
Abstract
Boundary-work research has extensively explored how professionals engage in boundary work to protect or expand their professional boundaries in interprofessional collaboration (IPC). Yet professionals’ contextual constraints in everyday work, such as time pressure or legal restrictions, often result in competing interests of the professionals involved in IPC, prompting them to engage in boundary work to limit—instead of protect or expand—their boundaries. Our empirical analysis uses comprehensive qualitative data on IPC in Germany between self-employed general practitioners (GPs) and registered nurses employed in nursing homes. In this IPC, GPs’ efficiency interests frequently compete with nurses’ safeguarding interests, leading both professionals to engage in boundary-work efforts to limit their boundaries. Our findings provide a comprehensive understanding and framework of professionals’ boundary work, showing that individual GPs and nurses typically hold a portfolio of various defending and accommodating micro-strategies. Based on our first-order findings, we identify how different sources of power enable particular micro-strategies and explore how the choice of micro-strategies depends on different forms of trust in the collaborating partner. Last, we outline interactions of micro-strategies, illustrating how the outcomes of professionals’ bilateral boundary work depend on the sequence of these strategies.
Keywords
Introduction
Interprofessional collaboration (IPC) brings together professionals with different specialized knowledge, expertise, and social status to perform a shared task (Abbott, 1988) and is carried out in various sectors, such as healthcare (Huq, Reay, & Chreim, 2017), construction (Ahuja, Nikolova, & Clegg, 2017), and creative work (Bechky, 2006). IPC is particularly suited to completing complex and ambiguous tasks (D’Amour, Ferrada-Videla, San Martin Rodriguez, & Beaulieu, 2005). At the same time, given the differences across professions, IPC requires professionals to ‘open up and renegotiate the boundaries that define their roles and practices’ (Comeau-Vallée & Langley, 2020, p. 1650); that is, IPC involves boundary work.
The notion of boundary work—as put forth by a recent burgeoning research literature—comprises the purposeful efforts of professional groups and their members to influence the boundaries between professions (Langley et al., 2019). Boundary-work research has investigated how professional groups or individual professionals try to protect or expand the practice domains of their profession. For example, Bucher, Chreim, Langley, and Reay (2016) showed how different professional associations in the healthcare field used framing tactics to prevent government initiatives from reshaping their jurisdictional boundaries. Boundary-work research has also studied professionals’ boundary-work activities on the micro level. Micro-level boundary-work research is inspired by negotiated-order theory—which views social order, and thus the form of IPC and the labor division within it, as shaped by an ongoing negotiation process in and through interaction (Strauss, 1978). According studies have revealed how professionals at the frontline engage in actions to protect or expand their professional jurisdiction (Allen, 2000; Håland, 2012). Allen (2000), for example, showed how nurse managers in a United Kingdom district general hospital engaged in strategies to demarcate the role of clinical nurses from other professions in the hospital in response to policy-driven jurisdictional changes. In micro-level boundary-work research, boundary work is primarily considered to be a response to acute external challenges, such as legal or organizational change that has the potential to shift professional boundaries and impact professionals’ jurisdiction and status.
While external challenges to professional boundaries are obvious triggers of boundary-work activities, boundary work is also an everyday work practice in IPC (Langley et al., 2019). Professionals’ different identities and values prompt them to engage in recurring efforts to protect or expand their professional domains and promote their professional approaches in their everyday IPC (Comeau-Vallée & Langley, 2020). Different approaches for achieving a shared goal require professionals to negotiate how to achieve this goal (DiBenigno, 2018; Huq et al., 2017). Such negotiation is particularly necessary because the complexity of everyday IPC often involves ambiguity about the exact location of interprofessional boundaries that distinguish tasks and roles, making it difficult to clearly define which professional should conduct which tasks in IPC (Comeau-Vallée & Langley, 2020). Boundary work, then, is used not only to demarcate but also to enable collaboration.
Recent boundary-work research has emphasized that while the frontline work of professionals—and thus their IPC—is prescribed by their identities and approaches, it is also strongly shaped by the contextual constraints that professionals face in executing their everyday work—such as limited time resources, economic pressure, or legal restrictions (Apesoa-Varano, 2013; Meier, 2015). Initial studies on boundary work that considered such constraints have examined how professionals engage in boundary work in order to achieve their overall goal despite these constraints (Liberati, 2017). Apesoa-Varano (2013), for example, showed how healthcare professionals’ everyday boundary work under conditions of limited time resources sometimes means transcending boundaries and doing the work of other professionals in order to ‘get work done’ and ensure optimal patient care when those other professionals are busy with other tasks.
What boundary-work research has so far rarely considered is that contextual constraints also result in professionals having specific interests in addition to achieving the overall goal, and that these interests may prompt professionals to engage in efforts to limit their involvement in IPC and thus their professional boundaries, instead of protecting or expanding them. Limiting boundaries, however, becomes particularly problematic when both collaborating professionals attempt to do so, thereby creating a gap in labor division that is not covered by either professional. For example, in our empirical setting of IPC in Germany between self-employed general practitioners (hereafter, ‘GPs’) and registered nurses employed in nursing homes (hereafter, ‘nurses’), GPs, as self-employed professionals with limited time resources, have efficiency interests, while nurses must comply with stringent legal requirements and have limited medical expertise, imposing on them interests of safeguarding. These interests compete in everyday IPC and result in both GPs and nurses trying to limit their involvement and thus their respective boundaries, requiring negotiation and renegotiation at the boundary.
Competing interests stemming from professionals’ contextual constraints thus seem to play a major role in why, how, and with what effects professionals engage in boundary work. Corresponding research is needed because contextual constraints of professionals in everyday work are pervasive, and initial studies have shown that boundary work as a response to such constraints may widely differ from boundary work as a response to acute triggers and from boundary work to promote professional approaches (Liberati, 2017; Meier, 2015). Our study therefore addresses the following research question: How do professionals involved in everyday IPC engage in boundary work to limit their boundaries in response to competing interests arising from contextual constraints?
Our empirical research on IPC in Germany between self-employed GPs and nurses employed in nursing homes presents a fruitful setting to study our research question. We find that individual GPs and nurses typically hold a portfolio of various micro-strategies to limit their boundaries and that these micro-strategies can be grouped into two types: defending strategies, aimed solely at limiting their own boundary; and accommodating strategies, aimed at taking into account both actors’ interests and preferred boundary location. Because defending strategies aim at enforcing one’s own interest against the other actor’s interest—therefore requiring the use of power—we further analyse and elaborate on how these strategies rely on different sources of power (social status and situational control) that professionals can draw on, particularly shedding light on the power sources of low-status actors, who so far have been found to be less successful at harnessing power in the boundary-work literature (Comeau-Vallée & Langley, 2020). We further explore when professionals use which type of strategy (defending or accommodating), revealing how professionals’ strategy choice depends on the different forms of trust that they have in the collaborating partner, allowing us to theorize on trust as an important condition of micro-level boundary work that has been largely neglected in extant boundary-work research (Meier, 2015). Last, we outline how different sources of power and different forms of trust shape the interactions and respective outcomes of boundary-work micro-strategies. Together, these findings help advance current boundary-work research by systematically exploring and theorizing how variations in micro-level boundary work relate to different contextual conditions and contingencies (Langley et al., 2019).
Theoretical Background
Professions, professional boundaries, and interprofessional collaboration
Professions are characterized by specialized occupations, and members of a profession—that is, the professionals—hold distinctive knowledge and expertise and are often granted the exclusive right to perform their occupation (Abbott, 1988). Professionals thus possess high levels of work autonomy, and their distinctive knowledge bases and control over applying that knowledge lead to occupational closure that forms boundaries (Currie, Finn, & Martin, 2009). Professional boundaries can therefore be understood as demarcations between professions that differentiate tasks, roles, responsibilities, and status (Lamont & Molnár, 2002).
