
Abstract
The theory of organizational path dependence helps us to understand why organizational change is sometimes extremely difficult, if not impossible. Although recent conceptualizations of path dependence allow for strategic agency, the theory is still underspecified regarding how to break an organizational path. In an attempt to develop the theory in this regard, we make use of a case in the sphere of global health with an undisputed life-saving impact. More precisely, we trace a significant improvement in the field of pediatric cancer care back to path-breaking organizational change: the successful introduction of multicenter cooperation within a healthcare system that is arguably locked into a centralization path. Drawing on longitudinal research conducted within Russian children’s hospitals, we conclude that path-breaking change is an intricate process based upon distinct activities, and supported by mechanisms, directed towards the creation of a new organizational path.
Introduction
Organizational change is an important issue in management research and practice. Nevertheless, the circumstances that make organizational change or restructuring difficult if not impossible do not seem to play a major role when looking at practitioner-oriented change models or into scholarly research that is used to substantiate these models (Stouten, Rousseau, & De Cremer, 2018). This is quite surprising, given the extensive reports on failed change initiatives and the fact that at least two well-established streams of research convincingly demonstrate that organizations, especially when large and old, exhibit rigidities known as either structural inertia (Hannan & Freeman, 1984) or strategic persistence (Lant, Milliken, & Batra, 1992). Path dependence theorists even go one step further by arguing that, under specific circumstances, organizations may not only be rigid, but even “locked-in” (David, 1985). Based upon the seminal works of David (1985) and Arthur (1989) on technological path dependence, as well as upon more recent contributions by David (1994), North (1990), and Pierson (2000) on institutional path dependence, the theory of organizational path dependence has been developed to explain such hyperstabilities of organizations and interorganizational arrangements (Dobusch & Schüßler, 2013; Koch, 2011; Lamberg, Pajunen, Parvinen, & Savage, 2008; Perchard & MacKenzie, 2021; Maielli, 2015; Sydow, Schreyögg, & Koch, 2009; Wenzel, 2015).
While most of these more recent conceptualizations of path dependence ultimately consider change possible (see also Bækkelund, 2021; Djelic & Quack, 2007; Garud, Kumaraswamy, & Karnøe, 2010; Law, 2018; Thrane, Blabjerg, & Møller, 2010; Valorinta, Schildt, & Lamberg, 2011), one pressing question has so far remained by and large unanswered: How can such path dependencies actually be broken? To approach this question, we need a theoretical understanding of path-breaking organizational change that, per definition, is of a transformative nature (Karim & Mitchell, 2000). This understanding can build on recent conceptualizations of organizational path dependence, but needs to go beyond simply assuming the restoration of organizational choice (Sydow et al., 2009).
Equipped with such theoretical considerations, we searched for organizational phenomena that may be interesting to look at in this light. Former Soviet Union countries have traditionally been an important field of applying path dependence theory to explain the difficulties of transformative change (North, 1990; Stark, 1991). By pure chance, when traveling back from another potential empirical project in Russia that failed because of denied access, the first author was introduced by a former medic from Charité Berlin to Russian healthcare as an interesting field; a field that is not only of vital importance for the country (to which persistently low life expectancy is attributed), but that additionally exhibits strong organizational persistence. Together with this expert, who is now a representative of a German-Russian medical forum, success stories involving organizational change in this country were screened for. The only case of apparently transformational organizational change that we were able to identify together occurred in a subfield of cancer care: the treatment of childhood acute lymphoblastic leukemia or ALL, a frequent form of blood cancer among children and a common cause of death for under 18-year-olds. Despite persistent overall centralization, considered to have been one of the major problems, the first and hitherto only multicenter cooperative group was established and later named the Moscow-Berlin or MB Group. As a consequence, and in sharp contrast to developments concerning all other oncological diseases, this group has been able to produce unprecedented treatment results across Russia: The survival rate of this disease, terminal without proper treatment, has soared nationwide from under 10 percent in 1990 (Karachunsky et al., 2008, p. 1) to over 80 percent today (see Appendix A; all appendices are available in the Online supplemental material of the article). This success within a healthcare system otherwise in general stagnation (Gontmakher, 2015) has puzzled the scientific community. Explanations of this “miracle” under such difficult conditions have been published in leading medical journals and have won several prizes. These focused entirely, however, on medical questions regarding the achievement of these results: more than 4,800 children have now been fully cured and are living normal lives (see Appendix B), many of them meanwhile even with children of their own.
We will demonstrate that not only medical advancements, but also organizational change, were crucial for this success. What is more, the former, to some extent at least, would not have been possible without the latter, and vice versa. Theoretically, the case led us in a first step complement path dependence with path creation theory that puts more emphasis on agency (Garud & Karnøe, 2001; Garud et al., 2010; see also Holmen & Fosse, 2017; Jing & Benner, 2016; Law, 2018; Sydow, Windeler, Schubert, & Möllering, 2012). Furthermore, as we understood, the organizational change from centralization to decentralization—to which we attribute a good part of the improvement in this particular subfield of cancer care—was gradually introduced over a considerable amount of time. This makes us argue that a focus is called for on the related activities and mechanisms and their intricate interplay over time to understand such path-breaking organizational change as process.
Our argumentation begins with a brief introduction to path dependence and path creation theory and its present difficulties to address change. The section that follows provides insight into our longitudinal research design and method. Our findings focus on path-breaking organizational change in the field of ALL, in particular on the activities necessary as well as the mechanisms working in favor of this change. Finally, we discuss the implications of the findings for theory elaboration and develop a process model of path-breaking organizational change. We conclude by connecting our insights to current theoretical advances regarding organizational stability and change in general, and in organizational institutionalism as arguably the most important theory of organization in particular.
Theoretical Background
Paul David (1985) was the first to study and theorize path dependence by showing how the course of history can lead to multiple, possibly inferior outcomes—rather than just to one optimal solution governed by rational choice. Using the now famous example of the Qwerty keyboard, David demonstrated that a whole industry, despite the rational decisions of individual actors, can be driven to adopt an inferior system (see also David, 2001). The argument gained even more prominence in economics and social sciences when North (1990) and, shortly thereafter, Stark (1991) used the concept to analyse institutional change in Eastern Europe. Significant theoretical advancement can also be attributed to political scientists such as Pierson (2000) or Crouch and Farrell (2004), who, among others, introduced strategic agency into the theory and therefore went beyond the bounds of only following the path emphasized by the theory’s originators. With a similar aim in mind, Garud and Karnøe (2001) developed their theory of path creation, emphasizing not only strategic but also distributed agency within the structures that actors have created, reproduced and/or transformed (see also Djelic & Quack, 2007).
Organizational path dependence and path creation
On the basis of these influential works, more recent theorizing has taken the discussion to the organizational level of analysis. Sydow and colleagues (2009) adopt the social constructivist perspective taken by Garud and Karnøe (2001) and position their approach between conventional path dependence theory on the one hand, which reduces agency to following the present path, and the more recent conception of path creation on the other, emphasizing not only structured but also structuring agency for creating and maintaining a path (see also Garud et al., 2010). Organizational path dependence, and by implication an organizational path, is defined here as “a process that (1) is triggered by a critical event leading to a critical juncture; (2) is governed by a regime of positive, self-reinforcing feedback constituting a specific pattern of social practices, which gains more and more predominance against alternatives; and (3) leads, at least potentially, into an organizational lock-in, understood as a corridor of limited scope of action that is strategically inefficient” (Sydow et al., 2009, p. 704).
The theory of path creation, in sharp contrast to Arthur and David’s theory of path dependence, follows a constructivist rather than a positivist ontology and emphasizes strategic agency. Its relational understanding of agency includes the ability of individual and collective, yet mostly distributed agents not only to shape an existing path, but also to create a new one by “mindful deviation” and “disembedding” from structures (Garud & Karnøe, 2001). This constructivist turn is, for one, reflected in the insight that “what is endogenous and what is exogenous is not given. Rather such a demarcation depends on how actors define their boundaries at various points in time” (Garud et al., 2010, p. 766). For another, it acknowledges that “initial conditions are not given but rather constructed by actors who mobilize specific sets of events from the past in pursuit of their initiatives” (Garud et al., 2010, p. 769).
Starting from a conceptualization of path creation that contrasted with the classic theory of path dependence, paths have since been conceptualized as being socially constructed, unfolding processes that endogenize material objects, relevance structures, and event time. These processes, although driven by strategic agency, involve exactly the same self-reinforcing mechanisms alluded to above; mechanisms such as complementarity and coordination effects, that imply the seed of path dependence (Garud et al., 2010; Sydow et al., 2012). Thus, path creation with its emphasis not only on deviating and disembedding, but also on generating momentum, always involves change, but not every change leads to the creation of a new path characterized by self-reinforcement.
