
Abstract
Despite the increasing deployment of formalized boundary spanning roles and practices, the mechanisms and dynamics of their legitimation remain under-explored. Using the Bourdieusian lens, we theorize legitimation of boundary spanning as accumulation, mobilization and conversion of several forms of capital unfolding in a configuration of intersecting fields. Drawing on a qualitative longitudinal case study of a collaborative partnership between a university and healthcare organizations, we describe changes in the structure, sources and mutual convertibility of capital assets over time. We also analyse the implications of this evolution for the relationships between the intersecting fields and the social trajectory of boundary spanners. We argue that legitimation of boundary spanning roles and practices is a highly transformative, collective and political process that increases the capital endowments and authority of individual boundary spanning agents but may lead to the erosion of the very same roles and practices that were being legitimized.
Keywords
Introduction
Analysis of boundary spanning phenomena is of particular interest to organizational theory as contemporary work is being transformed by postmodern patterns of organizing, including hybrid, network-based and temporary arrangements where collaboration, governance and partnership unfold across multiple boundaries (Bucher, Chreim, Langley, & Reay, 2016; Williams, 2012). Boundary spanning, which occurs when actors deliberately or inadvertently relate entities separated by a boundary (Levina & Vaast, 2014), is becoming an important part of mainstream jobs in the private (Levina & Vaast, 2005), public (Williams, 2012) and voluntary sectors (Fleming & Waguespack, 2007). The wider policy context characterized by an increased emphasis on service integration and dismantling of traditional hierarchies makes boundary spanning roles and activities an integral feature of mandated solutions to tackling ‘wicked problems’ that go beyond the remit of one organization (Currie & White, 2012; Evans & Scarbrough, 2014; Lander, 2016).
For their potential to be realized, novel boundary spanning roles and activities have to be seen as legitimate (Levina & Vaast, 2005; Reay, Golden-Biddle, & Germann, 2006), i.e. desirable, proper or appropriate within broader, socially constructed systems of values and beliefs espoused by the relevant social agents (Suchman, 1995). While legitimacy is seen as an important attribute of successful boundary spanning, mechanisms and consequences of its acquisition remain under-explored. Extant literature on legitimacy does not adequately address these issues, partly because legitimation of boundary spanning presents a unique case due to its intermediary, in-between position between multiple social fields (Kislov, Wilson, & Boaden, 2016). In addition, legitimation often tends to be theorized as a set of predominantly discursive strategies deployed by agents aiming to have their roles and practices accepted (Landau, Drori, & Terjesen, 2014; Sanders & Harrison, 2008; Suddaby & Greenwood, 2005) while their actual actions and the implications of the latter for the object of legitimation and for the relationships between multiple legitimacy-granting audiences have received less attention (Kislov, Hodgson, & Boaden, 2016).
We aim to fill this lacuna by deploying Bourdieu’s (1986) theoretical framework which conceptualizes legitimation as acquisition and redistribution of various forms of capital seen as valuable in a given social field. By linking the legitimation of boundary spanning to a system of mutually constitutive relationships between individual capital endowments of boundary spanning agents, their emerging collective dispositions and the broader configuration of intersecting fields in which they are embedded, this approach enables a multi-level analysis (Battilana, 2006; Özbilgin & Tatli, 2005). A Bourdieusian framework is also particularly well suited for unmasking hidden power relationships that are inherent in the process of legitimation (Golsorkhi, Leca, Lounsbury, & Ramirez, 2009; Kamoche, Kannan, & Siebers, 2014; McDonough & Polzer, 2012), whereby legitimacy is granted by the guardians of the very same cardinal rules of the field that boundary spanners aim to disrupt (De Clercq & Voronov, 2009a).
Our empirical inquiry is guided by the following two research questions. How does the deployment of different forms of capital in the process of legitimizing boundary spanning roles and practices change over time? What implications do these changes have for the relationships between the intersecting fields and the social trajectory of boundary spanners? We address these questions by a qualitative longitudinal case study of a large-scale UK-based collaborative partnership deploying nominated boundary spanners to facilitate the uptake of applied health research in clinical practice, thus ‘bridging the gap’ between academic researchers and clinical practitioners (Kislov et al., 2016b). In so doing, we highlight the potential of a Bourdieusian framework, usually applied to the analysis of single fields, to illuminate the processes unfolding in complex multi-field configurations. In our case, such configuration is comprised of an emergent joint field of collaborative practice (Levina & Vaast, 2005) and two established fields, namely the field of applied health research and the field of general medical practice (McDonald, 2009).
We start by outlining the Bourdieusian perspective on boundary spanning at the interface of multiple fields and discussing the challenges faced by boundary spanners in the process of legitimation. This leads to the explication of research gaps and questions, after which we describe the research setting and the procedures for data collection and analysis. This is followed by three empirical sections: the first of them describing the evolution of economic, cultural and social capital in the process of legitimation; the second, analysing the implications of these changes for the inter-field relationships; and the third, reflecting on how individual and collective social trajectories of boundary spanners are affected. These themes are then theoretically developed in the Discussion, which argues that the legitimation of boundary spanning improves the relative position of boundary spanning agents but, paradoxically, results in the erosion of the very same roles and practices that were being legitimized. The paper concludes with a summary of the contribution, limitations and implications of the study.
Bourdieusian Perspective on Boundary Spanning between the Intersecting Fields
According to Bourdieu (1991, 1993), society is divided into relatively autonomous social fields. Each field (often referred to as a ‘game’) possesses its own internal logic, a set of implicit rules determining the relative value of specific forms of resources (capital) pursued by the agents competing for access to the profits that are at stake (Bourdieu & Wacquant, 1992). In this context, boundary spanners are individual or collective agents that relate practices in one field to practices in another by negotiating the meaning and terms of the relationship between them (Levina & Vaast, 2005). Through membership in several intersecting fields, boundary spanners enable translation, coordination and alignment between different perspectives and facilitate transactions between previously separated practices (Kislov, 2014; Kislov et al., 2016a). They can be engaged both in boundary crossing, which enables and coordinates the movement of people, objects or ideas between the fields, and boundary redefinition, implying the blurring or reconfiguration of inter-field boundaries (Bourdieu, 2005; Evans & Scarbrough, 2014).
Existence of boundary spanning is enabled by the fact that, although the fields are not reducible to one another and have historically acquired certain autonomy, they are often ‘interlocked’ through a number of means (Bourdieu, 1991, p. 25). First, agents live across multiple fields, and boundary spanning exemplifies the broader phenomenon of ‘transverse movements’ from one field to another (Bourdieu [1984] 2010, p. 126). Second, fields are composite and can be divided into subfields (Bourdieu, 1991, 1996, 2005), such as the field of general medical practice within the broader healthcare field or the field of applied research within the broader scientific field. Third, fields are connected through the ‘field of power’, a meta-field in which the agents occupying dominant positions in their respective fields compete (or, occasionally, build alliances) with each other aiming to preserve or transform the balance of power between the fields (Bourdieu, 2000, p. 103; Bourdieu & Wacquant, 1992, pp. 8, 76).
The state wields power over the exchange rate between various forms of capital that circulate in different fields (Bourdieu & Wacquant, 1992). Establishing designated boundary spanning roles should therefore be analysed within the broader context of government-led initiatives aiming to reconfigure the relationships between the fields (and subfields) characterized by different degrees of autonomy from the ‘field of power’. These initiatives, exemplified by interprofessional and inter-organizational collaborations, aim to increase effectiveness and efficiency by promoting integration and cooperation between different sectors, organizations and professions (Bucher et al., 2016; Evans & Scarbrough, 2014; Kislov et al., 2016a). In the UK context, this is accompanied by the state’s attempts to challenge the autonomy of the healthcare field by introducing alternative managerialist logics of quasi-market and target-driven performance management (Battilana, 2011; Waring & Currie, 2009).
Both external boundaries of the field, defined by Bourdieu (1996, p. 226) as ‘dynamic limits, which extend as far as the power of its effects’, and its internal boundaries (i.e. classifications, hierarchies and divisions) reflect the established order and therefore can become the object of inter- and intra-field power struggles (also see Bourdieu, 2005). As such, boundary spanning implies challenging the established order, and boundary spanners need legitimate authority enabling them to produce effects on the field(s) they interact with (Kislov et al., 2016a; Levina & Vaast, 2005). In Bourdieu’s (1986) work, gaining legitimacy is linked to the processes of accumulation and mobilization of several forms of capital (economic, cultural and social) convertible into one another at different rates of exchange (Table 1).
Forms of capital.
