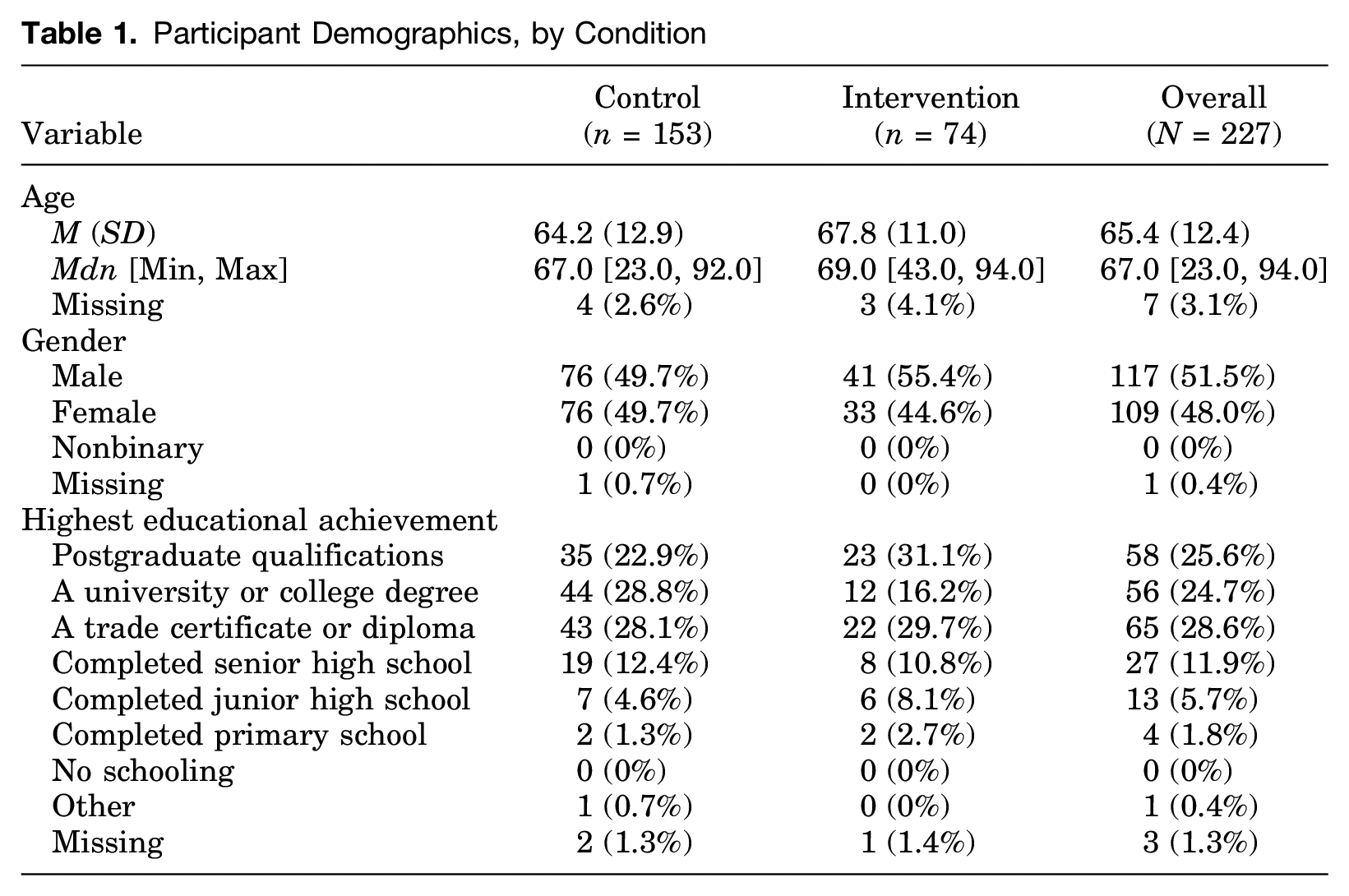
The intervention took place in Melbourne, Australia, where we evaluated the impact of an empathy-building conversation on prejudice against Muslim Australians. The project involved a baseline survey, and two follow-up surveys were issued at 6 and 12 weeks after the home visit period. A total of 227 participants received their allocated treatment or nontreatment, responded to the baseline survey, and also completed at least one of the two follow-up surveys. Of these, 117 (51.5 percent) were male, and 109 (48.0 percent) were female. Participants had a mean age of 65.4 years (SD = 12.4). As shown in Table 1, demographic profiles were similar in both conditions. Supplementary Table 1 further shows that the demographic profiles and baseline levels of prejudice were also similar among participants who were assigned to the intervention condition but did not receive it for the reasons listed in Figure 1.