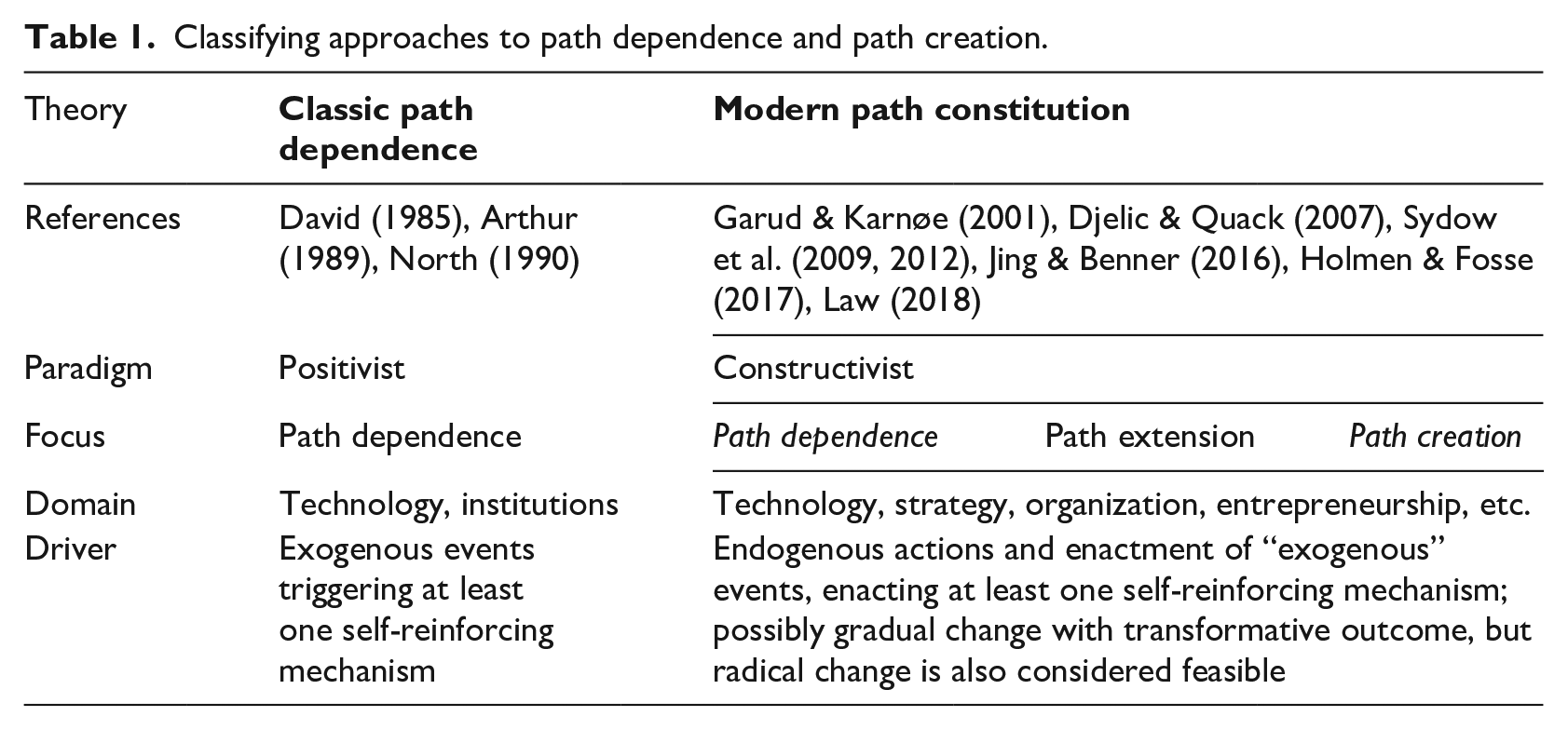
We subsume such recent works on path creation and dependence (as well as some connected literature on path extension, cf. Sydow et al., 2012) under the label “path constitution” (see Table 1). Due to their common ontological roots, we contrast them with classic path dependence that, particularly in the work of Arthur (1989, 1994), rests on positivistic roots inherited from economic theory. To date, however, even such advanced approaches do not specify how paths are likely to be broken.
Classifying approaches to path dependence and path creation.
Towards conceptualizing path-breaking organizational change
Even though numerous studies of technological, institutional or organizational paths assume the possibility of change (Araujo & Harrison, 2002; Djelic & Quack, 2007; Garud et al., 2010; Kalasin, Dussauge, & Rivera-Santos, 2014; Thrane et al., 2010), little research has so far explicitly addressed the activities and mechanisms required to make change possible under the adverse conditions of path dependence. One of the few exceptions is to be found—and quite prominently so—in classic path dependence theory, which points to the need of an external shock or crisis. More recent path constitution theories, by contrast, point to the potential of strategic agency and the enactment of “exogenous” events in a way that affects the working of at least one self-reinforcing mechanism (see, once again, Table 1). These two complementary approaches are obviously not new to studies of organizational development and change (cf. Burke & Cooke, 2012), which, however, rarely address organizational path dependence in this narrow sense of hyperstability. On the other hand, path dependence theorists not only held on for a long time to the need for external shocks. Rather, even in light of the more recent acknowledgment of the importance of strategic agency and the possibility of more than on-path (path-dependent) change, these theorists remain skeptical about the possibility of escaping an organizational path that is governed by self-reinforcement or positive feedback (e.g., Sydow et al., 2009).
Some path theorists have nevertheless already started to approach the question of how to escape an organizational path. They have done so, for instance, by emphasizing that collaborative organizational forms may counteract an existing path (Law, 2018; Sydow et al., 2012). Others point to “the dialectic between path dependence and path creation” (Mouritsen & Dechow, 2001, p. 358), or the importance of “vicious co-evolutionary cycles” (Garud & Karnøe, 2001, p. 25). Thereby, these theorists highlight necessary elaborations but even those concerned with the generation of a new path do not specify that an existing path needs to be “broken” and how this is done; although the availability of a viable alternative and external pressure is considered to be helpful (e.g., Djelic & Quack, 2007). Still others contribute to the debate by arguing that the creation of a viable alternative requires a separate process (Rothmann & Koch, 2014), or by distinguishing “change agency” from “reproductive agency” (Bækkelund, 2021). Change agency is ascribed a transformative capacity, allowing, in principle at least, for not only incremental on-path, but also path-breaking change. But a convincing account of organizational change under the adverse conditions of path dependence is still missing.
As already mentioned, organizational rigidities are—far beyond organizational path dependence research—widely addressed in the management literature, in particular as structural inertia (Amburgey, Kelly, & Barnett, 1993; Hannan & Freeman, 1984) or strategic persistence (Audia, Locke, & Smith 2000; Lant et al., 1992). Even literature that focuses on organizational development and change (rather than continuity), with the help of participative, dialogical or collaborative approaches (cf. Burke & Cooke, 2012), acknowledges the existence of such forces, though these are often overhastily conceived as causing resistance to change. However, none of these approaches analyses the rigidities that result from path dependence with its specifics of hyperstability, driven by positive feedback and therefore extremely hard to overcome. This is even true for most of the studies that, like Pettigrew’s (1985), leave the often a-contextual, a-processual and a-historical research on organizational change far behind (Sminia, 2016).
A more precise conceptualization of activities and mechanisms, building on path constitution theory, therefore promises to promote the understanding of organizational change under the particular adverse conditions of path dependence. For theorizing what we thus refer to as “path-breaking organizational change” we conceive activities, with a temporal-relational ontology (Emirbayer & Mische, 1998) in mind, as resulting from social (inter-)action, enabled as well as constrained by structure (Giddens, 1984); a process in which not only choice but also chance plays a role (Child, 1997; De Rond & Thietart, 2007; MacKay & Chia, 2013). Mechanisms, which have been considered as stabilizing elements in path dependence research right from the start (Arthur, 1989, 1994), currently re-enter research as a structuring element for change processes (e.g., Gray, Purdy, & Ansari, 2015). Thereby, mechanisms, in the case of path dependence, particularly those of a self-reinforcing nature governed by positive feedback (Sydow et al., 2009), link activities to outcomes. From a constructivist perspective, however, such mechanisms cannot be considered without the activities that enact them in practice to understand the interplay between stability and change in organizational processes. In view of these theoretical specifications, our two-part research question reads as follows: Which activities facilitate breaking organizational path dependencies? How do these activities relate to each other as well as to self-reinforcing mechanisms that are usually held responsible for creating such dependencies in the first place?
Research Design and Method
For the purpose of theory development or elaboration (Fisher & Aguinis, 2017; Vaughan, 1992), the case study method—across epistemological and methodological differences—is considered to be the method of choice in management and organization research, in particular for process research, as it provides details on how the underlying dynamics of the phenomena in question play out over time (Langley, 1999; Pettigrew, 1990; Yin, 2014).
Longitudinal case study design
Path dependence research has been based traditionally on counterfactual analysis (David, 1985), i.e., arguments were developed for a possible alternative path of history. Our research setting, however, allows an already existing alternative to be considered, i.e., “multicenter cooperation” within the specific subfield of ALL. The term is derived from the medical discourse and refers not only to organizational, but also to spatial decentralization (see, for example, Guttmacher, Marchuk, & White Jr., 1995). Spatially decentralized subunits of the Russian healthcare system, here the wards or centers where the young patients with this disease are actually diagnosed and treated, started to coordinate their activities in a cooperative manner, gradually replacing the dominant logic of centralization.