IPC describes a situation in which members of two or more professions collaborate across professional boundaries and thus across domains of specialized knowledge, expertise, social status, and sometimes even formal hierarchy (Strauss, 1978). While IPC has proven useful for tackling complex tasks, it is often difficult to achieve in practice because professional differences first need to be bridged before collaboration can be effective (D’Amour et al., 2005). A typical case of IPC is different professions collaborating in healthcare settings, often a collaboration between nurses and physicians. The healthcare example is a good illustration of a collaboration involving complex decision making, different approaches, different core assumptions arising from different educational backgrounds, and varying levels of hierarchy and status across professionals—all of which may result in professionals who have competing ideas about how to achieve a common goal. Thus, IPC requires professionals to (re-)negotiate the boundaries between them and their respective roles. In other words, they need to engage in boundary work.
Interprofessional boundary work at the micro level
Boundary work in the professions is commonly defined as the purposeful efforts of professional groups or individual professionals to influence the boundaries between professions (Langley et al., 2019). Boundary work is usually used to protect or expand a given practice domain or professional approach, while also clearly demarcating one profession from others. One stream of research studying the boundary work of professional groups considers them as collective actors at the level of the profession (e.g., Bucher et al., 2016; Hazgui & Gendron, 2015), while another stream has shown a growing interest in micro-level studies and considers boundary work as professionals’ work practice in IPC at the frontline (Håland, 2012; Lindberg, Walter, & Raviola, 2017). Studies of micro-level boundary work are inspired by negotiated-order theory, which investigates how social order—and thus the form of IPC and the labor division within it—are negotiated between the interacting individuals (Strauss, 1978). Such negotiation is often influenced by the different social status of professionals, typically granting those actors with high social status a powerful position (Comeau-Vallée & Langley, 2020).
Professionals’ boundary work on the micro level can be a response to external triggers, such as legal or organizational change that challenges professionals’ domains, jurisdictions, and status (Allen, 2000; Lindberg et al., 2017). Additionally, negotiation at the boundary may be rooted in professionals’ identities and values, which prompt professionals to defend their professional domains or promote their professional approaches (DiBenigno, 2018; Huq et al., 2017). Negotiating how a joint goal should be achieved is therefore an important enabler of collaboration, particularly because the complexity of IPC often involves ambiguity about the specific location of (task) boundaries (Comeau-Vallée & Langley, 2020).
A few boundary-work studies have identified the contextual constraints professionals face in their everyday work, such as limited time resources or economic or legal restrictions, as important additional causes for boundary work (Liberati, 2017; Meier, 2015). Apesoa-Varano (2013), for example, points out that boundary-work activities result from professionals’ time constraints in their everyday work, which may lead professionals to transcend boundaries in order to ‘get work done’ and ensure that an overall goal, such as optimal patient care, is achieved. Contextual constraints, however, may also imply that professionals hold individual interests in their IPC, such as being efficient or being safeguarded, resulting in efforts to limit their boundaries. This becomes particularly problematic when professionals have competing interests and both collaborating professionals intend to limit their boundaries—for example, when more than one party is subject to time pressure—thereby creating a gap in labor division that requires negotiation and renegotiation at the boundary. In this study, we explore how professionals involved in everyday IPC engage in boundary work to limit their boundaries in response to competing interests arising from their contextual constraints.
Method
Research setting
We conducted a qualitative study in Germany of the IPC between self-employed GPs (paid on a capped fee-for-service basis) and nurses employed by nursing homes for long-term care (paid a fixed salary). Contextual constraints and boundary-limitation efforts are common in this IPC and the differences between the collaborating professionals (e.g., regarding education, status, expertise, organizational affiliation) are very pronounced, thereby presenting a suitable setting to explore boundary-work activities.
In Germany, care in nursing homes is provided by nurses with a range of educational backgrounds, from nurse aids without vocational training who perform basic care tasks (such as assisting with personal hygiene), to registered nurses with three-year vocational training in geriatric or general nursing (Fleischmann et al., 2016). Registered nurses are qualified to perform all care activities, including minor medical tasks such as giving injections and communicating with GPs, and are therefore the focus of our study. Yet, in contrast to other countries, in which nurses often hold academic degrees and work more independently, registered nurses in Germany have a very limited scope of action—for example, they are not allowed to autonomously perform any medical interventions, and even for minor actions, such as giving a headache pill to a nursing-home resident (hereafter, ‘resident’), they need GP permission (Fleischmann, Geister, Hoell, Hummers-Pradier, & Mueller, 2017).
GP care of residents in Germany is not typically an integrated service that nursing homes provide, but instead is provided by independent GPs. Most GPs in Germany are self-employed and run their own practices or are employed by another GP’s practice. Just like anyone in Germany, residents have the legal right to choose their GP, which means that in one nursing home a number of different GPs are usually involved in patient care. Patients in Germany typically have long-standing relationships with their GPs, and when moving to a nursing home, residents usually keep their GPs. GPs terminating patient relationships is possible but uncommon (Busse & Blümel, 2014).
Because residents often have a multimorbid condition and cannot visit a GP practice on their own, GPs visit the nursing homes for consultation. Nurses are the residents’ primary caregivers, and they typically organize and coordinate GP consultations. While there are some political efforts to better structure and regulate IPC between GPs and nurses (e.g., joint training programs), GP-nurse IPC has very few formal specifications or standard operating procedures. The only exception is nurses’ statutory responsibility to involve a GP for any medical question and the GPs’ responsibility to render assistance when medical intervention is needed (Fleischmann et al., 2017).
Providing residents with high-quality care requires that GPs and nurses closely collaborate: GPs need current information about residents from nurses and nurses need information from GPs about diagnoses and how to integrate treatment into care. In everyday work, however, this collaboration is often characterized by conflict, which is particularly apparent in the case of residents indicating that they feel unwell, which is the focus of our study. As residents’ caregivers, nurses are responsible for supervising and assisting residents and are thus responsible for initiating further steps. Yet this situation is complicated because nurses have a limited ability to assess a resident’s condition, and when exactly to involve a GP. If they wait too long to involve a GP they may be accused of having failed to render assistance and may face legal consequences. These constraints result in nurses having strong safeguarding interests, aimed at avoiding any ambiguity about a resident’s condition and seeking to involve GPs as soon as possible when residents indicate they feel unwell.
GPs face a different situation. Because most of them have their own practices and are thus self-employed (or are employed at another GP’s practice), they have efficiency interests in IPC. This situation is amplified because GPs consider the care they provide to residents to be time-intensive (particularly because it involves visits) and the reimbursement via capped fee-for-service rates for nursing-home visits to be relatively low (Fleischmann et al., 2016). At the same time, GPs often consider nurses’ requests as unnecessary or as involving them too early, which is not only economically inefficient, but also strains capacity that could be used for their other patients. GPs therefore seek to be involved only when they believe it is necessary.
In sum, while the primary goal of both groups of professionals is optimal resident care—which they typically pursue wholeheartedly—their different contextual constraints give rise to competing interests and lead to efforts to limit their respective boundaries.
Data collection
We collected interview and observational data between March 2018 and June 2020 in a field study that is part of a larger study on IPC between GPs and registered nurses employed in nursing homes in and around Hamburg, Lübeck, and Göttingen with a minimum size of 40 residents. We selected nursing homes for the present study from the overall sample using a purposeful sampling approach and included nursing homes with different locations, sizes, and ownership structures to capture the variety of nursing-home settings in Germany. Additional data was collected for the sole aim of the present study.
Our main data source are 72 semi-structured interviews that one of the authors conducted—39 interviews with 34 nurses (73.5% female, 26.5% male) employed by 15 different nursing homes, and 33 interviews with 26 self-employed GPs (38.5% female, 61.5% male). GP interviewees had been working together with at least one nurse in our sample. While our level of analysis is the individual professional, including interviewees who actually worked together helped us to verify and better understand perspectives and perceptions of IPC from both sides of the dyad.
We contacted GPs and registered nurses in writing and via telephone and included them if they were available and willing to take part in our study. Most GPs and nurses we approached agreed to participate. We conducted the interviews either in person in the nursing homes, in the GPs’ practices, or via telephone. We interviewed some participants two or three times, with a break of around six months between the interviews, which allowed us to verify their accounts for consistency and to further explore the themes they mentioned in previous interviews. Interviews lasted between 20 and 77 minutes. All interviews were audiotaped and transcribed shortly after.