Participant Demographics, by Condition
Regression findings showed that the conversations significantly reduced prejudice 6 weeks after the intervention (d = .27, 95 percent confidence interval [CI] [.10, .44]). Those reductions remained present after 12 weeks (d = .18, 95 percent CI [.01, .36]) (Table 2). To contextualize the strength of these effects, consider a feeling thermometer scale in which participants rate how they feel toward Muslim people on a scale from 0 (cold) to 100 (warm). An effect of d = .27 implies that individuals who rated Muslim people as 45 (slightly negative) before the intervention would, on average, rate them as 52 (slightly positive) 6 weeks after the intervention (using the standard deviation of 24.64 reported in the American National Election Study [ANES] 2021) question on feelings toward Muslims). To place this in historical perspective, feelings toward Muslims among ANES respondents improved by 4.5 points between 2004 (the first-time feelings were measured by the ANES during the peak of the wars in Afghanistan and Iraq) and 2020 (ANES 2005, 2021). The effect of the intervention was 1.48 times that magnitude. Differences in means and distributions of outcomes in each condition are presented in Figures 2 and 3. As a robustness check, we also conducted intention-to-treat analyses that included all participants who responded to postintervention surveys (even those where participants were not home or did not answer when canvassers visited). These analyses showed an identical pattern of results, with a significant reduction in prejudice evident at both postintervention time points (see Supplementary Table 2).
Regression Outputs Showing Intervention Effects on Time 2 (T2) and Time 3 (T3) Outcomes, Controlling for Time 1 (T1) Scores
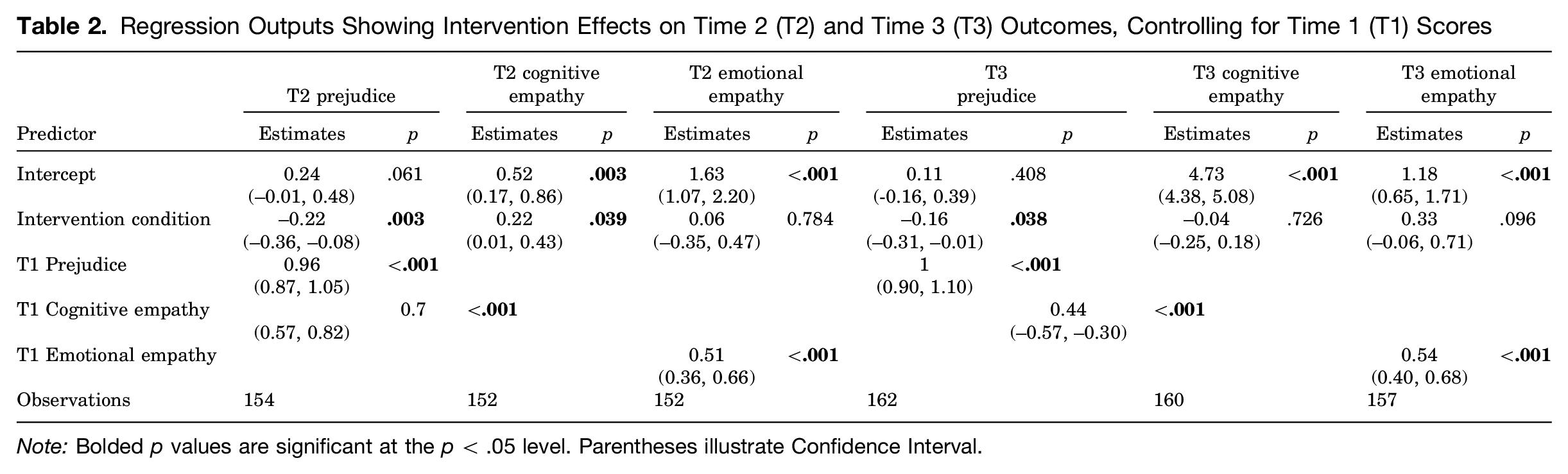
Note: Bolded p values are significant at the p < .05 level. Parentheses illustrate Confidence Interval.