To capture such a process over a long period of time is highly resource intensive. Choices regarding research sites and time spent in the field were thus crucial to ensure realizability. This also holds true in the case of the MB Group, a team of medical personnel employed by hospitals and involved in cooperatively diagnosing, researching and treating ALL on the base of a joint protocol and spanning the largest country in the world over more than 25 years. From the 59 wards it included in 2020, disregarding the study center that supports the coordination of the network, four wards were ultimately selected as research sites for the empirical study to enable the best possible coverage of its variety. The final sample covers four of the eight federal districts into which Russia is divided (see Appendix C) and, to the highest degree possible, the geographic extension of the network. Furthermore, it balances large cities and more provincial areas. With respect to facilities, different categories and sizes of hospitals in Russia are taken into consideration (see Appendix D). To account for the development over time, subunits of the network were selected to cover the timeline from the first ward (1991) up to the real-time observation of the accession of a further ward in 2010, in order to counter the bias of retrospective analysis in the best way possible (see Appendix E). With a similar aim, our longitudinal study of organizational change includes fieldwork conducted at four points in time: 1998–2000, 2009–2011, 2015–2016, and 2019–2020.
Data collection and analysis
Data were collected with the help of recorded interviews, ethnographic protocols, Internet research, archival documents, and medical statistics, allowing validity to be enhanced by triangulation (Jick, 1979; Yin, 2014). While interview data for the first period stem from a secondary source, later data were collected by the first author. Interviews were semi-structured and conducted in Russian, with the exception of interviews with the German actors who supported the development in Russia at the beginning of the 1990s. The first author had prepared an interview guideline which was then translated into Russian by a native speaker and adapted, depending on the situation and respondent. In total, 46 interviews were recorded with 34 respondents. They lasted between 45 minutes and more than three hours. The sample of respondents encompasses the German actors who were supporting the MB Group at the beginning (one professor, head of ward; one assistant medical director, and the head of a German charity fund). In Russia, medical professors, study center employees, heads of wards, doctors, head nurses, and psychologists were interviewed at the selected research sites. To understand as much as possible about the historical context, additional interviews were conducted with doctors in the “Oncocenter,” the entity responsible for centralized pediatric ALL research and treatment in Soviet times, as well as with experts working in leading positions in the Russian healthcare administration. The interviews from a secondary source were conducted by a Russian sociologist from 1998 to 2000 within the three wards in Moscow where multicenter cooperation started. The transcripts available to us were initially intended for use in a book which aimed to generate funding for the MB Group, a project that was never completed. In total, 17 protagonists were interviewed at that time, diminishing the potential bias of a retrospective analysis.
In addition to interviewing, the first author conducted further extensive fieldwork. We are referring to the use of this data source here as ethnographic technique, following contemporary efforts to use ethnography in organizational research (Zilber, 2014). Originating from anthropology, ethnography proves to be promising, especially in foreign cultural environments. The most important difference between this method and other forms of observation can be understood as being “to be rather than to see a member of the organization” (Van Maanen, 1979a, p. 539). The first author was allowed to gain first-hand understanding by living within this foreign environment for a total of three months over a period of two years. In the study center, he was able to learn intensively about the different steps of protocol treatment, and followed up on the daily work supporting the exchange between the participating hospitals before being exposed to patients. He was offered the desk of an absent doctor, worked on his computer as other doctors did on theirs, and discussed what he had observed during coffee breaks. This gradually became part of their daily routine.
In order to understand a wide variety of different developments, diagnosis and treatment of the disease within a short period of time, one large ward in Moscow was selected as the first hospital ward. Having learnt in principle how protocol treatment works in the study center, the first author followed up on what this meant with regard to practical work with patients. From the first day onwards, he was given a white doctor’s overall by the chief physician and introduced to the patients’ parents as a colleague from Germany. Consequently, he was able to shadow the doctors (cf. McDonald & Simpson, 2014). His first day of work was scheduled to start on the same day as that of three new assistant doctors. Following them in their first practical steps of training to be a doctor, he visited the patients with them, was present when they administered pharmaceutics, and even during minor operations. He was there afterwards when they discussed the patients in the doctors’ room with colleagues, and made his field notes when they learned patient histories by heart and made notes for their patient files; the main difference was that he did not have any patients of his own. Learning with them how chemotherapy treatment was administered and understanding “through their eyes” how they were socialized was an important aspect of our empirical work. This condensed in-depth insight in a large ward secured sufficient understanding of chemotherapy and helped to put data into context that were collected later on in smaller regional wards. In total, 307 handwritten pages of field notes were collected, mostly written in German, but also in the Russian language.
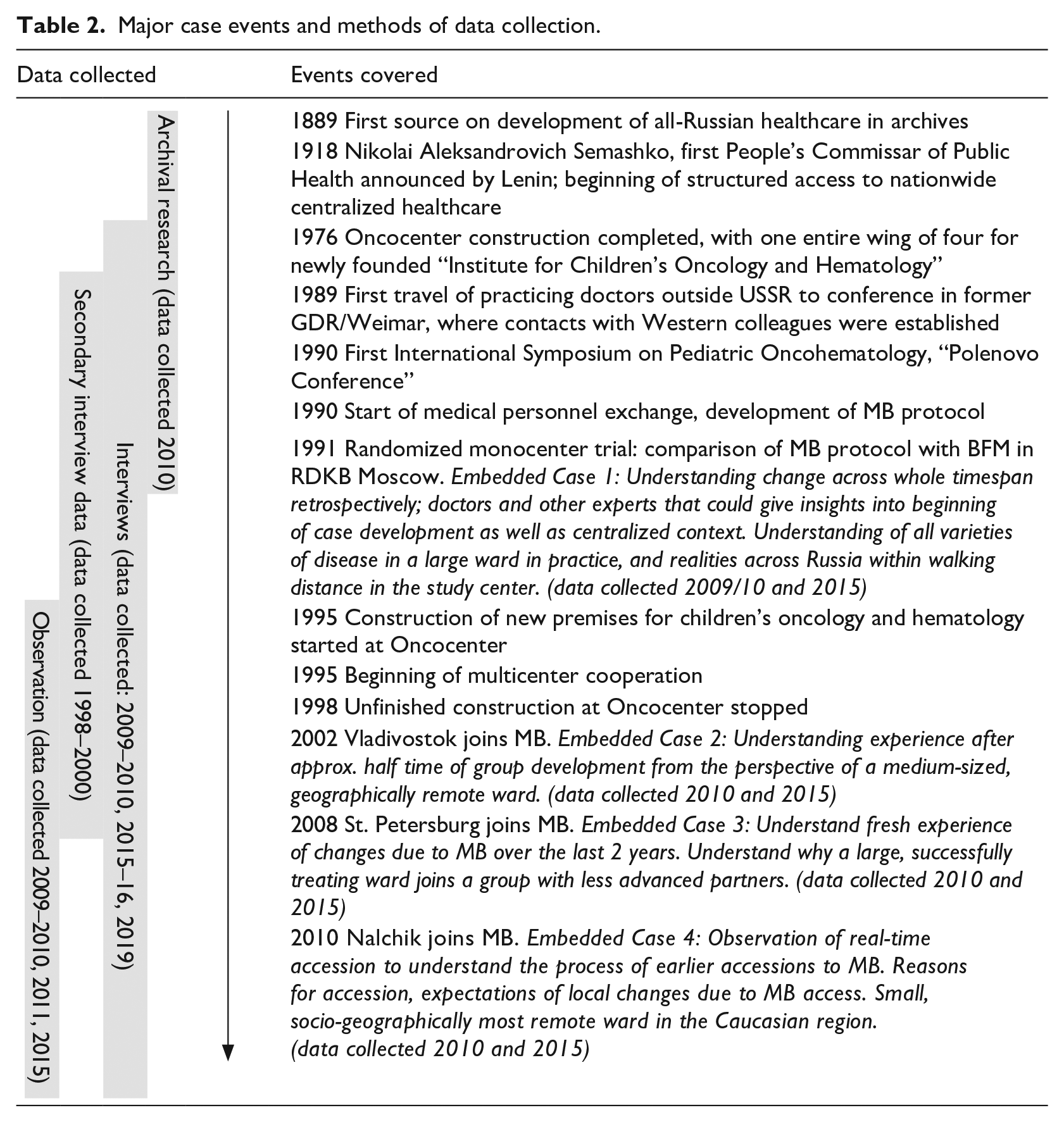
In preparation for research in the field, intensive Internet research was conducted on sources relating to healthcare in Russia. The associated documents include donor information from the small German NGO supporting the project, information about the historical development of the MB Group and its context, seen from the perspective of that time, and documents about the development of Soviet (later Russian) pediatric oncohematology. Archival work in the Pirogov Russian National Research Medical University completed the picture of the latter. In total, 3,192 pages of historical documents were digitalized. This material was screened in an order that focused first on the development of Russian healthcare in general, then on the field of oncology/hematology, and eventually specifically on pediatric oncohematology in documents ranging back from the first available ones depicting early attempts to establish nationwide care in 1889. In addition to that, the first author was given unlimited access to the medical study data of the MB Group. Table 2 gives an overview of major case events and methods of data collection.
