
Abstract
The increased use of advanced technologies generating new data and information, including algorithmic technologies and AI, has led to a renewed interest in the role of technologies in knowledge work. Some of these technologies act as epistemic technologies, a term derived from the work of Knorr Cetina on how sciences make knowledge. While previous studies provide important insights into how the outcomes of the technologies are used in expert work, the work needed to produce the outcomes in the first place is often overlooked and separated from use. The generation of new data and information is instead treated as both black-boxed and decontextualized. To highlight the work required to generate meaningful outcomes, and address the challenges posed by opaque algorithms, we present a longitudinal in-depth study of the medical imaging technologies of the Robotic X-ray and iMRI, used in combination with surgery. The study illustrates how technologies become epistemic through use: new data was produced by means of interactions within a relational and heterogeneous assemblage of people, technologies and devices. Through trained judgement, the experts made the data useful and possible to act upon in each specific situation. The study contributes to research into the use of algorithmic technologies in knowledge work by showing how opaque algorithms can be complemented by contextualized information, making it possible to interrogate and make trained judgements, in relation not only to outcomes, but also to their production. We conclude that epistemic technologies are involved in the ongoing construction of knowledge, during both the production and use of outcomes, and that enacting the technologies as epistemic includes a situational and material awareness.
Keywords
Introduction
The increased use of advanced technologies, generating new data and information, has led to renewed interest in the role of technologies in knowledge work (e.g. Anthony, 2018, 2021; Faraj, Pachidi & Sayegh, 2018; Kellogg, Valentine & Christine, 2020; Lebovitz, Levina & Lifshitz-Assaf, 2021; Lebovitz, Lifshitz-Assaf & Levina, 2022; Pakarinen & Huising, 2023; Scarbrough, Chen & Patriotta, 2024). Many of these studies have a strong focus on algorithmic technologies and AI, illustrating how these technologies support and enable experts in the performance of their work, e.g. predicting crime incidents (Waardenburg, Huysman & Sergeeva, 2022), and enable legal service delivery (Kronblad, 2020). Some of the algorithmic and AI technologies being explored in these studies are also claimed to ‘play a key part in the ongoing construction of knowledge’ (Anthony, 2018, p. 661), and also in the evaluation of knowledge claims (Lebovitz et al., 2022; Scarbrough et al., 2024). Therefore, they may be described as epistemic technologies, a term introduced by Anthony (2018) and derived from the work of Knorr Cetina (1999) as regards how sciences make knowledge.
While these studies provide important insights into how the outcomes of these technologies are used in knowledge work, often needing to be translated via human judgement in order to be useful (Geampana & Perrotta, 2023; Lebovitz et al., 2022; Waardenburg et al., 2022), the work needed to produce these outcomes in the first place is often overlooked and separated from use. The generation of new data and information is instead treated as both black-boxed and decontextualized (see also Pakarinen & Huising, 2023). This is because when the technologies rely on algorithms that are opaque, it becomes difficult to examine how these technologies have arrived at a particular outcome (Anthony, 2021; Lebovitz et al., 2022).
In this paper, we shift our focus away from the outcome of the technology toward the work required to both produce meaningful outcomes and act upon them. Pakarinen and Huising (2023) emphasize that the embedding of technologies in webs of interaction depends on how experts both attend to and tend to these technologies. To highlight this kind of work, and address the challenges posed by opaque algorithms, we propose studying advanced technologies that integrate both the digital and mechanical qualities of materialities (see also Barrett, Oborn, Orlikowski & Yates, 2012). This consideration is crucial because technologies initially appearing purely digital, such as AI and the algorithms processing digital data, may seem to lack physical embodiment or material presence, presenting as incorporeal technologies. However, in practice, they often manifest themselves physically, interacting with humans and physical objects (Bailey, 2022). From such a perspective, algorithms must be understood as part of a relational and heterogeneous assemblage of humans and other objects and technologies (Bailey, Faraj, Hinds, Leonardi & von Krogh, 2022; Glaser, Pollock & D’Adderio, 2021; Pakarinen & Huising, 2023). This also has consequences as regards how we understand the role of epistemic technologies: They are not acting alone, new data and information are instead being produced by means of interaction between the experts and the technologies, other devices and instruments (Kaplan, Milde, & Cowan, 2017; Knorr Cetina, 1999; Rennstam, 2012). The aim of the study is thus to describe and analyse the situated and contextual aspects of producing and acting upon new data and information, for example how epistemic technologies are used in expert work to produce meaningful outcomes.
The paper is based on a longitudinal in-depth study of the introduction and use of advanced medical imaging technologies in so-called hybrid operating rooms (hybrid ORs). These rooms are equipped with the cutting-edge medical imaging technologies of the robotic X-ray and the interoperative MRI. These large machines are powered by advanced algorithms, thus embodying ‘hybrid qualities of materialities’ (see Barrett et al., 2012, p. 1450), which provide opportunities for developing new methods of augmented surgical navigation, as well as so-called intra-operative imaging, where diagnoses and treatments are co-produced (e.g. Bazzi et al., 2021). Producing and acting upon images during medical procedures requires collaboration among medical teams specializing in radiology, anesthesia and surgery, fields which have traditionally been separated both physically and temporally.
The study illustrates how use of the imaging technologies was dependent on the assemblage of devices, other technologies and people in the hybrid ORs. Producing images was conditioned by the fact that the technologies integrated both digital and mechanical qualities. Making the algorithms work (in order to produce images) required a lot of tinkering with the material and physical aspects of the assemblage, which contributed toward creating a relational functionality. The assemblage was thus constructed and kept together by a relationship whereby devices, technologies and people continuously influence each other. This ongoing work provided the medical team with the contextualized information necessary for interpreting and making joint judgements during both the production and use of images. Moreover, this information was also necessary for recognizing which procedures and images were trustworthy, and which thus become embedded in the medical practice. These activities unfold recursively over time and contribute toward the co-constitution of technology, and the practice with which it engages.
This study contributes toward research on advanced algorithmic technologies in knowledge work by showing how technologies become epistemic through use: New data is produced by means of interactions within a relational and heterogeneous assemblage of people, technologies and devices. Moreover, the data produced is not treated as an objective outcome (knowledge claim) to act upon. Instead, through trained judgement (Daston & Galison, 2010), the experts make the data useful and possible to act upon in each specific situation. We conclude that epistemic technologies are involved in the ongoing construction of knowledge during both the production and use of outcomes, and that enacting these technologies as epistemic includes a situational and material awareness. In addition, this study also contributes to research into the use of algorithmic technologies in knowledge work by showing how opaque algorithms can be complemented by contextualized information, making it possible to interrogate and make trained judgements in relation not only to outcomes, but also to their production.
Advanced technologies in knowledge work
It is increasingly common to use advanced technologies, including algorithms, during knowledge work. This development has also increased the level of interest in research into how outcomes, for example new data and knowledge claims, become useful in practice and contribute to knowledge work. Importantly, the use of such technologies does not automatically lead to the straightforward generation of knowledge: Rather, as several studies have convincingly shown, uncertainties and ambiguities in work practices may arise (e.g. Geampana & Perrotta, 2023). The outcomes generated by the technologies may challenge both the expertise and jurisdiction of professionals (Scarbrough et al., 2024), and highlight the status differences among these (Anthony, 2018), with the potential to both enable and disrupt how new data and knowledge claims are acted upon and evaluated.