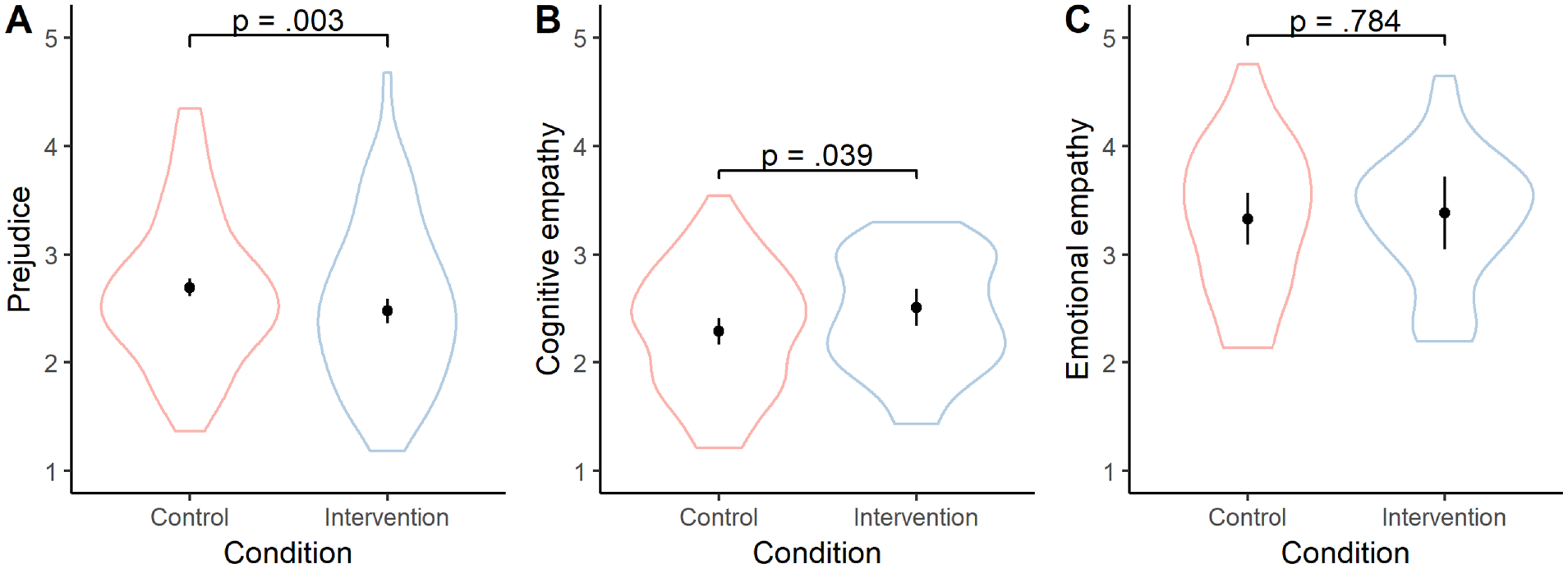
Marginal Means and Distributions of Time 2 Outcomes, Controlling for Time 1 Scores
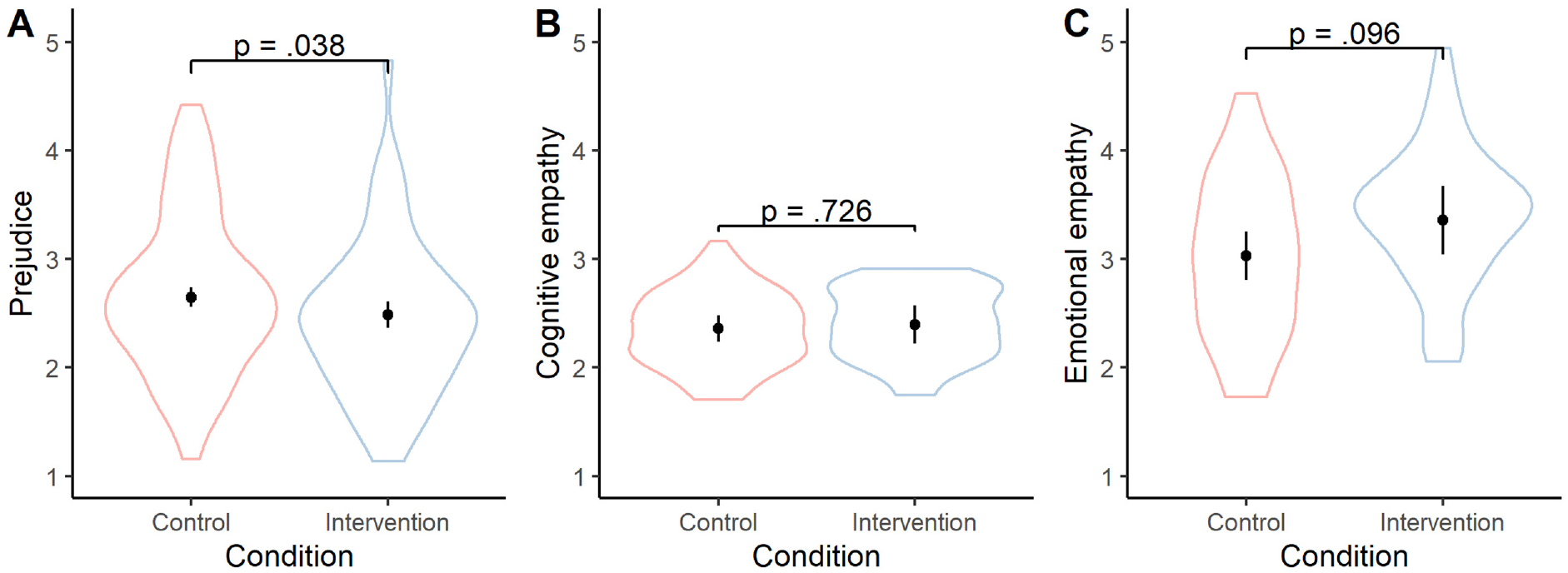
Marginal Means and Distributions of Time 3 Outcomes, Controlling for Time 1 Scores
As noted earlier, we aimed to cultivate empathy and reduce prejudice through cognitive (active processing of new information) and emotional (perspective taking) mediators. We found that cognitive empathy was significantly higher in the intervention group 6 weeks after the intervention period (d = .27, 95 percent CI [.01, .53]). However, there was no significant difference between conditions in cognitive empathy 12 weeks after the intervention (d = .05, 95 percent CI [−.35, .24]). Emotional empathy did not significantly differ between the treatment and control conditions at either 6 (d = .04, 95 percent CI [−.26, .34]) or 12 (d = .05, 95 percent CI [−.35, .24]) weeks after the intervention period. Path analyses further indicated that neither cognitive empathy (specific indirect effect = .001, SE = .013, p = .965) nor emotional empathy (specific indirect effect = −.001, SE = .003, p = .833) mediated the effect of the intervention on prejudice. These results are presented in Figure 4. This is an interesting finding, and we recommend future research to determine the possible mediating factors that may be significant—for example, compassionate empathy is linked to emotional and cognitive empathy and may be related.