The authors had jointly developed the semi-structured interview guideline, which encouraged participants to talk about their everyday work, particularly about what they believe IPC looks like, what activities are involved in IPC, and their perceptions of the collaboration. During the data-collection process, the authors regularly discussed initial ideas and adjusted the guideline to account for emerging themes.
In addition to conducting interviews, one of the authors and a research assistant also conducted roughly 70 hours of observation in nine nursing homes to better understand the everyday reality of IPC (Whyte, 1984). During these observations the researchers took notes, but strictly maintained an observer role and refrained from actively participating. Following the observations, we held separate informal conversations with GPs and nurses to ask them how they perceived the observed situations. We refined our field notes and converted them into observational reports. We discussed field experiences in research-team meetings, and in reflecting on the practices observed we gained a comprehensive and in-depth understanding of our research phenomenon while maintaining insider-outsider roles within the team (Evered & Louis, 1981).
Data analysis
Two of the authors separately and openly coded the data, following the principles of Gioia and Chittipeddi (1991). We identified the specific situation of residents feeling unwell as a case in which the efficiency interests of GPs and the safeguarding interests of nurses competed and led to boundary-limiting efforts from both professionals. The two authors then parsed out data that included descriptions of how individual GPs and nurses engaged in purposeful actions to pursue their respective interests. Both GPs and nurses used a variety of strategies, which we labeled ‘micro-strategies’. For each micro-strategy, we created first-order concepts. After critically evaluating the first-order concepts, in an iterative process we employed second-order analysis to reveal connections among our first-order concepts and aggregated them into micro-strategy categories—our second-order themes. In a third step, we abstracted the four second-order themes into two aggregate dimensions. During the aggregation steps, the third author (an organization scholar) and the fourth author (a medical scholar who works part-time as a GP and who was involved in this study only as a researcher and not as a respondent) acted as devil’s advocates to prevent us from getting ‘lost’ in the data (Gioia, Corley, & Hamilton, 2013). Figure 1 depicts our data structure.
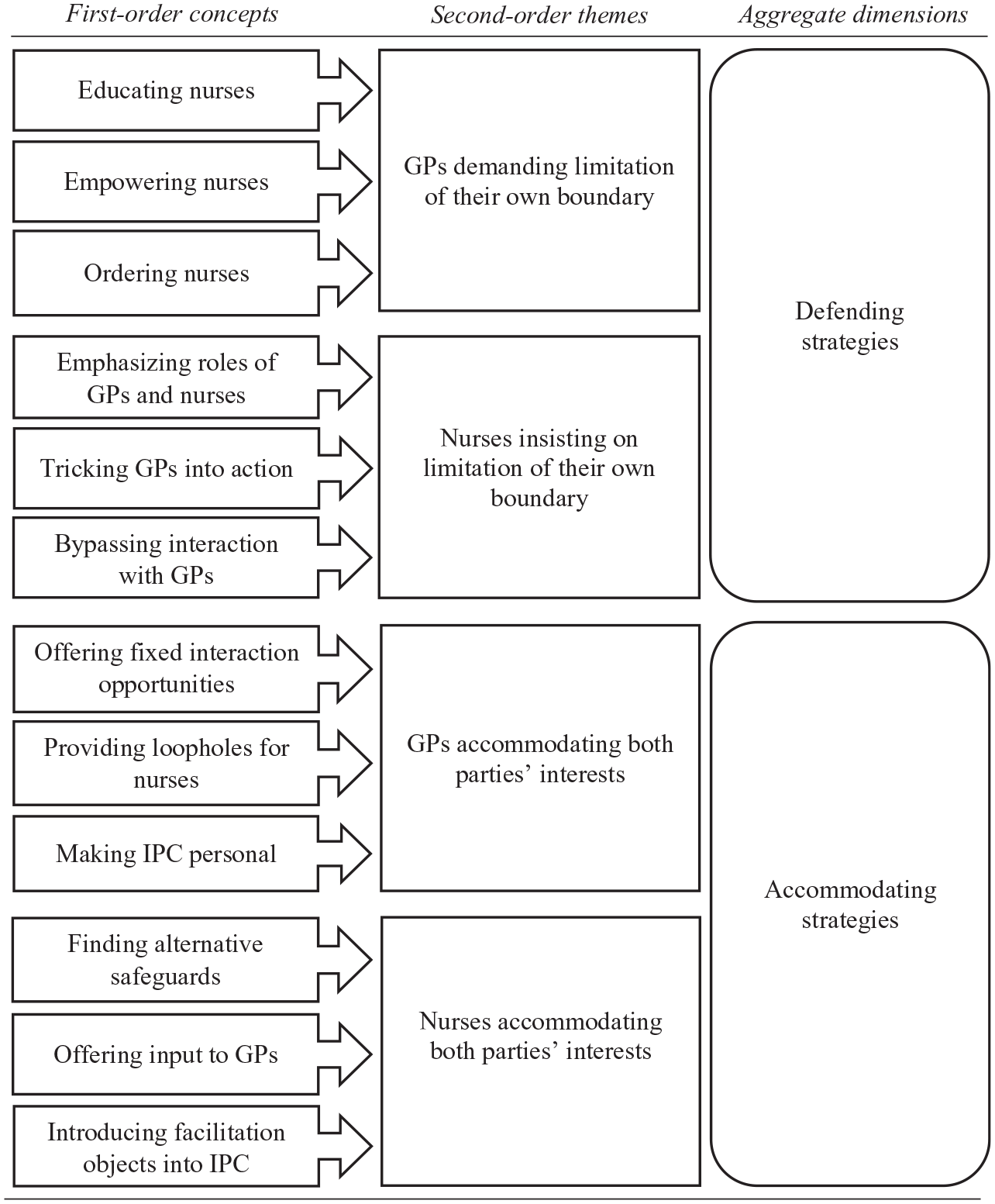
Data structure.
In addition to comprehensively accounting for professionals’ boundary-work strategies, our first-order findings brought forward two insights that prompted us to look more closely at the contextual properties under which the strategies were used (Corbin & Strauss, 2008). First, we found that both GPs and nurses had one set of strategies (‘defending strategies’) that enforced their respective interests against the other actor’s interest—thus precluding the use of power. Prior boundary-work literature has particularly emphasized high-status actors’ ability to harness power (Comeau-Vallée & Langley, 2020), yet we found that nurses’ (low-status actors) defending strategies were able to trump GPs’ strategies in some cases. We therefore more closely examined the underlying sources of power on which GPs’ and nurses’ defending strategies were built. Second, we found that the individual GPs and nurses typically had a portfolio of strategies that included not only defending, but also accommodating strategies, which aimed at accommodating both actors’ interests. We therefore further analysed our data to uncover when individual GPs and nurses chose to engage in which strategies, which brought to the fore the notion of different forms of trust. Last, we analysed our data regarding the sequences in which the strategies were enacted in practice in order to outline interactions of strategies and outcomes.
Since our data-collection and analysis phases overlapped, we were able to test emerging concepts and themes to establish the trustworthiness of our study. We conducted member checks with field members to ensure that our analysis and interpretation were accurate (Nag, Corley, & Gioia, 2007). Triangulation further ensured trustworthiness: We were able to get various perspectives on our phenomenon from multiple researchers with different scholarly backgrounds (organization studies and medicine), multiple respondents (GPs and nurses), and multiple sources of data (interviews and observations) (Lincoln & Guba, 1985).
First-Order Findings
The goal of IPC between GPs and nurses is optimal resident care, a goal that all interviewees emphasized as being fundamental to their work and their IPC. However, their contextual constraints led professionals of both groups to pursue additional interests in their IPC. The core additional interest of nurses is to safeguard themselves, since they are residents’ primary caregivers, have a limited ability to assess ambiguous resident conditions, and fear the (legal) consequences of taking action too late. To safeguard themselves, they want to involve GPs as much as possible and as soon as there is ambiguity about a resident’s condition. Self-employed GPs, on the other hand, want their interactions in IPC to be as efficient as possible—specifically, they only want to visit the nursing home when they believe such involvement is indicated. These two interests frequently competed, resulting in different conceptions of the location of the interprofessional boundary, with both professionals trying to limit their involvement.