One important aspect of the increased use of algorithmic technologies, and the strong focus on how the outputs become useful in practice, is that this will most likely ‘augment the importance of human judgment in knowledge work’ (Faraj et al., 2018, p. 66). This is because how these technologies arrived at a certain output is not always transparent, making it difficult to examine the production of outcomes. The opacity of the algorithms relates to the difficulties of understanding the reasoning behind the given outcomes (Lebovitz et al., 2022), representing a challenge to the knowledge claims of professional groups. For example, Waardenburg et al. (2022) show how opaque algorithmic predictions require knowledge brokers (intelligence officers) to pass judgement in order to translate the output for the users (police officers) in order to make the new data useful in practice, and how they substituted the algorithmic predictions for their own judgements when needed. In their study of diagnostic radiology, Lebovitz et al. (2022, p. 127) show how experts relate ‘AI results’ to their initial judgements, then engaging in interrogating practices to integrate the knowledge claims made by algorithmic technologies with their own knowledge claims. Due to the technology bypassing information used by radiologists to contextualize images, the outcome was sometimes found to be inconsistent with the experts’ diagnosis and judgement.
Even though the materially embedded assumptions included in the technologies are not immediately obvious to their users, they ‘can have a significant impact on the outputs created’ anyway, thus influencing how knowledge workers construct knowledge (Anthony, 2018, p. 661). Moreover, as the experts are held accountable for how the outcomes are used, they need to verify and explain those outcomes (Pakarinen & Huising, 2023). Allen and Choudhury (2022) argue that the experts have an advantage in using tacit knowledge, and that they have a better understanding of context and human values for making judgements. Therefore, the domain experiences of experts should be seen as complementing algorithmic outcomes. However, if the experts are unable to make sense of the decontextualized information, and not being able to supplement it with credible explanations, then the outcome of the technologies may be either contested or ignored (Kiviat, 2019). This may also lead to experts developing an ‘algorithmic aversion’, instead relying more on their own judgement (Allen & Choudhury, 2022).
These studies illustrate the problem of decontextualized information and opaque algorithms. However, it is not only the algorithms that are opaque, so too is the data ‘fed’ to the algorithms that the technologies depend on (Waardenburg & Huysman, 2022). For example, all the images stored in databases functioning as the basis of the radiological AI technologies for making predictions are of significance to the outcomes being produced. In their study of timelapse imaging during fertility treatment, Geampana and Perrotta (2023) point to how knowledge workers are aware of the conditions under which the technology is used. They show how embryologists make judgements regarding the quality of the embryo and override the output from the technology, which they see as an incorrect annotation. Thus, not only are the algorithms themselves of significance to the outcomes generated by the technologies, but also the data fed to them. This has also been pointed out by Pakarinen and Huising (2023), who emphasize that inputs into, as well as the outcomes of, the algorithmic technologies need to be adjusted, adapted and supplemented by the expertise contained within the assemblages where the technologies are used, and where knowledge work unfolds.
Therefore, researchers have recently been suggesting that studies of algorithmic technologies should pay attention to the relational and heterogeneous assemblages of humans and other objects that the technologies form part of (e.g. Bailey et al., 2022). From a relational perspective, the algorithmic technologies generating the outcomes used in knowledge work should be understood in relation to the communities and contexts where they are used (Pakarinen & Huising, 2023). For example, in their study of pharmaceutical robots, Barrett et al. (2012) demonstrated how the material aspects of digital innovations intertwine with everyday practices. They stress the necessity of considering the fact that many technologies consist of both digital and mechanical qualities. Bailey (2022) also points out that, since algorithmic technologies interact with humans or physical objects, this interaction unifies intangible and physical components, emphasizing the need to view these as intertwined entanglements.
The relational perspective thus emphasizes the fact that the technologies used in knowledge work are part of an assemblage, thus being entangled and intertwined with people and other technologies and devices. The technologies themselves, however, are not stable entities (Glaser et al., 2021), potentially changing through use and in relation to the assemblage they form part of. These technologies can thus be described as emergent, as described by Bailey et al. (2022); a set of evolving relations whose underlying components, configurations and arrangements are always in a state of flux. Using such a perspective, we must emphasize the co-constitution of technology and the practice with which it engages. This also means that the co-construction of knowledge cannot be understood independently of experiences, past transactions and established knowledge claims (Pakarinen & Huising, 2023). In order to do so, we will draw upon science- and technology-oriented studies of the role of epistemic objects and technologies in the ongoing construction of knowledge.
Epistemic objects and technologies
Advanced technologies that generate outcomes taking part in the ongoing construction of knowledge are sometimes described as epistemic technologies (Anthony, 2018; Lebovitz et al., 2022: Scarbrough et al., 2024). However, given the strong focus on the output of the algorithmic technology, and concern regarding black box production, recent studies entail the risk of treating epistemic technologies as stable entities rather than as something enacted into being. If this is the case, the concept may lose its original analytical momentum.
The concept of epistemic technology is derived from the work of Knorr Cetina (1997, 1999) on epistemic objects, work which is based on the idea that there is a relationship between the expert and the object or technology whereby these continuously influence each other. This means that the work of producing the outcome is as important as the outcome itself, and cannot be separated from it. The dynamic nature of epistemic technologies, as presented here, highlights the fact that objects and technologies become epistemic whenever they generate new data and information that is not yet fully known or categorized (see Knorr Cetina, 1999).
Epistemic objects and technologies have a changing and unfolding nature (e.g. Ewenstein & Whyte, 2009; Knorr Cetina, 1999): When in use, they ‘puzzle and provoke and invite to action’ (Rennstam, 2012, p. 1075). The use of epistemic objects and technologies thus reflects a process which involves raising questions, but also asks how they can be used collaboratively to find answers and jointly develop knowledge (Ewenstein & Whyte, 2009).
Epistemic objects are often contrasted with technical objects such as stable instruments and tools (Knorr Cetina, 1997; Rheinberger, 1997), with the object type being determined by its use. Schiemer (2024) describes this thus: ‘actors can either look at their tools or look through their tools’. Looking at tools means that these are taken for granted and thus disappear into the background, while looking through tools means that the epistemic object participates in the production and elicitation of the experts’ knowledge of what to do and how to do it. Rennstam (2012, p. 1074) exemplifies this in terms of how an engineer works with an electronic component which ‘. . . cannot be reduced to an instrument; instead, it is the object of the engineer’s knowing process’.
Different people interact differently with the same object or technology, something which may change them (e.g. Ewenstein & Whyte, 2009; Rennstam & Paulsson, 2024). Epistemic objects and technologies may also be transformed by interactions between different communities. McGivern and Dopson (2010) show how the interactions of several local professional communities, each influenced by different epistemic rules, transform an epistemic object over time: Through its use, it became taken for granted, being reincarnated into a technical object. Another situation is illustrated in Schiemer’s (2024) observations of the work done in a music studio where instruments and computer programs were the subject of creative engagement but subsequently faded into the background, albeit situationally structuring the time for new creative engagements. Such shifts are not, however, always smooth, and may include epistemic clashes, struggles and negotiations over technologies.
Ewenstein and Whyte (2009) emphasize that epistemic objects (and also technologies, we claim) are a fundamental component of experimental systems because they are objects of inquiry. Experts continuously need to unravel the features of a technology, and its implications, while also comparing the outputs of technologies with other sources. As Knorr Cetina (2001, p. 176) remarks: ‘Only incomplete objects pose further questions, and only in considering objects as incomplete do scientists move forward with their work.’ The use of epistemic technologies thus requires both reflection and the questioning of taken-for-granted assumptions and beliefs. Moreover, as suggested by Miettinen and Virkkunen (2005), paying attention to the circumstances under which epistemic objects and technologies are used makes them more transparent, but also shows their limitations when facing the challenges of the present.
One example of an epistemic technology is the particle accelerator used in experimental physics, being designed on the basis of current physics theory and producing new data that may either support or cast doubt on existing theory (Galison, 1997; Traweek, 1988). Both the performance of and the outcome produced by the epistemic technology thus need examination, interpretation and judgement regarding their significance (Rheinberger, 1997). Interpretation and judgement thus involve not only the outcome but also the use of the technology, and thus the process of producing outcomes. To capture such situated processes of expert interpretation, Daston and Galison (2010, p. 314) introduced the term ‘trained judgement’.
