
Abstract
This article extends understanding of trust repair by explaining in more detail the dynamics of trust at the network level. Building on organizational-level trust repair research, the article explains how two periods of trust repair – catharsis and catalysis – contribute to trust repair of an interorganizational network. In addition, the article describes how changes to network-level trust in an interorganizational network change the governance form of the network, making the interorganizational network more durable and stable.
Times of crisis, of disruption or constructive change, are not only predictable, but desirable. They mean growth. Taking a new step, uttering a new word, is what people fear most.
Introduction
Interorganizational networks are increasingly used to address societal issues that cannot be solved by a single organization working alone (Provan, Fish, & Sydow, 2007). Trust is crucial to successful interorganizational collaboration (Bachmann, Gillespie, & Priem, 2015; Provan & Kenis, 2008). In this article we examine how trust repair in interorganizational networks unfolds following a network-level trust crisis. Building on previous organization-level trust repair models (Gillespie & Dietz, 2009; Pfarrer, Decelles, Smith, & Taylor, 2008), we describe two periods of trust repair following a network-level trust crisis that change the dynamics of trust and the governance form of an interorganizational network.
Trust in interorganizational collaboration has been extensively researched (Lane & Bachmann, 1998; Sydow, 1998) and mechanisms that maintain institution-based trust are well established (Bachmann & Inkpen, 2011). Research has extended our knowledge of trust repair between interorganizational dyads (McEvily, Zaheer, & Kamal, 2017; Stevens, MacDuffie, & Helper, 2015). Prominent trust repair models provide understanding of how organizations can work to repair trust following a transgression (Gillespie & Dietz, 2009). Kramer and Lewicki (2010, p. 246) ask whether trust repair can enhance trusting relations and make them ‘more durable and stable’. The related research questions that motivate our study are: How is trust repaired in an interorganizational network following a crisis, and with what effect?
We present a case study of an interorganizational network based in an English city, which makes up a child protection network. Mistakes were made that led to the death of Elsa, a teenager suffering from anorexia, who died despite interventions from a range of health professionals in primary care, mental healthcare and acute hospital settings. We studied the network for nine years in total. We carried out fieldwork for a year prior to Elsa’s death, and for two years following her death, between 2006 and 2009. We remained in touch with the network for a further six years, returning to the field again for another year, following the coroner’s inquest into Elsa’s death, in 2015.
Drawing on theory from prior trust research (Bachmann et al., 2015; Gillespie & Dietz, 2009; Pfarrer et al., 2008) and public administration literature (Kilduff & Tsai, 2003; Provan et al., 2007; Provan & Kenis, 2008) we present an analysis of network-level trust repair that extends trust repair research in two ways. First, we identify two periods of network-level trust repair: a period of catharsis and a subsequent a period of catalysis. Second, we show how these two periods of trust repair change the dynamics of trust in the network and its governance. Building on Bachmann and colleagues (2015) we show a relationship between the type of trust that is manifest and network governance form (Provan & Kenis, 2008). Our conclusion is that both trust relations and the network itself become more stable as a result of the two periods of trust repair (Majchrzak, Jarvenpaa, & Bagherzadeh, 2015).
Theoretical Background
First, we clarify how organizations trust. Second, we explain how interorganizational networks have a bearing on the type of trust that exists between the organizations and the constitution of trust at the network level. Third, we discuss extant organization-level trust repair models and theory.
How do organizations trust?
Organizations can place trust in interorganizational relationships to facilitate network-level collaboration (Weber & Mayer, 2011). Alternatively, organizations can place trust in the network to provide the necessary regulations to ensure that organizations can collaborate effectively (Bachmann, 2011). For analytical clarity we refer to the former as interaction-based trust and the latter as institution-based trust (Bachmann & Inkpen, 2011).
Institution-based trust provides apparatus for the instigation and ongoing maintenance of trusting relations between organizations. In routine times it may be a preferable basis for maintaining interorganizational trust (Bachmann, 2001; Lane & Bachmann, 1996). This is because formally established institutional safeguards provide clear guidelines for compliance by explicitly articulating standards for behaviour (Swärd, 2016; Zhou & Poppo, 2010). Organizations can therefore place their trust in institutional safeguards rather than investing valuable time and resources in establishing and maintaining many dyadic interorganizational relationships (Bachmann, 2011).
Interaction-based trust foregrounds relationships between organizations as the primary means of managing interorganizational collaboration (Kim, Dirks, & Cooper, 2009; Ren & Gray, 2009). The advantage of regular interaction is that it establishes a shared understanding among organizations as to how they collaborate (Janowicz-Panjaitan & Krishnan, 2009; Provan & Kenis, 2008). If there is too little trust, organizations will be unwilling to invest further in collaboration (Zaheer, McEvily, & Perrone, 1998) and will underestimate the capabilities of their collaborating organizations (Gulati & Nickerson, 2008). Too much trust between organizations can lead to blind spots (Lumineau & Oliveira, 2018) and path dependencies (Möllering & Sydow, 2019) in the relationship. An ‘optimal’ level of trust (Stevens et al., 2015) is dependent on the type of trust in the network, the extent to which collaborating organizations share mutual goals and the governance form of the network.
Interorganizational trust and network governance forms
While serendipitously formed interorganizational networks are opaque with respect to membership and relationships between the organizations (Kilduff & Tsai, 2003), purposefully established networks – so-called goal-directed whole networks defined ‘as a group of three or more organizations connected in ways that facilitate achievement of a common goal’ (Provan et al., 2007, p. 482) – provide an opportunity to empirically study interorganizational trust at network level. This is because membership of the network, its shared goals and the organizations’ accountabilities are made explicit. Provan and Kenis (2008) 1 suggest a relationship between the density of trust ties in a whole network and its governance form, proposing that the dynamics of trust will differ depending on whether a network is participant- or lead-organization governed.
Participant-led networks, where organizations share responsibility for network governance, will rely on a high density of trust ties so that understanding is shared among network members as they collectively take responsibility for network-level decisions. In theory, such a network is likely to consist of only a small number of organizations (Provan & Lemaire, 2012). This is because the type of trust that forms the basis for collaboration in shared governance is principally interaction-based (Edelenbos & Klijn, 2007) and relies on a dense web of trust-based ties to ensure that shared values are understood in order to guide network-level decision-making (Provan & Kenis, 2008).
Lead-organization governed networks rely on trust coordinated by a central entity, through which ‘all major network-level activities and key decisions are coordinated’ (Provan & Kenis, 2008, p. 235). Dyadic trust ties exist between the lead organization and each of the network members. The purpose of the trust ties is to ensure coordination of network members with regard to the network-level objectives. For lead-organization governance to be effective, organizations’ jurisdictional responsibilities should be clearly articulated so that organizations are able to trust the network’s structures and protocols. This governance form relies heavily on institution-based trust since organizations have limited interaction directly with each other.
How is trust repaired following a crisis?
Since trust is context bound (Bachmann et al., 2015), the way in which organizations trust and the governance form of the interorganizational network will affect interorganizational responses to a breakdown of trust. While in some cases organizations may simply be able to leave the network, collaborating organizations often become bound together (Möllering & Sydow, 2019). Thus, there is a need to understand how organizations collaborating in an interorganizational network can repair trust in ways that ensure that the same failures do not take place again.
Models of organization-level trust repair (Gillespie & Dietz, 2009; Pfarrer et al., 2008) outline two phases of trust repair. First, identifying who or what is to blame for the trust violation and any immediate responses required; and second, ensuring that appropriate action is taken to punish transgressions and clarifying measures required to mitigate against subsequent trust violations. Gillespie and Dietz (2009, p. 137) distinguish these phases as ‘distrust regulation’ and ‘trustworthiness demonstration’ and show that they require different trust repair mechanisms, an analysis of trust repair confirmed in other studies (Kim et al., 2009; Tomlinson & Mayer, 2009).