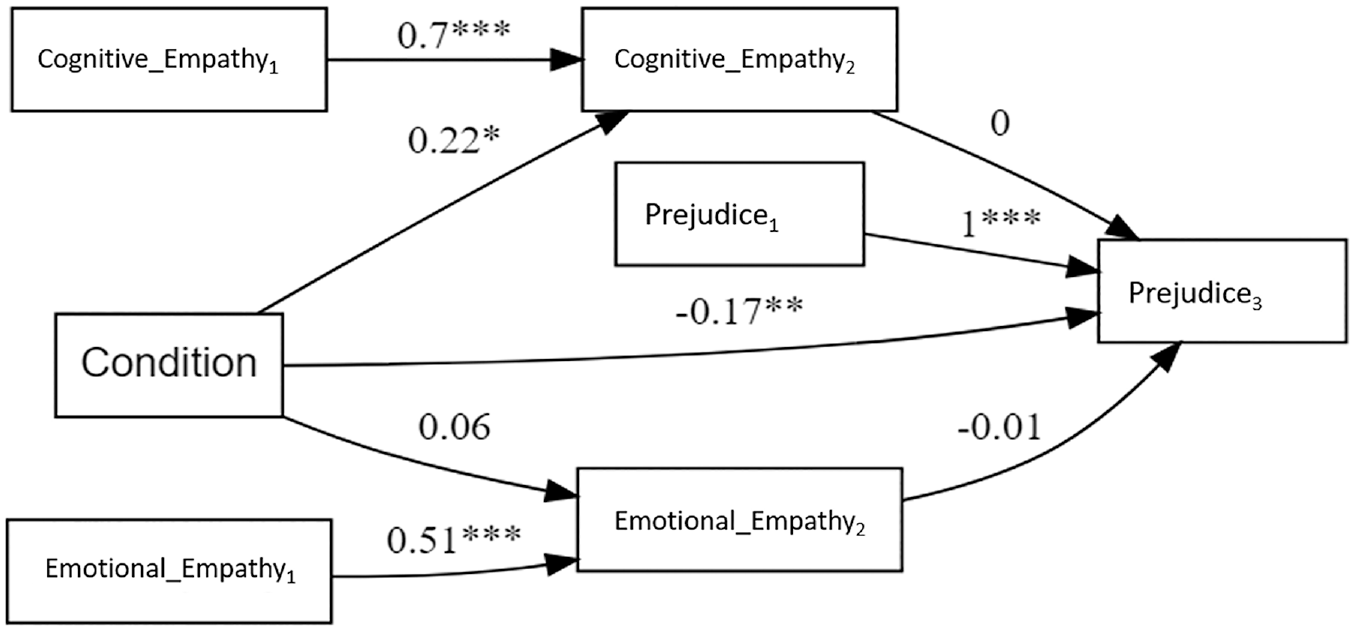
Longitudinal Mediation Model
Discussion
Scholars, governments, and organizations have been searching for strategies to improve social cohesion within the community. Under the principles of the contact hypothesis (Allport 1954), it is well established that prejudice against minority-group members can be reduced with intergroup contact, but practical solutions to arrange this contact are often difficult to facilitate and require those with low feelings of warmth to establish interactions with those of whom they are wary—a scenario that is unlikely to naturally occur. Our intervention is one potential solution.
Our central finding is that by creating conditions for dialogue, we can, under certain circumstances, reduce prejudice against Muslims and Muslim immigrants. Our control and treatment groups scored similarly on the baseline survey, but they diverged in our two follow-up questionnaires after the intervention was delivered. Compared with the controls, people who participated in scripted 15-minute conversations about Muslim immigration scored notably lower on measures of prejudice. Thus, although research shows that attitudes toward ethnic minorities are highly entrenched, our study demonstrates that it is possible to encourage viable conditions for change.
The importance of these findings is threefold: First, there are very few studies of prejudice-reduction interventions that focus on Islamophobia while also meeting the highest scientific standards—utilizing a randomized control group—for making claims about causality in the real world (Paluck and Green 2009). Second, anti-immigrant sentiments are on the rise across the West and are particularly strong in nations in which Muslims make up a large proportion of immigrants (Koopmans 2013). Islamophobia is unlikely to decrease by itself, especially as contemporary populists draw on Islamophobic frames to build support (Berman 2021). This suggests that prejudice-reducing interventions are critically needed. Third, this intervention was effective in reducing prejudice for individuals who are uneasy about Muslim immigrants. Given this group of people are also those most likely to be targeted and recruited by populist politics and right-wing movements (Blee and Creasap 2010), identifying strategies that prevent unease and the development of harmful sentiments toward others is crucial.