While professional judgement is often ascribed to the expertise and experiences of a single person (Dirsmith, Covaleski, & Samuel, 2015), trained judgement includes collective assessment and interpretation. In addition, judgement is used to make data useful (Daston & Galison, 2010; Galison, 2014) in each specific situation (here, medical procedures). However, this is not premised on the belief that epistemic technologies, for example imaging technologies, would offer ‘pure’ or ‘authentic’ data that mirrors actual conditions (Pantzar & Ruckenstein, 2017). Instead, trained judgement involves considering the context and background assumptions prescribing which parts of the assemblage are relevant, or how these parts are related to each other (Daston & Galison, 2010).
Taking a dynamic and emergent perspective on epistemic technologies, our view is that the technologies are part of ‘knowing in practices’, which means that they cannot be separated from their users. This means that we also need to focus on the relational and heterogeneous assemblages of humans and other objects that the technologies form part of. Next, we describe the methodology of the study, as well as how two advanced imaging technologies are intertwined with medical practices to become epistemic through their use.
Methods and Research Context
To investigate how epistemic technologies are used in expert work to produce meaningful outcomes, we draw on a longitudinal in-depth study of the use of advanced imaging technologies at a Swedish university hospital. A new centre hosts the bulk of that hospital’s state-of-the-art medical imaging technologies and image-guided treatments, including four hybrid operating rooms (ORs), used for both acute care and planned procedures, where high-risk patients suffering from severe and complex conditions are treated. This is also an R&D unit, with the staff working there being involved in both developing new procedures and refining existing ones. Making use of imaging technologies during surgery, so-called intra-operative imaging, in order to guide the work of the surgeons, was a new phenomenon. Thus, there were no established practices or standardized procedures to lean on.
The hybrid ORs are designed to combine the practices of radiology, anesthesia and surgery. They are almost twice the size of ordinary ORs and are equipped with technologies and devices connected with the medical practices. The ORs also need to simultaneously host all the staff working there. Before being allowed to work with the imaging technologies, all members of staff need to undergo training provided by the MedTech suppliers, with the doctors having attended specific training programmes on how to use the imaging systems to perform medical procedures.
Here, we present two hybrid ORs equipped with different imaging technologies; one with an advanced MRI scanner and the other with a robotic X-ray machine. The iMRI hybrid OR has a ceiling-mounted MRI scanner, which is housed in an adjacent room and moved into the operating theatre when needed. To produce images the patient is placed inside the large scanner. The X-ray hybrid OR has a floor-mounted robotic X-ray machine, which has a C-shaped arm that rotates around the patient and produces 3D images in real time. This C-shaped arm measures 130 cm in diameter and has both an X-ray tube and a detector mounted on each side of the C. This allows the production of different kinds of image using ionized radiation, that is, flat X-rays, fluoroscopy (a series of images – like a film) and 3D images.
Both imaging technologies are sizeable and heavy machines that demand considerable space, utilizing sophisticated algorithms to translate the signals from either the MRI scanner or the radiation detector to produce images shown on screens in both the ORs and the adjacent control rooms. These algorithms make it possible not only to produce real-time images during surgery, but also to compare and merge preoperative images with real-time images, thus facilitating the development of augmented-reality techniques of surgical navigation.
The imaging technologies became pivotal in the sense that doctors and nurses from various medical specialties needed to interact and coordinate their tasks with the technology in order to produce and act upon the images. This includes adapting the medical practice to the needs of the technologies while also adapting the technologies, as well as all the other devices, both to the general needs of the medical practice and to the specific needs of the patient.
Data collection
Between 2014 and 2019, two of the authors conducted extensive fieldwork in the hybrid ORs using a combination of field observations, shadowing and interviews (Czarniawska, 2014). The Ethics Committee for Sweden approved the studies, and the informed consent of the participants was obtained. Initially, we conducted interviews with all the groups of staff working in the hybrid ORs (healthcare assistants, nurses and doctors working in radiology, anesthesia and surgery) in order to gain a comprehensive understanding of these groups’ established work practices and medical specialties. As the rooms had just been commissioned, we observed training sessions for the various staff categories as regards how to use the imaging technologies, as well as workshops where anesthesia, radiology and surgical nurses, plus healthcare assistants, all collaborated to combine their different practices using the new rooms. Supplier representatives, medical technicians and physicists (specializing in imaging) were also involved in these sessions and workshops. These people were also interviewed and observed during their interactions with the staff of the hybrid ORs.
In the field, it immediately became clear that the medical staff had no standard operating procedures, protocols or routines to rely on when using the new technology. Many of the activities and discussions thus concerned how to use the imaging equipment, what constituted a ‘good enough’ image, and how to find new ways of interacting in the room. Inspired by Barley (1986), we greatly relied on observations when mapping emergent patterns of action and interpretations as regards the new technologies being used in medical practice, and as regards recording who interacts with whom, in what ways and at what times. Thus, when the rooms were ready for use, we continued to observe the nurses and doctors in their day-to-day work. We took part in pre-meetings, when the teams discussed and planned medical procedures in relation to the needs of specific patients. These meetings often included looking at previously captured images, and discussing how to position the patient on the table in order to produce new good-quality images, while also enabling surgery to be performed optimally.
Observing medical teams performing procedures in the hybrid ORs afforded us a unique insight into clinical practices, for example how these teams used tools and technologies, how they discussed and coordinated their activities, and the relational dynamics between the team members. Several groups of staff had never worked together before, and neither had they used imaging technologies. We therefore paid particular attention both to the coordination and the interdependencies between physicians with different specializations (mainly in surgery and radiology) and to the use of the technologies. We also attended post-procedure meetings when doctors discussed and evaluated both their work and the medical outcomes. During our observations, we took extensive fieldnotes, taking into account verbal interactions, the physical settings and, more generally, the collective actions and interactions of the participants. Moreover, during our observations, the staff often explained to us what they were doing, and we also had the opportunity to ask questions. Altogether, we conducted 116 interviews and 349 hours of observations (see Table 1).
Data Collection.