In these models it is assumed that a single organization is principally responsible for the violation of trust. However, the informal and formal arrangements that coordinate activity in interorganizational collaborations often blur (Long & Sitkin, 2018). Therefore, if a trust failure occurs at the network level, organizations may each perceive that they have fulfilled their jurisdictional responsibilities with respect to a trust violation. Legalistic remedies to punish an individual organization following a network-level trust breakdown will prove insufficient in repairing trust across the network unless there is clear evidence of an organization-level competence-based failure (Sitkin & Roth, 1993).
During the first phase of ‘distrust regulation’ (Gillespie & Dietz, 2009, p. 137) organizations seek to mitigate the risk presented by the trust crisis. They turn to ‘regulation and formal control’ mechanisms in an effort to repair trust (Bachmann et al., 2015, pp. 1130–1131). Organizations may attribute blame to the regulatory structures for the trust failure (Kim et al., 2009). If the failure is the ‘lack of ability’ of regulations to manage behaviours and coordinate activities then the governance mechanisms become the focus of trust repair efforts (Gillespie, Hurley, Dietz, & Bachmann, 2012, p. 187). Adjusting governance mechanisms has been shown to play a role in restoring trust in the regulations that govern interorganizational relations (Eberl, Geiger, & Aßländer, 2015; Spicer & Okhmatovskiy, 2015). Repairing trust in the governance of the network provides assurances that organizations can expect positive exchange between organizations once again (Kim et al., 2009) and addressing control mechanisms represents commitment to future relations (Klein Woolthuis, Hillebrand, & Nooteboom, 2002).
The second phase – ‘trustworthiness demonstration’ (Gillespie & Dietz, 2009, p. 137) – requires different trust repair strategies that show that lessons have been learned and acknowledge perceived failures. Research emphasizes the importance of apologizing to show that lessons have been learned (Lewicki & Brinsfield, 2017). An apology helps to demonstrate an understanding of the events that have taken place (Fehr, Gelfand, & Nag, 2010) and conveys a ‘desire to reconcile’ relations (Tomlinson, Dineen, & Lewicki, 2004, p. 169). Apologies thus signal a change in attitude towards trusting relations and assurance about the future (Lewicki, McAllister, & Bies, 1998; Lewicki, Polin, & Lount, 2016). While research shows that the timeliness of an apology is crucial (Gillespie & Dietz, 2009; Haesevoets et al., 2016), an apology must be supported by ‘social rituals and symbolic acts’ to demonstrate that the apology is sincere (Gillespie & Dietz, 2009, p. 135; Schweitzer, Hershey, & Bradlow, 2006). This includes committing money, time and manpower to demonstrate sincerity and commitment to change (Gillespie & Dietz, 2009).
Providing an apology to demonstrate trustworthiness is problematic at the network level if the failure is perceived to be in the governance mechanisms of the network. Organizations are unlikely to feel any need to apologize. Further, in the immediate aftermath of an interorganizational crisis, an apology can easily lead to blame being directed at the organization that is making the apology (Ferrin, Kim, Cooper, & Dirks, 2007), or the apology may be perceived as ‘cheap talk’ (Bottom, Gibson, Daniels, & Murnighan, 2002, p. 498). Responding to this particular challenge of trust repair at the network level and drawing on extant trust and network governance research, we examine an interorganizational network that encountered and then recovered from a network-level trust failure.
Research Context and Design
To explore the changes to the network we first reflect on the trust dynamics across the network prior to the crisis. Second, we reflect on the trust repair strategies adopted by organizations in the network in the immediate aftermath of the crisis. Third, we consider the trust repair strategy adopted by the lead organization after the initial crisis period. Fourth, we present data from the network six years after the crisis.
While maintaining the use of interaction-based and institution-based trust as two of the bases for interorganizational trust, we draw on what Mayer, Davis and Schoorman (1995, p. 724) refer to as ‘trusting action’. A decision to trust is therefore based on perceptions of the ability, integrity or benevolence of the referent and the willingness of the trustor to make themselves vulnerable in the expectation of positive behaviour from the trustee (Rousseau, Sitkin, Burt, & Camerer, 1998) as described by Stevens et al. (2015).
The case
Our study of the City Local Safeguarding Children’s Board (the CLSCB) proved a revelatory longitudinal case, meeting all the necessary conditions regarding trust breakdown and repair in an interorganizational network with the potential to provide rich description of, and explanation for, our theoretical concerns (Yin, 2003).
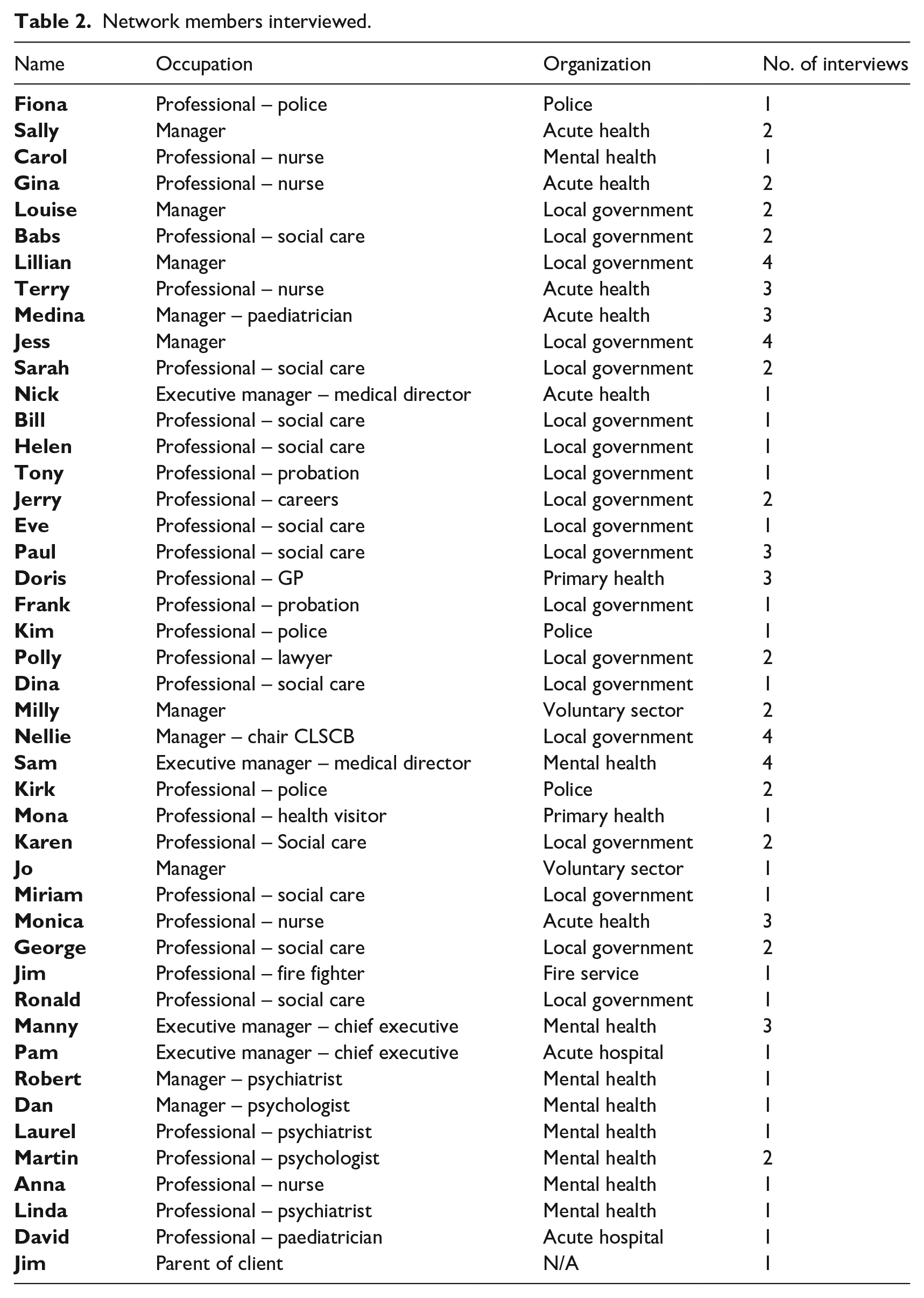
The CLSCB represents a goal-directed network (Kilduff & Tsai, 2003) with a lead-organization governance form (Provan & Kenis, 2008). The Chair is formally accountable for the CLSCB’s performance to the government regulatory agency. The network meets monthly and encompasses members from the acute hospital; the mental healthcare provider; primary care providers; police, fire and ambulance services; education providers; and voluntary sector organizations. The CLSCB’s membership over the nine years we engaged with it remained stable. This is illustrated by our ability to interview the same CLSCB members more than once (Table 2).