Professionals’ boundary work to pursue competing interests resulting from contextual constraints
Our analysis revealed that both GPs and nurses held a portfolio of various boundary-work micro-strategies to achieve their respective interests, including micro-strategies aimed at pursuing only their own interest and boundary limitation without considering the other professional’s interest (which we labeled ‘defending strategies’) and micro-strategies aimed at taking into account both parties’ interests (which we labeled ‘accommodating strategies’).
Category 1. GPs’ defending strategies: Demanding limitation of their own boundary
In order to pursue their goal of efficiency, we found GPs using three micro-strategies to limit their own boundary and involve nurses more: educating nurses, empowering nurses, and ordering nurses.
GP efforts at educating nurses were aimed at limiting GP involvement by teaching nurses to be more aware of efficiency in their IPC. Educating nurses involved giving them feedback about processes or practices that GPs perceived as inefficient, such as when nurses called them about minor issues that did not require immediate action.
I have educated [nurses]. . .I have taught them not to call [me] with minor issues; only if it’s urgent.
GPs’ education efforts extended to educating nurses about medical topics. GPs explained to nurses the rationale for their decisions and orders, with the aim of helping nurses understand the situation, enabling them to more independently assess it, and motivating them to contribute to a more-efficient IPC with less GP involvement.
I notice they don’t quite understand where my thought comes from. . .Then it is important that I explain it briefly. Or twice or three times, so that they understand it.
The second strategy GPs employed was empowering nurses. Empowering nurses entailed actively handing over authority to them; for example, by providing on-demand medical prescriptions. GPs filled out and signed medication plans and prescriptions and left them with nurses to use in ambiguous resident situations. As one GP told us, You have to schedule on-demand medication from the start, so that something like nausea or vomiting or diarrhea or pain or fever does not always lead to consultations just because [nurses] have to justify dispensing the medication. . .If this is documented and filed. . .beforehand, no doctor will be called.
Empowering nurses is a strategy that gave them the autonomy to take decisions on their own, allowing GPs to reduce their involvement and responsiveness. This strategy also involved GPs purposefully showing appreciation for nurses’ engagement, such as complimenting them when they carried out tasks and took decisions on their own, to increase nurses’ confidence and encourage them to more-actively engage in the IPC.
I think it’s not only about the medical advice, but you need to show appreciation when they have actually thought about what they tell you. You shouldn’t just treat them as a diaper changer.
Ordering nurses is the third micro-strategy GPs used to bring about more involvement of nurses. While self-employed GPs have no formal authority to direct the actions of nurses (who are employed by the nursing home), we found that GPs openly demanded that nurses get more involved. As one GP reported, I demand. . .that at least blood pressure and perhaps also the diabetes and the urine [tests] and such things. . .have already been done in advance.
GPs considered taking blood pressure and giving injections to be very time-consuming tasks, especially when these were the only reason for a nursing-home visit. For nurses, however, these orders left them with the responsibility over the situation, which often conflicted with their safeguarding interest.
Taken together, GPs’ defending strategies were aimed at establishing a modus operandi on the relationship level that increased nurses’ involvement in IPC in order to achieve more efficiency for GPs, thus limiting their own boundary and requiring nurses to go beyond their ideal boundary position. We found that GPs often applied strategies in concert and that educating, empowering, and ordering nurses complemented one another to systematically prevent nurses from involving GPs too soon in ambiguous situations.
Category 2. GPs’ accommodating strategies: Accommodating both parties’ interests
GPs’ accommodating micro-strategies took into account both their own efficiency interest and nurses’ safeguarding interest by offering fixed interaction opportunities, providing loopholes for nurses, and making IPC personal.
The first micro-strategy, offering fixed interaction opportunities, included offering fixed discussion times before consulting with residents during regularly scheduled on-site visits and being open and responsive to requests during these visits. While these offers required GPs to regularly invest time, fixed interaction opportunities allowed nurses to resolve problems in a timely manner, making it easier for them to temporarily postpone minor requests to GPs and to instead collect them and not contact GPs for every individual request. One GP told us, I believe that regular visits are useful for absorbing. . .simple, non-important changes of conditions, so on all the other days. . .they give you the opportunity to really only react to important and urgent issues.
Another GP stated, In my experience. . .if there is a fixed structure, the less-relevant issues just disappear and [fewer] inquiries [are] necessary. It is like a rope with many knots, [that nurses] can safely hold on [to].
GPs often combined fixed interaction opportunities with a second micro-strategy—providing loopholes for nurses—which was aimed at ensuring that nurses had the opportunity to directly interact with GPs in severe cases. One example of such a loophole was GPs giving out their (oftentimes private) mobile phone number or a special office number that allowed nurses to get a direct response from the GP in urgent cases.
They have my mobile phone number, where they [can] call me directly. And then I can give direct instructions, either ‘I’ll come,’ or ‘Call an ambulance,’ or ‘Do this and that and call back in half an hour.’
GPs’ rationale for using this micro-strategy was to provide nurses with a feeling of safety, letting them know that in emergencies they get an immediate response. Having a loophole available encouraged nurses to deal more confidently and independently with ambiguous situations, and they were more likely to accept being temporarily in charge when residents had an ambiguous health situation. As one nurse told us, We have some GPs. . .we can also approach. . .on weekends, we have their mobile phone number. But. . .we have to decide, ‘Okay, this is urgent. . .I can’t wait until Monday.’
Nurses who knew that they could call anytime valued this service and typically called with smaller issues less often.
The third GP micro-strategy, making IPC personal, was aimed at creating personal relationships between GPs and nurses. GPs employing this strategy purposefully engaged in personal conversations with nurses and actively sought to create a friendly atmosphere. For example, they asked nurses about what they did in their free time: Asking for personal stuff, starting with, ‘How is it going? How was the weekend?’ and not straight away with ‘What do you have for me?’ It may take 20 seconds longer, but of course they feel recognized as a person.
During observations, we also witnessed GPs interacting with nurses as if they were friends or close colleagues, greeting them with a hug and joking around. GPs’ rationale in relaxing the professional barrier was to create a safe atmosphere for nurses, and to give them more confidence in their IPC, which GPs hoped would make nurses more willing to delay involving them in non-urgent cases.
When you get to know each other and you work together well, then they [nurses] know: ‘I can stretch [my] competencies up here, and only then call [the GP]’.
Even though this strategy required the GPs to invest time, it made IPC more efficient. For example, we observed that nurses who had a more personal relationship with GPs were more willing to wait to call them in seemingly non-urgent cases and to instead observe those cases on their own, reducing the overall number of calls to GPs because these minor instances often resolved without having to involve the GP.
Taken together, GPs’ accommodating strategies were aimed at establishing a modus operandi on the relationship level by implementing structural features into IPC to satisfy nurses’ safeguarding interests while also decreasing GP involvement. The aim of these strategies was thereby establishing a compromise boundary position. GPs often combined these accommodating strategies to complement one another.
Category 3. Nurses’ defending strategies: Insisting on limitation of their own boundary
Nurses engaged in efforts to enforce their goal of safeguarding and to limit their own boundary by emphasizing roles of GPs and nurses, tricking GPs into action, and bypassing interaction with GPs.
To limit their boundary, nurses’ first strategy was emphasizing roles of GPs and nurses. To avoid any ambiguity, nurses explicitly defined their limited scope of actions and insisted on maintaining it when residents indicated they felt unwell. We observed that nurses justified their stance by referring to their own legally constrained scope of actions and to the controls imposed on them by the German Health Insurance Medical Service. As one nurse told us, I can’t act without instructions, that’s my problem. Even if I knew what I should do, I am not allowed to do it. Sometimes it’s really logical [what has to be done], but I am not allowed to do it without instructions. . .I have no other choice, I can’t make the decisions. I am not a doctor, I am only able to do certain things and everything above that is not at my discretion and it is the doctors who need to decide how to proceed.
Nurses applying this strategy, we observed, contacted GPs even for small issues; for example, when a resident’s blood pressure changed only slightly. They justified their decision by explicitly referring to the law and the need for involving the GP. When residents showed signs of feeling unwell, we found that nurses often refused to independently assess the situation, even when the GP asked them to. One nurse told us, So I tell them, ‘Gee! Just come around and have a look [at the resident]! I cannot explain [certain] conditions over the phone!’