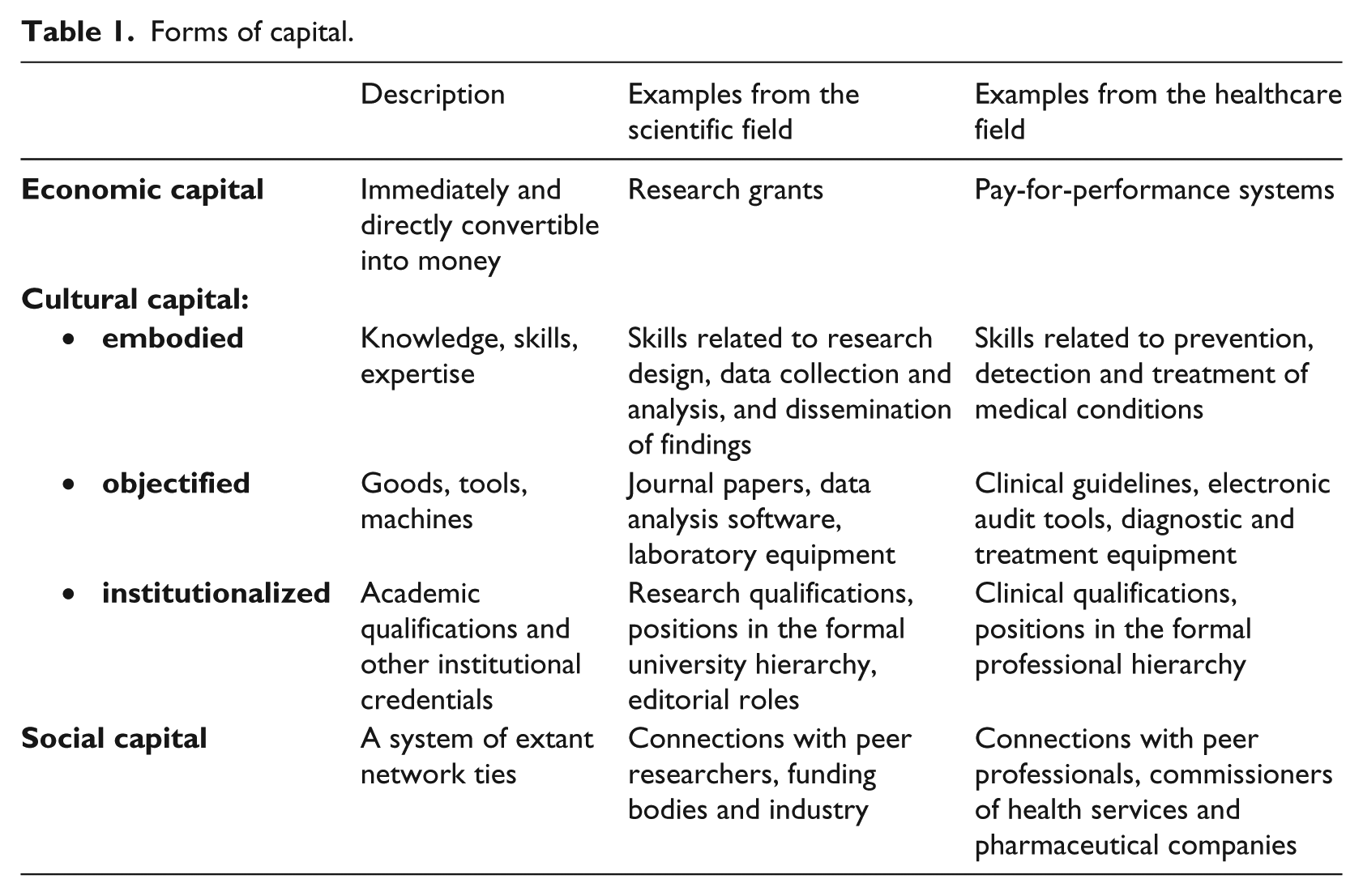
Capital plays a dual role in boundary spanning. On the one hand, any form of capital may act as a weapon in the boundary spanners’ struggle for legitimacy and authority, functioning as symbolic capital whose arbitrariness as a source of power is not recognized as a form of domination but misrecognized as a legitimate competence (Bourdieu, 1977, 1986, 1994, 2000). On the other hand, boundary spanning aims to transform the distribution and ‘exchange rate’ of the agents’ capital assets (Bourdieu, [1984] 2010). For instance, collaborative partnerships between universities and healthcare organizations aspire to modify the ‘rules of the game’ by increasing the relative value of scientific capital in the healthcare field and the relative value of clinical capital in the scientific field (Lander, 2016). Furthermore, they are expected to institutionalize these novel patterns of capital valorization (and related cross-boundary practices), thus opening up a ‘new game’ which would be markedly different from pre-existing established fields and practices with their specific sets of (old) rules (also see Kislov, 2014). Such changes are likely to have profound effects on the agents’ power, position, social trajectory and strategic orientation in the field(s) involved (Bourdieu, 1991; Bourdieu & Wacquant, 1992). Legitimation of boundary spanning is therefore highly contestable and laden with tensions. The latter are explored in the next section.
Challenges and Scenarios of Legitimation in Boundary Spanning
The first set of tensions is related to the highly context-dependent nature of capital and its distribution. Agreements about what capital assets are valuable are rooted in field-specific habitus, i.e. durable, collectively shared schemes of perception, thought and action shaped by the field and accounting for the ‘sense of one’s place’ (Bourdieu, 1994, p. 128) and ‘feel for the game’ (Bourdieu & Wacquant, 1992, p. 128). 1 In order to legitimately participate in the field, agents therefore have to possess a definite configuration of capital (Bourdieu, 1986) (see examples in Table 1). However, habitus of those boundary spanning agents who are external to the field they aim to influence will reflect their previous social trajectories rather than the ‘rules of the game’ in the given field. Extreme consequences of this mismatch may potentially result in the failure to actually span the boundaries (Kislov et al., 2016b) or conflict between the newcomers and dominant agents (Bourdieu, 1983, 1993; Bourdieu & Wacquant, 1992).
Another group of tensions stems from the peripheral and/or intermediary position of boundary spanners. Although a formal boundary spanning job title and position may confer on its holder a certain amount of structural legitimacy (Lockett, Currie, Waring, Finn, & Martin, 2012; Suchman, 1995), i.e. symbolic capital inherent in the position itself (Bourdieu, 1994), on its own this is not enough for establishing the legitimacy of newly created formal, or nominated, boundary spanning posts (Levina & Vaast, 2005). In uniprofessional, non-boundary-spanning contexts, legitimate peripheral participation has been described as a mechanism through which peripheral actors gradually learn the ‘rules of the game’ and move towards dominant positions in their fields (Lave & Wenger, 1991). ‘Ambiguous potentialities of legitimate peripherality’ (Lave & Wenger, 1991, p. 36) may well apply to boundary spanners. On the one hand, they can use the ‘in-between’ nature of their position to carve their own role at the interface between different fields (Chew, Armstrong, & Martin, 2013; Omidvar & Kislov, 2014). On the other hand, peripheral agents can be denied access to the field due to their lack of power, visibility and recognition (Lockett et al., 2012; Yanow, 2004).
Finally, legitimation of boundary spanning is likely to depend on the approval of multiple professional and organizational groups, many of which will be superordinate to boundary spanners (Johnson, 2004). These groups can be internal (e.g. the organization’s own managers) or external (e.g. regulators, partners and other external stakeholders) to the organization (or field) from which boundary spanners originate (Bourdieu, 1991; Drori & Honig, 2013). Although the acceptance of legitimacy has an appearance of consensus (Johnson, Dowd, & Ridgeway, 2006), it often involves several co-existing legitimation narratives (Landau et al., 2014; Sanders & Harrison, 2008) reflecting inter-group competition over capital within the field and potentially implicating peripheral agents in power struggles between the groups (Bourdieu, 1991, 2000). Healthcare provides a particularly interesting example in this respect due to the presence of a sharply demarcated internal stratification which manifests in rigid professional hierarchies reflecting unequal distribution of capital between its constituent professions and occupations (Currie & White, 2012; Waring & Currie, 2009).
Empirical analysis of boundary spanners’ legitimacy presented in this paper builds on two interrelated strands of Bourdieu-informed theorizing. The first strand focuses on inter-organizational collaboration and emphasizes the dynamic nature of boundaries which enables the development of an emergent joint field with a unique distribution of capital and the development of novel cross-boundary practices (Levina & Vaast, 2005, 2014). Under the conditions of novelty and ambiguity, newcomers and peripheral actors, who are often marginalized in pre-existing established fields, may use the liminal conditions of the novel joint field to transform power structures (Levina & Orlikowski, 2009; Reay et al., 2006). Becoming a legitimate boundary spanner implies participation, at least peripheral, in the pre-existing fields, possession of symbolic capital enabling the agent to negotiate the power relationships and an inclination to span the boundaries (Levina & Vaast, 2005). How this symbolic capital is acquired in practice amid inter- and intra-field tensions, however, remains under-explored.