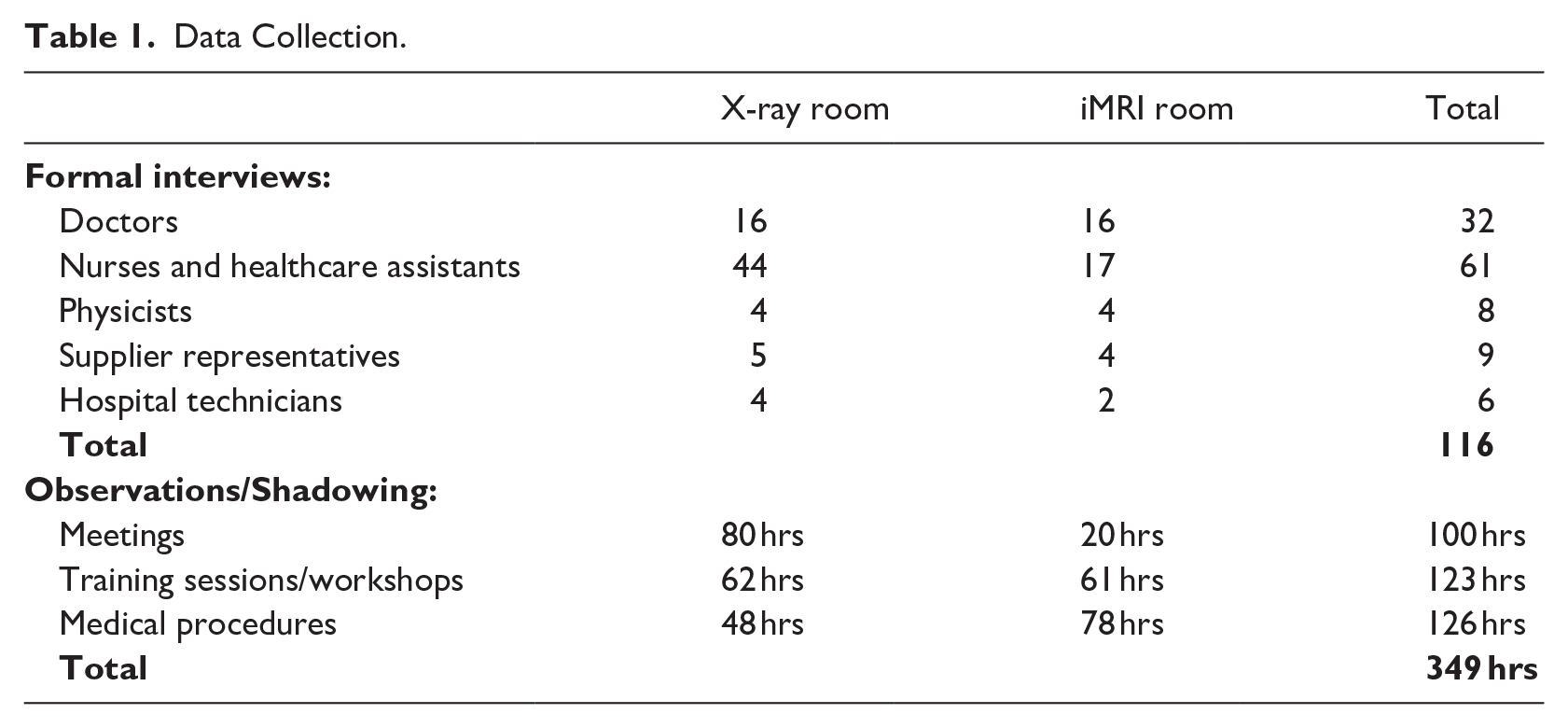
The interviews lasted between 1 and 2 hours and were recorded and transcribed. We also engaged in informal conversations during coffee breaks and in corridor meetings, which gave us further insight into each respective practice. Moreover, we also gathered documents, for example medical reports, method cards and publications written by the medical teams. Sometimes, texts served as the input for questions and discussions during the interviews, while on other occasions these were referred to during meetings: We checked them afterwards in order to gain further insights into practices. Taken together, the studies have resulted in extensive field material.
Data analysis
Inspired by a grounded theory approach (Charmaz, 2006; Czarniawska, 2014), we have engaged in an iterative process of comparing the data from different sources over time. During our fieldwork, we continuously discussed ‘the practices in the making’ and, as we found no systemic difference between the activities carried out in the two hybrid ORs, we collapsed the data from both rooms during our analysis.
To capture a broad range of emerging codes, we read fieldnotes and interview transcripts and we also wrote memos to track and explore the emerging codes and the connections between them (Charmaz, 2006). We started by focusing on the interviews and the observations of training sessions and meetings, when the technologies were new at the hospital. The field material mainly concerned the practical aspects of how to make use of the technologies, and how to develop new procedures and routines in the room when several medical specialties were interacting. The interviews also included reflection on both the potential of and the concerns around using imaging technologies. The initial codes included, for example: a lack of experience of the technologies, exploring the potential of the technology, and interdependencies between staff of differing expertise.
During our subsequent analysis, we paid special attention to the longitudinal and situated nature of our data in order to examine the activities and interactions of the medical staff working in the hybrid ORs during surgery. We mainly focused on the field material from observations, both notes on activities and conversations between the staff and with us, specifying in detail the activities and interactions of the medical staff working in the hybrid ORs when the new technologies were in use. We then compared the notes from observations with the interview transcripts where the staff reflected upon their activities. We mapped how the medical staff worked toward producing images and noted that a lot of work had to do with preparing for the production of images, interdependencies between entities (devices, technologies and people in the OR), and how to attend to different needs and align different entities in order to produce images. We also noted that the production and use of images was entangled: For example, when the experts interpreted the images, they often referred to how the image was produced, then decided how to proceed and act upon these images in order to finalize the surgical procedure. We also paid attention to the post-procedure discussions in order to capture how the participants reflected upon the process of producing images, and how they were making their interpretations explicit and creating confidence in these interpretations by drawing upon previous experiences and established knowledge claims. We also noted how they explained their interpretations to each other and what they recognized as trustworthy images.
One key insight gained from coding was that, to make the algorithms work toward producing high-quality images, there was a lot of tinkering and situational adjustments to the physical aspects of the technologies, and also to other devices, technologies and people (staff and patients). Over time, it became clear that the work of producing and acting upon the images was intertwined with ongoing and joint judgements. The medical experts made judgements about both the process (the production and use of the technologies) and the results (the images). Three key themes emerged: creating relational functionality, moving from interpretation to explanation, and recognizing images as trustworthy. Common to the themes was the situational and material awareness necessary in order to make the imaging technologies work. They jointly illustrate how the imaging technologies are used in expert work to produce meaningful outcomes.
We continued by further elaborating upon the themes and their connections with the literature on judgement, and the use of advanced technologies in knowledge work. The field material shows that judgement was part of the ongoing process of producing, interpreting and acting upon the images, thus not only being in relation to the outcome, and that this was done jointly by several experts. To further analyse these ongoing processes, we continued by drawing upon the literature from science and technology studies of epistemic technologies and trained judgement. We reanalysed all our fieldnotes, transcripts and memos. This allowed us to investigate the ongoing accomplishment of the relational and heterogeneous assemblage of devices, technologies and people in the hybrid OR, and to reveal how the joint work and judgement of the medical staff contributed toward enacting the imaging technologies as epistemic technologies. In the following sections, we present our analysis of the field material.
Enacting Epistemic Technologies: Producing and acting upon images in the hybrid OR
Making use of the imaging technologies in the hybrid ORs is based on integrating the practices of radiology and surgery, with the support of anesthesiologists, into a collaborative process of making diagnoses while providing treatment at the same time. The technologies participate in the medical practice within an assemblage of people, devices and technologies, all of which are necessary to produce medical procedures. The work done in these rooms thus breaks with convention regarding established and previously separated medical practices, requiring staff with different expertise to align their practices and jointly investigate how to both produce images, including new data, and act upon these during surgery.
In what follows, we present how the imaging technologies were enacted as epistemic technologies, as well as how the work of producing and using intra-operative imaging was intertwined with joint judgement.
New technologies, new opportunities
The introduction of advanced imaging technologies into hybrid ORs brings both new opportunities and challenges to medical practices. The medical staff set out to discover the potential of the technologies, as well as how to produce images during surgery which would augment surgical navigation. As the use of inter-operative imaging was quite a new phenomenon, the medical staff, both jointly and through the ongoing use of the technologies, had to figure out how to use them. As one neurosurgeon working in the iMRI room explained: We’re the first in Sweden to have this technology, and it’s also unique in global terms, so there are no established procedures regarding how we’re supposed to do things. It’s so new and we don’t have too much experience of it, or data on it yet, so it’s something we’re working out as we go along.