Trust broke down among members of the CLSCB following the death of Elsa who was a teenager suffering from chronic anorexia. Elsa had been subject to various clinical and therapeutic interventions from a range of health professionals in primary care, mental healthcare and acute hospital settings over six years. During this period her condition deteriorated, with her weight plummeting to 25 kilograms, eventually leading to her premature death from multiple organ failure in the intensive care unit of a hospital. Following the inquest into her death, the coroner noted that ‘systematic weaknesses in the organization of health services led to Elsa’s unnecessary death’, but was satisfied that the organizations involved in her care had remedied previous flaws (media report of coroner’s inquest, anon., 2015).
Fieldwork
Our case allowed us to examine the trust dynamics of the network before the crisis and well beyond the two episodes of trust repair that took place following the death of Elsa. We interviewed individuals who represented their constituent organizations and we made it clear to interviewees that our interest lay in their organizations’ interactions with the other network member organizations. A limitation of prior trust research is that it uses single informants as a proxy to assess interorganizational trust. Prior research relies heavily on a single informant from each organization such as a boundary-spanning individual (Williams, 2002) or partnership manager (Muthusamy & White, 2005). This means that the level of analysis is not clear (Currall & Inkpen, 2002). To address this, we interviewed multiple informants from the organizations across the network, sampled from different levels in the organizations. We supplemented insight from interviews with documents and observational fieldnotes to capture an aggregate perspective of each of the organizations in the network (see Table 1 for summary of fieldwork).
Timeline of the case organization and data produced.
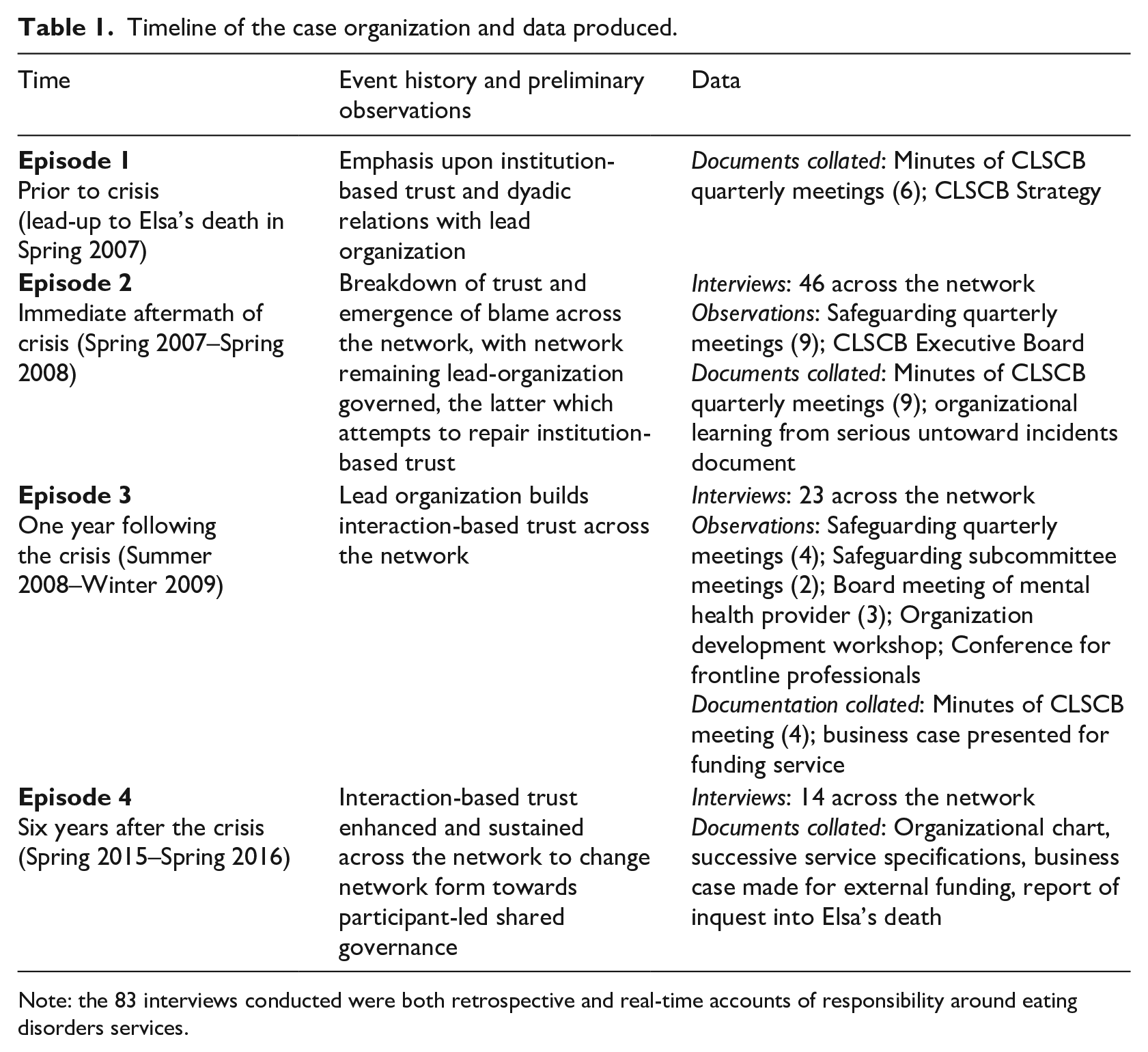
Note: the 83 interviews conducted were both retrospective and real-time accounts of responsibility around eating disorders services.
In total, we conducted 83 interviews with 45 interviewees over the study (see Table 2 for membership of the CLSCB and interviewees). Some informants were interviewed more than once as we judged that they provided particularly rich insight into the changing trust relationships between the organizations. Interviews ranged between 45 minutes and two hours. In addition, over 200 hours of meeting observations were undertaken (see Table 2). Observations were documented in field journals and the interviews were recorded using digital equipment, before being transcribed verbatim.
Network members interviewed.
Data analysis
Having collated documentary evidence, observations and interviews into a password protected case study database, we undertook our analysis. The need for authentic explanation called for more contextual accuracy at the expense of theoretical generality (Langley, 1999; Langley, Smallman, Tsoukas, & Van de Ven, 2013). For this reason, in our initial coding we pursued a temporal bracketing strategy, anchoring the data into episodes. Our analytical strategy was iterative in nature as we sought to interpret the complexity of trust relations and their interaction with the network form over time (Langley, 1999; Langley et al., 2013). Employing abductive reasoning (Locke, Golden-Biddle, & Feldman, 2008; Mantere & Ketokivi, 2013) we were driven by a focus on the theoretical problem in conjunction with the need to provide an explanation of the case (Alvesson & Kärreman, 2007). Our abductive approach promoted continual dialogue between theory and empirical findings, which underpinned an analytical strategy based on the continuous formulation and iteration of questions and answers from literature to both focus and explain emerging findings (Alvesson & Kärreman, 2007; Locke et al., 2008; Mantere & Ketokivi, 2013).