The second strand focuses on the entry of newcomers into an established field and develops Bourdieu’s (1983, 1993, 1996) conceptualization of a field as a site of struggle between the newcomers, who are least endowed with field-specific capital but often want to impose new modes of thought, and dominant agents seeking to protect the continuity and reproduction of existing power relationships. For instance, De Clercq and Voronov (2009a, 2009b) argue that aspiring entrepreneurs gain legitimacy by meeting the field incumbents’ expectations about conformity and innovation and, by enacting field-specific habitus, become complicit in the perpetuation of the current power arrangements in the field. In other words, newcomers’ ability to amass capital is not entirely under their control and they must enact field-specific habitus to develop legitimacy. It is, however, unclear to what extent these patterns are applicable to intermediary roles and practices located at the interface of multiple fields.
Research Gaps and Questions
In Bourdieu’s terms, boundary spanning can be conceptualized as a specific position-taking, i.e. a ‘structured system of practices and expressions of agents’ (Bourdieu & Wacquant, 1992, p. 105) arising from the encounter between the dispositions of the boundary spanners’ habitus (a collectively reinforced inclination to span the boundaries) and their (peripheral, boundary, intermediary) positions in relation to the fields involved (Bourdieu, 1983). 2 We propose that legitimation of boundary spanning roles and practices, taking place at the interface of several ‘intersecting’ fields, will involve changes in the volume and structure of capital available to boundary spanning agents (Bourdieu & Wacquant, 1992, p. 127).
Given the function of boundaries as protected entry points (Bourdieu, 1996), these changes are likely to challenge the established order in several fields and therefore affect inter-field dynamics. However, the role of multi-field configurations as sites of legitimation is under-theorized. While the broader literature on legitimacy suggests that the legitimation of novel work practices often involves extending ‘the existing stock of legitimacy’ (Walker, Schlosser, & Deephouse, 2014, p. 628) or borrowing the ‘accepted legitimating elements’ from established legitimate practices (Walker, 2004, p. 249) or broader cultural accounts (Creed, Scully, & Austin, 2002), there is a lack of understanding of how various forms of capital originating from different fields become selected and mobilized and what implications this process has on the direction of boundary spanning and power relationships between the intersecting fields.
As the amount and nature of capital at the agent’s disposal determine his or her position in the social space, any changes to capital distribution will inevitably affect boundary spanners’ social trajectories (Bourdieu, 1996, [1984] 2010). However, previous theoretical accounts of boundary spanning tend to approach legitimacy as a desired state enabling the transformation of ‘nominated boundary spanners’ into ‘boundary-spanners-in-practice’ (Levina & Vaast, 2005). Relatively little attention has been paid to the mechanisms of legitimation as a transformative process or to its effects on boundary spanners’ trajectories beyond their point of entry into the field. Similarly, generic processual models of legitimation, exploring the progression of novel practices from initial local acceptance towards institutionalization within a broader field (Drori & Honig, 2013; Johnson et al., 2006) do not adequately explain the temporal dynamics of capital redistribution or its effects on the exponents of these practices.
Aiming to explore the theoretical assumptions and address the research gaps outlined above, our empirical inquiry will be guided by the following research questions. How does the deployment of capital in the process of legitimizing boundary spanning roles and practices change over time? What implications do these changes have for the relationships between the intersecting fields and the social trajectory of boundary spanners?
Case and Method
Research setting
This paper draws on a qualitative longitudinal case study conducted in a large-scale collaborative partnership (‘Collaboration’) established in 2008 between a university and UK National Health Service (NHS) organizations. This partnership illustrates a recent international policy trend towards the creation of system-level collaborative entities in which researchers work closely with other stakeholder groups, such as clinicians and managers. Such collaborative initiatives seek to create an environment in which research findings can be more readily applied in day-to-day clinical practice, increasing the effectiveness and efficiency of healthcare service provision (Evans & Scarbrough, 2014).
This particular case was selected because the Collaboration was one of the few similar organizations in the country deploying designated boundary spanning roles to support knowledge translation between the producers and users of research. It also granted us a broad access to collect research material prospectively and longitudinally. Most importantly, the Collaboration represented a theoretical case suitable for exploring our research questions: from an ‘organization-as-field’ point of view (Emirbayer & Johnson, 2008, p. 22), it can be conceptualized as a joint ‘field-in-the making’ emerging at the interface of the established domains of science, medicine, management and policy (Kislov, 2014).
The Collaboration recruited eight designated non-clinical facilitators (‘boundary spanners’), whose broadly defined remit included a two-way transfer of knowledge between the university and multiple primary medical care organizations (‘general practices’) and supporting the latter in applying research evidence in their day-to-day practice. Designed by the Collaboration’s management academics, this newly created full-time role was adapted from the Knowledge Transfer Partnership (KTP) scheme which facilitates the links between the academic research base and industry in order to identify research-informed solutions to specific problems faced by practitioners (Acworth, 2008). Prior to joining the Collaboration, two facilitators worked in the NHS as nurses, three were employed in various managerial roles in the public and private sector, and the other three had recently graduated from university and had no previous full-time work experience. Embedded in cross-boundary multiprofessional project teams, the facilitators had hot desks both in the university and the NHS. They received guidance from (and were accountable to) management academics, clinical academics and programme managers, all of whom contributed to the development of this novel role.
The Collaboration’s boundary spanning activities were aimed at the creation of new co-produced programmes of research implementation, ultimately resulting in improved patient care in the participating general practices. In the UK, general practices are the main organizational actor in the field of general medical practice, a subfield within the field of medicine with a number of unique characteristics that need to be taken into account for the subsequent analysis (McDonald, 2009; McDonald, Checkland, Harrison, & Coleman, 2009). First, general practitioners (GPs), endowed by a high amount of field-specific cultural capital, are the most powerful professional group in this field, which contrasts with their relatively low status in the broader field of medicine. Second, most of the GPs, rather than being salaried public sector employees, enter into a contract with the national commissioning body, which means that GPs’ economic capital is invested in their practice and that the latter needs to be economically viable if they are to remain in the ‘game’. Finally, general practices are organized into clinical commissioning groups (CCGs) whose governing bodies are responsible for commissioning the majority of health services in the country (Checkland et al., 2013). 3
Data collection and analysis
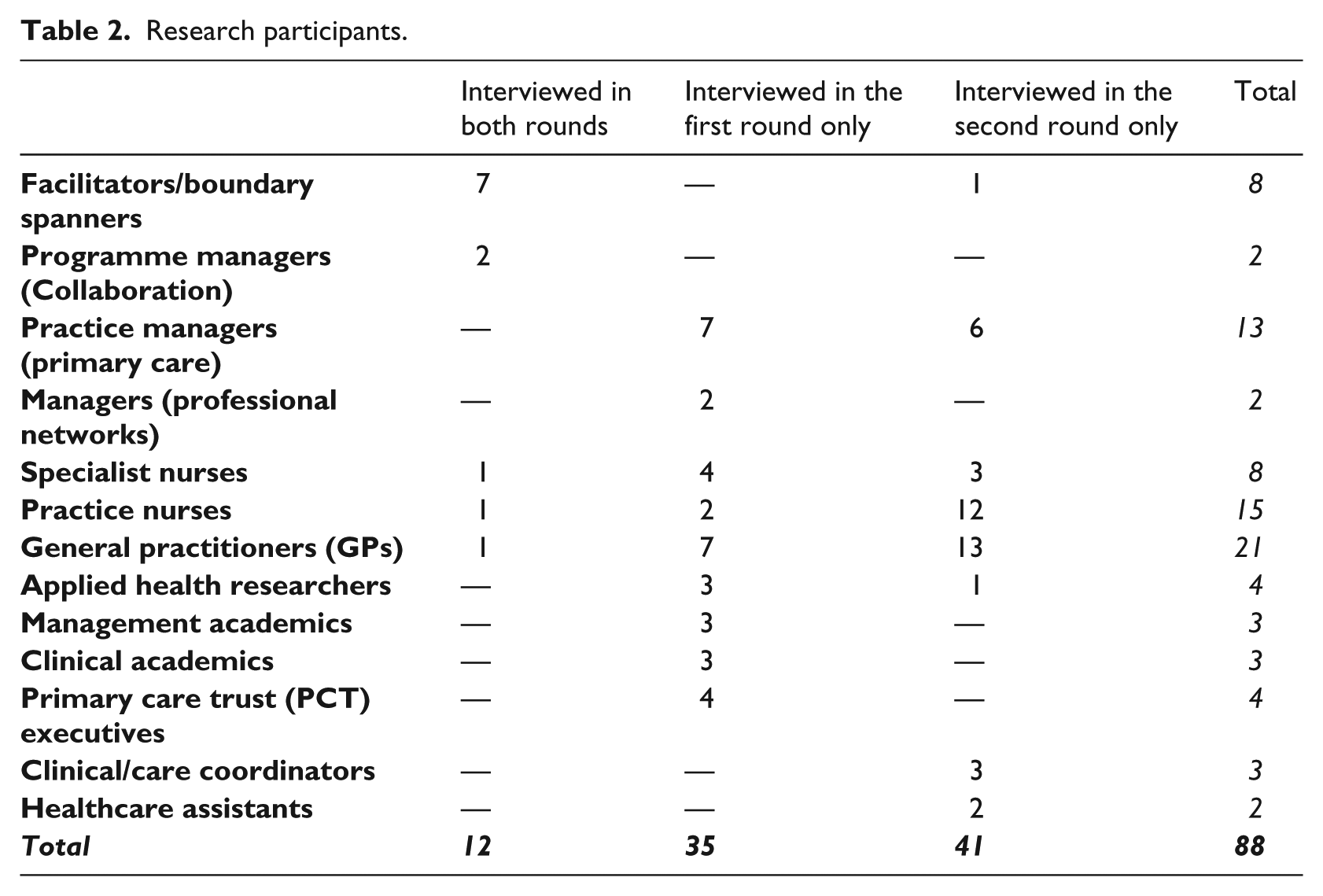
This study emerged from a broader research programme which was conducted in 2009–11 and explored the internal boundaries of the Collaboration (Kislov, 2014). Changes in the patterns of boundary interactions that became apparent relatively early in the course of fieldwork inspired a longitudinal extension of the initial programme with an explicit Bourdieusian focus on the legitimation of boundary spanning roles and practices. In total, 88 research participants were purposefully sampled both from the Collaboration’s core team and the fields of applied health research and general medical practice. The eight facilitators were naturally seen as key informants, and all of them were interviewed in the course of this research. At the same time, we significantly expanded the sample by including representatives of multiple groups who were involved in the intrinsically collective boundary spanning activities (Currie & White, 2012; Kislov et al., 2016a) and/or were in a position to contest or disapprove the legitimacy of the Collaboration’s boundary spanning roles and practices.