The medical staff emphasize the fact that the technologies present a complex and emerging way of working for the medical team, meaning that it is not possible to fully anticipate or know beforehand all the potential opportunities and challenges these technologies are offering. The imaging technologies were treated as open-ended and dynamic entities that require ongoing negotiation and adaptation in order to produce new data and information, rather than prepackaged, standardized tools. Thus, even if the technologies appear to be stable entities, they will be open to inquiry in the sense that, in being used, they are adaptable and become integrated into the medical practice. Despite extensive training and simulations, the real opportunities afforded by the technologies are only explored during real-time surgical procedures. One surgeon observed the following: You don’t really know what you’ll be facing until you’re in the middle of surgery, and that’s when you start thinking: ‘Okay, how else can we use this tool to get what we need?’ It’s about making full use of all the opportunities that exist, and I don’t know if we’re doing that. There are probably even more opportunities that we don’t even know about yet, or that we haven’t fully explored. The more we use the technology, the more we learn, and the more opportunities we see.
This highlights the emerging nature of these technologies, as well as their role in refining existing medical procedures and developing new ones. Unlike many other medical technologies, operating within established routines and tending to be taken for granted, the imaging systems used in hybrid ORs are not fully known or predetermined in terms of their use. In order to unpack the imaging technologies and use them during advanced medical procedures, the medical staff working in the hybrid ORs also need to be open to experimenting and adopting a participative interaction style (see Edmondson, Bohmer & Pisano, 2001). They are experts and confident in their roles, but they are also novices in relation to the use of imaging technologies in this particular setting. As a radiologist explained: The technology is great, but it’s only as good as the way in which we, as a team, can jointly make sense of it. A lot of the time, it’s the discussions taking place between the radiologist and the surgeon that make us realize: ‘Hey, we can actually use the technology in a way we hadn’t thought of before.’
The medical experts jointly figure out both how to use the technology and what it can offer in terms of improving medical procedures. Interaction with the technology is thus inquisitive and exploratory, highlighting how the potential of the imaging technologies is discovered and developed in use. The technologies are thus treated as open to inquiry and the potential of the technology is realized incrementally, through joint and situated work, whereby the technology and the experts’ knowledge influence and reshape each another (e.g. Knorr Cetina, 1999; Rennstam, 2012). Thus, opportunities and challenges emerge from using the technologies. As we will show in the following sections, it requires practical hands-on work to make these technologies function in the ORs.
Tinkering in order to create a relational functionality
In order for the imaging technologies to function, they need to be aligned with other devices, technologies and the patient in the hybrid ORs so as to form a relational and heterogeneous assemblage that fits and keeps together. The interdependencies between all these entities require situational adjustments and adaptations of the assemblage in the ORs. The hybrid ORs feature an operating table in the middle of the room, and a huge number of other technologies and medical devices around that table. In producing images, there are different material aspects and requirements, for example patient and equipment positioning, in addition to spatial constraints which need to be considered. The medical staff tinker with the different devices, the patient’s body and the physical and digital aspects of the technology. This includes exploring, adapting and paying attention to detail, and changing these until a relational functionality is achieved. Thus, the production of images is dependent not only on the accuracy of the imaging technology but also on the interdependencies between the entities in the assemblage.
One challenge in this new context lies in positioning the patient’s body so that the imaging technology can come as close as possible to the relevant body parts, and at the right angle, in order to produce high-quality images. One neurosurgeon explained how the surgical team, together with the supplier representative, dealt with this issue: It’s been a challenge; we’ve needed to think carefully about how to position the head fixation device. There were a lot of problems in the beginning. For example, in the first couple of cases, we could hardly get the patient into the MRI scanner. I think Benny [an MRI application specialist] had to temporarily remove a rail from the table, or something. These kinds of things are very difficult to predict, even if you do carry out simulations and train in them. So, it’s only been during real-time procedures, after several cases had been dealt with, and when we’d encountered ‘real-life situations’, that we’ve started learning about this.
Their actions reflect being attuned to the situation, as the patient’s positioning impacts the functionality of the imaging technologies. Another practical aspect was that the table had to be adjusted to fit into the MRI scanner. This illustrates the fact that, even if these technologies look remarkably solid and sturdy, they are adaptable and able to accommodate change (see also Mol, 2008).
Another challenge lies in positioning other devices and objects in the OR so that the imaging technology can access the patient without any interference. One example of this is the activities undertaken before performing a rotation of the robotic X-ray. The system senses the outer limits of the table to avoid the risk of collision, but it does not sense other devices and technologies. The technologies take up a lot of space and everyone needs access to the patient. Quite often, the staff have to rearrange all the machines and devices in the room to make sure that the imaging technologies have access.
While the doctors are discussing what protocol to use to produce an image, the nurses check all the surgical devices around the table. Loosely fitted hoses are strapped onto the table, trays attached to the table are removed, and trollies carrying surgical tools and other medical equipment are moved away in order for the robot to rotate freely around the table. When everything is ready, the staff move out of the zone surrounding the patient. The chief radiologist looks around the room to check that all staff are using protective shields and then she announces that a rotation is about to occur. (fieldnote, 5 May 2016)
This shows how the interdependencies between the devices, tools and people in the OR have to be attended to in order to produce images. The medical staff are engaged in adjusting these to accommodate the needs of the technologies, while simultaneously taking their needs into account. This reflects the importance of the situated and relational aspects of the assemblage in allowing the technologies to function effectively (Bailey et al., 2022). The physical elements of the technology and the rest of the assemblage thus have to be finely tuned to enable the digital algorithms to work properly.
Yet another example illustrates how the medical staff tinker with both the digital and physical aspects of the imaging technology. The robotic X-ray needs to be positioned as close to the patient as possible, to optimize the quality of the image, and to minimize scattered radiation. For the most common procedures, the control panel displays a choice of programs that include pre-defined sets of radiation doses, how many X-ray images are to be taken within a defined time interval (sequence), and how many seconds a sequence of images is to last. Quite often, however, the parameters need to be altered in relation to the needs of the individual patient in order to produce a high-contrast image.
During vascular surgery, the doctors decide to do a fluoroscopy. They gather round the control panel to discuss different settings. The radiologist asks one of the surgical nurses about the patient’s liver status before deciding what level of contrast medium to use, as well as what radiation dose to use. The supplier representative interrupts and shows how they can use the software to make more finely-tuned adjustments. The doctors decide to zoom in on a specific part of the body. This means that a lower radiation dose can be used, but concentrated to a defined area. (fieldnote, 12 May 2018)
This example shows that there is a need to adjust the digital aspects of the technology for each specific procedure to ensure the best outcome. This highlights what Burri (2013, p. 376) claims: ‘The experts know that every image can be manipulated at every single step of its production.’ The team needs to manually adjust the digital settings of the technologies in order for the algorithms to produce images. They combine instructions regarding the functionality of the technology with their knowledge of the patient’s condition in order to produce images. These adjustments are discussed and then jointly carried out by the medical staff, here too with the support of the MedTech supplier representative.
Taken together, the activities that make the technologies produce images reveal a pattern of tinkering with, as well as situational adaptations of, the assemblage of the devices, other technologies and people in the hybrid OR. This was based on a collective understanding of the process and required ongoing joint judgements regarding what to do and how to do it. The examples above demonstrate how the medical team’s work required an understanding of the situated and contextual aspects of both the OR and the technology, as well as how all the entities in the assemblage are adjusted and aligned to create a relational functionality (see Bailey et al., 2022). The medical team’s ability to fine-tune these entities in relation to each other reflects the inherent uncertainties that arise in each case, where the specific needs of the patient and the conditions in the OR demand flexibility. This means that the technologies cannot be separated from the users and from other devices and technologies.
Making the technologies ready to produce images also involves constant negotiation between the digital and mechanical components of these technologies, and the assemblage they form part of. Moreover, this also shows that, while the output (the images) might appear to be a purely digital product, the production of the images is deeply dependent on the physical setup and configuration of the OR, the positioning of the patient, and the alignment of the various technologies and devices. It is not simply a matter of following set protocols, but involves continuous tinkering and joint judgement. Creating a relational functionality is, thus, an ongoing accomplishment whose successful performance is not only dependent on technical skill, but is also closely intertwined with material and situational awareness, where hands-on and real-time problem-solving is required in order to adapt to both the situation at hand and the context.