Despite the significant contributions of our research to the literature, we do note a few limitations. First, we were not able to facilitate a canvassing interaction in the control condition due to time and financial constraints. The analyses demonstrate a robust effect of the treatment when no parallel conversation was held. However, because the control and treatment groups differ in that only the latter was exposed to a human interaction with the volunteers, we cannot rule out the possibility that treated participants may have been more likely to express socially desirable answers in the follow-up surveys for fear of being seen as prejudiced. Future research could use a placebo-type control group to rule out this possibility. Second, it was proposed that the effectiveness of the intervention may be dependent on the specific volunteers who door knocked. To ensure that there was minimal door-knocking bias, we ensured that partnerships were rearranged several times throughout the project so that different individuals were working together on different days. Third, in the canvassing discussion, we used a video with a Muslim woman to foster relational empathy as evidence shows that women are more likely than men to be subjected to verbal and physical acts of Islamophobia (see, e.g., Elsheikh and Sisemore 2021). The intervention could be less effective with a video conversation between men. We propose that a larger, future study consider intersectionality effects, perhaps by including different conversation-starter videos.
The primary goal of our study was to develop an effective and scalable way to reduce Islamophobia. Our findings suggest that canvassing is one option that is low risk, is low cost, and can be done in the comfort of the participant’s own home. We spent considerable time developing an intervention that was theoretically grounded, practically feasible, and locally adjusted, but the volunteer training was straightforward, typically involving one to three hours of discussion and role-playing per group, and our canvassers had no major issues with facilitating the scripted conversation. Moreover, several nongovernmental organizations are already experienced door-to-door campaigners and could prove resourceful collaborators. Considering the vast resources that governments invest in efforts to promote inclusion (e.g., the budget for the European structural and investment is ?450 billion; European Commission 2020), large-scale interventions may be both feasible and worthwhile.
A secondary goal of our study was to examine the underlying mechanisms that explain how short discussions can reduce prejudice. We hypothesized that two mediators discussed but not formally tested by Broockman and Kalla (2016)—cognitive empathy through information processing, and emotional empathy through perspective taking—explain these effects. Here, our results are inconclusive. Although our measure of cognitive empathy was significantly higher in the treatment group 6 weeks after the intervention period, this difference was not significant after 12 weeks. Moreover, emotional empathy did not significantly differ between conditions at either time point. Results from our path analysis indicated that there were no significant specific indirect effects involved, suggesting that neither cognitive nor emotional empathy mediated the effect of the intervention on prejudice. We are thus unable to explain which mediator contributed to reduced prejudice. There may be additional mediators at work that were not measured here. It is our hope that future research will investigate which causal mechanisms are at play.
Conclusion
The purpose of our study was to develop a scalable, reliable method of reducing prejudice and xenophobia against Muslim people. In multicultural cities like Melbourne, developing strategies to reduce prejudice is vital to encourage social cohesion in neighborhoods that are fragmented by difference, diversity, and inequality. Our results indicate that a simple, structured conversation temporarily increased cognitive empathy toward a minority group and significantly reduced prejudice to lasting effect.
We call for scholars to expand upon our findings, just like we built on Broockman and Kalla (2016). In particular, we encourage scholars to advance our intervention approach using larger samples and to identify the causal mechanisms that lead to attitude change. In immigration destinations such as the United States, Canada, and New Zealand, where the integration of foreigners is central to social and economic policy goals (Koopmans 2013), funding agencies should support the development and implementation of effective prejudice-reducing strategies like the one we have outlined and tested here.
Supplemental Material
sj-docx-1-spq-10.1177_01902725231217246 – Supplemental material for Reducing Islamophobia through Conversation: A Randomized Control Trial
Supplemental material, sj-docx-1-spq-10.1177_01902725231217246 for Reducing Islamophobia through Conversation: A Randomized Control Trial by Kathryn Benier, Nicholas Faulkner, Isak Ladegaard and Rebecca Wickes in Social Psychology Quarterly
Footnotes
Acknowledgements
We thank the Victorian Government’s Department of Justice and Community Safety grants for funding this project. We also thank the editors and reviewers for their comments and Dr. Claire Moran for research assistance during the project’s fieldwork. We also thank the canvassers for their participation.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available as the participants of this study did not give written consent for their data to be shared publicly.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was funded by the Victorian Government's Department of Justice and Community Safety grants.
Supplemental Material
Supplemental material for this article is available with the online version of the article.
1
Ethics approval was granted by Monash University Human Research Ethics Committee (approval no. 21644).
2
Bios
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.