Semi-structured interviews (30 to 95 minutes in duration) served as the main method of data collection and were conducted (face-to-face or by phone) in two rounds (2009–10 and 2012–13) (Table 2). Almost all of the Collaboration’s facilitators and managers remained in their posts for the second round of data collection and were interviewed twice. However, as different general practices participated in the Collaboration’s projects in 2009–10 and 2012–13, this part of the sample significantly differed between the two rounds, remaining comparable in terms of the professional and organizational groups represented. In addition, a focus group was conducted with all facilitators at the end of 2013 to discuss the development of legitimacy over time. The first author also regularly engaged in informal conversations with research participants and observed meetings in which they participated, which provided opportunities for clarification and triangulation, significantly enriching the analysis.
Research participants.
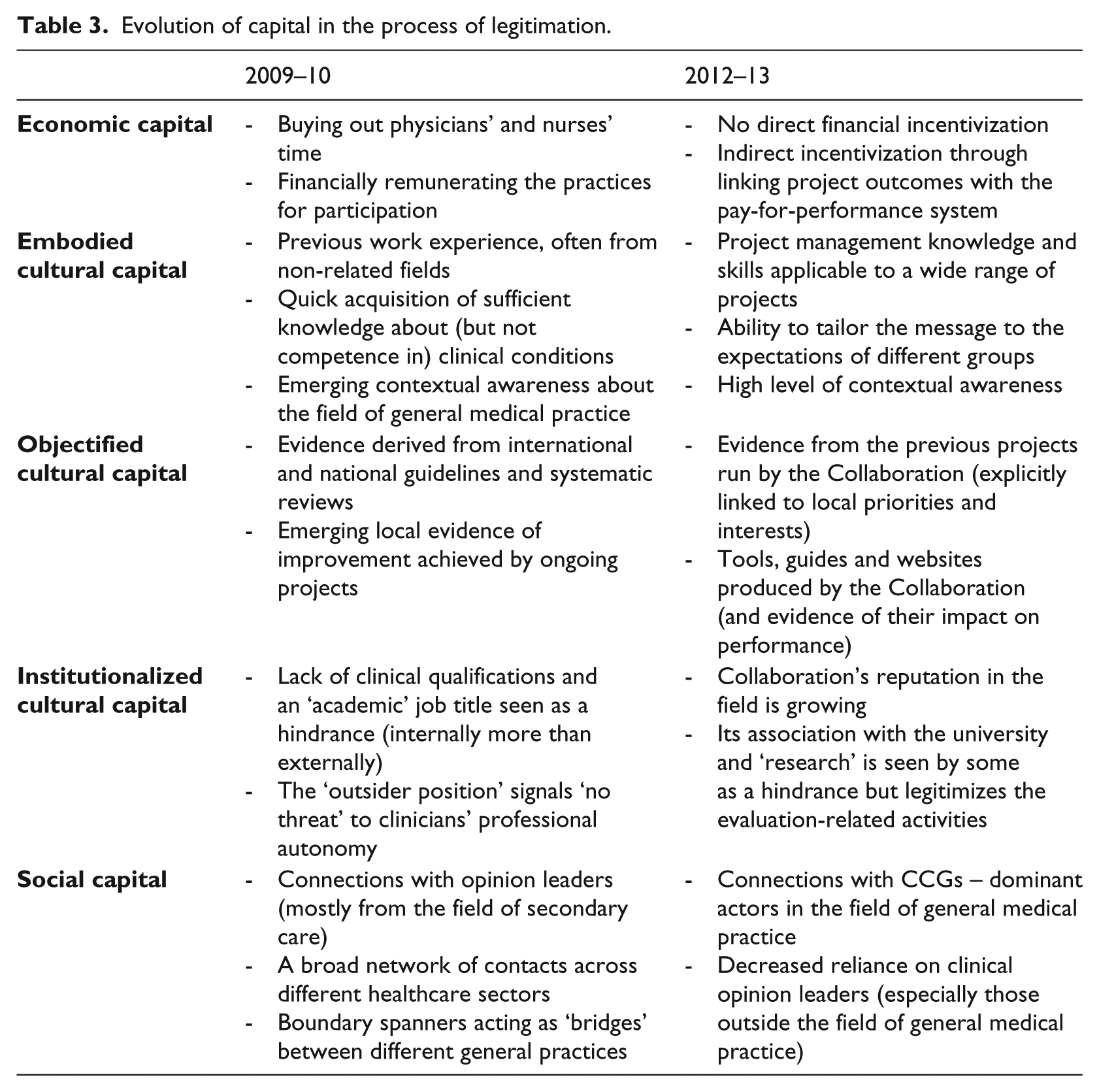
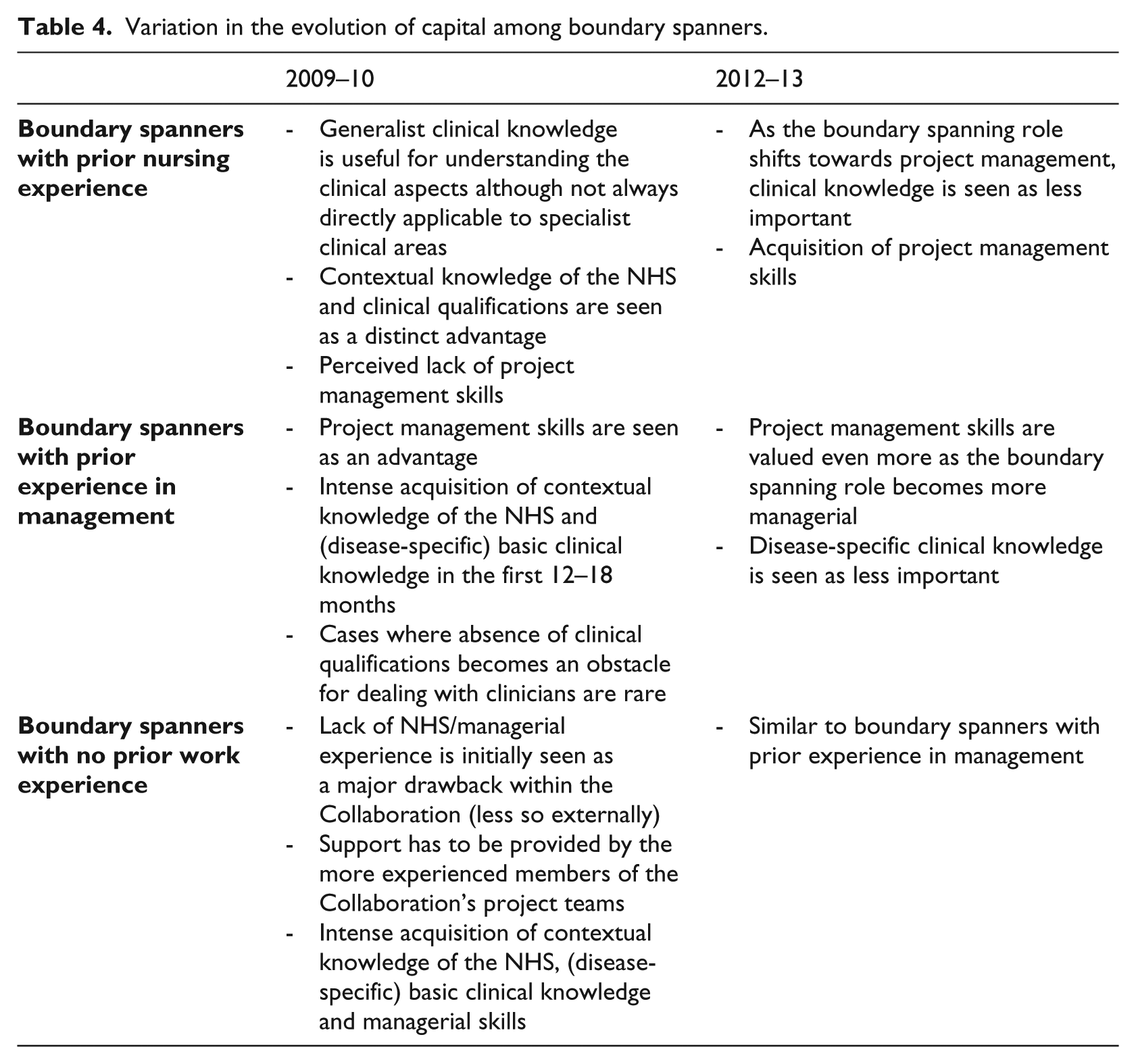
The interviews and the focus group were digitally recorded and transcribed verbatim; transcripts were coded and analysed with the aid of NVivo. The first stage of data analysis was predominantly inductive, involving a series of emergent descriptive codes and following a narrative analytical strategy that aimed at the construction of a detailed story from the raw data (Langley, 1999). The second stage of analysis involved a shift towards an ‘interpretative/theoretical case’ (Pettigrew, 1990, p. 280), linking the emerging narrative with the Bourdieusian framework and related theoretical debates in the literature. This involved the recoding of the two datasets, with most of the codes derived from the work of Bourdieu (e.g. embodied cultural capital; field boundaries; social trajectory). Matrix analysis was deployed to compare the coded material across different rounds of data collection (Table 3) and subgroups of boundary spanners (Table 4). This resulted in developing three main themes described in detail in the following empirical sections: (1) changes in the distribution of economic, cultural and social capital mobilized by boundary spanners; (2) implications of these changes for the relationships between the intersecting fields; and (3) effects on the social trajectories of boundary spanners.
Evolution of capital in the process of legitimation.
Variation in the evolution of capital among boundary spanners.
The Evolution of the Boundary Spanners’ Capital Structure
Economic capital
Our data clearly indicate the decreasing role of direct financial incentivization in the process of legitimation. In the beginning, some of the Collaboration’ projects provided remuneration to general practices for their participation and/or bought out clinicians’ time which could then be used for project work. Interestingly, the clinicians held somewhat ambiguous views about the Collaboration’s incentivization policies, perhaps due to the intrinsic propensity of economic capital to remain misrecognized (Bourdieu, 1986). Most clinical respondents claimed that their engagement was driven by the need to improve knowledge of a certain clinical area and the quality of patient care rather than by financial incentives, saying that the money ‘didn’t enter any of the team members’ heads’ (PM1-R1).
4
At the same time, they often admitted that economic incentivization was an important factor for ‘some other people’ working in the same practice and increased the practices’ motivation and capacity to do project work with the Collaboration’s boundary spanners: For me, [the funding issue] wasn’t [important], I must admit. For the GP it was, because we had to get a locum in to cover him. (PM5-R1) We worked more than we’ve been paid for, but it certainly comes in handy . . . (PM2-R1) Money certainly helps. It does certainly make people more motivated. . . (GP2-R1)
Over time, however, direct financial incentivization of practices started to be seen as requiring too many resources, making it unsustainable in the long run. In addition, it turned out to be insufficient on its own for recruiting the practices and engaging them in joint work with the Collaboration’s boundary spanners. In the later stages, the Collaboration stopped providing monetary remuneration to project participants, relying instead on indirect economic incentivization through linking the project activities with the pay-for-performance system adopted in the primary care sector: I personally don’t think we should [pay people to take part in the project] because it’s work that they should be doing anyway. . . . As a team we have definitely taken a different approach to that. We don’t pay people like we did at the beginning. (BS7-FG) There are [pay-for-performance] indicators around improving your register. So that was the main driver for the project. (BS8-R2)
Making these links explicit was often used by the boundary spanners, especially in the second half of the Collaboration, as a way of engaging the general practices in the Collaboration’s projects: We can demonstrate some of the benefits [to the practices] . . . ‘Every patient you add on to your register is however many [pay-for-performance] points and this amount of money’ kind of thing . . . (M2-R2)
Cultural capital
The boundary spanning roles created at the outset of the Collaboration were explicitly non-clinical, although two of the boundary spanners had a background in nursing. This meant that most boundary spanners did not possess sufficient clinical knowledge, skills and expertise (embodied cultural capital) or clinical qualifications (institutionalized cultural capital) and had to build their legitimacy with clinicians in other ways. First, the boundary spanners quickly acquired some knowledge about the clinical conditions they were working with, which often required an extensive reading of research papers and clinical guidelines until they felt that this knowledge was ‘good enough’ to allow them to implement their duties: After a time you realize that you can’t know everything. I’m not a clinician, I’m not going to know everything, but I can get to the point where I know enough and understand enough to hold a conversation without stepping on anybody’s toes, and then liaising or speaking to people who know an awful lot more than I do. (BS2-R2)
Second, they developed a deep understanding of the NHS context in which they were operating. One of the managers described this growing contextual awareness as: Understanding the context, understanding the NHS as a whole and understanding how the different groups of stakeholders that you work with within the NHS all fit together and what their motivations are and what are . . . the levers you can use to engage them. (M2-R2)
This knowledge allowed the boundary spanners to tailor their message differently for different groups operating within the field: At a CCG level it’s more about delivery . . . so we adapt to that level and we tap into what we know they want . . . We know they want an increase in prevalence . . . so when we go and talk to them, we will emphasize that . . . Whereas in a feedback meeting [at a general practice], if that’s not what we think makes them tick, then we won’t focus on that. We’ll focus more on clinical management. (BS3-R2)
Finally, boundary spanners emphasized their position outside the medical field as a way of differentiating their role from that of clinicians and preventing the latter from perceiving boundary spanning activities as an infringement of their professional autonomy: It can be an advantage, this outsider position: ‘I have no clinical knowledge at all; I don’t touch your expertise there. We are working in two very different arenas and let’s find a way to work together.’ We’re establishing almost the same goal and then saying, ‘I’m not a risk to your credibility and your status.’ (BS5-R1)