From interpreting to explaining images
When navigating inside the patient’s body and in order to guide their surgery, the surgeons depend on accurate high-quality images. The data produced by the technologies has a dual effect; that is, the images augment surgical navigation but also alleviate clinical uncertainty. Ambiguity and uncertainty may grow because, with new information, different kinds of epistemic issues arise. Thus, merely producing an image does not necessarily guarantee that it will be ready to act upon: Instead, given their different kinds of medical expertise, the doctors need to make their image interpretations explicit. They justify their interpretations by referring to other images, by giving examples of previous experiences and by questioning the imaging technologies. The relevance of the information conveyed by the images will only be established if their interpretations can be explained to the others. Thus, the images only become relevant when plausible solutions are interpreted and proposed (see Burri, 2013).
Neurosurgeons operating on the brain are aware that, if they remove healthy tissue, then there will be a high risk of the patient ending up injured or badly disabled. However, as these surgeons are trained in evaluating medical procedures on the basis of what they observe in wounds, for example, or how tissue reacts when touched, they are not always automatically confident about trusting what the images show. One surgeon explains why interpreting images is difficult: It can be the case that some images are not anatomically correct. You have to look at them quite carefully, and with a certain level of scepticism. So that you don’t get fooled, and so as to make sure that [the image] is really accurate.
Radiologists also agree that the inter-operative images are not always easy to read, and that sometimes the visual information needs to be questioned. As these images form part of surgery, it is not only up to the radiologist to detect, for example, the size of a tumour, but the image is immediately acted upon by the surgeon. The medical team are thus dependent on each other’s interpretations and explanations regarding both the new data and the situation at hand. As the team represent different medical specialties, including various knowledge claims, they need to align these and acknowledge each other’s expertise. Thus, the image needs to be supplemented by credible explanations (see Kiviat, 2019) in order to be acted upon during surgery.
During one surgical procedure, a brain tumour resection, the surgeons suddenly spot something in the surgical wound that they suspect may be a cerebral aneurysm. The response of the radiologist working in the adjacent control room is that he does not think this is the case. He then says aloud: ‘Could this really be a thrombosed aneurysm? I think it’s old blood from a previous biopsy.’ He goes through the old images again and then says, ‘I can’t see an aneurysm here.’ The radiologist enters the OR and is now looking, both directly into the wound and through the microscope, at what the surgeons suspect may be an aneurysm. They continue discussing this, then decide to perform a real-time MRI scan. The radiologist and the surgeons first look at the new images, and then say they can’t really see any signs of an aneurysm, when comparing with images taken before this round of surgery. After some discussion, sharing their thoughts, they agree that it’s safe to continue with the surgical procedure. (fieldnote, 28 March 2019)
Together, they discuss what they already know about the patient on the basis of previous examinations and the images available, serving as important input that has to be linked with their experiences and expertise regarding the specific procedure to be performed. This means that they are drawing on their past experience in order to assist the activities currently being conducted. They also need to make these assumptions and interpretations explicit in order to make them trustworthy, so that they can be acted upon. In this case, the initial interpretation made by the radiologist seems to be correct: Based on their discussions about what they see in the new images, they agree that it is safe for the surgeons to continue resecting the tumour. The data produced and expressed in visual form thus needed to be trusted, while simultaneously being treated with scepticism (see Anthony, 2021) whenever the images were conveying information that was ambiguous and/or inconsistent with previous experience or expectations. If the medical team is unable to jointly make sense of the images, they will be contested and may possibly be ignored (see also Kiviat, 2019).
Another episode reveals how abdominal surgery is combined with the use of 3D images, produced by the robotic X-ray, to facilitate navigation during surgery. During the procedure, the surgeons encounter a situation where they do not know the ‘depth’ of the tumour, or how close to an artery it is. In collaboration with the radiologists, the surgeons decide to produce a 3D image by using a pre-defined protocol for the radiation dose. Once finished, the doctors gather round the screen to discuss the image: One of the surgeons is quite sure of his interpretation: ‘Look here, it’s close to the artery, but I think it’ll be ok if we continue as planned.’ The other surgeon doesn’t agree: ‘Well, I’m not so sure . . . If I can see it from another angle perhaps?’ The radiologist starts working on the computer, zooming in and out and rotating the image. The surgeons point to certain parts of the image, and discuss what they see, as well as what they can’t see. As they’re still in disagreement, the radiologist suggests that producing a new image using some other settings (i.e. a different dose and time interval) would assist them in making a better decision. After the second rotation of the robotic X-ray, all the doctors gather round the screen again to look at the new image. ‘Yeah, now I see what you mean,’ says the hesitant doctor. The more self-assured doctor says; ‘Well, the artery is much closer than I first thought. This image is better.’ (fieldnote, 5 May 2017)
This example demonstrates how each image is scrutinized and discussed. In order to make progress during medical procedures, the medical team need to align their interpretations, and to make qualified assessments in order to discern what the images actually show. If necessary, the medical team produce additional images until reaching the point where they jointly agree that they have achieved a result that they can act upon. However, the experts accept that agreements made on the basis of joint judgements may be overturned whenever new data is provided.
Even though the radiologists were experts in the imaging technology, they also needed to learn how to read and interpret intra-operative images, requiring consideration to be paid to certain aspects of surgical practice. Quite often, the radiologist and the surgeon sit together in front of a screen to discuss what they are observing in an image. One radiologist explains the procedure thus: We need to be humble when addressing what we actually see. So, it isn’t uncommon for us to get involved in a good discussion in the OR. From these discussions, a collective and joint judgement emerges, based on both what the neurosurgeon has observed in the operation wound and on what I have observed in the images, and we jointly determine what the image might plausibly represent.
During their discussions, the doctors move away from their individual interpretations, based on experiences and established knowledge claims, toward explanations which they can act upon. Thus, they need to make their interpretations explicit, and they also need to be open about negotiating around them in order to reach a joint agreement (see also Sachs, 2020). Through these discussions, the medical teams not only learn how to interpret and explain intra-operative imaging, they also learn how to make joint judgements based on information from various sources. They develop a joint capacity to recognize and understand the epistemic and practical uncertainties, requiring a readiness to (re-)negotiate around what the images show and sometimes also a readiness to question the team members’ assumptions.
This means that the technologies do not produce straightforward ‘objective knowledge’. Instead, they produce new data that must be interpreted and explained in order to be acted upon in situ. Thus, there is room for some subjectivity when clinically assessing the image (Burri, 2013), which needs to be complemented with trained judgement to make it useful in each specific situation (Daston & Galison, 2010; Galison, 2014). Taken together, the examples above illustrate how using the technology does not automatically lead to the straightforward generation of knowledge, instead reflecting the dynamic interplay between the production and use of images where knowledge is co-constructed in practice (Faraj et al., 2018).
Recognition of images and embedding experiences
Making use of the new technologies not only involved acts of exploring the potential of these technologies, or of exchanging different interpretations of the new data represented in the images. To maintain their credibility, the medical team needed to explain and account for the images, as well as how they were produced. Therefore, the doctors needed to assess and negotiate the significance of the images, and to continuously account for their different interpretations, in order to achieve a shared view of the situation. It is only after an image had been verified and recognized as trustworthy that the users were able to act upon it. Thus, the medical team critically reflected upon, and then documented, their recent experiences in order to be able to reproduce specific successful practices. Their joint judgements generated useful information that served both to expand the repertoire of options available to other medical teams and to reduce some of the uncertainty surrounding the use of the technologies. As the medical procedures carried out in the hybrid ORs continued, it became important to reproduce the activities that were successful in order to develop medical procedures and expand the groups of staff working there. To achieve this, the experiences gained from performing the procedures, even though they were only temporary agreements (see also Fahy, 2018), had to be embedded in practice. This also included refining and updating the algorithms of the technologies.