During this temporal bracketing process, each of the authors separately engaged in a fine-grained reading of the data, following which they formulated a narrative account of events preceding and following the eating disorder patient’s death. The production of a chronological narrative is a common first step in organizing data for further analysis and provides important validation as it allowed us to check our subsequent interpretations against this raw narrative (Langley, 1999). We then continued to examine organizational interactions and outcomes of their activities within the network, which allowed us to implement the temporal bracketing strategy and identify what were initially three episodes preceding and following Elsa’s death, and then subsequently a fourth episode on our return to the field.
These four episodes provide the structure for our empirical findings. True to the principles of abductive reasoning (Mantere & Ketokivi, 2013), our theoretical analysis of trust relations and their interaction with network form developed alongside our empirical analysis. While we accept that our account is one of many potential interpretations with respect to the network change observed (Van Maanen, 1988), we worked to ensure that we did not retrofit the data to service our theorizing (Wodak & Busch, 2004) in two ways. First, we considered and discussed several theoretical explanations, which were reflected in the different generations of data structures that we constructed during different stages of the research process. Using principles of abduction (Mantere & Ketokivi, 2013), we ruled out several theoretical explanations in search of the clearest explanation that best fitted the data (Mantere, 2017). In the coding process, we explored earlier generations of data structures built on concepts from literatures such as sensemaking, organizational learning and attribution theory. While all such literatures offered partial explanations for what had happened, changing trust relations and their effect on network form was found to be the clearest descriptor of the outcome. Second, we triangulated between data types. With unfettered access to the network granted by the Chair of the CLSCB, we ensured that we took advantage of opportunities to observe meetings and other events, as set out in Table 2, and to discuss our analysis of these against our interview analysis. As an example of our data triangulation, we interrogated the account of the chief executive of the mental healthcare provider (Manny), who attributed much of the organizational change to his own efforts. In part, this conclusion was validated during observations, but we judged a stronger explanation for the response towards initiating trust repair was attributed to the CLSCB Chair in our observational findings. The final generation of data structures for each episode, elaborating the empirical and theoretical concepts that underpin our data structure, is presented in Figure 1e.
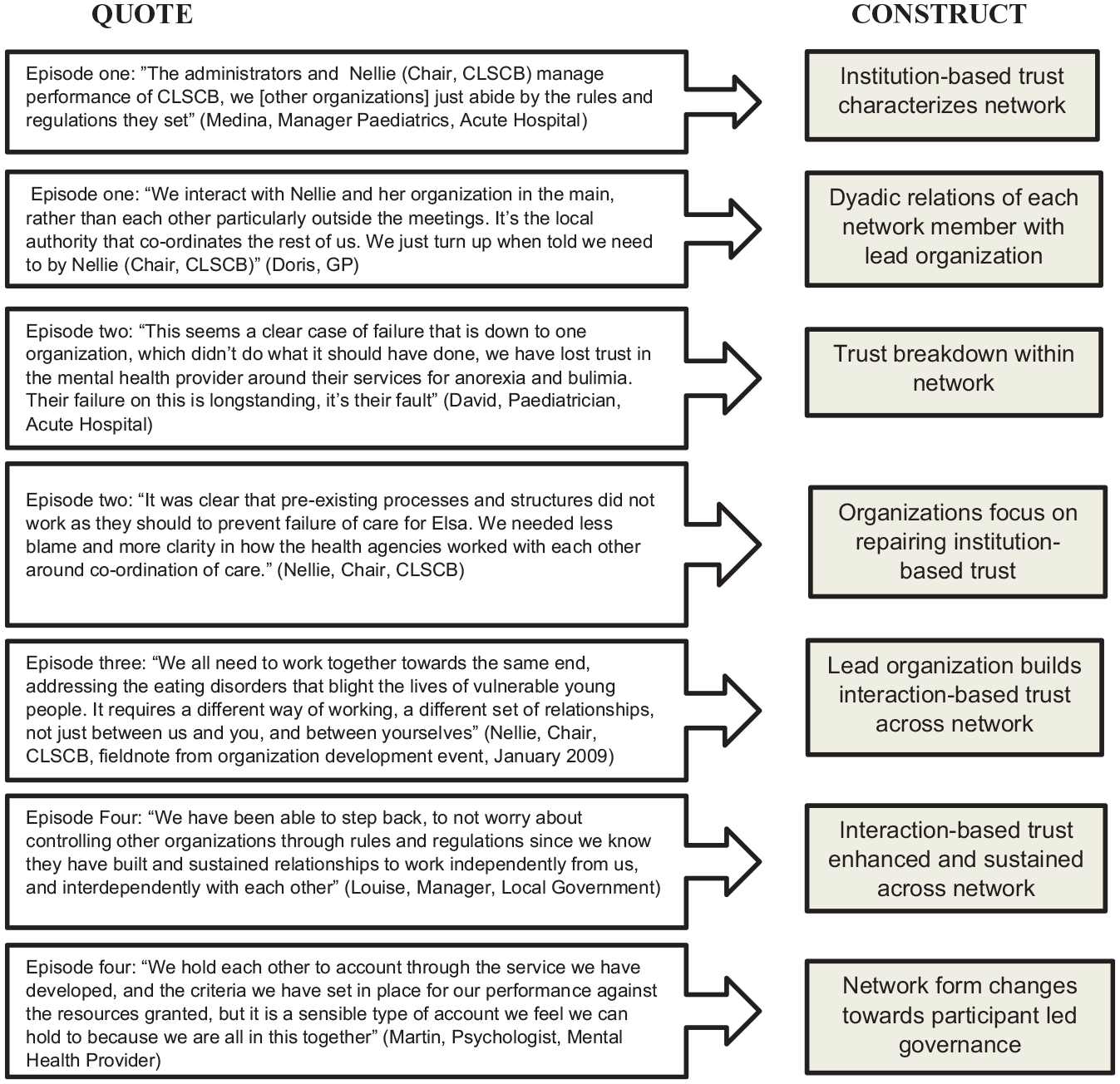
Coding structure.
Findings
We present data from the interorganizational network members at four points: (1) prior to the crisis (Spring 2006–Spring 2007); (2) in the immediate aftermath of the crisis (Spring 2007–Spring 2008); (3) one year following the crisis (Summer 2008–Winter 2009); and (4) six years after the crisis (Spring 2015–Spring 2016).
Episode 1 (Spring 2006–Spring 2007)
Prior to Elsa’s death, there were dyadic trust relations between the lead organization and constituent organizations, which ‘allowed the job of ensuring safeguarding to be done’ (Sam, medical director, mental healthcare provider). Professionals drawn from the organizations that made up the CLSCB ‘trusted them [the lead organization] to get on with it. They just co-ordinate our efforts and make sure everyone is doing what they should’ (Medina, nurse, hospital acute care). The lead organization, ‘ran the show. We arrange quarterly meetings, set the agenda, invite the relevant people along, and ask them to report back matters of concern. We can’t directly control what they [other organizations and professionals] do. They are not accountable to us’ (Lillian, administrator, CLSCB).
In a benign context in episode 1, the operations of the CLSCB seemed routine, with the constituent senior professionals of the CLSCB representing our organizations and reporting back to our organizations where we need to. For my part, there is a standing item in our Risk and Governance Sub-Committee for safeguarding, which I report on. (Sam, medical director, mental healthcare provider)
Another constituent member organization in the CLSCB viewed the network as a sideshow to our mainstream business. I turn up at the meetings, report to them, go back to base, get on with things. As long as nothing goes wrong, then everything is fine. Nothing much has gone wrong since I have been going along, the odd complex case, but we have well established protocols. (Nick, medical director, hospital acute care)
There was minimal interaction between the constituent professionals that represented their organizations within the CLSCB. Interactions were between the lead organization and each member. This was reflected in the informal interactions around the CLSCB meetings, with the Chair of the CLSCB commonly finding that they would phone ahead of meetings to touch base. Sam [medical director, mental healthcare provider], we just catch up and check everything is going smoothly, and he knows what he needs to do. It helps build trust between us. None of us will be surprised by anything raised in meetings. We deal with issues outside the meetings. I’m clear what I expect from them. (Nellie, Chair, CLSCB)
As one member of the CLSCB commented, ‘if there is a problem, they [Nellie, the CLSCB Chair] come to us since they are the ones accountable to the regulator for performance’ (Nick, medical director, hospital acute care). Nellie (Chair, CLSCB) observed that ‘the regulator hasn’t been too interested in us. We are performing well in terms of our safeguarding responsibilities against our protocols.’ These comments were to prove prescient.