The use of objectified cultural capital (documents, tools and evidence) by boundary spanners also changed over time. While national-level guidelines and statistics were heavily relied upon as a source of legitimacy in the beginning, the focus shifted in later stages towards relying upon the context-specific evidence produced by projects in the local health economy. Where electronic tools or improvement guides were produced by the Collaboration teams, a conscious effort was made to present the evidence of their effectiveness on financial savings and/or patient outcomes: So you just have to find that thing that really plays on them and influences them. Sometimes it can be the financial outcome of it; sometimes it can be the patient outcome of it. (BS1-R1) Starting to use the audit tool in the second phase of work was actually a really powerful way to change practice because we were able to present concrete evidence to people. (BS6-R2)
Social capital
Unsurprisingly, the importance of building relational networks was seen as a major enabler of legitimacy. The focus of these networks, however, differed across the two rounds of data collection. In the early stages, connections with clinical opinion leaders, some of whom were formally affiliated with the Collaboration, were used by the boundary spanners both as a source of contacts and as a symbolic form of capital conferring legitimacy by virtue of their perceived reputation and influence in the field of general medical practice: The Kidney Tsar is a great reference source, who gives us a lot of credibility when we’re giving information [to the practices]. We can pass it on to a third party and they say, ‘Where’ve you found this from?’ and we can say, basically, ‘This is where we’ve heard this from.’ It’s a very, very credible source to have. (BS6-R1)
The second-round data show a relative decrease in the importance of clinical opinion leaders as a source of boundary spanners’ legitimacy. First, many of the opinion leaders were hospital doctors, which increasingly rendered their reputations, knowledge and contacts less relevant for the boundary spanning activities which were becoming more focused on the field of general medical practice: When it comes to practice-level delivery . . . they couldn’t give two hoots if [the hospital doctor’s] name is at the top of it or not; it doesn’t really have an impact then. (M1-BS2)
Second, as the boundary spanners were increasingly accumulating other forms of social and cultural capital, they relied less on their connections with influential clinical opinion leaders: It was [the clinical lead’s] contacts, liaisons, links, clinical colleagues who were really important initially, and now she kind of takes a step away from that and we use her . . . for advice about new things emerging rather than for a contact into different places . . . [Boundary spanners] do all that work rather than using [her] contact here, [her] contact there, because you have much more knowledge . . . (BS2-FG)
Finally, while the authority of clinical opinion leaders was instrumental for the initial engagement with practices, it proved insufficient for recruitment on a large scale and, in particular, for the spread of interventions from the practices taking part in the piloting stage of the Collaboration’s projects to a wider group of primary care organizations. In the later stage of the Collaboration, relationships with CCGs – local commissioning bodies – were seen as the most important form of social capital: Now it’s gone beyond just having that one person, like one GP, and in the projects that we’re running now . . . we’re invariably dealing with the CCG . . . (BS7-R2) The CCG level – that’s where our credibility comes; being able to pull things together to demonstrate that it’s not just about these individual practices. (BS3-R2)
Implications for the Relationships between the Intersecting Fields
Power relationships between the fields
The impact of the boundary spanners’ evolving capital structure on power relationships between the Collaboration and its primary care partners was complex. In many cases, boundary spanners were perceived as influential change agents, helping clinicians modify their everyday clinical work by applying clinical guidelines or service improvement approaches: [The boundary spanner] could bring the knowledge of how to manage the patients. . . and through the meetings that knowledge was transferred to us which is now in our practice and working there. (PM6-R1) [The boundary spanner]’s role was. . . reminding us about where directing us, where we needed to be . . . We were glad when it was over, in some respect. Because . . . we felt under a lot of pressure to perform with it. (PM2-R1)
The work that the general practices had to do as part of the Collaboration’s projects almost always fell within their normal clinical remit, relied on voluntary participation, was agreed with participants prior to the beginning of the projects and was financially rewarded either directly (through cash payments from the Collaboration) or indirectly (through meeting the practices’ performance targets). However, as the last quote shows, the requirement to perform more work was often met with at least some degree of resistance. In some cases, where the expectations, needs and opinions of local powerful players were not taken into account, the Collaboration failed to gain legitimacy with and exercise influence over primary care partners: We hit a brick wall in terms of our credibility when we went out and said, ‘This is what we are doing here.’ And our credibility in some places, where that didn’t align, plummeted . . . Where that happened, we’re not credible at all because we didn’t deliver what they expected, and their expectations weren’t managed at all. (BS3-FG) Rather than imposing something on people – it’s not about some secondary care clinician who happens to be a clinical lead for [the Collaboration] who’s got this idea and then goes out and tries to impose that on various PCTs – it’s more what [the partners] are interested in. (M2-R2)
As the last quote indicates, the authority of the Collaboration and its boundary spanners to enact change in primary care was contingent on how well their activities were aligned with the interests of primary care stakeholders. In the early stages, the recruitment of the practices and gaining access to them was managed on a practice-by practice basis, often involving ‘ego massaging’ (BS2-R1) of locally influential clinical opinion leaders, with an understanding that ‘you have to make yourself useful’ (BS5-R1) to general practices. In the later stages, the boundary spanners were able to negotiate involvement of larger groups of practices through demonstrating the ‘dirigible outcomes’ of projects (BS2-FG) to commissioners and persuading them that participation in the Collaboration could help them meet their financial and patient care targets.
Exclusion of applied health research from boundary spanning
It was expected that the Collaboration would span the boundaries between several key domains, including applied health research, implementation, health policy and clinical practice. Bridging the boundary between researchers and practitioners was seen to be of utmost importance. However, the accumulation of capital viewed as legitimate in the field of general medical practice was not matched by a corresponding increase in boundary spanners’ legitimacy with applied health researchers. Boundary spanners were seen by the latter as ‘ill-equipped to be trying to propagate best practice’, both due to the lack of research skills and because they ‘hadn’t got enough of a relationship’ (HR2-R1) with clinicians to gain access to the data that the researchers were interested in obtaining. Boundary spanners, in turn, felt disadvantaged by their lack of scientific knowledge and credentials: I haven’t got the academic background and I’m always aware of that, and sometimes it makes me feel uncomfortable when I’m sat around a lot of researchers because I can’t talk on your level. (BS4-R1)