Major case events and methods of data collection.
Using ethnographic technique means that data collection and analysis are not separated entirely (Van Maanen, 1979b, p. 521). During fieldwork, the ethnographic technique and formal, recorded interviews proved to complement each other and supported our endeavor to understand organizational change in both an alien environment and a foreign culture. New questions emerging during the first author’s extended presence in the field were entered into formal interview guides to enable their continuous further development. At this stage, field notes enabled the author to recall the setting in which he wrote down his observations and provided informal background information, without which a Western researcher would not be able to understand organization in Russia. Additionally, the recorded material has made it possible to adhere to the actor’s original (though translated) wording and now enhances the transparency of our own conclusions.
The interviews (primary and secondary data) that referred directly to the interactions within the MB Group at specific stages of development (n=21) were coded in full. Analysis was conducted with the help of the qualitative data analysis software Atlas.ti, which enabled transparent uniform coding across single transcripts. Coding followed an iterative process, aiming to connect statements with path dependence and creation theory. For example, the original statement “And so our practical collaboration started [. . .], showing astonishing results. By 1997 we had reached a survival rate of 76.5% for children with ALL—and that in Russia!” from an interview with a high-ranking official in Russian healthcare administration would be subsumed under the label “communicating an improved organizational solution.” The interviews cover organizational change within the subunits as well as specific aspects of history or context—and were therefore analysed partially regarding these specifics. In a similar way as when using grounded approaches (Glaser & Strauss, 1967), we used insights from the field to elaborate theory. In particular, we made use of temporal bracketing and ordered sequences of activities and mechanisms to mold a process model (Langley, 1999). Overall, our interpretive methodology is based upon abductive reasoning (Alvesson & Kärreman, 2007; Mantere & Ketokivi, 2013) and, because of the complexity of the case, the report of the findings follows a conceptualized (rather than inductive or model-led) composition (Berends & Deken, 2021), arranged in phases taking time and temporality seriously. For utmost data transparency, we present the details of our interview and ethnographic data on activities in Appendix F.
Documents, Internet research and archival work were used to triangulate with the interview and ethnographic material, and to reconstruct the specific development of the context starting with the October Revolution (see below). To understand the specialty of pediatric oncohematology as a whole, a timeline—from its creation as a sub-discipline in the Soviet Union (set in 1951) up to the present day—was developed and discussed with contemporary witnesses, going as far back in time with them as possible. Quantitative data from the medical study entered the rationale for the selection of research sites and helped to demonstrate improved results in multicenter cooperation.
Findings: Path-breaking Organizational Change in Russian ALL Care
If we refer to organizational change as being a “path-breaking” occurrence in this context, we need to demonstrate that it took place under conditions of path dependence. For that reason, a brief historical account of the path-dependent development of the Russian healthcare system is given in Appendix G. Here, we will focus on path-breaking organizational change (see Figure 1).
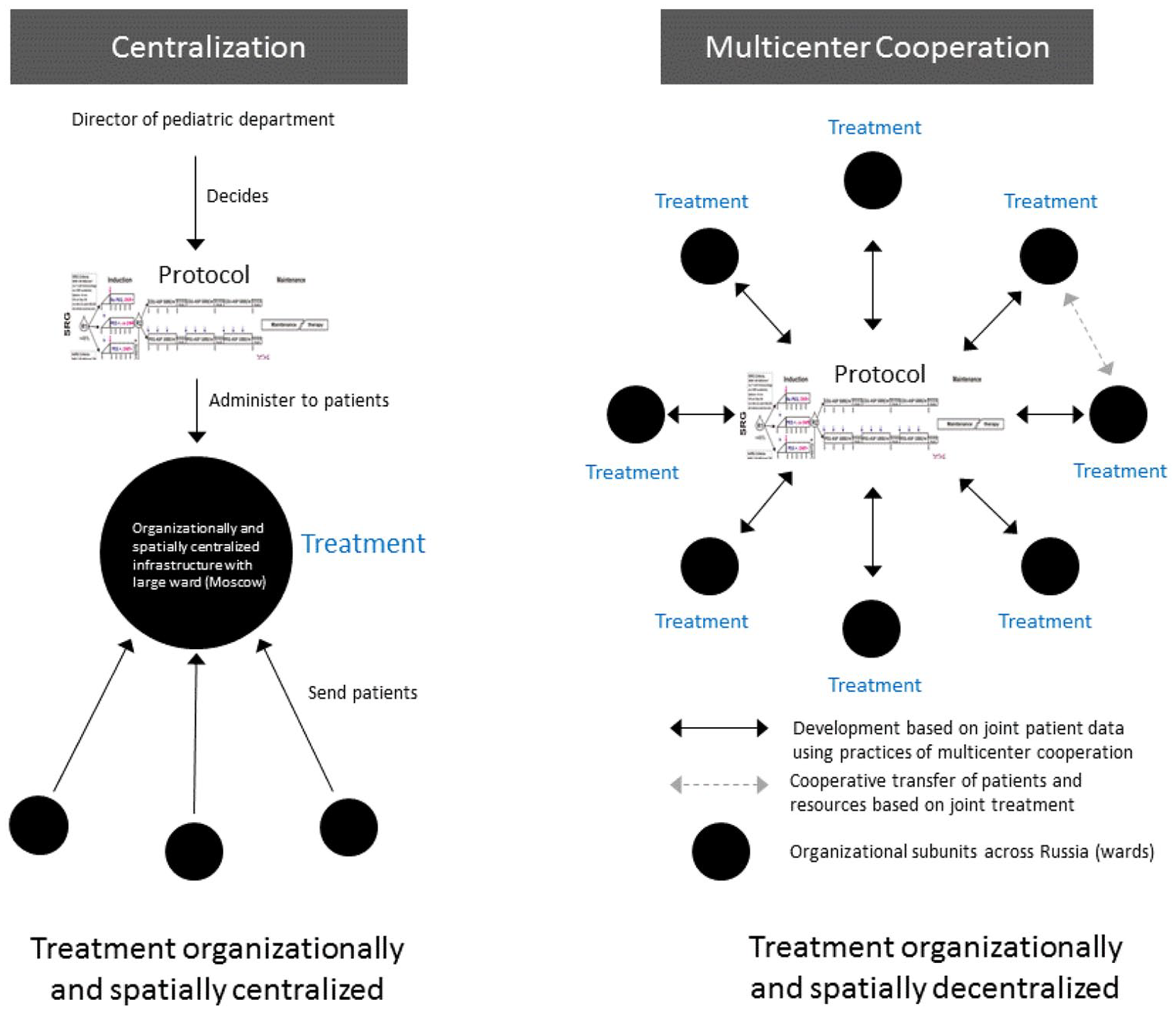
Comparison of the “old” and “new” organizational solution.
Path-breaking change in the case of ALL
Looking for empirical insights that may help to develop path constitution theory further with regard to path-breaking organizational change, we aimed at identifying activities and mechanisms that drove the change process under the adverse conditions of the Russian healthcare system. For reasons of clarity and abstraction (Langley, 1999), we order them into three stages characterized by distinct sets of activities: (1) reflecting with an external lens; (2) enacting self-reinforcing mechanisms; and (3) communicating a superior organizational solution. While several activities are important in each stage, we argue that there are certain “leveraging activities.” Such activities are more impactful than others, not least because they increase the influence of other activities to bring about path-breaking organizational change.
Reflecting with an external lens
In the early 1990s, after decades of isolation, the Iron Curtain suddenly became permeable. A different context appeared enabling comparison and reflection. With reference to Russian pediatric oncohematology, a rather sudden change in what had hitherto been taken for granted in the field can even be traced back to a particular conference in Polenovo near Moscow in January 1990. Following decades of isolation, Western experts (from Scandinavian countries, Israel, France, the United Kingdom, the United States, and Germany) were invited and more than 300 doctors from over 90 regions and provinces of the former Soviet Union participated in a professional exchange. To adhere to the example of ALL, “an analysis of long-term survival within the Soviet Union had been conducted in 1989 and is reported to have shown a survival rate over 10 years of 6.7 percent” (of the children who had managed to make it to the centralized cancer organization in Moscow). In other words, over 90 percent of the children with ALL died in the USSR. And then they heard that in Germany, for instance, over 70 percent of these children were being cured and “the survival rate for some forms of lymphoma is 100 percent” (as one of the organizers of the conference recalled). These results were obviously not merely Western propaganda and were confirmed by experts with whom attendees could talk about their work during discussions and afterwards in private. According to witnesses, there were Soviet participants who cried; for some, the achievements of a lifetime had been brought to naught; the immediate necessity to catch up quickly became consensus. Russian experts were now allowed to visit conferences abroad. Doctors and nurses went for internships to Western hospitals. Western doctors, in turn, visited Russian clinics giving advice, and pharmaceutics were even sent from Western countries. The idea was to enable “the same” treatment in Russia. These efforts represent an activity of applying general medical knowledge from other contexts, here relating to ALL treatment.