This embedding of successful activities and experiences unfolded in two main ways: in real time during specific procedures and over time as more procedures were performed. The first way was achieved by internalizing methods of working, which were agreed upon and became taken for granted through repeated procedures. For example, with the new technology, patient positioning became a challenge as it needed to meet the requirements of both the surgeon and the radiologist, in addition to the technological requirements. Achieving this became a critical activity as the issue of how the patient was positioned had direct consequences for the quality of the images being produced, and also because the chosen position could not be adjusted during surgery. One radiologist commented on this issue: We’ve learnt how to get very good quality images, I think. Surprisingly good actually, considering that the patient is in the middle of an operation. It’s been tricky because some patients are positioned a bit strangely, and then the coils [used to mark the tumour] are further away. It’s really crucial that everything’s positioned exactly right in order to receive the signal [generated by the imaging technology] from the right place. We’ve gradually learnt how to position it all, so it’s very important that we know what we’re doing.
Gradually, as additional procedures were performed, the doctors developed a collective understanding of patient positioning, ensuring that specific images were taken in certain situations. Nurses also took part in the discussions, updating the ‘method cards’ with new information and codifying the agreed-upon way of working into brief step-by-step instructions. This device was essential for expanding the groups of staff working in the hybrid ORs. Over time, their work of generating new data and acting upon it in practice became a joint experience that they drew upon when making judgements in new situations.
The second way of embedding successful activities involved the more formal documentation of procedures and how to perform these. This included formalizing protocols for the technologies and adjusting algorithms post-operatively. For example, radiology staff, application specialists and surgeons spent hours in front of their monitors optimizing and formalizing protocols and sequences in order to turn them into systematic instructions for other surgical teams (to make the algorithms work as well as possible). One surgeon explained how, after a number of attempts and reaching a plausible solution, they had begun writing down and formalizing the images that had been deemed the most significant, and in which order these should be generated for different categories of patient: We’ve talked about what kind of tumour it is and what sort of sequences we need to do, and what we might not need to do [so as to produce good images]. We’ve written down all of this kind of information . . . We’re extremely satisfied with the image quality, but it took a long time in terms of effort and work, making adjustments and so on, before we ended up with the best protocol, and feeling satisfied. In the beginning, you just want to make sequences to test, and so on. But along the way, you might be able to slim them down a bit more.
By collaborating over time, the doctors compared and matched new data and experiences, including various contingencies and specific conditions, with previous practical and theoretical experiences. By documenting what they had learned, the medical team produced scripts to be used during the next procedure, sharing these with the medical community. This requires expertise that builds upon material awareness and processual understanding, that is, being able to draw on the past and anticipate the future, mutually adjusting technologies and staff needs in time and space.
Another episode shows how the doctors, after a procedure had been completed, gathered in the control area where several computers are in use. The settings used when producing the images are written into the clinical record, together with comments made by the doctors.
An application specialist from the supplier of the imaging technologies is also present in the room. He’s taking notes. He tells the doctors; I’ll talk to our specialists in Germany tomorrow. Based on what we saw today, I think we need to discuss some other settings, maybe modify and update the software. Moreover, the surgeons emphasized that they also needed to compare the settings of the imaging technology in use on a specific occasion with other similar procedures. One surgeon said: We need to document and save all the imaging material that we get from the procedures in order to analyse the accuracy and benefits of these new imaging technologies.
As their work was part of a research project, the doctors also filled in a specific form used for this type of abdominal surgery. The information was used not only to document the specific procedure, but also to compare and evaluate several procedures to find new ways of combining radiological and optical imaging, and to develop augmented-reality techniques for assisting surgical navigation. The doctors examined outputs to assess whether or not the analyses were trustworthy, then translated certain episodes into more generally valid accounts that could guide them practically in actual situations and be reproducible in the future. This data was also fed back to the algorithms that the technologies depend on. Moreover, the surgeons and radiologists also published articles based on outcomes, which then became conceptual accounts of their experiences, to be shared with the medical field. In this way, use of the technology and the different doctors’ explanations of the outcomes were deemed credible, being manifested in documents which also became accessible to others.
Taken together, the ongoing work done in the ORs entails that the experts, together with the technologies, will continue to produce data which is not yet fully known and which will require ongoing joint judgements in order for these experts to take their work forward (see Knorr Cetina, 2001). Thus, in line with Pakarinen and Huising (2023), we show how the technologies are intertwined with the work of the experts, thus becoming embedded in the nested assemblage of humans and non-humans. In this way, they are enacted as epistemic technologies.
Discussion
The study presented here illustrates how epistemic technologies are used in expert work to produce meaningful outcomes. Drawing upon a longitudinal in-depth study, we show how medical imaging technologies, powered by advanced algorithms, participate in medical practice to produce images that are acted upon in situ to guide surgical procedures. While previous studies provide important insights into how the outcomes of the technologies are used in expert work, the work needed to produce the outcomes in the first place is often overlooked and separated from use. The generation of new data and information is thus treated as both black-boxed and decontextualized. In our study, the users neither treated the technologies as black-boxed solitary entities nor as producers of any straightforward ‘objective knowledge’. Instead, to produce meaningful outcomes involved interaction between the experts and the technologies, other devices and instruments. Use of the imaging technologies was thus dependent on the relational functionality of the assemblage, with these technologies becoming part of the process of constructing new knowledge when acted upon in situ. In what follows, we discuss our findings and spell out our key contributions.
Enacting epistemic technologies into being
By focusing on the work required in order to produce and act upon images, the study illustrates how the advanced imaging technologies were not epistemic per se, instead becoming epistemic through use. During this work, the technologies appeared as open for inquiry and as transforming entities, rather than as stable ones (Rennstam, 2012). Much of the work had to do with preparing the technology to produce images; adapting the assemblage of people, devices and other technologies to the needs of the technology; and adjusting the technology for specific conditions. The medical staff in the hybrid OR routinely faced equipment problems and engaged in situated problem-solving. To deal with, and take the responsibility for the material problems, and to make the assemblage fit together, they engaged in what Lipp (2023, p. 676) describes as ‘endless tinkering, ad hoc improvisation and a kind of localized gathering of knowledge and people’. This work created a relational functionality (Bailey et al., 2022) which both relied on material and situational awareness and provided the experts with the contextualized information necessary in order to produce and act upon the images.
The study contributes to research into the use of advanced technologies in knowledge work by means of highlighting the ongoing work of constructing relational functionality, which was a prerequisite enabling the technology to be enacted as an epistemic one. Use of the technologies thus reflected a process whereby nothing was taken as entirely fixed or fluid (Mol, 2008): Rather it entailed a pragmatic accommodation of the assemblage that the technology forms part of. The assemblage was constructed and kept together by a relationship whereby devices, technologies and people continuously influence each other by acting and reacting in order to serve each other’s needs. The epistemic technology thus participated in the production and elicitation of the experts’ knowledge regarding what to do and how to do it (Schiemer, 2024), not only producing new data but also co-constructing the context and circumstances under which the new data and information were produced.
Moreover, the study thus contributes by highlighting how using the imaging technologies reflected a dynamic interplay between the production and use of images. While Lebovitz et al. (2022), for example, demonstrate that experts interrogate the outcome generated by AI technology, and incorporate AI knowledge claims into their own, our study reveals how medical experts engaged in the interrogation and incorporation of knowledge claims during production as well. Together, they developed a joint capacity to recognize and understand the epistemic and practical uncertainties, requiring a readiness to (re-)negotiate as regards what the images show and sometimes also a readiness to question the team members’ assumptions. The imaging technologies, acting as epistemic ones, were thus supplemented by the experts’ ongoing joint judgements, taking not only established knowledge claims into account, but also the relational and heterogeneous assemblage they were part of. The participants in the assemblage were related to each other by the function they were performing, and also by ongoing judgements regarding the significance of their actions. Thus, if the assemblage where work was being done was not being held together by relational functionality, then the technologies would be less useable or would fail (see also Pakarinen & Huising, 2023).