Up to this point, characterized by lead-organization governance, and in a benign context, the network appeared to be functioning effectively in line with its goal-directed mandate. We observed dyadic relations between the lead organization and each of the CLSCB’s constituent members. These dyadic relationships were characterized by institution-based trust in the regulations. Dyadic relations between constituent members were correspondingly latent and dormant, since they appeared unnecessary. Member organizations trusted the regulatory structure and were held to account through their dyadic relations with the lead organization that were based on well-established protocols.
Episode 2 (Spring 2007–Spring 2008)
Following Elsa’s death in Spring 2007, trust in the network broke down. Organizations responded by underlining that they had adhered to the mandated rules, clarifying their own actions to other members of the network based on their jurisdictional accountability. Each of the organizations maintained that they had done everything that they could have done to provide an appropriate level of care as set out in protocols for addressing the condition of eating disorders. Doris [GP, representing the general practice providers in the city] argued that the GP that cared for Elsa discharged the professional jurisdictional tasks for which they were accountable: ‘the GP referred the patient to the hospital when required, so did their bit properly’ (field note from observation of CLSCB meeting, September 2007, p. 13).
After clarifying that they had adhered correctly to the rules, organizations involved in Elsa’s care questioned whether others had discharged their responsibilities as set out in protocols to prevent Elsa ‘falling through the cracks of care’ (Sam, medical director, mental healthcare provider). There was some concern raised about the lead organization, who had been ‘trusted to run it [the CLSCB meeting], but do they have the professional experience to do so?’ (Jim, GP). The dyadic relationships between the lead organization and other organizations broke down in the wake of Elsa’s death and trust in the governance mechanisms broke down as organizations perceived they had fulfilled their responsibilities as mandated by the lead organization. However, somewhat counterintuitively, blame was not placed upon the lead organization. Such was the governance structure of the network at this point that knowledge of working practices across the network was limited. Network members speculated that other network members might be to blame. Of particular note was the blame that the two largest healthcare providers in the CLSCB placed on one another: We are not working effectively together because of the suspicion each of our medical directors has about the other’s motives and actions. Each feels they are being ‘hung out to dry’ by the other for Elsa’s death. (Manny, CEO, mental healthcare provider)
Nick (medical director, hospital acute care) blamed the mental healthcare provider for the failure, based upon their professional jurisdiction: ‘ultimately this is a mental health failure. CAMHS [Children and Adolescent’s Mental Health Service] is responsible for eating disorders’ (field note from observation of CLSCB meeting, September 2007).
Nellie was ‘fully aware of the relationship breakdown across the two organizations [mental healthcare provider and hospital acute care]’ (Nellie, Chair, CLSCB), following which she encouraged the CEOs of the hospital acute care and mental healthcare provider to address the breakdown of trust between the two medical directors: I recognized it was difficult for me to reach into these particularly powerful players that shaped how our two most important organizations interacted. I needed to work through their chief executives, they needed to develop the medical relationships across their organizations, rather than both come through me . . . they agreed, I left it to them. (Nellie, Chair, CLSCB)
The CEOs took their respective medical directors aside to ‘sort out the medical politics, which to be fair they did, and they put their differences aside without poisoning things among the wider group of clinicians in each of our organizations’ (Manny, CEO, mental healthcare provider).
At the same time, Nellie (Chair, CLSCB) also ‘wanted to focus all organizations on tightening up the way we worked together through our protocols and wider communication’ (Nellie, Chair, CLSCB), and set up a sub-committee to the CLSCB, which was given the remit of examining coordination among organizations in the network, specifically, to develop a better protocol that framed how a client with an eating disorder was cross-referred from one agency to another, and how the information about him or her was shared across agencies. We were particularly concerned about the health organizations, ensuring primary care, the GPs, the mental healthcare provider and hospital related better to each other in dealing with the client. (Louise, manager, local government)
Within the sub-committee, medical directors worked with their colleagues in their respective organizations to develop an approach to repairing trust following the crisis that focused on clarifying how they referred to each other: There is now a clear protocol that sets out how we respond. If a patient comes in through accident and emergency, we deal immediately with the problem, say intravenously feeding them, checking their physical condition, stabilizing them. If we suspect anorexia, we inform the GP, the mental healthcare provider, and the safeguarding board of their admission. (Medina, paediatrician, hospital acute care)
By Spring 2008, one year after Elsa’s death, the organizations in the network had seemingly addressed the failings that led to Elsa’s death by restoring trust in the network’s regulatory provision through reworked protocols that governed the organizations’ behaviours and by restabilizing the dyadic relations between constituent organizations and the lead organization so they could continue to work towards their mandated goal. This might have been the end of the story for this network, since they had ostensibly addressed the crisis by repairing trust in the regulatory provisions of the network.
Episode 3 (Summer 2008–Winter 2009)
As we continued our fieldwork, we observed a change in the ways that the organizations interacted in Summer 2008. It became evident once trust in the regulatory provisions of the network had been restored, that the lead organization sought further assurances against another crisis. In episode 3 the lead organization facilitated interaction between the constituent organizations in the CLSCB, recognizing this was important for the effective functioning of the CLSCB in the future.
Despite ‘feeling threatened’ during the initial period when tensions were running high between the organizations in the network, Nellie reflected that there remained a need for further change: from a hierarchical relationship between us [the lead organization] and them [constituent organizations of the CLSCB] to a more, what I would call collective relationship. Privately I took it hard to start with as my individual failing, but then saw it as a more collective thing. I had to bring others to the same conclusion that we had all failed and that we had to work together. This was not just a matter of tightening up our protocols, but of attending to the ‘softer’ [Nellie signalled quotation marks around her use of this term], less tangible aspects of our relationships. (Nellie, Chair, CLSCB)
With the aim of enhancing interorganizational relationships, Nellie called a meeting, which she described as an organizational development event where she ‘rallied the troops’ (Nellie, Chair, CLSCB, January 2009, field note from conversation with Nellie, p. 5). Nellie’s opening speech was ‘Churchillian in its resonance’. She concluded that ‘we are all in this together’ (January 2009, reflective note of organizational development event, p. 3). The ‘rousing war cry’ (January 2009, reflective note of organizational development event, p. 3) channelled the CLSCB members towards their collective goal. As Nellie put it in the meeting: ‘united we stand, divided we fall’ (January 2009, reflective note of organizational development event, p. 3). This pivotal speech articulated common failures, but focused principally on the common goal among members of the network: If we go it alone, we just pass the problem around. The aim of the meeting today is to move this approach forward. I want you to learn from each other, and develop a shared vision for safeguarding the vulnerable children of this city. Together we can stop these things happening, but only together. (Nellie, January 2009, field note, organization development event, pp. 1–2)
Nellie invoked feelings of responsibility for Elsa’s death, to channel others towards the same end, focusing upon the vulnerable nature of the clients, such as Elsa, whom the CLSCB served: I tried to deflect personalization of blame, and move debate away from our own failings, to imagine how safeguarding boards might work more effectively to deliver care to vulnerable young people. (Nellie, Chair, CLSCB)
This had the effect of reorienting the network members’ relationships to the network’s priorities: ‘It’s a simple thing to focus upon. We do care. She [Nellie] just pushed us on it. We really do care about girls such as [Elsa]’ (Sam, medical director, mental healthcare provider).