As a second more specific activity, Russian doctors were trained abroad to apply specific treatment standards from other contexts and subsequently use them in Russian wards. It was assumed that the most modern of these standards, here treatment protocols (see Appendix J) embodying current state-of-the-art best practice knowledge, were the key to quickly raising Russian ALL treatment to the international level. “Western doctors [. . .] distributed those protocols there like cooking recipes,” as a German doctor involved in Russia at the time remembers. Interestingly, even down to the terminology used, this is reminiscent of Stark and Bruszt’s (1998) criticism of “cookbook capitalism” in other spheres of Eastern Bloc societies at that time: “You do that—that’s good, that is how we get our kids healthy, too.” And they did exactly that. That was the beginning of the 1990s, and then they had to struggle a lot with toxicity, with the side effects. It is a super-intensive protocol with many side effects, where you need experience and where you need the full range of antibiotics, supportive care and blood products that were not available at that time. Blood banks were really horrible there, often infected with hepatitis. [In consequence, . . .] they realized that they could not handle the protocol well enough. So, either they lost their children due to the toxic effects of the therapy itself, as then happened too often, or did so because they feared exactly that and interrupted treatment for too long, with the result that therapy was no longer effective. (German doctor involved in Russia at the time)
These two activities have in common that they worked only one way: readily available knowledge from the West was transferred to Russia. This is said to have been the dominant approach across medical disciplines after the fall of the Iron Curtain.
Nevertheless, within the subfield of ALL treatment, a third activity can be identified, which cannot be observed in adjacent fields of healthcare. Here, doctors from Russia engaged in jointly recombining medical knowledge together with foreign doctors, drawing on rules and resources from both contexts to develop a new treatment protocol viable under the specific circumstances prevailing in Russia. A German professor agreed to become tutor to several Russian doctors who had written their dissertations in Berlin about specific problems in Russia. The ward in Berlin had traditionally been a major contributor to a treatment protocol which was used internationally and being revised at that time (BFM-90). One of the Russian doctoral students who stayed there for a whole year had the opportunity not only to learn how to apply the acquired knowledge to patients, codified within a chemotherapy protocol, but also to attend the development of the new version of the protocol itself. He was familiar with the conditions in Russia, and now became deeply familiar with the environment in which the BFM protocol produced its superior results. In addition to that, and most unusual at that time, a German doctoral student spent approximately one year in Moscow and worked with Russian doctors on patients in the context of everyday work in a Russian hospital. On his return, this provided the ward in Germany with profound contextual insights into the practices which either fostered or reduced the potential effectiveness of treatment under these conditions and were vital for its subsequent development: “. . . and then it is difficult if one is not able to disassociate from one’s own experience, and is not able to look and ascertain: ‘What do they want, what do they actually need?’” (German medical professor).
Thus, the external lens started to work in both ways, allowing for joint recombination of knowledge and enabling more context-adequate treatment. Departing from here, pediatric ALL care developed in a completely different way to other subunits of oncology/hematology in Russia: actors on both sides learned to take the specific conditions in Russia into account and, instead of applying an existing protocol as a blueprint, to meticulously identify existing rules and potential resources in the country, on the basis of a wider perspective, as being elements from which to create something new “out of the ruins” (Stark & Bruszt, 1998, p. 82). “What are the problems with the BFM protocol in Russia, and what resources are available there? What could enable engagement in effective treatment, if possible with the resources that are available in the country?” were the questions they asked themselves (German medical professor).
With their mutual understanding of the respective context, the organizational actors engaged in a practical process of “recombination” (see Stark & Bruszt, 1998) of elements of the existing chemotherapy protocols in order to create a treatment standard designed especially for application to the local circumstances: And then we compiled the treatment, which consisted of certain elements of protocols that had been used in Holland, Germany, and the USA, of which one could say: “Here are the active ingredients in this protocol which are likely to produce a good result.” And then we sat down like [. . .] with a puzzle, assembled it all together and said: “that should actually work.” We wanted to avoid high-dose therapy, we wanted to avoid therapies that cause a very strong suppression of the bone marrow function in order to reduce infections and therefore the requirement for blood transfusions—blood transfusions were, of course, an issue because of the transmission of infectious diseases—hepatitis, HIV, poorly controlled blood banks, and all those things. And then we wanted a therapy that meant as little as possible hospitalization, which meant a shorter stay in hospital because the wards were full—the family lived there, everyone camped there—because, of course, they had no accommodation. [. . .]. And then we composed this therapy the way we expected, for good reasons, that it would work, I’d say. And it worked. (German medical professor)
Retrospectively, anything that resembled a logical option at hand was at the time a big step into uncharted terrain. To refrain from applying protocols that delivered high survival rates under Western conditions was not only considered audacious by critics, but as violating existing best practice. The protocol was named MB-91, as it was developed in Moscow and Berlin and first applied in Moscow in 1991. It was first put to the test in a ward in Moscow in a so-called “mono-center trial,” comparing its results with those in patients treated with BFM in the same ward. The survival rate under the prevailing Russian conditions proved to be at least as good as of patients treated with BFM, but the protocol was easier to handle and less toxic (Stackelberg et al., 1999).
We conclude at this point for a later discussion in the light of theory elaboration that there was indeed an external shock which opened a window for change. However, simply looking outside one’s own context and applying what proved to work well elsewhere did not suffice. Instead, the case unveils that the decisive, leveraging activity in this early phase is the joint recombination of knowledge across contexts, which in our case meant the joint development of a treatment protocol together with organizational practices adapted to the Russian situation.
Enacting self-reinforcing mechanisms
Following this initial success, other wards in Moscow adopted the new protocol, and then the first wards in the Russian periphery joined: Yekaterinburg and Sochi. Today, the group comprises 59 wards (see Appendix H for a complete list) that agreed to group treatment on the basis of the jointly developed protocol. We argue that the first slow and then accelerated growth can be understood in terms of the concept of self-reinforcing mechanisms. Put simply, these mechanisms have one logic in common: “the more, the better,” which can lead to strong momentum. Here, “the more” refers to wards joining together with their respective patients. This holds true in our case, because the group pools not only its resources, but its patients as well: all patients treated with the group protocol enter the joint statistics. And the more wards with patients join, the faster the group learns and can improve the protocol, the more attractive it is in turn to join the growing group. In other words: the more wards can be attracted to join the group, the more patients can be successfully cured than in any single ward alone, and the easier it becomes in turn to attract more wards to join, because success is proven here by the number of children cured. These dynamics contributed a momentum so strong that change became possible: helping the creation of the new, decentralized alternative that increasingly replaced the existing centralized organizational path. Within a constructivist approach, however, it seems central to understand the concrete activities that enacted such self-reinforcing mechanisms and allowed for change.
The first activity that enacts a self-reinforcing mechanism can be described as exchanging medical expertise within the group. In the early development of multicenter cooperation, this exchange occurred by phoning each other for advice. Later, this aspect became more formalized by setting up a study center with financial support from a small foreign charity fund to facilitate the exchange of treatment knowledge within the group. Should complications arise, it is possible for any cooperating ward to call the study center 24/7 to receive support. The MB protocol, the common standard throughout the group, proves its importance: the steps and content of the chemotherapy treatment over time are defined explicitly, as well as the metrics of the diagnosis regarding, for example, the amount of tumor cells that may still be left after treatment. This “common language,” as one of the doctors calls it, makes knowledge exchange very efficient. Metrics of diagnosis often only make sense within the context of the joint protocol. As any patient in any ward enters the joint survival statistics of the group and is thus equally valuable for all wards, there is a strong incentive to exchange such medical expertise across organizational boundaries, as a doctor from the small remote ward in Nalchik argues, where such a complex therapy would never be possible without external support: “Each patient is taken into account; these data do not disappear. They are needed for this study. Therefore, each patient is invaluable. And this is a big plus in our circumstances.”
This element becomes even more obvious when looking at the related activity of sharing medical material within the group. Protocols have been developed because combination chemotherapy treatment success is most sensitive to dosage and timing. If any of the prescribed steps cannot be taken or are delayed, the chance of survival drops immediately. The accessibility of all of the medicine prescribed by any chemotherapy protocol is therefore pivotal for treatment success—plus immediate access to further medicine in case of complications. The environment in Russia for the MB Study is quite different in this respect from comparable medical studies in the West, as the following statement from the geographically most distant ward in Vladivostok highlights: And then doctors came from Seattle [. . .], they were sitting drinking tea with our doctors and nurses here. And one of the nurses asked: “What do you do when you do not have drugs?” Because for us, it was the most important thing that there were no drugs, she asked that [. . .] and they could not understand what we were talking about. Finally, one of them says: “we tell the nurse to get some.” That then made an incredible impression, because it was a very real question: “What do you do if there are no drugs?” because that’s what we encountered at every moment.