Algorithms and contextualized information
This study illustrates how the production of images was conditioned by means of the technologies integrating both digital and physical qualities: Making the algorithms work (to produce images) required tinkering with the material aspects of the assemblage. The ongoing work of constructing relational functionality, which relied on a material and situational awareness, provided the medical staff with contextualized information.
The work of preparing the assemblage in the OR was done in order to make the algorithms produce the best possible images for guiding surgery. Even though the algorithms were opaque to the users, our study illustrates that the ongoing adaptation of, and tinkering with, the assemblage of devices, other technologies and people in the OR, in order to fit with the needs of the technologies, played a significant role in the production of the outcomes. Thus, in contrast to, for example, the investment bankers in Anthony’s (2021) study, who evaluated the outcomes from algorithmic technologies without any knowledge of their generation, we show how knowledge of the way in which the new data was produced mattered when it came to interpreting and evaluating the outcomes.
Previous studies of algorithmic technologies have often treated the generation of new data as both black-boxed and decontextualized. These studies do not take into account the specific circumstances under which the outcome is produced, or the fact that the inputs to the algorithmic technologies consist of data produced elsewhere, and by someone else; for example databases of images are produced by radiologists, or statistics and crime reports by police officers. Thus, they separate the production and use of the outcomes: The contextual aspects of these inputs are not addressed, accounted for, or integrated into the recognition and validation of the outcome.
The study contributes to research into the use of algorithmic technologies in knowledge work by showing how opaque algorithms, as well as the lack of explainability regarding how the outputs are produced (Anthony, 2021; Pakarinen & Huising, 2023), can be complemented by contextualized information about production. Instead of focusing on the transparency of the algorithms, this study focuses on the situational aspects and circumstances under which the algorithms work. In line with the study of Kaplan et al. (2017), of the ongoing generation of nanotechnology knowledge emerging from interaction between scientific actors and instruments, our study highlights the fact that we cannot separate outcomes from insights into their production. In line with Kiviat’s (2019) observation, we found that when experts were unsure how the technology had produced a specific outcome, they actively contextualized it through their own interpretations and explanations. We thus contribute to recent studies of algorithmic technologies, mainly calling attention to the outcomes of technologies, by illustrating how the circumstances of production were integrated with the interpretation and use of the outcome. Thus, the black box of the algorithm does not necessarily need to be opened to create trustworthy outcomes: Instead, it may be complemented by contextual knowledge.
Trained judgement and enacting epistemic technologies
When enacting the epistemic technologies, the medical staff engaged in ongoing and joint judgements during both the production and the use of images. During the medical procedures, they discussed disagreements over the data (the image) and made their interpretations explicit by linking the new data to their existing knowledge claims and also to their contextualized knowledge of how the image was produced. This revealed how the surgeons and radiologists engaged in collective assessment and interpretation in order to make the data useful in each specific situation, what Daston and Galison (2010) describe as trained judgement. The medical experts using the imaging technologies did not treat the data produced as an objective output (knowledge claim) to act upon: Rather, they agreed upon what they considered to be the right course of action for the specific situation.
Trained judgement was thus a joint achievement, which allowed subjectivity when clinically assessing images (Burri, 2013; Carragher, MacLeod, & Camargo-Plazas, 2021) and acknowledged the fact that the data was situated and open to various interpretations (Pantzar & Ruckenstein, 2017). The images were thus treated as a ‘matter of concern’ rather than a ‘matter of fact’ (see Latour, 1999), and interpretations were dependent on the contextualized information about production. The experts accepted that agreements made on the basis of joint judgements could be overturned whenever new data is provided. Engaging in trained judgements thus included moving away from individual interpretations toward explanations and joint judgements, in search of temporary agreement (Fahy, 2018).
The study also illustrates how trained judgement formed part of creating and maintaining relational functionality. It involved considering the context and background assumptions prescribing which parts of the assemblage were relevant, and how these parts were related to each other. However, these interactions and temporary stabilizations did not lead to a transformation of the epistemic technology, whereupon it became taken for granted and functioned as a technical object, as shown in McGivern and Dopson’s (2010) study, for example. Rather, the technology was the subject of creative engagement when producing images, but faded into the background (see also Schiemer, 2024) when the surgeons and radiologist reached a plausible understanding of the image and moved on as regards surgery. However, as they were continuously producing new information, the algorithms needed to be adjusted, modified and updated from time to time: By using the technologies collaboratively, they jointly developed knowledge (Ewenstein & Whyte, 2009).
Taken together, our study shows how the medical experts made judgements during production in order to deal with non-routine issues and seek solutions outside the realm of their established expertise. We thus contribute to previous studies of the role of judgement when using advanced technologies by illustrating how judgements were not only made in relation to outcomes, but also throughout the process of using the technologies, when making the technologies ready for use and agreeing upon which information was recognized as trustworthy in each specific situation. Trained judgement thus became a significant part of the work the experts engaged in when confronting non-routine problems and produced new data by means of interactions within a relational and heterogeneous assemblage of people, technologies and devices.
Concluding Remarks
The use of advanced technologies generating new data and information, including algorithmic technologies and AI, requires an awareness of the co-constitution of the technology, and the practice in which it engages, in order to understand how technologies play a part in the ongoing construction of knowledge.
Inspired by STS-oriented studies (e.g. Knorr Cetina, 1997; Rennstam, 2012), we have tried to widen the perspective of epistemic technologies by showing that they are dynamic and emerging in the sense that they are ambiguous and incomplete, and also that they are being intertwined with ongoing judgements in order for their potential to be realized. Hence, there are no technologies that are epistemic ‘by nature’, only technologies which function, in a particular time and place, as epistemic technologies. Thus, we contribute to the emerging organization studies literature on epistemic technologies by showing how these only become epistemic on the basis of how they are enacted, due to the new data not becoming meaningful and practically useful, and thus recognized as trustworthy, until the experts engage in joint judgements.
Moreover, the study advances our understanding of how judgement is intertwined with the ongoing use of these technologies. While previous studies have focused on judgements needed by experts in order to interpret and incorporate the output and data being produced by epistemic technology, we add to these studies by illustrating how judgements also take place during the actual production of the data and the knowledge claim. By drawing upon the notion of trained judgement, our study contributes toward understanding judgement as an ongoing and jointly performed process, instead of treating it as a cognitive and individual process (see Styhre, 2013).
We encourage future research to take our insights further by addressing other professional contexts and other types of epistemic technologies and to examine how technologies arrive at a particular output. We suggest that researchers pay particular attention to technologies that integrate both the digital and mechanical qualities, and how AI and algorithmic technologies manifest themselves physically, interacting with humans and physical objects. To capture such processes, we propose ethnographically inspired studies that enable an understanding both of these technologies and of how their interconnected practices evolve over time.
Footnotes
Acknowledgements
We would like to thank the senior editor, Peter Fleming, and three anonymous reviewers for their time and helpful feedback. Their insightful and constructive comments have been crucial when revising the paper.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kajsa Lindberg and Alexander Styhre would like to thank the Wallander and Hedelius Foundation (P19-0121) for its support of the project “Robotic surgery, visualization and the work of experts”. Daniel Tyskbo would also like to thank the Wallander and Hedelius Foundation (W20-0033) and the Knowledge Foundation for their support.