Nurses applied a second micro-strategy—tricking GPs into action—typically when the ‘emphasizing roles’ micro-strategy was not successful. In this micro-strategy, nurses forcefully requested that GPs visit a resident and take over responsibility as quickly as possible. Nurses deliberately exaggerated the urgency of situations to ensure that a GP would visit a resident on short notice, knowing that if they did not exaggerate, GPs likely would not make the visit. Exaggerating a situation left the GP with little leeway but to drive to the nursing home and see the patient. One GP was astonished that a nurse called and told him that a resident was sick with pneumonia. When he arrived at the nursing home, though, he found this claim to be strongly exaggerated.
[The nurse said,] ‘Yes, I intentionally described it [as an urgent case] because I knew if I explained it realistically, you [the GP] probably wouldn’t have come, but I wanted you to see her [the resident] before the weekend.’ That’s why he [the nurse] just said [on the phone], ‘She [the resident] has pneumonia’ and then she didn’t have pneumonia at all. ‘Yes, well at least you were here before the weekend and I’m safe’ [the nurse said].
In addition to employing such framing tactics, nurses also intentionally pestered GPs or their practices by repeatedly calling and sending faxes to try and get the visit to the resident. One nurse explained: . . .It’s about how quickly you get an appropriate response and all I can do is to pester the GPs, [and] the [GPs’] offices. Even if I am sorry for it. Yes, I pester them. Of course they are bothered, but as I said, I don’t call without a reason.
A third micro-strategy nurses adopted to achieve their safeguarding interest was an extreme form of defending: bypassing interaction with GPs. If nurses could not successfully persuade a GP to visit and consult with a resident, some nurses had another GP intervene instead. Some nurses went even further: Sometimes. . .we wait until the doctor’s office is closed. . .to then call the emergency service; they come to us and have another look [at the patient], so we get a second opinion when we are not satisfied with the result [of the GP’s assessment].
Nurses shared another form of bypassing: hospitalizing residents without informing the GP. Nurses justified their actions by claiming that a resident’s condition was extremely severe and required immediate action, even when the resident’s condition had only slightly changed. In contrast to all other micro-strategies, an unnecessary hospitalization may have negative consequences for the resident, given that hospitalization is a very stressful experience (Dwyer, Gabbe, Stoelwinder, & Lowthian, 2014). However, it is important to note that nurses—having little ability to assess the urgency of the situations—also have in mind the best interests of the resident when doing so, for example, because they believe that a GP may have misinterpreted the symptoms the nurse communicated. Nurses bear the risk when a resident needs intervention but does not get it, which may have adverse consequences for the resident and lead to accusations that a nurse has failed to render assistance.
Taken together, the nurses’ defending strategies were aimed at quickly absolving themselves of responsibility in ambiguous situations, thus limiting the own boundary. While each strategy had a different degree of forcefulness, we found that nurses applied them in escalating fashion; for example, using tricks when emphasizing roles did not work. The nurses’ defending strategies differed from GPs’ defending strategies in that the nurses’ strategies are ad hoc means to remove themselves from ambiguous situations and targeted singular, temporary solutions to limit their own boundary and resolve a specific case. Furthermore, the nurses’ defending strategies were more vigorous because they could immediately summon the GP and force them to get involved (by tricking GPs into action) or even terminate the collaboration altogether (by bypassing).
Category 4. Nurses’ accommodating strategies: Accommodating both parties’ interests
This category comprises nurses’ strategies that supported both their own safeguarding interest and accommodated GPs’ efficiency interest by finding alternative safeguards, offering input to GPs, and introducing facilitation objects into IPC.
In the first micro-strategy, finding alternative safeguards, nurses actively sought out and found alternative ways to safeguard themselves. Nurses applying this micro-strategy engaged, for example, in teamwork with other nurses to share and learn from others’ experiences and competencies, solve problems on their own, and thereby avoid unnecessary interaction with GPs.
I safeguard myself. . .[I] call [other nurses in the nursing home] and ask, ‘What do you think? What should we do now?’ and. . .mostly we agree [what to do]. . .That actually works quite well. . .we watch, check in frequently, take turns. . .and if it doesn’t improve, only then [do] we call a doctor.
Instead of immediately forwarding issues to the GPs, we observed that nurses using this micro-strategy engaged in problem solving by proactively measuring vital signs, checking a resident’s documents for previous symptoms and diagnoses, and repeatedly assessing the resident’s condition.
Well, I keep the resident under close control. I watch the resident closely; if necessary, every ten minutes, just to check how he or she is doing.
Observing the situation for a certain period and taking actions to stabilize a resident’s condition delayed GP involvement and—if a resident’s condition improved—avoided it altogether. The responsibility for the resident thus initially stayed with the nurse, supported GPs’ efficiency interest, and also served as an alternative way to fulfill the nurses’ interest for safeguarding.
A second micro-strategy nurses used was offering input to GPs. With this micro-strategy, nurses tried to support GPs by proactively sharing their experience of caring for the residents and giving GPs their opinion of residents’ conditions, for example, telling GPs about a resident’s personal problems or mental health when contacting GPs. Nurses used this knowledge to make suggestions to GPs, even though doing so is not part of their formal responsibilities and their opinion is not binding. One nurse explained: Simply communicating the symptoms, maybe also let them know what it possibly could be, because we know the residents. Sometimes you just know what’s going on, sometimes it’s psychological issues that physically [impact them] or [explain] why someone doesn’t eat or drink.
Nurses who proactively offered input aimed at speeding up and improving the quality of GP decision making, making it easier for GPs to assess residents’ condition over the phone and to distinguish less-urgent cases from urgent ones. These micro-strategies contributed both to the GPs’ efficiency interest and to the nurses’ safeguarding interest because this input helped GPs make more-thorough assessments.
So you try to prepare as well as possible for the doctors, so you can give them some input and say, ‘Look, now we have to do something here. We can’t do [what we’ve been doing] anymore.’
The third micro-strategy we observed was introducing facilitation objects into IPC. An example of nurses using this strategy was their documenting residents’ conditions in handouts, which helped both parties more quickly and easily process information. These handouts supplemented the standard resident records that nursing homes typically keep. Some nurses went even further, creating a dedicated visit book to present to the GP, in which they had compiled minor issues and questions about residents—thus allowing them to temporarily postpone involving the GP while ensuring that any concerns about residents were resolved in a timely manner. Having a visit book enabled GPs to easily and quickly deal with all open issues during their regular visits and provided structure to nurses’ conversations with GPs. One nurse told us: During the week, we get together and write down. . .questions for the doctor, information for the doctor. . .And then I go through every column in the system with the doctors and their patients and then we work this off [one-by-one].
Other objects included nurses’ self-made forms for informing GPs about residents’ deteriorating conditions or requests for prescriptions. We observed that nurses often prepared these objects so that GPs just had to sign them or fill in a few lines. These customized objects not only provided nurses with a safeguard, they were also convenient for the GPs because they could quickly assess information and efficiently respond to requests.
Taken together, nurses’ accommodating strategies were aimed at accommodating GPs’ efficiency interest, while also satisfying nurses’ own safeguarding interest and compromising on the boundary position. Nurses applying these micro-strategies were more actively engaged in the IPC and even extended to some extent their preferred boundary location. Nurses applied these strategies either in concert or stepwise; for example, nurses would first monitor a patient and take vital signs before offering input to GPs. In contrast to the nurses’ defending strategies, their accommodating strategies were more forward-looking and were aimed at creating a modus operandi for IPC relationships.