It is therefore unsurprising that the intermediary position of boundary spanners at the interface of applied health research and general medical practice shifted towards the latter: There’s been very little work with [facilitators] . . . from the perspective of my research. (HR2-R1) There’s clearly some academic research work going on, but I’m not sure what it is, and I’m not quite sure how relevant it is to us as a primary care trust and working with our GPs . . . The [facilitation] stuff is the important stuff. It’s the research stuff that feels less important and distant to us. (PCTE1-R1)
At the same time, there remained some ambiguity in the boundary spanners’ relationship with research. On the one hand, there was little interaction with applied health researchers, and a perceived connection between the Collaboration and the scientific field was claimed to have a negative effect on the boundary spanners’ legitimacy with the field of general medical practice: Sometimes there’s a bit of misunderstanding, that [primary care staff] maybe think that we do research . . . It can really put practices off then, can’t it really? (BS7-FG)
On the other hand, boundary spanners claimed to be using peer-reviewed papers and the national guidelines to inform the implementation projects in primary care (especially in the initial phase of the Collaboration). In addition, they admitted that the research-informed evaluation work built into most of the projects was perceived by healthcare organizations as an enabler of the boundary spanners’ legitimacy: The CCG . . . see us as being much more forthright and more credible [than a consulting firm] regarding evaluation work. (BS2-FG)
Implications for the Social Trajectory of Boundary Spanners
Variation in initial capital endowments and internal legitimacy
In the first round of data collection, boundary spanners’ core responsibilities included a wide range of frontline activities involving coordination, negotiation and facilitation: [The boundary spanners] transferred knowledge about problems that other practices were having, and how they’d got over that; they transferred knowledge about things we were doing to other practices. (PM1-R1) What am I doing? It’s a lot of networking, stakeholder engagement, chasing people up and making things happen, negotiating, finding solutions, convincing people, and a lot of data analysis. (BS5-R1)
While remaining within the broad remit described above, in the first half of the Collaboration’s lifetime internal legitimacy of boundary spanners within the Collaboration was affected by their initial capital endowments determined by their previous experiences in other fields. Facilitators with a nursing background experienced a distinct advantage of possessing both institutionalized (clinical qualifications) and embodied (general clinical and contextual knowledge) cultural capital specific to the field of general medical practice. This enabled them to ‘open doors earlier and quicker’ (M1-R2), not least because ‘having certain letters behind your name helps in dealing with clinicians’ (BS5-R1), but also meant that they were not free from ‘the cynicisms and the preconceived ideas’ (M2-R2) about the NHS. By contrast, those facilitators who had no work experience prior to assuming the boundary spanning role were significantly disadvantaged by their lack of capital and widely perceived within the Collaboration as ‘pretty green and pretty junior and inexperienced’ (CA3-R1): That was a bit of a stumbling block at the beginning, because they knew nothing about the NHS, nothing about the culture, or anything . . . They’ve had to learn, quickly, how the NHS works. (BS7-R1)
In addition to having ‘a lot to pick up in a very short space of time’ (BS6-R1), novice non-clinical facilitators had to be supported by the more experienced academic and managerial staff: Because, obviously, [the clinical academic] is a working clinician and she was kind of the other part of me with these people, then that kind of filled the full . . . So I always had the best possible clinical input that I didn’t provide. (BS3-R1)
With the exception of rare cases where non-clinical boundary spanners were dismissed by clinicians due to the lack of clinical knowledge and credentials, in general these strategies (along with those described earlier) proved successful in establishing their external legitimacy with the NHS despite their capital deficiencies: Medical background was our territory. . . .What [the boundary spanners] were telling us is: what we should be looking [at] next, what we should be doing next. And it was our clinicians’ job to reach those targets. So they didn’t need to have medical knowledge. (GP4-R1)
Shift from boundary spanning towards project management
With an accumulation of managerial knowledge, contextual awareness and relational networks, initial differences between boundary spanners became less prominent, with a corresponding increase in the status of novice non-clinical boundary spanners within the Collaboration: . . .Now we see our guys are very skilled at working with primary care and they are able to relate to them a lot better than they were three or four years ago. . . .When you actually get in the meeting now, [non-clinical facilitators] can soon come over as very credible and they can soon build an effective relationship. . . They’ve become like opinion leaders in their own right. (M1-R2)
As their authority grew, boundary spanners started to be more involved in managing multiple projects, with a corresponding prioritization of skills related to project management over disease-specific knowledge: With the [previous project]. . . I was reading high-level clinical journals. . . With the [current project] it’s completely different. I don’t know anywhere near as much detail. . . it’s much more about the process where my key skills lie. . . in providing advice to help facilitation, almost being like a project manager, structurally organizing things, developing systems. . . much more so than having to know the clinical ins and outs of disease management. (BS2-R2)
The ongoing shift from an intermediary boundary spanning role towards a more traditional project management function was further reinforced by the secondment to the Collaboration’s project teams of several part-time clinicians, who took over some of the boundary spanning functions (Kislov et al., 2016a): It’s been a natural process that as we’ve become more experienced in delivering and leading the project, we’ve become more project management focused. And then the specialists we’ve brought in to support the project have become more of the actual boundary spanners. (BS6-R2)
In an interesting reversal of fortune, clinical knowledge and credentials of boundary spanners with a nursing background now mattered less, with the managerial skills of non-clinical boundary spanners being favoured in the new distribution of capital within the Collaboration: When I first started I know what made me credible is the fact that my background is in nursing . . . but I don’t think it’s as much as it was at the beginning. (BS7-R2) It might be worse to bring clinical staff in, because they don’t have the more core business skills really. . . But there’s an advantage to bringing in people with some . . . core project management skills. (M1-R2)
Discussion
Evolution of capital
Similarly to previous observations (Levina & Vaast, 2005), the boundary spanners in this study both accumulated and related different forms of capital in the process of joint working with the field of general medical practice. However, as our findings show, legitimation not only increases the volume of the overall capital mobilized but also involves significant changes in the relative weights, mutual convertibility and original sources of its specific forms, leading to the transformation of capital structure over time.