Following the organizational development event, activities among the network members took several different forms, guided by Nellie. She formed a working group that fed into the sub-committee previously instituted in episode 3, that was to ‘explicitly analyse the relationships across organizations in the CLSCB and make suggestions for how organizations could work more effectively together, rather than as just directed from above’ (Nellie, Chair, CLSCB). The tone had shifted from one of blame within the network to one of shared responsibility, recognizing their collective goal and acknowledging their collective failings, following which ‘they were expected to work more effectively together, not only reliant on protocols to do so’ (Nellie, Chair, CLSCB). Nellie continued to lead the network-level goals: ‘we need to ensure what we want fits with managerial priorities, gets into the right arenas to secure resource. I’m speaking to them all individually’ (Nellie, Chair, CLSCB). During this period, we saw the organizations in the network begin to behave in ways that indicated interaction-based trust had begun to develop not just with the lead organization but between other organizations in the network: We began to feel we could do something. Nellie was encouraging us to do something, giving us permission to move things forward. We needed to work more collaboratively to do this. (Medina, paediatrician, hospital acute care)
The working group, encouraged by Nellie to think about ‘how to structure the delivery of eating disorders care across the myriad of organizations involved’ (Martin, CAMHS psychologist, mental healthcare provider), proposed the development of a specialist eating disorders service to be designed and delivered collaboratively by the network members. ‘This represented a practical solution to engender the type of relationships across organizations delivering the service to prevent future failure’ (Nellie, Chair, CLSCB). As the organizations worked together in establishing the eating disorders unit they began to acknowledge more frankly in open fora the collective failings Nellie had identified at the organizational development event. Clinicians in acute hospital recognized they had to work beyond their clinical jurisdiction: ‘We failed because we are too busy holding on to our expertise, “it’s someone else’s responsibility”. How did we let this happen to a vulnerable girl?’ (Medina, paediatrician, hospital acute care). The development of the specialist eating disorders unit also required organizations to commit to developing relationships beyond those mandated by the governance structure in order to work effectively: ‘we sought to build a better relationship with our colleagues in [the mental healthcare care provider], which until this point had been too distant, structured through protocols not through people’ (Gina, paediatrics nurse, hospital acute care). This outlook was reciprocated: ‘they [clinicians from the acute health provider] come across here regularly, which allows us to get to know each other better, to understand each other more. I know what happens their end, they know what happens our end, rather than before, distant from each other’ (Carol, nurse, mental healthcare provider).
As collaboration among network members on the development of a specialist eating disorders service began, the organizations became more engaged collectively with the shared goal of the network: We started developing our service in terms of our own CAMHS [Children and Adolescent Mental Healthcare Service] configuration and then realized we needed input from other organizations. (Sam, medical director, mental healthcare provider)
While it was clear that the CLSCB remained the lead organization accountable for the broader issue of child protection, a service delivery network developed within which constituent organizations began to engage directly. The mental healthcare provider and acute hospital, who had previously blamed each other over the crisis for failing to discharge their respective responsibilities, had developed a close working relationship: Protocols are necessary, they really are, but they are not enough. You have to work closely together and build the relationship on the ground. We did this to develop the eating disorders service . . . we could rely on them, they could rely on us to work with them. (Medina, paediatrician, hospital acute care)
However, at this point, the service remained incipient, described as ‘fragile, just a response to find a way forward, but we needed to sustain our relationships’ (Manny, CEO, mental healthcare provider). We highlight how the ongoing efforts to develop the eating disorders unit sustained the relationships across the network and impacted the network form in episode 4.
Episode 4 (Spring 2015–Spring 2016)
Following the publication of the coroner’s inquest into Elsa’s death, we returned to the field site again between Spring 2015 and Spring 2016 to examine how the eating disorders service had developed. Our motivation was to examine not just the relationship between the lead organization and others, but also how relationships between organizations within the network had sustained and developed. We observed a change in the network governance as trust relations had continued to develop between the constituent network members.
Despite the optimism surrounding the development of a new eating disorders service in 2009 we suspected that there would be challenges to sustaining the momentum of activity. We reflected on how the trust repair efforts that took place in episodes 2 and 3 had impacted the relationships between the organizations in the network in the longer term. When we returned, institution-based trust had been repaired, even enhanced, through not just protocols for how we co-ordinate our actions, but a set of criteria that we have developed to satisfy the CLSCB Chair about our performance on the ground and that are likely to mitigate against future failure. They make sense in relation to how we deliver services across organizations. At the same time, they allow the chair clear sight of our activities for managerial purposes. (Martin, CAMHS psychologist, mental healthcare provider)
However, new interaction-based trust was also now evident. We observed how trust between network members was manifest in three types of behaviour within the network that had not been observed prior to the crisis.
First, we observed that although the organizational membership of the network remained the same, and the interorganizational network remained goal-orientated, the relationships among the organizations had shifted away from the reliance solely on dyadic relations with the lead organization observed in episode 1. Nick (medical director, acute hospital) commented that the mental healthcare provider ‘holds the ring for us into which we all work, the area of eating disorders’. This comment from the medical director of the hospital acute care was of particular note. The two medical directors who previously levelled blame at each other’s organizations for the failures in the immediate aftermath of crisis were now working closely together towards the common goal of the network. This was emblematic of the fact that the dyadic interaction-based trust relations we observed developing in episode 3 had sustained. This was reflected in other dyadic relations. Mona (health visitor, primary care) reflected, ‘I feel I know what they [mental healthcare provider] need from me. I can get on with actually doing my job and have an understanding of how they do theirs.’
Second, the organizations continued to engage directly with one another in the ongoing delivery of the eating disorders unit and did not just rely on the regulatory governance of the network in delivering the service: ‘we were no longer a dangerous service, we became tight knit, holding each other responsible for what we delivered as a team’ (Linda, psychiatrist, CAMHS, clinical lead). These relationships went beyond the jurisdictional accountabilities mandated by the CLSCB. For instance, David (lead paediatrician, hospital acute care) liaised closely with the service delivery team located in the mental healthcare provider, reflecting on the benefits of the trust that now existed between the two members of the network: Young people [with eating disorders] are probably more likely to turn up here [hospital acute care] than there [mental healthcare provider], but I need to cross refer to them, previously difficult, but now facilitated by a specialist service to whom I can directly relate. I am much more prepared to address underlying issues, rather than patch them up and send them on. It is less a matter of coordination and more a matter of having a relationship with the mental healthcare provider.
Third, through their collaboration on the development of the eating disorders unit the organizations had become engaged with the governance of the network rather than simply adhering to their individual jurisdictional responsibilities within the CLSCB. One member observed, ‘I am much more proactively looking for young people with eating disorders in my clinic so that we don’t experience missed opportunities [for care], that’s service failure, and we are not a failing network’ (Jim, GP). Even Nick (medical director, hospital acute care), who previously blamed others for failure, contributed towards network governance: I used to attend network meetings sporadically, it was a sideshow, I would delegate others to represent the organization. Now I attend and contribute fully. We, me, are part of the network. It’s not a sideshow anymore.
Therefore, rather than viewing the network’s regulations as the sole basis for trusting relations, organizations were also relationally engaged with their collaborators and the priorities of the network. Episode 4 shows that the nascent dyadic trusting relations between constituent organizations observed in episode 3 had sustained. The consequence of this is that trusting relations amongt the network were now more distributed. Institution-based and interaction-based trusting relations now exist in the network. This is in contrast to trusting relations in episode 1 where the lead-organization governance form relies principally on institution-based trust.
Discussion
Figure 2 presents a model that sets out changes in the network and associated trust repair strategies. We first discuss the changes to network-level trust and governance form. Second, we distinguish the two periods of trust repair (catharsis and catalysis) and clarify how they bring change to network-level trust and governance form. Third, we reflect on whether the new network form is ‘more durable and stable’ (Kramer & Lewicki, 2010, p. 268), and whether stability is always beneficial (Majchrzak et al., 2015). We conclude by clarifying some of the boundary conditions, limitations and avenues for future research.