Second-Order Findings
Micro-level boundary-work strategies in context: The roles of power and trust
In a subsequent step, we looked more closely at the contextual properties under which these strategies were used (Corbin & Strauss, 2008). Our analysis was guided by two observations from our first-order findings. First, GPs and nurses both used defending strategies that aimed at enforcing their own interests against the other actor’s interest, which therefore required the use of power. Prior boundary-work literature has particularly emphasized that high-status professionals (such as GPs) have the ability to use power (Comeau-Vallée & Langley, 2020), yet we found that nurses’ (low-status professionals) ad hoc defending strategies were even more vigorous than the strategies that GPs used. We therefore further explored the underlying sources of power that allowed GPs and nurses to make use of their defending strategies. Second, we found that individual GPs and nurses typically had a portfolio of both defending and accommodating strategies. We therefore further analysed when individual GPs and nurses chose to engage in their respective strategies—which brought to the fore the notion of different forms of trust in the collaborating partner.
Figure 2 provides an overview of our findings.
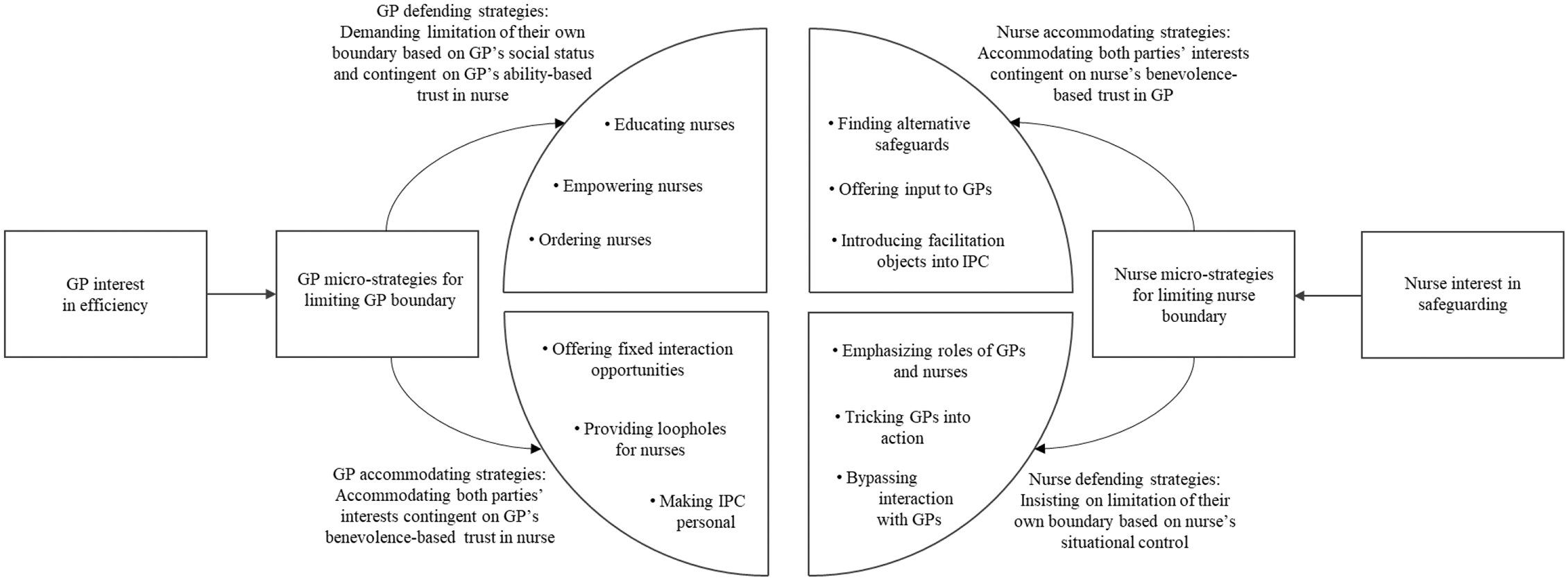
Boundary-work micro-strategies in response to competing interests arising from contextual constraints.
Social status and situational control as power sources for defending strategies
When actors try and impose their own interests against another actor’s interest—as in the defending strategies—they must rely on sources of power. Power is thus a recurring notion in the boundary-work literature (Nugus, Greenfield, Travaglia, Westbrook, & Braithwaite, 2010) and is often associated with actors’ social position. The medical profession has an inherently high social status, which determines boundary-work strategies and outcomes (Allen, 2000; Bucher et al., 2016) because it provides physicians with a taken-for-granted authority. Our data confirms this notion, which one GP exemplified when he told us, If the doctor says, ‘We do it that way,’ then they [nurses] are fine with it.
This position allowed the GPs to openly engage in strategies to enforce their interests, such as teaching nurses to cater to their efficiency demand or to give them direct orders. As one nurse stated, If the GP says, ‘We do it that way,’ then we have to do it, of course, whether I am pleased with it or not.
Unlike most physician–nurse IPC in hospitals, in our study GPs and nurses operated in a setting without formal hierarchy and in which GPs had no formal authority to give nurses directives. Even so, GPs’ higher social status provided them with the opportunity to order nurses to do something, allowing GPs to openly limit their boundary even if doing so came at the expense of the lower-status actors’ interest.
While the role of social-status power in enforcing interests is not surprising given prior boundary-work literature (e.g., Comeau-Vallée & Langley, 2020), we found that nurses—as the low-status group—also engaged in defending strategies, and that these strategies were able to trump GPs’ defending strategies based on nurses’ situational control. Nurses’ defending strategies were based on their unique knowledge of residents and on the fact that the residents were located in the nurses’ spatial domain. In contrast to GPs, nurses interacted with residents every day. They typically knew them, their families, and personal backgrounds very well. As one nurse told us, We know the residents in their daily life. We see them every day and know how they walk, how they eat, how they speak, and [we] can sense changes easily.
Because of the GPs’ physical distance from the nursing home, which prevented them from obtaining situational insights about the patient’s actual condition, nurses had a situational advantage that gave them the ability to influence GP actions. As another nurse told us, Well, I try. . .to frame the situation as best as possible. . .because I see [the resident] every day.
GPs have a moral and legal obligation to ensure residents’ medical care and visit the resident in case of a medical need. Thus, they have little leeway but to drive to the nursing home and see the patient when the nurse describes a non-urgent situation as urgent. Information asymmetry enabled the low-status nurses to frame a situation as risky for the high-status GPs, removing any ambiguity about the boundary location and precluding the opportunity for any further negotiation. The task—and the associated risk if the task was not fulfilled—was now unequivocally located in the domain and responsibility of the GP.
These findings provide interesting insights that inform boundary-work research. Boundary-work literature highlights the notion that power underpins boundary-work activities (Langley et al., 2019), emphasizing that high-status actors are the ones that primarily base their boundary-work activities on power and tend to ‘win’ (Comeau-Vallée & Langley, 2020). How low-status actors make effective use of power is so far less explored in the boundary-work literature, even though early boundary-work studies indicated that different power sources may play an important role (Allen, 1997). This lack of research is particularly surprising because negotiated-order theory—a main theoretical root of boundary-work studies on the micro level—has emphasized the multiplicity of power relations in negotiations, positing that different actors rely on different sources of power (Strauss, 1978). This notion is also reflected in research on micropolitics in organizations, where Crozier and Friedberg (1980) argued early on that actors gain and make use of power by controlling ‘zones of uncertainty’. Exploring nurses’ safeguarding interests and their resulting boundary-work micro-strategies based on situational control—which effectively means controlling ‘zones of uncertainty’—allows us to highlight how alternative sources of power are strategically applied and are forcefully at play in boundary-work dynamics. Comeau-Vallée and Langley (2020) have recently shown how a low-status group’s collectivizing attempts, which were intended to strengthen their position in boundary negotiations, were unsuccessful and even backfired, further weakening the group’s position. Our findings indicate that low-status actors’ situational control can allow them to remove ambiguity about the location of the interprofessional boundary, which renders their micro-strategies effective in everyday boundary disputes. Boundary work on the micro level is necessary and possible because the complexity of everyday IPC often involves ambiguity about the exact location of interprofessional boundaries that distinguish tasks and roles within IPC, making it difficult to clearly define which professional should conduct which tasks in IPC (Comeau-Vallée & Langley, 2020). Through their defending strategies, based on physical distance and resulting information asymmetry, nurses created a situation in which such ambiguity was no longer a given. Instead, responsibility and risk were clearly located in the GP domain, coercing them to accept the boundary in the location the nurse preferred.