Under these conditions this second activity—enacting self-reinforcing mechanisms—provides an additional logistical function seemingly not necessary to the same extent abroad. Medical material is shared within the group as a doctor from Nalchik explains: As far as I’m concerned, I don’t have access to most of the medication we need for BFM, I don’t have many of the drugs: something always has to be looked for, bought, the parents always have to go off and find it. To be in a situation where you have such support through the protocol, when you can say “I’m here—this medication is not available here”—and the group can organize its delivery, etc.—this is not just a plus, it’s just the biggest blessing in the world.
In case the specific necessary resources for treatment cannot be mobilized, patients can alternatively be transferred within the network: “Within this structure there are various tasks, for example there is a center that cares especially for relapses; Minsk [. . .]; and there are babies that already have leukemia, and Yekaterinburg took over the responsibility for them,” as a Western doctor well acquainted with the Russian multicenter group stated. The same holds true for highly cost-intensive immobile treatment materials: only St. Petersburg, Moscow, Yekaterinburg, and Minsk (Belorussia) have operating theaters where bone-marrow transplantation can be carried out. The promise to distribute patients allows even small remote wards to provide treatment of these specific needs on a high level within the MB Group and contributes to enacting the wish to join, ultimately becoming a self-reinforcing mechanism. But it does so, in turn, for large, advanced wards, too: they are provided with the critical number of patients from the whole group to justify highly specialized and often expensive investments.
Still, our empirical material shows that change does not occur quite so smoothly in reality and is not a priori understood on the level of all wards in the group; nor is such detailed information about how this new group functions easily available in wards dispersed across the largest country on earth. The data indeed show that collaboration within the group needs to be promoted actively. As the advantages of the group, however great they are, would not even be known, and self-reinforcing mechanisms could therefore not be enacted, we argue here that the activity of explicitly convincing others to participate is a leveraging activity of specific importance. This activity has been institutionalized over time and can be observed in a concentrated way during the biennial group meetings. For any ward in Russia with ALL patients, even non-member wards, two doctors are reimbursed for their travel expenses to enable participation across the country. During these meetings, each time different doctors from the wards in question are given the opportunity to develop their own personal expectations regarding the benefits of joining the MB Group “in practice.” They are given the opportunity to become acquainted with beneficial group activities like the ones described above and the resulting improvements for the wards that have already joined the MB Group.
All wards in our sample that joined the multicenter cooperation had sent doctors to the meetings for several years beforehand. The following statement illustrates how this functions: I think it’s [taking part in the group meetings before becoming member] really important, because I, for example, had to talk to people and convince them that it makes sense to participate in the multicenter group. I was speaking about the results of the therapy, and that the major centers, like the one I am in charge of, still benefit more, even though they are on the same protocol as the smaller centers that can apply this therapy, too. And I was explaining all the pros that emerge from a multicenter study. And, of course, all the advantages I spoke of make working extremely interesting: interesting and important, and necessary, and it brings real benefits. Therefore, as you know, we now have more than 40 participants [wards in the group] and of course that did not happen all at once—the people “quietly pulled in that direction.” (head of ward, St. Petersburg)
Therefore, during group meetings, but back in their respective wards as well, doctors convince each other to cooperate with the help of a joint standard. Zooming into this aspect shows the cooperative, bottom-up character of change witnessed here. At this point, the close interdependence of the activities described above with the momentum of self-reinforcing mechanisms becomes most evident. From the perspective of each ward, the prospect of having others to share their treatment experience or having access to a joint pool of resources, even across organizational and spatial boundaries, makes their own treatment outlook more promising. Still, it is the group activity of convincing others to join that makes these advantages known. The self-reinforcing character of such a growing movement of actors convincing each other can be imagined easily; nevertheless, it is structured by and structures the joint standard that secures the increasing benefits of learning and healing jointly.
Communicating a superior organizational solution
Delving deeply into the change process urged us to differentiate between two aspects that may easily be confused. One is the insight of every single ward that it can treat its patients better when it joins (documented together with accession dates in Appendix H) and enacts self-reinforcing mechanisms through repetition. A quite different question is whether treatment of pediatric ALL in Russia as a whole has actually improved. Our data give detailed insights into how such an improved situation is socially constructed, which shifts the perspective from benefits for the single organizational entity—here the ward—triggering a change process to a general improvement on the level of the whole organization—here the organization of ALL care in Russia.
One distinguishable activity is communicating improved outcomes internally. This kind of communication was repeatedly observed during the biennial group meetings (2010, 2011, and 2015). An important feature of internal communication is showing the latest survival rates across all wards of the group (see Appendix B for a statistic originating from the group), which demonstrates that work within this organizational solution is superior. Improvements are generated jointly: at regular intervals, an existing protocol is discontinued and a new one, on the base of generated insights, is developed to enable future cooperation (hitherto in 1991, 2002, 2008, and 2015) with even better results. Protocols include randomized treatment alternatives, provoking minor differences in the likelihood of survival that are taken into consideration when developing the protocol further at a later date. Between these intervals, every six months, small amendments to the existing protocol are discussed, or sometimes side research questions developed by a subgroup when drawing on the joint statistics. All amendments are discussed from the viewpoint of cost and benefit, taking into consideration the resources existing locally in the multifarious wards across the group. Rather advanced, research-driven wards may suggest changes in treatment or diagnosis; smaller wards contribute by voting. The representative of a charity fund describes these discussions, some of which the first author could observe, as “an indication that something new has happened here: this study group is democratically organized [and] develops within the scope of a democratic process [. . .] by voting.” The first author witnessed three different sessions, each two days of intensive group work, with experts on specific topics presenting on the stage, discussions and disputes taking place via two microphones in the audience, and subsequent voting procedures.
As a second activity that he observed in this context was the external communication of improved outcomes. We define actors as being external if they neither belong to nor intend to join the group. For example, results of the group and related information are communicated to international experts, who are regularly invited to the biennial multicenter meetings. Or, vice versa, members of the group are invited to international conferences: “There are a lot of Russian doctors everywhere at international conferences. But the only ones visible across oncohematology, contributing presentations at these conferences themselves, are from the MB group,” as an internationally renowned medical professor from a Western country sitting next to the first author during one of the multicenter meetings in Russia whispered into the latter’s ear. Results are eagerly communicated, even outside the field of oncohematology. When the first author contacted the leading international expert working on the Russian demographic crisis in general, he was given the following written reply: Of course, improvements of children’s health and a reduction in child leukemia only represent a small fraction of the tremendous death toll in Russia. But it is a story of success! As far as I know, the improvement was caused by introducing the MB-91 protocol for better treatment of acute child leukemia.
Here, we witness another extension of the point of reference in internal as well as external communication: whereas previously, identification with the group and its results (instead of those of the single ward) could be observed, results in this last step are now projected onto Russia as a whole. Today, the vast majority of Russian wards active in the field of ALL care work in multicenter cooperation, and communicate their successes internationally.
The core of this success, which we again consider a leveraging activity, appears to be guaranteeing transparency concerning data collection and analysis. This transparency across organizational boundaries is considered the pivotal new, unique element, and the reason why the communication of group results is taken so seriously, both within the group and outside it. This element for leveraging organizational change becomes most obvious when it comes to an issue in medicine that is always rather delicate: failure.
That is the same for everyone, everyone feels that way, that if you do something, if you bear so much responsibility as well, and a lot can go wrong, and does go wrong, where there is always something to criticize, then you do not necessarily want to have someone looking over your shoulder, you do it that way, and you want to be in control of what is known outside [. . .]. And such collaboration within a group means that you disclose everything, that you are criticized by others, and that you offer your results for discussion. And that was just totally unfamiliar. (German doctor supporting the introduction of MB in Russia)
With reference to data collection, the group developed specific stages at which information is to be transmitted to the joint study center. For example, any new patient entering one of the connected wards across Russia has to be registered within 24 hours by filling predetermined data into a form or calling the study center in case of doubt. From then on, the steps which are to be taken to enable diagnosis and treatment are defined exactly (see Appendix J). These steps are the same for any ward—and are adhered to individually by the ward doctors. These know from their own experience how the joint data is constructed, and how biomaterials for diagnosis are usually sent to two laboratories which independently offer their services to the whole group for a double check. All data—collected for all patients during and even up until ten years after treatment in case of survival—are entered into a common database. Access to this base is granted on request at any time to any ward within the group. Study center employees (trained pediatric oncohematologists, one working full-time, two part-time) are regularly available for questions, and support the organization of the group meetings where they display joint results. Institutionalizing the support of group coordination became an indispensable element of the new organizational solution. Fortunately, its costs are negligible, averaging less than half the cost of treatment for a whole year of one single child with ALL in Western countries (see Appendix K).
Personal experience of contributing to data collection even from any remote ward, combined with the ability to question and discuss any element of data supply and analysis down to single patients with any other participating ward or study center employees, and access to the joint data collected across organizations as a basis for joint progress and communication seem to be the key to success. Guaranteeing this transparency, even across wards far away from each other, makes all the difference: it is not communicating results internally and externally per se that does so, but the fact that the underlying data collection and analysis is transparent and accepted as credible by each of the internal and external audiences. All relevant actors know and believe, that today, children with ALL in Russia are being cured better thanks to multicenter cooperation. A superior organizational solution has been constructed successfully.