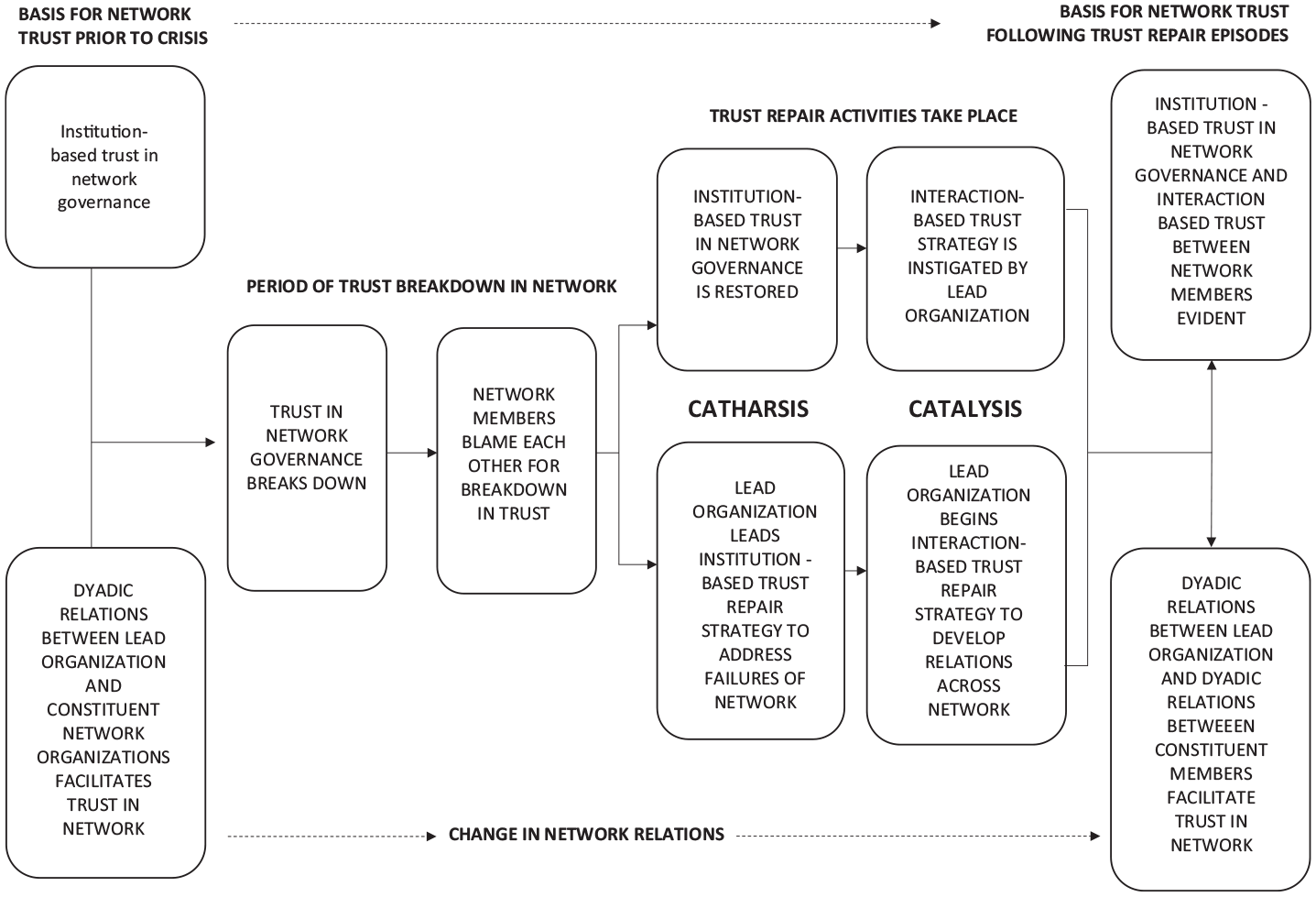
Model of interorganizational trust repair following a crisis.
Changes to network-level trust and governance form
Prior to the breakdown of trust (episode 1), organizations placed trust in the network’s governance mechanisms. This was facilitated by a lead organization that ensured each organization was clear what their responsibilities were. At this point institution-based trust provided the basis for network trust (Bachmann, 2001). Thus, centrally managed governance with organizations placing institution-based trust in the network structures is shown to be an effective way to facilitate interorganizational collaboration in routine circumstances.
On our return to the field in 2015 (episode 4), the network remained formally lead-organization governed; organizations continued to rely on institution-based trust to ensure effective collaboration across the network. However, dyadic trust relations between network members were now established. The new dyadic relationships between network members had come to form a dense web of interaction-based trust ties between organizations that gave the network characteristics of a participant-governed network, while retaining characteristics of lead-organization governance (Provan & Kenis, 2008). The following section examines how the two periods of trust repair brought about this new network governance form.
Network-level trust repair
Episodes 2 and 3 show two phases of trust repair underpinned by different trust repair mechanisms that bring change to network-level trust. The first phase of trust repair is a period of catharsis where trusting relations are restored to their previous state (episode 2). The second phase of trust repair is a period of catalysis which brings change to the trusting relations (episode 3).
Trust repair as catharsis
Each organization believed it had discharged its jurisdictional duties and complied with the mandated rules of the network with respect to the failures surrounding Elsa’s death. Organization-level trust repair models indicate that acknowledging the incident and taking active steps to understand the reasons why the incident took place would be the effective course of action to repair trust between the stakeholders (Gillespie & Dietz, 2009; Pfarrer et al., 2008). However, the lead organization does not pursue this in the first instance. Instead, a period of catharsis unfolds, in which organizations blame one another.
Given the lead organization’s central role in the governance of the network it seems puzzling that they are not scapegoated for the crisis (Gangloff, Connelly, & Shook, 2016). This is because the lead organization has dyadic relationships with each organization, yet dyadic relations between the other network organizations are not present at this stage. The network structure at this point is such that organizations do not have all the information regarding the failings (Pfarrer et al., 2008). Therefore, in line with Kim and colleagues (2009), we see that organizations assign blame where they have limited information about other organizations to ensure they are not the focus of blame. Contrary to Gillespie and Dietz (2009) the lead organization chooses not to publicly express regret or assign blame at this point, instead allowing network organizations to establish their own accounts of events (Elsbach, 2003).
Current theory would suggest that expedient examination of the institutional arrangements that govern the network would be prudent. However, efforts to make changes to the regulatory structures are not immediate. The lead organization instigates this after the period of organization-level blame has taken place. The lead organization’s timing again provides insight into how to navigate trust repair in interorganizational networks. The constituent organizations have reflected upon who is to blame for the failure and assigned blame to other organizations in the network. However, assigning blame to other organizations has not restored trust in the network. The lead organization is then able offer an alternative account, which focuses on the governance structure of the network. Since the focus thus far has been on assigning blame to other organizations, the lead organization is able to facilitate the restoration of trust in the network by refocusing repair efforts on the governance mechanisms (Gillespie & Dietz, 2009). This moves the organizations beyond blaming one another and towards repair of the institution-based trust that organizations placed in the network governance.
The organizations re-examine protocols and address perceived inadequacies of the governance mechanisms (Kim et al., 2009). This restores the social equilibrium and organizations are able to return to their previous arrangement where institution-based trust is placed in the governance of the network. Dyadic relations between the lead organization and each of the network members resume to ensure that the new rules are adhered to. Trust has therefore been restored to its previous state (Bachmann et al., 2015). Adjusting regulations can effectively restore interorganizational trust.
Trust repair as catalysis
The second phase of trust repair is initiated by the lead organization and catalyses change in the behaviour of the other organizations in the network. The changes to behaviour bring about new dyadic trusting relations between network members. As the organizations’ behaviour and relationships change, their disposition towards network objectives is shown to change.