While nurses’ defending strategies proved effective, it is however important to note that their power source only gave them influence in singular cases and only as a last resort to enforce their interest over a GP’s. Situational control as the sole form of power thus precluded nurses from enacting more complaisant and forward-looking boundary-work strategies that the social-status power of GPs allowed for. We believe that more systematically exploring low-status actors’ use of power in boundary work is an interesting topic for future research.
Exploring nurses’ situational control as a source of power also corresponds with Langley et al.’s (2019) call to further explore the role of physical space in boundary work. In our study, nurses’ power resulted from residents being located within the nurses’ physical domain, resulting in information asymmetries between GPs and nurses that nurses could use strategically. Physical space in IPC was thus crucial for harnessing power and being effective in boundary disputes, presenting additional opportunities for future research.
Benevolence- and ability-based trust as conditions for micro-strategy choice
Because our first-order findings showed that individual GPs and nurses typically engaged in both defending and accommodating strategies—that is, individuals had a portfolio that includes both types of strategies—we were also interested in when they applied which strategies. When we further analysed our data, we found that different forms of trust that an individual GP or nurse has in the collaborating partner influenced which strategy they applied. The notion of trust may at first seem paradoxical, given that we were considering two parties seeking to achieve competing interests. Yet a recurrent pattern in our interviewees’ accounts revealed that their application of strategies depended on their believing that a specific partner can appropriately cope with the implications of these strategies. GPs and nurses purposefully chose the partner with whom they would use strategies because applying strategies implied risk—either for the initiating actor or even for the resident.
Employing accommodating strategies involved taking into account the other party’s interest and thus required an investment and concession from the initiating party. In other words, accommodating strategies entailed costs and risk and thus required that professionals believed that the investment would not be exploited. Simply put, these strategies required benevolence-based trust (Mayer, Davis, & Schoorman, 1995). A GP pursuing strategies to accommodate a nurse’s interest, such as providing a loophole to the nurse by handing over a private mobile number, required that the GP believed in the nurse’s goodwill to not exploit this opportunity. For example, we observed a GP handing over her mobile phone number to a nurse on a small piece of paper, saying to the nurse, ‘Here, you can call me if conditions get worse, but don’t pass it on [to other nurses]. I trust you.’ By handing over this number, the GP implied that the nurse could contact her at any time—on weekends, on holidays, at night—and required a leap of faith (Möllering, 2001) from the GP that the nurse would not take advantage of or abuse this opportunity. The notion of the other party’s benevolence was also prevalent in the nurses’ accounts of their accommodating strategies. A nurse pursuing these strategies required to have benevolence-based trust in the respective GP, for example, when a nurse offered an explanation for a resident’s condition. Such stretching beyond the preferred boundary location accommodated a GP’s efficiency interest but also created risk and did not fully align with nurses’ safeguarding interest. A nurse who offered input about a resident’s condition risked being wrong which, if true, could have annoyed the GP because it would have increased rather than reduced inefficiencies. As one GP told us, That has a lot to do with trust. When they [nurses] know they can trust the GP. . .then it’s okay; if not, they forward every single issue because they don’t want to do something wrong.
To engage in accommodating strategies, nurses commonly referred to the need for believing in a GP’s benevolence, so that independently carrying out these activities would not have negative consequences. Trust, then, can provide the necessary psychological safety that allows one party to give up their preferred boundary location to some extent, take a risk, and meet the other party halfway.
With regard to GPs’ defending strategies, the belief that nurses had the necessary skills and competence to cope with their involvement beyond their preferred boundary location was a recurrent notion in our interviewees’ accounts. GPs engaging in defending micro-strategies (demanding nurses to transcend their preferred boundary location to some extent) required that GPs had ability-based trust in a respective nurse, the belief that the other party will be able to complete a given task (Mayer et al., 1995). For example, demanding that nurses conduct specific tests or watch for specific changes in a resident’s condition entailed the risk that the nurse might make mistakes which, for the resident, could be fatal. Believing that a nurse has high levels of expertise and competence allowed GPs to enforce their own interests without endangering the overall goal of resident well-being. As one GP, who ordered certain nurses to measure and monitor the blood glucose level of residents, told us, I have to trust [these nurses]. If they cannot assess the blood glucose level correctly, it can be dangerous [for the resident].
Another GP, talking about some nurses she had taught to collect vital parameters on their own before calling, commented, It works very well [with these nurses]. If I ask ‘How is the fever now?’, then I can be sure to get the numbers immediately because they have already done it. It depends on how competent they are, on how well they are trained.
These findings inform the boundary-work literature because they highlight how specific boundary-work strategies are contingent on trust in the collaborating partner and reveal that multifaceted forms of trust are at play. While notions of power have been given ample attention in the literature as governing conditions of boundary work (Langley et al., 2019), the notion of trust as a relational mechanism in boundary work has been virtually absent from this research (for notable exceptions see Meier, 2015 and Kilpatrick, Lavoie-Tremblay, Ritchie, Lamothe, & Doran, 2012). This absence is particularly surprising because for decades organization studies have explored the role of trust in collaboration (Nooteboom, 2002). Still, boundary-work literature—despite its interest in collaboration—has rarely considered this relational mechanism. Allen (1997) mentioned more than twenty years ago that trust may play a role in boundary work, highlighting that nurses were more likely to engage in boundary-blurring activities when these activities benefitted physicians they trusted, but she did not further elaborate on this notion. Our findings on the role of benevolence-based trust connect with these initial observations and make them more explicit and specific. When actors engage in boundary-work strategies that require an investment—thus putting the initiating actor into a risky position—benevolence-based trust can be the relational mechanism that makes taking that risk acceptable.
As mentioned above, two initial studies that have initially engaged with the role of trust in interprofessional boundary work are the works of Meier (2015) and Kilpatrick et al. (2012), highlighting how trust is an important aspect of boundary work for collaboration across professions, particularly when boundary work is trying to dissolve traditional boundaries and when contextual conditions are challenging. While she did not explicitly discuss the form of trust, Meier’s (2015) study illustrated how trust in another party is vital for establishing a ‘common ground’ for boundary work. As our study shows, ability-based trust is an important condition that ensures that boundary-work strategies do not put the overall goal that everyday IPC seeks to achieve at risk. As ability-based trust creates ‘common ground’, it is particularly necessary when demanding the other party to extend their preferred boundary location. We fully agree with Meier’s (2015) notion that the role of trust in boundary work deserves much more attention.
Interaction of strategies and outcomes
While our level of analysis is the individual GP and nurse, the comprehensive insights of our first- and second-order findings also allow us to tentatively outline how different constellations of trust between actors relying on different sources of power are likely to lead to different interactions of strategies on the bilateral level and to different outcomes.
The starting point for all constellations is a resident indicating they feel unwell and the nurse having to decide how to react. First, a GP who trusts in a nurse’s ability and has therefore engaged in defending strategies at an earlier point in time (e.g., by having empowered the nurse) implies a limitation of the GP boundary—assuming the nurse goes along with this demand. The nurse, however, is then stuck with responsibility for the resident for a longer time, thereby hindering safeguarding interests. As one nurse told us, There are GPs who say. . .‘Administer this medication and continue monitoring’ [instead of coming to the nursing home]. That’s bad because we have no safeguard.
A nurse who then responds with defending strategies (e.g., by bypassing interaction), fends off the GP’s efforts to limit the GP boundary, and instead enforces a limitation of the nurse’s boundary. As one GP explained, If I decide, ‘He [the resident] does not go to the hospital’ and they [the nurses] are like, ‘Oh that’s a bad decision,’ they—in case of doubt—do it in the evening with the emergency service and say, ‘Oh he had to go anyway. . .he got worse.’
If the nurse, however, has benevolence-based trust in the GP, the nurse may also engage in accommodating instead of either defending or simply going along. As one nurse told us, I consider very well how urgent I make it. . .I don’t want to burden the GP with something unnecessary.
This interaction (GP defending and nurse accommodating) implies the least extent of boundary limiting for the nurse because the GP not only extends the nurse’s preferred boundary location, but the nurse proactively gets further involved as well. This outcome is conducive to the GP’s interest, while the nurse achieves partial safeguarding by alternative means (e.g., by discussing with other nurses, thus sharing responsibility).