Discussion and Conclusion
These empirical insights allow us to advance theoretical approaches to organizational change (Poole & Van de Ven, 2004; Demers, 2007), including those that emphasize structural inertia (Amburgey et al., 1993) or strategic persistence (Audia et al., 2000), in two specific ways. On the one hand, we contribute to the understanding of the duality of stability and change (Farjoun, 2010; Klarner & Raisch, 2013; Sonenshein, 2010) that is central to organizational studies in general and theories of organizational development and change in particular. On the other hand, directed more at research on organizational path dependence, we advance theorizing organizational change under adverse conditions by looking at a very important, not yet sufficiently developed, aspect: the question of if and how change may still be possible.
Towards a process model of path-breaking organizational change
Our case of path-breaking change in Russian healthcare confirms the importance of what was earlier named an “external lens” (Sydow et al., 2009). But although a first, important sudden shock occurred in the field—here a conference that shattered existing views of how cancer can be treated—the case leads us to the insight that the process of path-breaking change only starts from here, most certainly requiring “mindful deviation,” “disembedding from structure,” and “generating momentum” as emphasized by the theory of path creation (Garud & Karnøe, 2001; Garud et al., 2010). All three activities, that in the end lead to significant distance between the old, established and the new, envisaged path, are based on strategic agency and continue to play an important role in our model (see upward arrow on the right of Figure 2). Path-breaking change, however, does not just happen with the help of one strategic action. Rather, change, including organizational change, needs to be enacted and promoted repeatedly.
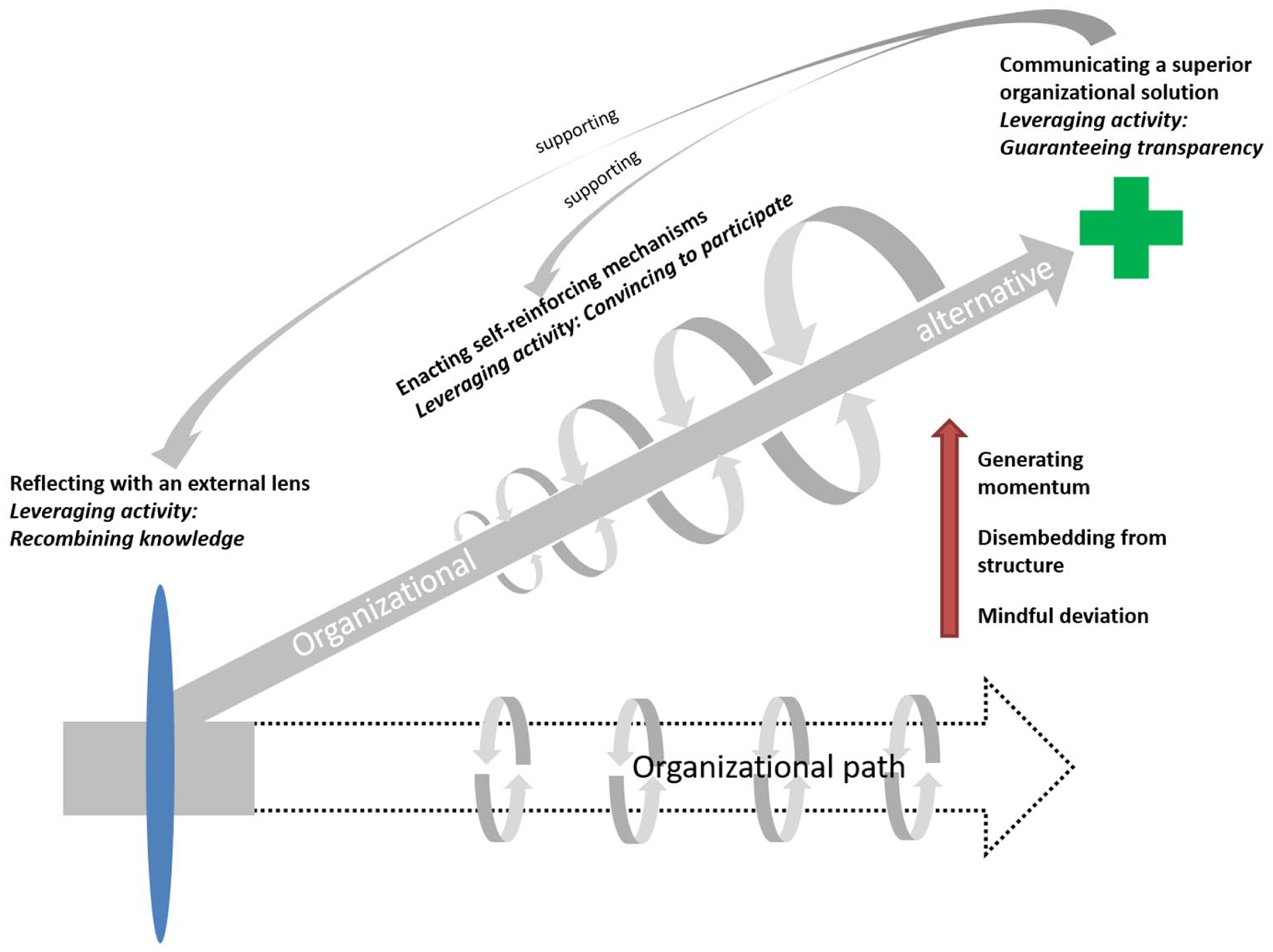
Breaking an organizational path by creating a new one: A process model.
Our empirical data allowed us to zoom into this demanding, multi-stage process of breaking an organizational path, where we subsume the first set of activities under the broadened notion of “reflecting with an external lens.” Activities of transferring knowledge in one direction (as the idea of a “lens” suggests) were omnipresent in the field of Russian healthcare. The successful case in question, however, advises that recombining knowledge with the help of close collaboration across contexts over a longer period of time was crucial for success; with organizational actors actively editing (Sahlin & Wedlin, 2008), translating and mutually integrating knowledge (Carlile, 2004; Zahra, Neubaum, & Hayton, 2020). The case suggests that this insight has such importance that we speak of a leveraging activity for path-breaking change, in our case towards a much more decentralized structure that, some may even argue, resembles a network form of organization (Powell, 1990). A leveraging activity such as recombining knowledge not only enables path-breaking organizational change directly more than others. It also has an indirect effect by making other activities, like applying general knowledge to and specific treatment standards from other contexts, more effective. This activity of jointly recombining knowledge across contexts, codified here with the help of a treatment standard (that emerges as the result of stage 1), comes nearest to Djelic and Quack’s (2007) insights into the creation of a transformational space for negotiating standards (in their case: international accounting standards) across institutional settings. This leveraging activity may be particularly important for path-breaking change in what are considered, like health care, science-based fields populated by knowledge-intensive organizations (Millar, Lockett, & Mahon, 2016).
With regard to the second stage in our model, our research suggests that self-reinforcing mechanisms do not necessarily lead to stability as it is known from path dependence research (see arrow on bottom of Figure 2), but that they may be enacted, quasi as “counter-mechanisms,” to drive organizational change (see gradient arrow). The case shows that actively convincing to participate—in the group, using the joint standard—leverages change at this stage: it is this activity that we distil as being crucial to enacting and redirecting self-reinforcing mechanisms. Such mechanisms, that drive incremental change with a radical outcome (Plowman et al., 2007; Streeck & Thelen, 2005), then help to provide the necessary momentum. At the same time, they become ingrained into the new organizational path, increasingly countering the old one (Page, 2006). Path-breaking change thereby involves self-reinforcing mechanisms that may lead to path dependence again at a later stage, possibly even to another lock-in. As in the case studied here, path-breaking change is likely to be based on the successive decisions of distributed agents, again underlining the importance of the leveraging activity of convincing others to participate. The joint treatment standard is the most visible element to which “participation” refers. This standard, like organizational procedures in other contexts, is not only an outcome of multicenter cooperation, but also structures the “emerging collective” that produces it (Garud & Karnøe, 2001, p. 20)—as highlighted by path creation theory. While enacting and redirecting self-reinforcing mechanisms that contribute to path-breaking organizational change may be important in all fields that give rise to complementarity and coordination effects, it is again particularly salient in science-based fields such as healthcare, which strongly rely on standards and procedures to guide (joint) action.
Finally, regarding the third stage, we identify for our model of path-breaking organizational change the activities of actors “communicating a superior organizational solution.” Activities of internal and external communication—not unlike discursive or narrative approaches to organizational change (e.g., Grant & Marshak, 2011; Sonenshein, 2010)—attribute a prominent role to language (cf. Lawrence & Phillips, 2019), and result in the fact that, in our case, all the experts on Russian healthcare we consulted, inside or outside Russia, unanimously referred to the MB Group—and the respective network this group had created across 59 wards by 2020—as an outstanding positive example of organizational change. Nevertheless, there seems to be a leveraging activity again: all this communication effort would not be credible, and even in vain, if the group did not invest religiously, apart from in communication activities, in guaranteeing transparency to which we, again, denote a leveraging activity. Like reflecting with an external lens, which allows for recombining knowledge and triggers self-reinforcing mechanisms working against the present organizational path (via convincing to participate), this leveraging activity may again be of extraordinary importance in science-based fields, in particular in those in which the current state of scientific knowledge continues to be debated.