The trust repair strategy pursued by the lead organization starts with a non-apology for the failures. The non-apology is successful in persuading the organizations that the future will be better. Contrary to suggestions by Gillespie, Dietz and Lockey (2014), the lead organization does not acknowledge culpability for the failings. Instead, the non-apology emphasizes the collective responsibility of the organizations in the network to avoid another failure. In doing so the non-apology does not dismiss the past; rather, there is a call for the organizations to respond to the past by collectively addressing the failings.
Despite not acknowledging culpability for the failings, the lead organization’s non-apology is perceived to be a sincere effort to repair trust (Schweitzer et al., 2006; Tomlinson et al., 2004). This is for two reasons. First, any apology appears unnecessary at this stage; the network has recovered from the crisis and institutional trust has been restored in the governance mechanisms of the network. Therefore, choosing to be vulnerable at this point involves exposing the organization to unnecessary risk; the lead organization could be subject to retrospective blame which could lead to ‘a changing of the guard’ (Gillespie et al., 2014, p. 371). Second, the non-apology shows that the lead organization recognizes that simply restoring institution-based trust has left the network susceptible to repeating previous mistakes. Thus, the non-apology signals commitment to further change (Lewicki et al., 2016).
The non-apology catalyses change first by changing the attitudes of the organizations towards their collaborating partners (Lewicki et al., 1998; Mayer et al., 1995). Clearly articulating the organizations’ shared values by reminding them of their collective responsibility leads to the organizations changing their disposition such that they too make themselves vulnerable. In this sense, the lead organization has taken the first ‘leap of faith’ (Möllering, 2006, p. 105) and shown a willingness to be vulnerable. The organizations also become more expectant of positive behaviour because the apology signals a fresh start and renews hope about the future (Lewicki et al., 1998).
Furthermore, confirming arguments by Gillespie and Dietz (2009) and Tomlinson and Mayer (2009), the non-apology is effective because it is supported by practical action to address the failures, thus demonstrating that the apology is not ‘cheap talk’ (Bottom et al., 2002, p. 498). The practical solution becomes a collaborative endeavour and performance measures that align with the common values of the organizations are devised. The practical solution is resourced such that it adequately operationalizes the vision for change. This confirms the need for commitment of time and resources for effective trust repair (Gillespie & Dietz, 2009).
The non-apology serves as a catalyst for independent dyadic relationships to develop between the network members as they work together on the shared solution. Working together in this way increases the density of trust ties in the network. The interaction-based trust is more than simply a collection of trusting dyadic relations; these relations are aligned with the collective goals of the network (Provan & Kenis, 2008).
Is network-level trust more durable and stable?
After the two periods of trust repair there are new interaction-based trust ties among the organizations in the network. The new interaction-based trust informs, but does not supplant, the institution-based trust in the governance of the network. Interaction-based trust ties are therefore an addition to, rather than a replacement for, the institution-based trust placed in the network observed before the crisis. Therefore, following the two periods of trust repair, network trust appears more ‘durable and stable’ (Kramer & Lewicki, 2010, p. 268).
Further, the new dyadic trusting relations bring about change to the governance form of the network. The new governance form no longer conforms to either of the pure forms described by Provan and Kenis (2008), which we outlined earlier, showing that in practice networks may exist with a hybrid form of governance (Keast, 2016). The new governance form benefits from a shared sense of responsibility among organizations for network-level outcomes (typical of participant-governed networks) while retaining the benefits of clearly articulated protocols and centrally mandated goals (typical of lead-organization governance). Thus, the new trust dynamics brought about by the two periods of trust repair have made the network itself more stable.
Returning to Majchrzak and colleagues’ (2015) question as to whether stability in a network is beneficial to interorganizational collaboration, our findings indicate that where organizations are required to work towards a specific goal, stability is beneficial in line with Provan and Milward (1995). A governance form that reflects institution-based and interaction-based trust is thus one way to provide this stability.
Provan and Kenis (2008) outline that the network governance form should reflect its objectives. The network dynamics we describe suggest that stability is not always beneficial if, as Majchrzak and colleagues (2015) indicate, stability may stymie innovation, or, as Provan and Kenis (2008) hypothesize, make the network less flexible. This aligns with other trust research that suggests that too much trust may expose organizations to the problem of possible ‘trust lock-ins’ making them susceptible to path dependencies (Möllering & Sydow, 2019, p. 142). Therefore, stable trust relations and the hybrid governance form we have outlined may have unintended consequences for network-level trust beyond the scope of this paper.
Conclusion
Our study addresses the research questions, How is trust repaired in an interorganizational network following crisis, and with what effect? We provide an analysis of network-level trust repair to advance theory on trust repair. The two phases of trust repair revealed in our study show trust repair as both catharsis and catalysis. Together they contribute to the stability of network trust and change its governance form. As Dostoevsky alludes, continuing trust repair efforts beyond the crisis and ‘taking a new step’ can change the constitution of the interorganizational network making network trust more durable and stable. Whether this is beneficial is context bound; the governance form should reflect its objectives.
The model extends current organization-level trust repair theory (Gillespie & Dietz, 2009; Pfarrer et al., 2008) to provide a network perspective of the dynamics of interorganizational trust repair. Building on Bachmann et al. (2015) we show that both institution- and interaction-based trust repair efforts play a role in restoring network-level trust. We show that repair efforts bring change to the type of trust that is manifest at the network level. This changes the network governance form (Provan & Kenis, 2008). Our conclusion is that, as a result of the two periods of trust repair, trust relations and the network itself become more stable (Majchrzak et al., 2015).
In reflecting upon the limitations of our study and prospects for future research, we recognize that our analysis is developed using findings from a lead-organization governed network. Our analysis is generalizable to interorganizational networks that must continue to work together, where there is a lead organization present and where organizations share similar objectives. Such networks are increasingly used to address issues critical to society such as social care and disaster management, or managing vital public sector services (Graddy & Chen, 2006; Keast, Mandell, Brown & Woolcock, 2004; Vasavada, 2013).
The role of the lead organization in the network requires further clarification. Research may provide theoretical insight by addressing more general questions regarding the interplay between levels in the trust repair process (Bachmann et al., 2015). Specifically, others may interrogate whether the network governance form meant that the lead organization was in this particular case uniquely placed to traverse the two phases of trust repair without becoming the object of blame. This poses the question, could another organization in the network have catalysed change by making themselves vulnerable in the ways we outline here? Answering this question would require further consideration of the organization-level perception of risk, and what might motivate an organization to believe that the risk is worth taking if they must continue to work together. This raises a further question, could – or rather, in what circumstances would – an organization in a participant-led network take on a similar role to the lead organization?
Reflecting more broadly on participant-led governance provokes questions about the fluidity of the order of the trust repair phases in the model. If, as Provan and Kenis (2008) suggest, there are a large number of dyadic, interaction-based trust ties in a participant-governed network, would the order of the trust repair phases be different if such a network faced a similar trust crisis? Put another way, does catharsis necessarily come before catalysis in a network that does not rely principally on institution-based trust?
In theory the sequencing of the two phases (first catharsis and then catalysis) could reverse, for example, where informal networks are faced with a crisis and come to realize the need for clearer governance arrangements. Likewise, it may be that in other contexts it is beneficial to have just a brief period of catharsis, for instance, in highly regulated sectors where innovation is required, such as the financial services sector. On the other hand, certain cultural factors may require a longer period of catharsis. For example, Chinese business networks have been shown to emphasize the importance of regular interactions and relationships (Ferrin & Gillespie, 2010).
While our case confirms that network-level trust is context bound (Bachmann et al., 2015), it also highlights the need to consider trust repair as an opportunity for constructive change. As Dostoevsky suggests, such a perspective may elicit fear, but embracing times of crisis as an opportunity for constructive change can help to ensure the network remains effective.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This research is supported by the National Institute for Health Research (NIHR) Applied Research Centre (ARC) West Midlands. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.