Second, when the GP trusts in a nurse’s benevolence and has implemented accommodating strategies, these strategies satisfy the nurse’s safeguarding interest and limit the nurse’s boundary. The GP’s accommodating strategies will in part satisfy their efficiency interest, yet these strategies require the GP to have made time investments. When the nurse likewise trusts in a GP’s benevolence and thus engages in proactive accommodating strategies (e.g., by finding alternative safeguards, thereby slightly shifting their preferred boundary and allowing the GP to limit their boundary), both parties make an investment (additional work for the GPs, nurses being held responsible longer), yet the situation has improved for both sides. As one nurse told us, If there is a deterioration and I know the GP visit is scheduled for tomorrow, I write it into the doctor’s documentation [instead of calling the GP] and deal with it tomorrow.
A nurse engaging in defending strategies in response to a GP’s accommodating is rather unlikely. The nurse’s interest has already been satisfied and there is little need for the nurse to engage in defending strategies. Thus, GPs who have applied forward-looking accommodating strategies render obsolete nurses’ applying defending strategies.
Third, when a GP holds both ability- and benevolence-based trust in a nurse, the GP may have engaged in a combination of defending and accommodating strategies (e.g., having empowered nurses and having provided them with loopholes). In this scenario, the GP’s defending strategies have limited the GP boundary, while at the same time the accommodating strategies provide safety for the nurse. In this constellation, again, a nurse employing defending strategies is unlikely. When the nurse then even additionally trusts in a GP’s benevolence and engages in accommodating strategies, the situation will further improve for the GP.
The above considerations illustrate the dynamic and processual character of boundary work in IPC (Comeau-Vallée & Langley, 2020; Quick & Feldman, 2014) and reveal how the choice of strategies is influenced by the sequence of strategies applied. In particular, forward-looking boundary-work strategies that have established a specific modus operandi on the relationship level can reshape the negotiation context for the other actor, thereby impacting the further process and its outcomes. For example, if GPs have applied accommodating strategies and thus provided nurses with a safeguard, nurses’ employing of defending strategies becomes unlikely. However, while the long-term orientation of GPs’ strategies may shape individual instances ex ante, nurses can break up the negotiation for their own benefit by applying ad hoc defending strategies when their interest in safeguarding is not addressed, such as when GPs have applied defending—instead of accommodating—strategies. Nurses’ defending strategies are then a counterweight to the decisive nature of the GPs’ moves.
Discussion
Using qualitative data on the everyday IPC in Germany between self-employed GPs and nurses employed in nursing homes, we studied how professionals engage in boundary work to limit their boundaries in response to competing interests that arise from their contextual constraints. Our contribution to the literature on boundary work and IPC is threefold. First, we provide a comprehensive understanding and framework of professionals’ boundary-work micro-strategies to limit their own boundary as well as the interplay and effects of these micro-strategies. Professionals not only engage in boundary-work strategies to achieve the overall goal of IPC (e.g., Apesoa-Varano, 2013; Liberati, 2017), to protect or expand their professional jurisdiction or status (e.g., Allen, 2000; Håland, 2012), or to enforce their specific professional approach for completing a shared task against the background of their professional identity (e.g., Comeau-Vallée & Langley, 2020). They also do so in response to their contextual constraints and resulting competing interests, which may lead professionals to engage in boundary work to limit their own boundary instead of protecting or expanding it. Our study provides a fine-grained understanding of the forms and nuances that boundary work takes in this case. In particular, we find that professionals typically hold a portfolio of micro-strategies, including both defending strategies—solely aimed at limiting their own boundary—and accommodating strategies—aimed at taking into account both parties’ interests and preferred boundary location. Furthermore, outlining the interactions of strategies illustrates how the outcomes of professionals’ bilateral boundary work depend on the sequence of these strategies, which points to the adaptive choice and temporal nature of boundary-work micro-strategies (long-term vs. ad hoc). In particular, forward-looking boundary-work strategies that establish a specific modus operandi on the relationship level can reshape the negotiation context for the other actor and thus the later process and its outcomes.
Our second contribution is advancing our understanding of the role of power sources in boundary work. Our analysis revealed how both GPs and nurses engaged in defending strategies, which required using power. Extant boundary-work research has highlighted that boundary work and its outcomes are strongly driven by social-position–based power, while low-status actors have been found to be less successful in harnessing power for boundary-work activities (Bucher et al., 2016; Comeau-Vallée & Langley, 2020). Our study draws attention to situations in IPC that might be more or less likely to privilege low-status actors’ situational control over social status as a source of power in boundary work. As our findings suggest, power based on situational control trumps power based on social status when information asymmetry between actors—resulting, for instance, from physical distance or different knowledge bases—allows the low-status actor to frame a situation that removes any ambiguity about the location of the interprofessional boundary, thus precluding any further negotiation. These findings invite future boundary-work research to further explore sources of low-status actors’ use of power in boundary-work activities. Prior studies on physical space (Boon, 2007) and physical control over objects in boundary work (Bechky, 2003) may present fruitful starting points.
Third, our study contributes to understanding trust in boundary work, a central relational mechanism in collaboration (Nooteboom, 2002) that so far has not been given much attention in the boundary-work literature. Our findings reveal a nuanced picture of how different forms of trust are important for applying micro-level boundary-work strategies, thereby shedding light on how variations in micro-level boundary work relate to different conditions and contingencies (Langley et al., 2019). In particular, our findings show how the risks involved in boundary-work strategies (either for the initiating party or for achieving the overall goal in IPC) determine the form of trust necessary (benevolence-based or ability-based trust) for applying specific micro-strategies. Based on our study and on initial studies that have pointed out the role of trust in boundary work (Kilpatrick et al., 2012; Meier, 2015), we believe that trust in its different forms is a crucial yet neglected condition of boundary work that should be explored in more depth.
Our study is not without limitations. First, we focused on a very specific empirical context—the IPC in Germany between self-employed GPs and nurses employed in nursing homes. We believe that similar dynamics between high- and low-status actors who have a shared goal but who face contextual constraints and thus want to limit their boundaries are likely in other healthcare settings (e.g., between pediatricians and childcare workers, and between psychologists and social workers) but also in IPC beyond healthcare (e.g., between scientists and technicians working on experiments in laboratories or between lawyers and social workers working with adolescent clients). Still, future research should explore whether other settings (for example, acute-care hospitals or university hospitals), other countries, and other industries produce different micro-strategies and dynamics. Second, exploring the long-term effects of boundary-work strategies in recurring interactions was beyond the scope of our study. For example, the nurses’ defending strategies were highly effective, yet such strategies might prove problematic when applied recurrently. Such dynamics are an interesting topic for future research. Third, while different forms of trust emerged as important conditions of micro-strategy choice, there may be other conditions and contingencies that our data did not reveal. Further research in this regard should thus explore additional factors, including those on the individual level (e.g., professionals’ self-efficacy or risk propensity).
Last, the empirical setting of our study has some practical implications. In particular, ensuring that nurses have safeguards in their IPC seems to be paramount. One way to foster these safeguards would be implementing structural features into IPC, such as having GPs provide emergency phone numbers, which would accommodate both efficiency interests and safeguarding interests. From a policy perspective, the recent political efforts to implement cooperation contracts between GPs and nursing homes (Fleischmann et al., 2016), which may entail creating standard operating procedures for how to proceed in unclear situations, seem worthwhile for creating conditions that could improve the situation for all actors involved.
Footnotes
Acknowledgements
The authors would like to thank Senior Editor Jörg Sydow and three anonymous reviewers for their guidance, advice, and support. We further gratefully acknowledge helpful feedback on earlier versions of this article by Davide Nicolini, Ila Bharatan, Nitzan Rimon-Zarfaty, participants of the European Group for Organizational Studies (EGOS) Colloquium 2019, the Organizational Behavior in Health Care (OBHC) Conference 2020, the Annual Meeting of the Academy of Management 2020, and research-seminar participants at the University of Göttingen. We would also like to thank members of the interprof ACT working group and our research assistants for their support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Innovation Fund, Federal Joint Committee (grant number G-BA grant VF1_2016-079).