First, we demonstrate the changing role and nature of economic capital mobilized in the process of legitimation. Despite the acknowledged importance of economic factors in general practices as independent businesses (McDonald, 2009), boundary spanners increasingly relied on cultural and social capital rather than on the direct use of economic capital. The latter, however, was often mobilized indirectly, whereby linking the projects and their outcomes to the nationally mandated metrics led to a delayed but substantial financial benefit for the participating general practices. This shows how the linking of disparate forms of objectified cultural capital, such as project data, audit tools and performance measurement systems, can lead to their (partially disguised) conversion into economic capital (Bourdieu, 1986). At the same time, increasing reliance on performance targets can be explained by their legitimating function as a form of symbolic capital in its own right. These have become internalized by the field of general medical practice partly due to a strong tradition of healthcare standardization within the dominant discourse of evidence-based medicine (Cheraghi-Sohi & Calnan, 2013), and partly because performance measurement is deployed for benchmarking individual general practices notorious for their competitiveness (McDonald et al., 2009).
Second, we highlight the mechanisms through which boundary spanners surmount the lack of field-specific embodied and institutionalized cultural capital, i.e. clinical knowledge and credentials. Although we did observe the acquisition of basic disease-specific knowledge by boundary spanners at the beginning, this does not reach the level of competence possessed by clinical professionals. However, boundary spanners can successfully use these deficiencies to their advantage by discursively positioning themselves outside the jurisdiction of clinical professional groups and thus decreasing the perceived threat of boundary spanning projects to clinicians’ professional autonomy. Another strategy involves developing architectural knowledge (Currie & White, 2012), or knowledgeability (Omidvar & Kislov, 2014). This subtype of embodied cultural capital denotes a deep understanding of the ‘rules of the game’ unfolding in the field, its key players and relationships between them, forming an integral part of emerging boundary spanners’ habitus. Boundary spanners’ own capital deficiencies can also be compensated by the ongoing accumulation of social capital which can either be directly converted into the form of cultural capital being sought (for instance, through directly involving clinical professionals in the boundary spanning project) or used as a source of indirect ‘legitimacy by association’ with powerful local agents who have established clinical credibility (Baum & Oliver, 1991, p. 189).
Finally, it is important to trace the changes in the sources of the social and cultural capital mobilized by the boundary spanners over time. While it could be expected that the boundary spanners would acquire and/or mobilize a diverse range of capital assets derived from multiple fields, what we observed was the increasing focus on the cultural and social capital derived from one of the interrelated fields, namely the field of general medical practice, accompanied by the decreasing influence of social connections and objects from other fields. This is exemplified by the switch from national guidelines to the project-specific, locally tailored evidence as the preferred form of objectified cultural capital as well as by the shift from secondary care clinicians to primary care commissioners as the most legitimate co-producers of social capital. This indicates that an influential position in one (sub)field does not easily translate into symbolic capital in another, echoing previous accounts of the decreasing role of clinical opinion leaders beyond the initial stages of change initiatives (Hendy & Barlow, 2012).
Relationships between the fields
Legitimation through acquisition, mobilization and conversion of capital has traditionally been associated with gaining power within a given field (Bourdieu, 1986). Concurring with previous observations that boundary spanning is an inherently political and collective process (Currie & White, 2012; Kislov et al., 2016a), our findings demonstrate that the evolution of boundary spanners’ capital results in complex two-way power play which both shapes and is shaped by several intersecting fields at the interface of which they are operating.
On the one hand, our data demonstrate the growing reputation and influence of the Collaboration and its boundary spanners in general practices, with the increasing number of primary care organizations engaged in its projects. This often involved co-opting clinical agents and drawing on their capital assets. On the other hand, the influential representatives of the field of general medical practice had the power to approve or disapprove the Collaboration’s activities. The selection of clinical conditions for improvement projects, the formulation of their objectives, the recruitment of general practices and the spread of resulting improvement were all contingent on such approval. Overall, the relative gain of power achieved by boundary spanners only becomes possible through acknowledging (and utilizing) the field-specific rules of the game, the power structures and the distribution of capital endorsed by the most influential members of the (established) field they are interacting with.
According to Bourdieu (1977), legitimate authority is a misrecognized, i.e. socially recognized, form of domination. However, neither the Collaboration and its boundary spanners nor primary care clinicians seem to clearly fit the ‘dominant’/‘dominated’ dichotomy (also see Kamoche et al., 2014). The blurring of the distinction between these categories can be explained by the formation of an alliance (Bourdieu, 2000) between the Collaboration’s boundary spanners and the influential agents in the field of general medical practice. This alliance enabled the former to meet their objective of facilitating the application of research evidence in clinical practice. The powerful agents within the field of general medical practice, in turn, gained an opportunity both to increase the volume of capital in their possession and to preserve its structure, potentially acquiring an important bonus in their power struggles with the rival field of secondary care (McDonald et al., 2009). Interestingly, through an increasing alignment with the patterns of capital distribution adopted in primary care, internal legitimacy of boundary spanners within the Collaboration became contingent on their external legitimacy in the field of general medical practice to the detriment of the scientific field (see Drori & Honig, 2013).
As a result, boundary spanning increasingly took place between the Collaboration’s multiprofessional implementation team (the joint field of collaborative practice) and primary care organizations (the field of general medical practice) rather than directly between the latter and applied health researchers (the scientific field). This suggests that, where marked power differentials exist between the intersecting fields, some of these fields can be prioritized in the process of boundary spanning at the expense of others. At the same time, given the low credibility of the boundary spanners in the eyes of applied health researchers, excluding one of the established fields from the emergent field of collaborative practice can also be interpreted as a rather innovative way of responding to the contestation of boundary spanners’ legitimacy. Ironically, the marginalization of a certain group of agents (e.g. researchers) from the emergent collaborative field does not seem to preclude utilization of capital (e.g. evaluation methods) associated with these agents as a way of reinforcing the external legitimacy of boundary spanners and of the emergent field of collaborative practice in general.
Social trajectory of boundary spanners
Newcomers into a field may differ in the volume and structure of their initial capital at the point of entry due to the natural differences between their career trajectories shaped by their previous experiences in other fields (Bourdieu, [1984] 2010; De Clercq & Voronov, 2009b). One might anticipate that different groups of boundary spanners, i.e. those with a nursing background, those with managerial experience and those with no job experience, would differ in their legitimation strategies and social trajectories (Battilana, 2006; Lockett, Currie, Finn, Martin, & Waring, 2014; Lockett et al., 2012). However, despite significant initial differences in the volume and structure of cultural capital in their possession, variation in the legitimation dynamics between individual boundary spanners proved much less pronounced. This may suggest that the peripheral and relatively low-status nature of the boundary spanning position can, at least partly, level out the impact of previous professional and status differences on its incumbents’ subsequent trajectories within the field.