The process model we develop from these insights contributes to the discourse on organizational path dependence (Sydow et al., 2009) and path creation (Garud & Karnøe, 2001) that can be brought together under the constructivist umbrella of path constitution (Jing & Benner, 2016; Sydow et al., 2012; Singh, Mathiassen, & Mishra, 2015). Path-breaking activities, as depicted by our model, of course overlap and depend on each other (see again Figure 2). The model unveils “the structuring of recursive relations” (Fisher & Aguinis, 2017) that are at stake in complex path constitution processes; not least, as it is based upon a temporal-relational understanding of agency as advocated by Emirbayer and Mische (1998) and subsequently adopted by a number of process researchers (e.g., Feldman & Pentland, 2003; Smets & Jarzabkowski, 2013).
In sum, our process model helps to understand organizational change under the adverse conditions of path dependence and, thereby, contributes to research on path dependence and path creation in at least three respects. First, we detect important activities, not least leveraging activities, that help to break a path: recombining knowledge, convincing to participate, and guaranteeing transparency; we also clarify the recursive relations of these activities in a multi-stage process. Second, we discover that self-reinforcing mechanisms, which are usually considered to cause path dependence and are triggered by and maintained with the help of such activities, can create a path that counters and, as in our case, breaks the established path. Third, unearthing these activities and mechanisms adds nuance to former insights into path creation processes. The overarching insight of our study, with regard to this discourse, however, is that the theories of organizational path dependence and path creation are not as opposed, as it may seem at first sight when applied to organizational contexts, specifically not when path creation, as common in economic geography (cf. Martin & Sunley, 2006; Simmie, 2012), is conceived as a particular phase in the overall process. Drawing on empirical insights relating to organizational change under the adverse conditions of path dependence, we show that advances from both streams of research—integrated into a theory of path constitution—provide valuable elements for a better understanding of organizational path dependence and the possibilities for path-breaking change, in particular in knowledge-intensive fields.
Highlighting both activities and mechanisms, and conceptualizing their intricate interplay in change processes, not least with regard to leveraging activities, can connect our research to theorizing organizational change more generally. Although we see a wide variety of research streams which our results can potentially address, we would like to highlight the current attempt to rethink organizational stability and change as duality (rather than dualism), as they are both contradictory and complementary (Farjoun, 2010), a view that may have far-reaching implications for understanding organizational development and change. Farjoun (2010) considers not only stability as an outcome enabling change, but also change as a precondition for stability (see also Klarner & Raisch, 2013). Our study shows that even change with path-breaking consequences may rely on relatively stable processes when replacing an organizational path with a new one, that is, incremental change with radical outcomes (Djelic & Quack, 2007; Plowman et al., 2007).
Such path-breaking change, as should have become clear by now, differs significantly in kind from on-path or “path-dependent change” (Karim & Mitchell, 2000). While the latter is also of an incremental nature and allows for deviating actions (as known from performances of routines; cf. Feldman, 2000, or practice diffusion; cf. Ansari, Fiss, & Zajac, 2010), path-breaking organizational change is per definition transformative (Karim & Mitchell, 2000), i.e., close to what Pettigrew (1985) and others termed “strategic change.” More importantly, this change implies not only a greater distance to the old, but follows a different process logic emphasizing “organizational circularities” (Tsoukas & Pina e Cunha, 2017). In effect, detecting sources of stability in the process may greatly help us to understand how change can be brought about incrementally with transformative results. In our case, change was promoted by enacting the same kind of self-reinforcing mechanisms again and again; mechanisms that have been associated with stability in the literature. Therefore, self-reinforcing tendencies can not only be highly compatible with such a perspective of stability and change as duality, but also add nuance to our understanding of organizational change under conditions of path dependence.
Prospects for future theorizing and practicing
Our case shows that organizational change can indeed turn into institutional change. Today, in the subfield of ALL, the taken-for-granted, institutionalized approach to treatment is multicenter cooperation. This has changed gradually in this particular subfield, whereas in neighbouring diseases children or adults are still sent to Moscow or even abroad for adequate treatment.
These findings suggest that our work has implications for neo-institutional theory as well. While traditionally, neo-institutional theory has looked at stabilization processes, the more recent emphasis on agency and change (e.g., Lawrence & Phillips, 2019) is similar to current developments in path theory. Connecting with this theorizing—with its increased emphasis on strategic agency and, at the same time, continued consideration of self-reinforcing mechanisms with regard to the reproduction and eventual transformation of rules and resources (Giddens, 1984)—could help to develop an improved understanding of the challenges institutional work and other change-oriented activities face under the particularly adverse conditions of organizational or institutional path dependence (Berthod & Sydow, 2013). While such adverse conditions are not yet the focus of neo-institutionalism, turning more towards them may be an important task for a future that increasingly seems to ask for organizational and institutional change of a transformational rather than incremental quality.
Although the process model derived from our case is certainly not intended for implementation as a blueprint, its elements are worth considering for practice when confronted with organizational change under conditions of path dependence. First, the model directs managerial attention to reflection via an external lens, initiating a rather bidirectional process of knowledge combination; a view that seems to be neglected too often when employing external advisers or consultants, but is nicely reflected, for instance, in more inclusive-interactive and pluralistic-political conceptions of managing “issue-focused multi-stakeholder networks” (Roloff, 2007). As the case shows, the joint development of rule-based, context-adapted standards becomes a crucial element when developing an alternative course of action, in particular in knowledge-intensive contexts. Second, the process model unveils the dual role of self-reinforcing mechanisms both in path-dependence and in path-creation processes. Thereby, it draws attention to the fact that such mechanisms may strongly support stability and change, but rely heavily on agency, as they need to be continuously enacted, not least with regard to the direction of their impact. It is here where practitioners’ efforts will have the largest leverage to support the generation of the momentum necessary to accomplish change. Third, the process model shows that a superior organizational solution is the outcome of an active process of social construction, which puts emphasis on internal and external communication and particularly on transparency to enhance credibility, involving a growing knowledge community until agreement on the improvement is considered a general fact.
Limitations and suggestions for further research
Like any study, this one has limitations that provide opportunities for future research. First of all, we drew on a single case in a particular field over a certain period of time and in a specific national setting, which limits empirical generalizability. However, this case offers rich insights which can only be unearthed with single case designs. This allowed us to zoom into the case in the detailed way necessary, even across a longer process, which we captured by using a time-lagged case study design. Furthermore, it was the field that offered such a unique case of organizational change (the only multicenter cooperative group in Russia so far), that is, at the same time, an exceptional case of success (an unparalleled improvement of survival demonstrated across the expanse of Russian territory after this organizational change)—and therefore a welcome opportunity to study measurable, successful change for the better under apparently adverse conditions.
Second, we sacrificed the potential of our data to delve deeply into specific aspects in order to facilitate a broad understanding of the whole process. Thus, one of the challenges remains to improve our understanding of the subtle interplay of organizational and technological dynamics in path-dependent and path-creating processes within and among organizations (Bohnsack, Kurtz, & Hanelt, 2021; Thrane et al., 2010), together with a closer look at the variety of possible self-reinforcing mechanisms (Djelic & Quack, 2007; Dobusch & Schüßler, 2013). Equally important, change processes never take place within an institutional vacuum, which means, for instance, that not only institutional heterogeneity (Jing & Benner, 2016), but also power differentials are likely to be important for path constitution processes (Crouch & Farrell, 2004; Djelic & Quack, 2007; Maielli, 2015; Pierson, 2000; Valorinta et al., 2011). These shortcomings deserve more attention, but the respective limitations of our work, we hope, will inspire further studies into the fascinating paradox of specifically difficult organizational and institutional change under conditions when they seem to be required the most.
Supplemental Material
sj-docx-1-oss-10.1177_01708406221103965 – Supplemental material for Breaking a Path by Creating a New One: How Organizational Change Boosts Children’s Cancer Care
Supplemental material, sj-docx-1-oss-10.1177_01708406221103965 for Breaking a Path by Creating a New One: How Organizational Change Boosts Children’s Cancer Care by Florian Stache and Jörg Sydow in Organization Studies
Footnotes
Acknowledgements
We would like to thank OS Senior Editor Beth Goodrick and the three reviewers for their helpful advice and encouragement in developing this article. Koch-Metschnikov-Forum and Kontakte-Kontakty, two NGOs, helped to establish access to the field. Alexander Karachunskiy at the Federal Center of Pediatric Hematology, Oncology and Immunology, as well as Günter Henze at Charité–Universitätsmedizin Berlin, Department of Pediatric Oncology and Hematology, provided invaluable help to make the ethnographic work possible.
Funding
The author(s) declared the following financial support for the research, authorship, and/or publication of this article. We are grateful to the German Research Foundation (DFG) for generously funding the Research Training Group “Pfadkolleg” (GRK 1012) at the School of Business & Economics of Freie Universität Berlin. Moscow and to the German Academic Exchange Service (DAAD) for supporting with travel expenses.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.