We show that initial capital deficiencies of individual boundary spanners can be compensated not only by gradual accumulation of missing capital assets but also by reliance on capital accumulated by agents they are interacting with. By highlighting the complementarity and exchange of capital in the process of boundary spanning this study enhances our understanding of the mechanisms underpinning its inherently collective nature (Currie & White, 2012; Kislov et al., 2016a). Interestingly, although boundary spanners with a nursing background had a distinct advantage in the form of clinical knowledge and qualifications, i.e. field-specific cultural capital, its legitimating effect was limited to the earlier phases of the Collaboration. Possible explanations may include limited applicability of discipline-specific clinical knowledge to other clinical disciplines (Martin, Currie, & Finn, 2009), the dependence of legitimacy upon continuous engagement in professional practice (Kislov et al., 2016a) and, most importantly, a general trend towards managerialization of boundary spanning over time.
Our findings demonstrate that successful legitimation can effectively transform nominated boundary spanners, i.e. agents utilizing their ambiguous ‘in-between’ position to span boundaries between the intersecting fields, into project managers, i.e. occupants of a traditional role recognized by (and embedded within) one of the fields. This tendency illustrates the transience and instability of nominated boundary spanning roles as a novel mode of organizing and the relatively high risk of its reversal to more traditional modes of management (Chew et al., 2013; Kislov et al., 2016b). Interestingly, despite an associated increase in status and authority, the managers-in-the-making did not generally attempt to contest the existing distribution of capital, internal boundaries and ‘ways of doing things’ within the field of general medical practice. Absence of such strategies, which are often associated with middle-status agents (Bucher et al., 2016; Lockett et al., 2012), can be explained in our case by relative peripherality of boundary spanners in relation to inter-professional struggles within the field, lack of formal ‘consecration’ of their de-facto managerial role (Bourdieu, 2000, p. 243) as well as by the ‘inertia’ of their habitus which was shaped by their previous lower-status position in relation to the field (McDonough & Polzer, 2012).
By describing the radical shift in boundary spanners’ trajectory, our study reveals a highly transformative potential of legitimation, demonstrating that its possible ‘successful’ outcomes are not confined to transitions from an ‘apprentice’ to ‘master’ (Lave & Wenger, 1991) or from a ‘nominated boundary spanner’ to ‘boundary-spanner-in practice’ (Levina & Vaast, 2005) but may include lateral shifts within the field. Furthermore, boundary spanners, perhaps due to the increased propensity of peripherally located lower-status agents to decipher ‘the rules of the game’ and ‘unmask’ power relationships (Bourdieu, 2000; Bucher et al., 2016), can relatively quickly overcome the mismatch between their individual dispositions, which are shaped by their previous engagement in past fields, and the current field (see McDonough & Polzer, 2012). The fact that we observed this shift across all of our boundary spanners allows us to interpret it as a non-random and relatively durable change of their emerging collective habitus under the influence of the forces operating in the most influential field they are interacting with (Bourdieu, 1983, [1984] 2010; Emirbayer & Johnson, 2008).
Postscript to the empirical case
One year after we finished the fieldwork for this study, five boundary spanners were still employed by the Collaboration, all of them now holding formal managerial positions. Three of them embarked on postgraduate courses in healthcare management. These developments support our argument by demonstrating that the capital accumulated by boundary-spanners-turned-managers was objectified as a formal organizational position and further enhanced by educational credentials (Bourdieu, 1977).
Conclusion
Legitimation of boundary spanning at the interface of several intersecting fields is underpinned by the evolution of economic, social and cultural capital accumulated and mobilized by nominated boundary spanning agents. This evolution involves a number of changes: first, in the overall volume of capital at boundary spanners’ disposal, with some of the capital assets being ‘borrowed’ from other agents with whom the boundary spanners interact; second, in the sources of mobilized capital, whereby one of the fields involved is prioritized at the expense of others; and, third, in the relative weights of different forms of capital, with an increasing emphasis on the knowledge of the ‘rules of the game’ unfolding in the dominant field. These developments lead to an increase in the boundary spanners’ influence and authority but, at the same time, firmly position them within the existing schemata of capital distribution adopted by the dominant field. Ironically, this may result in the marginalization and erosion of the very roles and practices that were being legitimized.
Our theoretical contribution is threefold. First, we present a multi-layered analysis of boundary spanners’ legitimation by explicating two-way links between micro- (individual capital endowments of agents), meso- (their emerging collective dispositions and position-takings) and macro-level (configurations of intersecting fields) components. In so doing, our enquiry responds to the calls ‘to draw together and amalgamate’ different forms of capital (Özbilgin & Tatli, p. 861) and shifts analytical focus from discursive practices deployed in the process of legitimation (Landau et al., 2014; Sanders & Harrison, 2008; Suddaby & Greenwood, 2005) towards its underlying mechanisms and unintended consequences. It specifically highlights the transformative nature of this process that can, paradoxically, result in the radical transformation of ‘the object of legitimation’ itself (Johnson, 2004, p. 11).
Second, we demonstrate the applicability of a Bourdieusian theoretical framework, traditionally deployed for the analysis of internal processes within single fields, to complex configurations of intersecting fields, differentially related to the broader ‘field of power’ (Bourdieu & Wacquant, 1992, p. 18). More specifically, we show that legitimation of agents and activities representing the new ‘joint field of practice’ (Levina & Vaast, 2005, p. 335) that emerges in the process of collaboration between several established institutional fields is likely to be determined by the old ‘rules of the game’ adopted by the field whose field-specific capital is seen as more valuable within the meta-field of power. Not only can this imbalance constrain the previously described renegotiation of power relationships in emergent fields (Reay et al., 2006), but it is also likely to present formidable obstacles to their ‘maturation’ and institutionalization.
Finally, by exploring the experiences of novice boundary spanners longitudinally, ‘beyond the entry phase’ (De Clercq & Voronov, 2009b, p. 409), this study enhances our understanding of the social trajectory of individuals located at the field periphery. It demonstrates that vulnerability and instability of a peripheral position (Yanow, 2004) may be resolved through a lateral shift of the agent’s trajectory, exemplified in our case by the switch from boundary spanning to project management. We highlight that following ‘the rules of the game’, which underpins this shift, inevitably constrains boundary spanning roles and practices but, at the same time, allows the agents to surmount their individual capital deficiencies. From the agentic perspective, this journey could therefore be interpreted as reflective adaptation of habitus allowing the boundary spanners not only to ‘stay in the game’ but also improve their standing in it.
At the micro-level, our analysis challenges the assumption that boundary spanners can be expected to maintain equanimity and neutrality of their ‘in-between’ position (Chew et al., 2013; Kislov et al., 2016b). At the meso-level, it highlights constraints arising from the inherently collective nature of boundary spanning, where dependence on the capital assets of the co-opted agents may lead to the ‘colonization’ and redefinition of boundary spanning by the more powerful groups. At the macro-level, it puts into question the ability of mandated boundary spanning initiatives to enact substantial reconfiguration of boundaries located in multi-field contexts with significant power differentials between the fields. Our conclusions are likely to be applicable to a wide range of collaborative contexts, particularly those deploying specifically designed boundary spanning, knowledge brokering and change management roles positioned at the lower end of organizational hierarchy.
This study is not without limitations. First, given the focus on boundary spanning as a collective phenomenon, the exploration of the individual dispositions and identities of boundary spanners remained beyond the scope of this work. Second, different project contexts within the Collaboration were not compared because over time all of the boundary spanners became involved in more than one project. Third, due to the relatively short-term nature of the Collaboration’s projects, different groups of general practices were included in the two rounds of data collection, although the analysis did not identify any significant differences that could potentially impact the interpretation of the legitimation patterns observed. Finally, this paper did not address issues specific to the legitimation of boundary spanning clinicians as these are discussed elsewhere (Kislov et al., 2016a).
The findings suggest that boundary spanners’ professional background has a certain effect on their legitimation strategies, for instance through symbolic deployment of clinical knowledge and credentials. We call for an in-depth exploration of these issues by utilizing the notion of habitus as a link between the past and the present (Bourdieu, 1993; Emirbayer & Johnson, 2008) as well as between the individual and the collective (Bourdieu, 1990). We would particularly encourage inquiries into the complex interplay between individual boundary spanners’ characteristics (e.g. their status in the organization/profession or employment history) reflecting their past trajectories and the emerging collective boundary spanning practices developing within the current multi-field configuration in which they are embedded.
Footnotes
Acknowledgements
We are grateful to Julian Williams, Etienne Wenger-Trayner, Sophina Choudry and other convenors and participants of the Social Theories of Learning course at the University of Manchester for providing insights and encouragement at the conception of this study. We would also like to thank Federica Angeli and the participants of Sub-theme 55: Re-examining the Organization of Healthcare: Institutional, Technological and Clinical Challenges at the 31st European Group for Organizational Studies (EGOS) Colloquium; Royston Greenwood and the participants of the 3rd Annual University of Edinburgh Business School Paper Development Workshop; and the three anonymous Organization Studies reviewers for their constructive comments on the earlier versions of this article.
Funding
This work was supported by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC) Greater Manchester. The views expressed in this article are those of the authors and not necessarily those of the NHS, NIHR or the Department of Health.